
Abstract
Background
A growing number of older adults in the United States have multiple chronic conditions which contribute to decreased functional ability and increased healthcare utilization. Unmet supportive care needs place considerable strain on caregivers, particularly of persons living with dementia. Community-based palliative care can help seriously ill individuals manage their conditions and improve their quality of life. How palliative care staff explain these services to older adults and caregivers can impact engagement with palliative care.
Objectives
To explore knowledge of palliative care among older adults and caregivers in a Medicare Advantage population, including dementia caregivers, and identify areas for improving education and explanations.
Methods
Semi-structured interviews were conducted with seriously ill Medicare Advantage plan beneficiaries and caregivers (n = 22) who declined the plan’s palliative care program in the past year. Focus groups were conducted with palliative care staff (n = 5).
Results
Beneficiaries and caregivers had mixed understandings of palliative care, including: no knowledge, belief that it was the same as or pre-hospice, and accurate, but often one-dimensional understandings of it. Participants recommended providing individualized, tailored explanations focused on the person’s health concerns in simple language with follow-up materials to improve engagement with palliative care.
Conclusions
Small adjustments to how palliative care is explained may increase understanding among older adults and caregivers, particularly among those with limited or inaccurate knowledge. Among those familiar with palliative care, providing accessible and clear explanations customized to the person’s specific care needs can further broaden understanding and increase perceived relevance.
Keywords
Introduction
The growing aging population in the United States means increasing numbers of older adults with disability and functional limitations requiring assistance managing their health.1,2 Three to four out of five individuals aged 65+ live with multiple chronic conditions and may have unmet care needs resulting from serious illness,3-5 including increased symptom burden, acute care utilization, and diminished quality of life.6,7 Identifying and accessing appropriate support is particularly challenging for those with complex conditions such as the one in ten older adults living with dementia and their caregivers.8,9
Palliative care is an approach to health care that focuses on preventing and relieving suffering for those living with serious and advanced illness and their families, encompassing physical, psychosocial, and spiritual domains.10,11 Community-based palliative care (CBPC), an integrated model of care offered in outpatient settings, 12 can help those living with serious illness to reduce symptoms, improve quality of life, and reduce healthcare costs, enabling seriously ill individuals to stay safely at home.13-15 It is offered by a growing percentage of Medicare Advantage (MA) plans as part of value-based care models. 16 Unlike home health care, CBPC does not require an intermittent skilled need for eligibility. 17 CBPC can be offered at any point in serious illness and offers additional coordination, symptom management, and supportive services to what geriatrics primary care typically provides. However, many individuals decline services when offered, potentially due to lack of knowledge about it and how it may help them.18,19
Prior research has demonstrated that the majority (70%) of U.S. adults have no knowledge of palliative care 20 and that there is persistent association with hospice care. 21 Familiarity with CBPC may vary significantly by sociodemographic characteristics, including education level and personal history of disease/diagnosis.20,22 Many individuals who are eligible for CBPC may have inaccurate or incomplete understandings that may contribute to declining services, even when they are concerned about challenges CBPC can address. 23
This pilot study uses perspectives of seriously ill individuals, family caregivers, and CBPC staff to elucidate the understanding of CBPC in a group of MA beneficiaries and their families—including caregivers of persons living with dementia—who were eligible for CBPC and declined it. We also sought to identify how explanations and education around CPBC can be improved.
Methods
Study Design and Setting
This qualitative study was conducted between April and November 2024 with a not-for-profit care management and home healthcare organization in a large, Northeastern United States city. The MA plan they offer provides CBPC at no additional cost through telephonic and in-home visits by nurses, social workers, and nurse practitioners in consultation with physicians. Individuals are eligible for CBPC, regardless of age or diagnosis, if they are referred from the MA plan’s home health care or are identified at high or very high risk for 12-month mortality by a machine-learning algorithm developed by the MA plan and receive a score of 10 or more on the screening tool developed by the healthcare agency. As part of the eligibility determination process, they undergo further telephonic assessment by care managers and receive an in-home evaluation by a nurse practitioner.
Study Population
MA plan beneficiaries (“beneficiaries”) and caregivers (e.g., family members, friends) were considered for this study if they had declined CBPC, offered as part of their MA plan, in the previous year and were English-speaking, regardless of diagnosis. Caregivers were contacted if the beneficiary was unable to participate (e.g., due to dementia). Seventy out of 75 individuals meeting inclusion criteria were contacted for participation: 24 consented, 14 were not interested, and the 32 were unreachable (n = 20) or ineligible (n = 12) (e.g., deceased). Five were not contacted due to thematic saturation. Thirty were caregivers of persons with a primary diagnosis of dementia: 11 consented, 11 declined, and 8 were unreachable/ineligible. The final sample of twenty-two was comprised of beneficiaries (n = 4) and caregivers (n = 18) who completed an interview.
Five PC staff included all full-time employees that supported the CBPC program and were trained in explaining CBPC to eligible individuals and families. Outreach/care managers (n = 3) responsible for screening eligibility and case management and the nurse practitioners (n = 2) providing in-home visits had 7-40 years of professional experience (mean = 18.8, standard deviation (SD): 13.5); between 1-3 of those years on the CBPC team (mean = 2, SD: 0.7).
Data Collection
Question guides were developed by EAL in consultation with KHB. One-time individual interviews with beneficiaries and caregivers and 3 focus groups with PC staff were conducted by study staff trained in qualitative interviewing over videoconference, audio recorded and transcribed using automated transcription, then checked for accuracy and deidentified. Interviews lasted, on average, 27 minutes (SD: 12). Focus groups lasted, on average, 53 minutes (SD: 12); 2 individuals participated in 2 focus groups. All participants provided informed consent and received a $75 gift card for each interview or focus group. This study was approved by the Rutgers University and VNS Health Institutional Review Boards (IRB).
Data Analysis
We analyzed transcripts for themes related to understanding of palliative care (PC) and how it might be better explained. 24 Codes were developed deductively by EAL, based on the research and interview guide questions; we added a small number inductively during analysis, based on recurring sub-topics. 24 Two study staff trained in qualitative methods independently coded and reviewed discrepancies. 24 Intercoder reliability was assessed in NVivo (mean Cohen’s kappa score: 0.96; SD: 0.015). 25 Upon coding completion, 2 study staff reviewed findings and organized content into themes. The individuals who conducted the analysis are not clinicians. However, the interview guide was developed and subsequent findings interpreted collaboratively by individuals experienced in clinical care KHB and palliative care research, EAL.
Results
Demographic Information for Participants
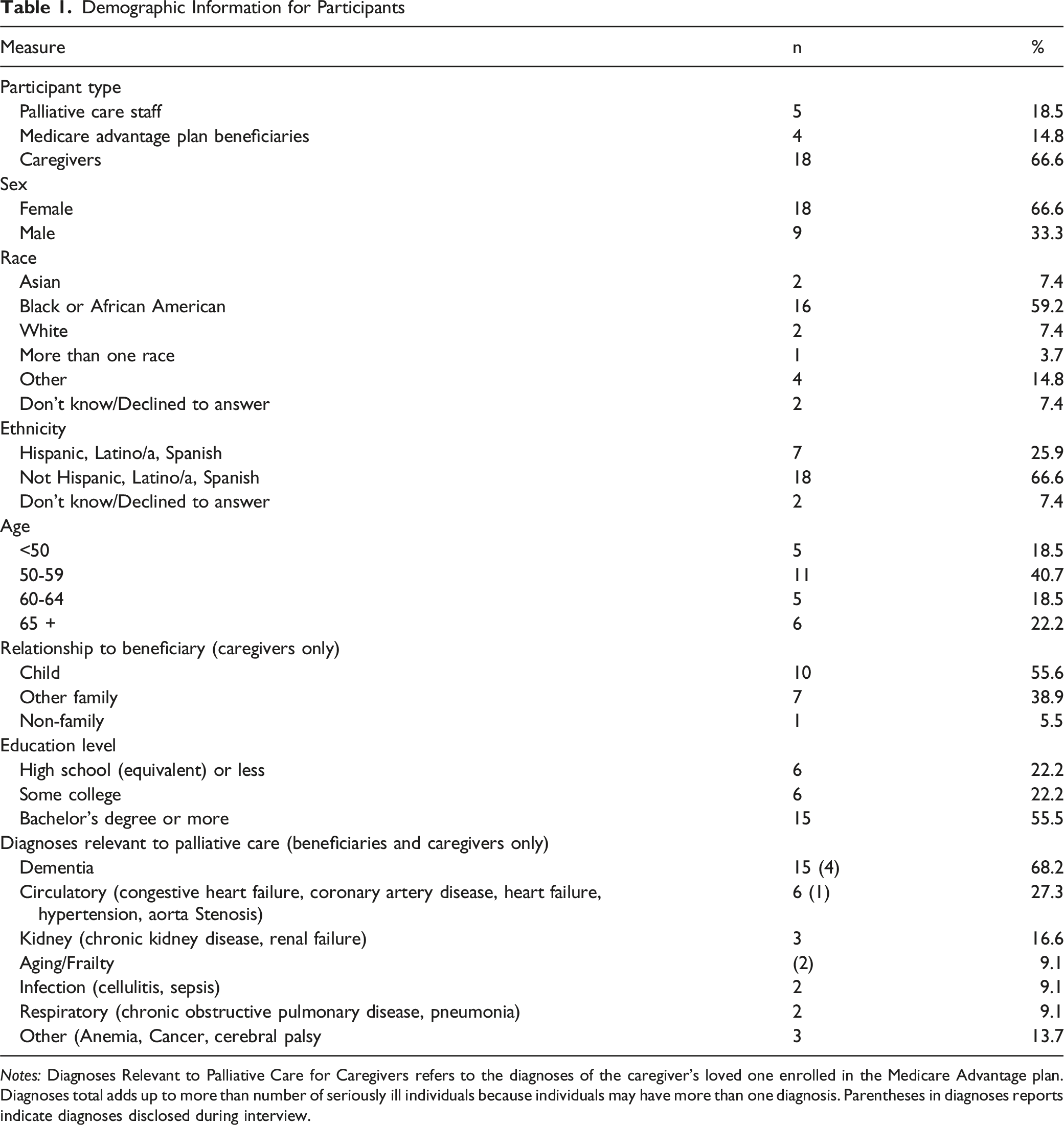
Notes: Diagnoses Relevant to Palliative Care for Caregivers refers to the diagnoses of the caregiver’s loved one enrolled in the Medicare Advantage plan. Diagnoses total adds up to more than number of seriously ill individuals because individuals may have more than one diagnosis. Parentheses in diagnoses reports indicate diagnoses disclosed during interview.
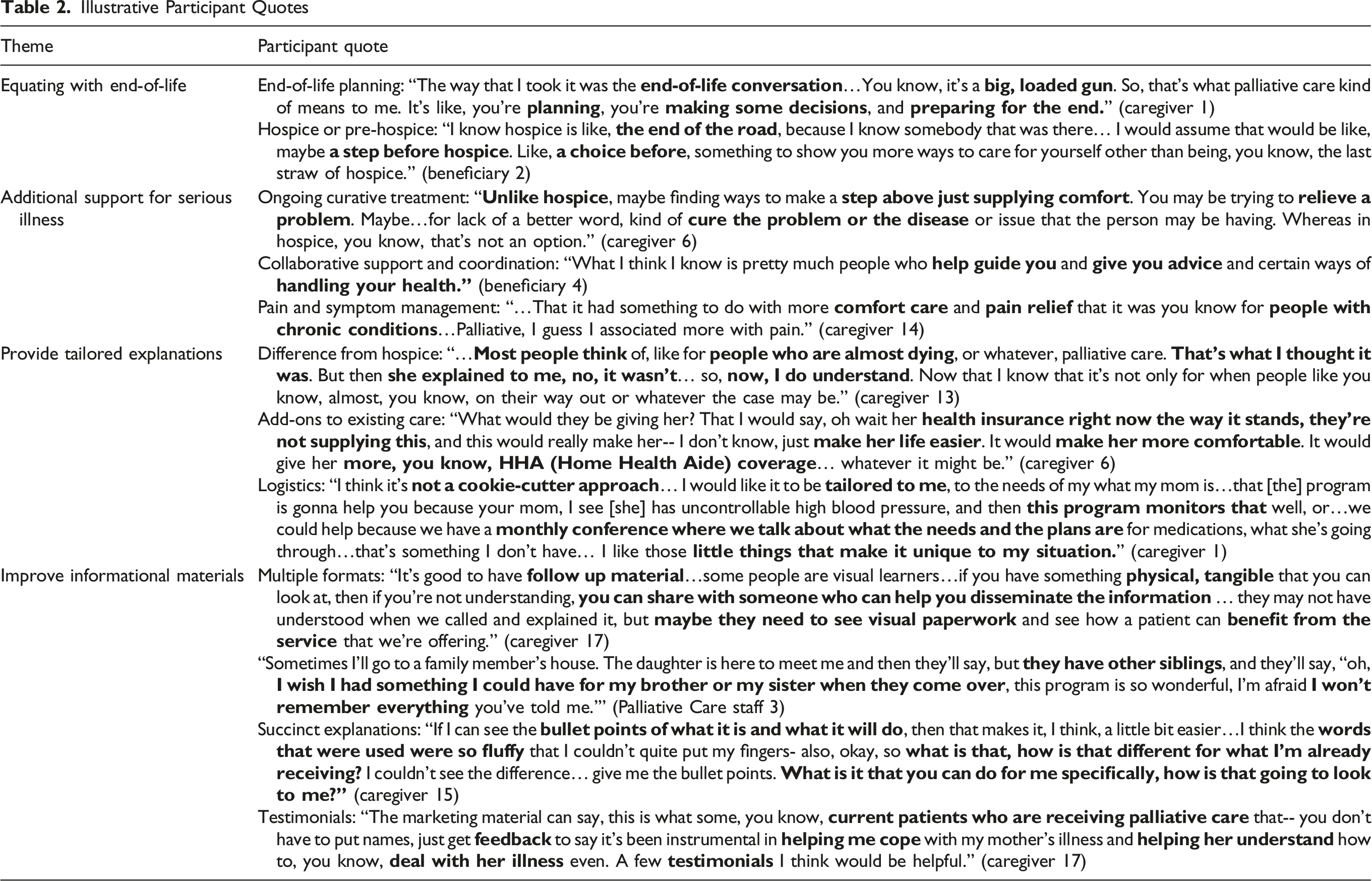
Illustrative Participant Quotes
How is palliative care understood?
“The end of the road”: Equating with end of life. About one third of beneficiaries and caregivers associated PC with end-of-life planning and care, including some who viewed PC as hospice or pre-hospice care. One caregiver described that they now understand the difference between the 2 after receiving explanation from PC staff, but did not at the time of call. PC staff regularly encountered families and patients who believed hospice care always followed PC.
“Palliative care is hope:” Additional support for serious illness. Two thirds of beneficiaries and caregivers understood PC with varying degrees of accuracy. Over half of beneficiaries and caregivers differentiated PC from hospice, indicating that it allows for continued curative treatment and that it is more optimistic than hospice. About half of beneficiaries and caregivers indicated PC provided collaborative support and coordination for managing serious or chronic illness. One third of beneficiaries and caregivers emphasized pain and symptom management as a key component of PC. One fourth of beneficiaries and caregivers identified all three of these aspects when describing PC. PC staff also observed these understandings among the beneficiaries and caregivers they encounter.
How can explanations of CBPC be improved?
“It's not a cookie-cutter approach”: Provide tailored explanations. Two caregivers suggested a clearer explanation of how PC differs from hospice. Seven caregivers identified a need for explanations of CBPC that clearly distinguish it from their current healthcare and explain how it is relevant to their specific, individual needs, including addressing ambulatory limitations, psychosocial aspects of caregiving, and general ongoing medical issues associated with aging. Seven caregivers indicated it would be helpful to understand logistics regarding service provision. These findings were nearly exclusively discussed by caregivers of PLWD. PC staff echoed the importance of tailoring messaging about PC and emphasized the value of clear communication with beneficiaries and caregivers around expectations for how services are provided.“Something to turn back to” and eliminating “fluff”: Improve informational materials. Beneficiaries and caregivers suggested developing printed informational material (e.g., pamphlet, flyer, or folder) describing the CBPC program that beneficiaries and caregivers could refer back to and use to facilitate decision-making with other family members. One caregiver suggested informational materials include clear, concise bullet points to facilitate understanding of the CBPC program. Participants also suggested including testimonials about the CBPC program to increase beneficary and caregiver confidence in it.
Discussion
This pilot study improves our understanding of what MA beneficiaries who decline PC and their caregivers, including a large proportion caring for PLWD, know about it and how to explain PC in a way that increases receptivity. One third of beneficiaries and caregivers associated PC with hospice or end-of-life care, consistent with limited knowledge and mis-associations regarding PC observed in broader the population.20,21 Two thirds offered explanations of PC that were accurate, but only partially explained PC. Notably, the 4 who provided more comprehensive and multi-dimensional explanations of CBPC had at least an associate degree. Two worked in healthcare, which might make them more familiar with PC. Requests for individually tailored explanations that explain how CBPC addresses specific health concerns, expands on current care, and detail surrounding logistics were often discussed by caregivers of PLWD. This may be related to PLWD’s distinct care needs and underscores a need for explaining CBPC in a way that addresses these needs directly.
One approach to addressing inaccurate and incomplete understandings of CBPC is to provide explanations that provide a more complete picture of what CBPC offers and how it can address unmet needs to improve alignment with goals of care. Acknowledging the hesitance of patients being offered CBPC and leading with information to address concerns or common misconceptions, such as services being exclusive to those at end of life, may help beneficiaries and caregivers feel heard and understood. One approach is to emphasize the benefits of PC, such as improved symptom control, quality of life, and opportunities for advanced care planning. This approach may make individuals more receptive to reconnecting CBPC if something changes in their health status. Additionally, building on the tendency for individuals to understand concepts and health information in terms of what is relevant to them,26,27 providing explanations of CBPC that focus on first identifying an individual’s needs and then tailoring CBPC explanations to specifically address those needs may increase receptivity to accepting. This may be facilitated by having staff introducing CBPC utilize tailored phone scripts or educational materials that offer information about how CBPC can address challenges of their specific illness (e.g., one for heart failure, another for dementia, etc.). Developing materials using insights from seriously ill individuals and their caregivers and from clinical staff, such as care managers and nurse practitioners, could facilitate more relevant and customized descriptions of CBPC, tailored to the populations served by each program. Explanations of CBPC should be offered in multiple formats and using language that is easily understood and fosters confidence in the program.
This pilot study is limited to the experiences of individuals at a single MA plan. However, it provides important information about how to think about presenting CBPC to seriously ill individuals in a way that is individually tailored and easily understandable. Additionally, it is possible that some individuals who received an explanation of CBPC may not have benefitted from it had they enrolled. Feedback provided by CBPC-eligible participants, regardless of suitability for CBPC, can be used to improve the clarity and quality of all CBPC explanations, which allows individuals to make more informed decisions about their care. Future research might focus on understanding similarities and differences in how CBPC should be explained based on care setting (e.g., hospital, doctor's office, telehealth) and serious illness profile.
There is a persistent lack of knowledge and mis-associations surrounding PC that represent opportunities for further education to enable seriously ill individuals and caregivers to make informed healthcare decisions. This pilot study demonstrated that many people have some, albeit a limited, understanding of PC. Providing individualized explanations tailored to a person’s needs, in simple and clear language, may be key components in increasing seriously ill individuals’ and caregivers’ comfort with and acceptance of CBPC services.
Footnotes
Ethical Considerations
All study procedures were approved by VNS Health and Rutgers University’s Institutional Review Boards.
Consent to Participate
All participants provided informed consent.
Author Contributions
EAL and KHB developed the conceptual idea for this project. EAL supervised the study and collected the data. KGS and EAL conducted the analysis and interpretation of the results. KGS drafted the manuscript with input from all authors.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by a pilot grant from the University of Pennsylvania Roybal Center on Palliative Care in Dementia and the National Institute on Aging (NIA), a department under the National Institute of Health (NIH) under award number P30AG064105.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.