
Abstract
Objectives
This study aimed to: (1) explore Chinese nursing interns’ perspectives on a “good death” through their participation in the Heart to Heart Tea House; (2) derive insights for nursing education; and (3) inform the improvement of end-of-life care narratives in China.
Methods
Using convenience sampling, 24 nursing interns participated in the Heart to Heart Tea House activity in eight groups of three. Each group engaged in facilitated discussions centered around three self-selected cards. All dialogue was recorded verbatim and analyzed using Braun and Clarke’s thematic analysis until data saturation was reached, with no new themes emerging from subsequent interviews.
Results
Four main themes emerged: (1) emphasis on autonomy and dignity in end-of-life care, (2) natural acceptance of death and reflections on life’s meaning, (3) the need for comfort and physical care in the terminal stage, and (4) considerations of social relationships and emotional support. The interns highlighted the importance of respecting individual choices, maintaining dignity, achieving a peaceful state of mind, managing physical symptoms, and fulfilling emotional expressions.
Conclusion
The Heart to Heart Tea House proved to be an effective platform for nursing interns to reflect on and articulate their views regarding a good death. The findings offer valuable guidance for developing targeted nursing education programs and enhancing patient-centered end-of-life care services, emphasizing the significance of integrating such initiatives into healthcare practice.
Introduction
A “good death” is conceptualized as the process through which terminally ill patients achieve acceptance of death while addressing their social, emotional, and material concerns. 1 The core objective is to achieve peace and serenity at the end of life. 2 This concept reflects not only respect for the dignity of individual life but also signifies the progress of social civilization. Hospice care represents a clinical application of the good death philosophy. 3 For hospice care providers, a correct understanding of the “good death” concept is fundamental. This concept encompasses elements such as dignity, symptom management, autonomy, preparedness, and emotional peace, all of which are crucial for delivering compassionate, patient-centered end-of-life care. 4 As future hospice care providers, nursing interns are clinical trainees in transition from students to professionals, currently undergoing a critical phase in the development of their professional values and identity. 5 Therefore, understanding nursing interns’ perspectives on “good death” holds significant implications. It serves not only as a reflection of their attitudes toward death but also directly correlates with clinical care quality and family experiences, while profoundly impacting their professional identity development and psychological well-being.
Existing qualitative studies have revealed that nursing interns commonly experience significant negative emotions, including depression, anxiety, fear, and distress, when confronted with patient death.6,7 These emotions not only impair their physical and mental well-being but also exacerbate the severe issue of nursing talent attrition in China (with an annual nurse turnover rate reaching 7.7%). 8 Therefore, there is an urgent need to systematically investigate nursing interns’ understanding and perspectives on “good death” to develop learner-centered hospice care education. While some prior research has explored nursing interns’ attitudes toward death,9,10 their in-depth conceptualization of “good death” remains underexplored, particularly within the Chinese cultural context. This gap is largely attributable to the cultural sensitivity of the topic; the deep-seated taboo surrounding death in Chinese tradition poses a significant challenge to obtaining genuine and reflective responses. 11 In this context, the Heart to Heart Tea House presents an innovative methodological solution. By utilizing specially designed cards and a facilitated group format, it creates a relaxed and non-threatening atmosphere. 12 This environment is crucial for lowering psychological defenses and enabling participants to engage in open, profound discussions about this otherwise sensitive subject, 13 thereby allowing researchers to access their authentic perspectives.
Methods
Study Design
This study employed a descriptive qualitative design to explore nursing interns’ perspectives on “good death” during their participation in the Heart to Heart Tea House. 14
Study Setting and Participants
This study employed convenience sampling to recruit nursing students for participation in the Heart to Heart Tea House during November-December 2024. Eligible participants met the following inclusion criteria: (1) Nursing students currently undergoing clinical internships in hospitals; (2) Willingness to participate in the study. Exclusion criteria includer: (1) Students not interning at the study hospital during the research period (eg, due to sick leave or personal leave); (2) Those who withdrew due to physical or psychological difficulties.
Heart to Heart Tea House Process
The Heart to Heart card set consists of 54 cards, including 13 cards for physical needs (♠), 13 for psychological needs (♦), 13 for social needs (♣), and 13 for spiritual needs (♥). Additionally, there are two special wish cards (jokers) to express unlisted needs when the other 52 cards cannot adequately address participants’ requirements. In this study, each session of the Heart to Heart Tea House was co-facilitated by a facilitator and a guide, with each group comprising three nursing interns. The process of the Heart to Heart Tea House is illustrated in Figure 1. Heart to Heart Tea House Process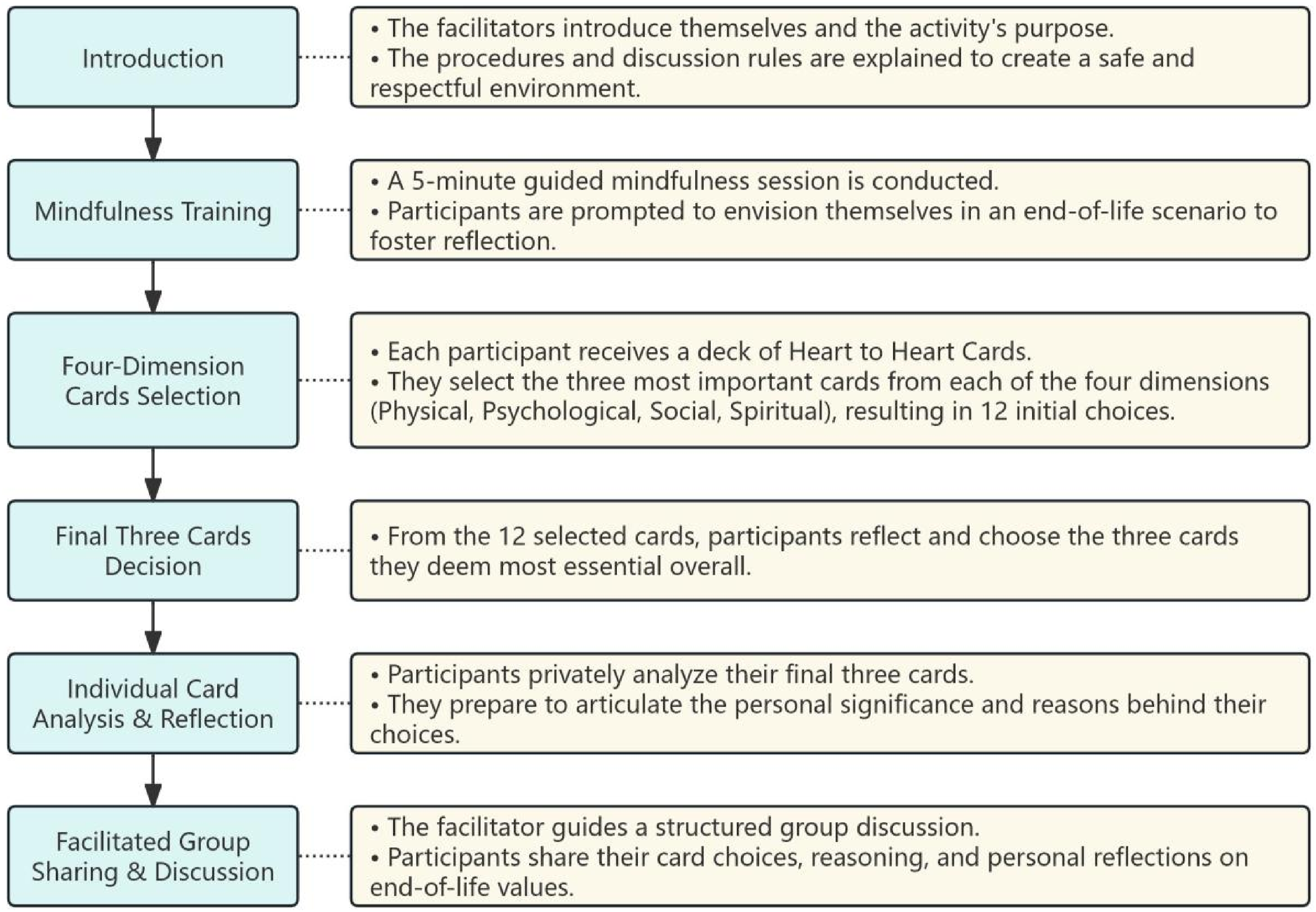
Data Collection
Participants Recruitment
Participants were recruited from five tertiary hospitals between September and December 2024. The first author screened potential participants for eligibility, explained the study objectives and procedures, and obtained written informed consent.
Group Interview Procedure
Data were collected through semi-structured, one-on-three interviews using open-ended questions. Group interviews were employed to facilitate in-depth discussion by leveraging group dynamics, allowing participants to refine their perspectives through mutual exchange and collective deliberation. 15 This approach elicited diverse viewpoints and stimulated deeper reflection, thereby generating richer insights than individual interviews. 16
An initial interview guide was developed by CACCC, with relevance and clarity verified through pilot interviews with three nursing interns. The finalized guide centered on the core question: “Could you share the three cards you selected and your rationale for choosing them?” This question was systematically posed during Step 6 of the Heart to Heart Tea House activity. Interviews were conducted in a relaxed atmosphere in a medical demonstration classroom. The study adhered to the Standards for Reporting Qualitative Research (SRQR). 17 To mitigate potential social desirability bias, facilitators emphasized the non-judgmental nature of the activity and encouraged honest expression.
The research team comprised two professors, four nursing graduate students, and the head of the nursing department. The team leader oversaw the study design and quality control, while other members were responsible for research coordination, participant recruitment, interview implementation, and data analysis. All interviews were conducted by the first and second authors, who are postgraduate nursing students trained in qualitative research methods and had no direct working relationship with the participants.
Data Saturation and Transcription
Data saturation was achieved after eight interviews involving 24 nursing interns, confirmed by no new codes emerging in two subsequent interviews. 18 Each interview began with a restatement of procedures and confirmation of participants’ rights. All interviews were audio-recorded and lasted 40-60 min. The first author transcribed recordings verbatim in their original language immediately after each interview.
Data Analysis
The interview data were analyzed using qualitative thematic content analysis, which is primarily used to validate, refine, or extend a theoretical framework in a new context. 19 Data collection and analysis were conducted concurrently. First, two researchers read the transcripts repeatedly to immerse themselves in the data and gain a general understanding of the interns’ perspectives on good death. Following this, the first author conducted initial open coding. The codes were then reviewed by another researcher, and any disagreements were resolved by referring back to the original interview text. Subsequently, the first author categorized the main themes by selecting participants’ quotes that supported each theme. When analyzing quotes, the researchers carefully considered the central ideas of participants’ conversations to understand their viewpoints on good death. All authors discussed the assigned codes repeatedly until consensus was reached. The entire data analysis process was conducted in Chinese, and the data were ultimately translated into English.
Rigor
To ensure trustworthiness, data analysis involved multiple researchers in the coding and theme development process to foster analytical triangulation and reduce investigator bias. Additionally, to mitigate potential social desirability bias arising from the facilitators’ presence, the facilitators received specific training to maintain a neutral and non-judgmental stance throughout the activities. Participants were emphasized that there were no right or wrong answers, encouraging authentic sharing.
Ethical Considerations
This study followed the ethical principles of the Declaration of Helsinki for medical research involving human subjects. Prior to implementation, ethical approval (No. 2024082) was obtained from the Ethics Committee of Hangzhou Normal University. Participants received full disclosure of study aims, procedures, and anonymization protocols before providing informed consent. Data confidentiality and exclusive use for research purposes were guaranteed.
Results
Demographic Data
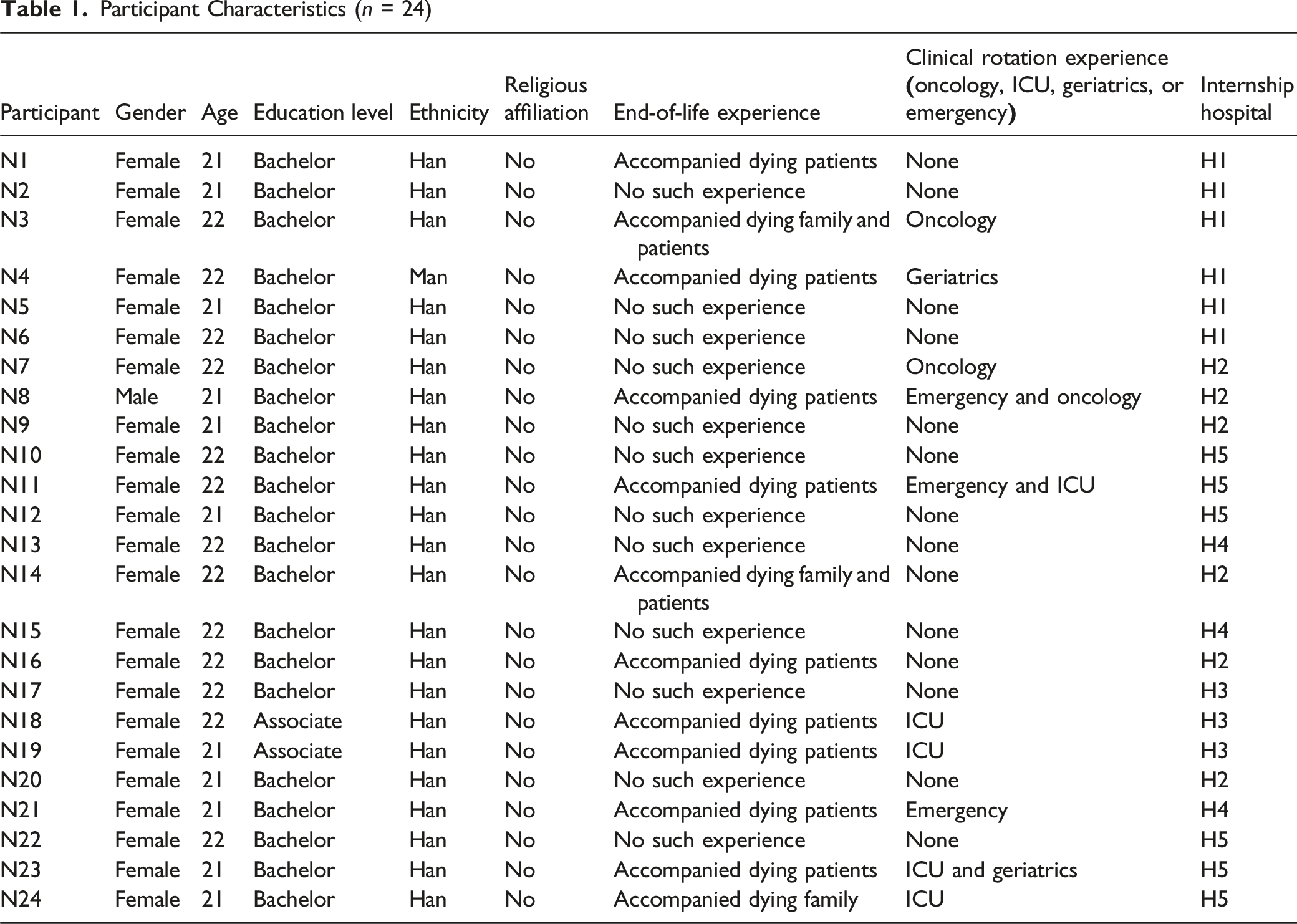
Participant Characteristics (n = 24)
Qualitative Research Themes
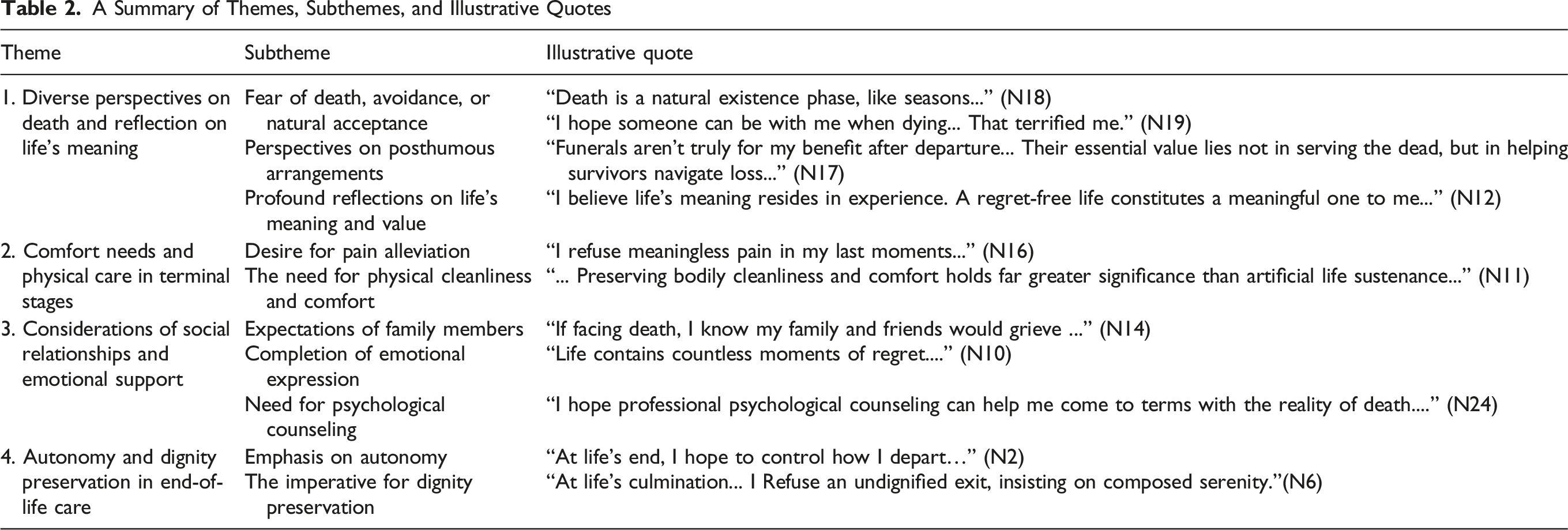
A Summary of Themes, Subthemes, and Illustrative Quotes
Theme 1: Diverse Perspectives on Death and Reflection on Life’s Meaning
Fear of Death, Avoidance, or Natural Acceptance
The nursing interns expressed varied perspectives on death. Most viewed death as an inherent phase of life, advocating natural acceptance over aggressive interventions. While the majority emphasized that serene acceptance outweighs agonized resistance, some expressed fear stemming from anticipated loneliness or distressing manifestations of dying. Death is a natural existence phase, like seasons—where life exists, death must follow. Mortality defines life’s fundamental condition. Since the outcome is inevitable, why forcibly alter it? What must come will come; natural acceptance may be optimal. Mechanical interventions might prolong life transiently but often fail to ensure genuine comfort, potentially compromising final dignity and peace. (N18) I hope someone can be with me when dying. In my ICU rotation, an elderly grandmother vomited blood with rolling eyes—alone without family. That terrified me. (N19) My grandmother recently passed. I want to express missing her, but dare not mention her to my grieving parents. Our family never discusses death openly, especially now. (N3)
Perspectives on Posthumous Arrangements
Participants demonstrated a pragmatic view of funeral rituals, perceiving them as serving the emotional needs of the bereaved rather than the deceased. They concurrently emphasized the importance of autonomy in planning personal funeral arrangements. Funerals aren’t truly for my benefit after departure. They function as a cathartic mechanism for the bereaved—providing structured emotional expression, memorialization, and ritualistic closure. While death terminates the deceased’s existence, for the living, funerals are transitional rites facilitating reality assimilation and grief processing. Thus, their essential value lies not in serving the dead, but in helping survivors navigate loss and reconstruct meaning. (N17) I’ve never attended a funeral—growing up, it seemed forbidden and mysterious. My family believed children shouldn’t be exposed. But I’ve read about people planning their own farewells. I’m drawn to pre-arranging mine. Life involves compromises, but shouldn’t death at least be on my own terms? (N1)
Profound Reflections on Life’s Meaning and Value
Participants universally affirmed that life’s essence resides in meaningful experiences, where both joys and adversities become indispensable in shaping identity. They aspired to minimize lifelong regrets, pursuing fulfillment without remorse. Many emphasized sustaining passion until life’s end—such as through travel to appreciate worldly beauty—thereby embracing life’s continuing vitality and possibilities. I believe life’s meaning resides in experience. A regret-free life constitutes a meaningful one to me. Even if my life were to end in my twenties, having lived without regrets would enable me to face death with equanimity. (N12) You know, my whole life I've loved discovering how big and beautiful this world is. Even now, if I’m nearing the end, I’d still choose to keep traveling—seeing new places, meeting different people. It’s not just about the trips themselves. When I'm out there moving through mountains or cities, I feel... alive. Competent. Like I’m still part of things, not just lying around waiting for death. Every journey feels like a quiet rebellion—proof that as long as I can step forward, life keeps its magic. (N13)
Theme 2: Comfort Needs and Physical Care in Terminal Stages
Desire for Pain Alleviation
Participants expressed a strong desire to avoid unnecessary suffering and aggressive interventions during the terminal phase. They specifically identified uncontrolled pain and respiratory distress as critically compromising quality of life, inducing anxiety and helplessness. Thus, they emphasized symptom management as paramount for a peaceful transition, asserting that effective pain control and bodily ease enable confronting death with equanimity. I refuse meaningless pain in my last moments, having witnessed terminal patients trapped in agony—tethered to tubes, struggling between suffering and helplessness. (N16) Severe pain obliterates all considerations—how could one contemplate final wishes? (N4) Respiration is life’s most fundamental need, directly determining comfort. Dyspnea and physical pain induce intolerable distress, requiring meticulous management. Only with comfortable breathing and bodily ease can one face mortality with equanimity. (N24)
The Need for Physical Cleanliness and Comfort
Participants universally emphasized that maintaining cleanliness, comfort, and quality sleep constitutes fundamental requirements for physical and mental well-being, particularly during the terminal phase of life. My ICU rotation demonstrated that while intubation and CPR may transiently prolong life, they often entail profound suffering and dignity loss. I categorically reject such interventions for myself. Preserving bodily cleanliness and comfort holds far greater significance than artificial life sustenance through mechanical means. (N11) Cleanliness and comfort represent basic human needs that transcend physical sensations to directly influence psychological states. When the body exists in comfortable conditions, the mind naturally achieves greater serenity. (N22) Proper sleep not only alleviates physical distress but maintains cognitive clarity and positive outlook. Regardless of life's stage, the ability to sleep well constitutes a precious source of strength and contentment. (N9)
Theme 3: Considerations of Social Relationships and Emotional Support
Expectations of Family Members
Participants expressed a desire to prevent their families from suffering emotional distress, hoping they can accept death as a natural conclusion and live on with peace and happiness. Financial burden due to treatment was also a concern, as participants did not want their families to sacrifice well-being for life extension. If facing death, I know my family and friends would grieve - the very scenario I most wish to prevent. While I understand their sorrow stems from love, I would feel helpless, even anxious, knowing my attempts at comfort might deepen their pain. I want them to face my passing peacefully, remembering our joyful times rather than mourning my absence. (N14) I hope they can view death properly, without sadness, and spend my final moments with me happily, not missing our last time together due to grief. (N20) Coming from a modest background, I would feel profound guilt if my treatment burdened my family financially or compromised their wellbeing. Their happiness and stability matter more to me than life extension. (N8)
Completion of Emotional Expression
Participants expressed a strong desire to articulate previously unspoken gratitude, love, and apologies during their final days through the practice of the “Four Themes of Life”, seeking inner peace and closure. They believed this emotional catharsis would not only facilitate their own tranquil departure but also assist family and friends in processing grief and achieving healing. Life contains countless moments of regret. To voice genuine thanks, love, and apologies at the end would provide perfect closure, making one’s journey truly worthwhile. (N10) For whom do we truly live? In my final hours, I yearn for heartfelt conversations with my most cherished ones, articulating every unspoken word and suppressed emotion. (N15) I wish to properly bid farewell to loved ones and the world itself. Just as I entered this life with hope and experienced its beauty, so too do I wish to depart with grace. Whether saying goodbye to dear ones or expressing gratitude for existence, I hope to do so peacefully and warmly—making my passing not just an ending, but a final tribute and blessing to life itself. (N23)
Need for Psychological Counseling
Although only one participant explicitly expressed the desire for professional psychological counseling, this view was retained as a subtheme because it represents an underrecognized but critical aspect of end-of-life care, particularly in a cultural context where psychological support is often stigmatized. The participant explained: I hope professional psychological counseling can help me come to terms with the reality of death. I believe such counseling would not only provide me with feelings of being understood and supported, but also help release my inner anxieties and suppressed emotions. More importantly, it would offer a safe space where I can freely express my deepest feelings without worrying about burdening those around me with my emotional state. (N24)
Theme 4: Autonomy and Dignity Preservation in End-of-Life Care
Emphasis on Autonomy
Nursing interns strongly preferred maintaining end-of-life decision autonomy, viewing bodily integrity as both a symbol of autonomy and an expression of personal value—a state to preserve throughout life and death. They emphasized that authentic expression of feelings is essential for peace. When facing advanced disease and uncontrollable suffering, they favored choosing timely departure as liberation, preserving dignity and tranquility in final moments. At life’s end, I hope to control how I depart—not passively accept everything while losing life control. Expressing genuine thoughts brings peace and comfort. (N2) I entered the world with a complete body and wish to maintain this integrity when leaving. Bodily wholeness symbolizes autonomy beyond physicality. In life or death, preserving this completeness demonstrates respect for my life and commitment to personal values. (N5)
The Imperative for Dignity Preservation
Nursing interns emphasized preserving terminal privacy and composure, rejecting undignified public exposure. They equally demanded post-death dignity, opposing impersonal handling while insisting on meticulous, respectful care. At life’s culmination, I demand absolute privacy. Death is an intensely intimate experience shielded only from my most cherished relations. I seek a tranquil, dignified departure—not a spectacle of diminishing propriety. Death transcends biological cessation; it must be a final act of self-preservation. I refuse an undignified exit, insisting on composed serenity. This is my ultimate self-respect and final existential expectation. (N6) Honoring ante-mortem wishes to enable self-determined dignified passage epitomizes life’s supreme reverence. Human dignity and autonomy remain inviolable at existence’s threshold. (N7) Post-death, I require the same dignity as in life. I merit respectful treatment in existence and beyond. I categorically reject perfunctory death management, demanding meticulous care in final disposition. (N21)
Discussion
Self-Education Achieved by Nursing Interns Through Heart to Heart Tea House Participation
The results showed that although the participants presented diverse attitudes towards death, they were able to express their views rationally. This psychological shift, breaking the traditional death taboo, can be attributed to two factors. Demographically, the sample, consisting of Millennials, demonstrated greater openness to discussing death. 20 More importantly, the Heart to Heart Tea House provided a dedicated space for end-of-life dialogues. 21 By hearing diverse opinions and real-life stories, students engaged in deep reflection on life’s value, forming a rational view of death. This reflection not only reshaped their perspectives on life and death but also motivated them to overcome emotional expression barriers prevalent in Chinese culture. 22 Several participants reported during debriefing that they were more likely to practice the “Four Themes of Life” concept after the activity, expressing long-suppressed gratitude, apologies, and love to their relatives, thereby achieving psychological reconciliation and emotional relief. Essentially, this process reflected deep self-education through self-reflection, highlighting the Heart to Heart Tea House’s innovative value in promoting death education and emotional communication.
Nursing Interns’ Multidimensional Perspective on Good Death: Physiological Needs, Dignity Preservation, and Family Responsibilities
The findings demonstrated that participants in the Heart to Heart Tea House articulated their understanding of good death through the lens of physiological needs, identifying pain management, bodily cleanliness, and physical comfort as fundamental criteria. This perspective aligns with Maslow’s hierarchy of needs, reaffirming the primacy of physiological requirements in human wellbeing. 23 Additionally, the interns emphasized end-of-life dignity concerns, particularly privacy and decorum maintenance during terminal stages. Their heightened awareness of these bodily and dignity-related needs likely stemmed from direct clinical exposure to dying patients, 24 where they witnessed firsthand the foundational role of symptom management and dignity preservation in palliative care.
Notably, the study revealed a pronounced sense of familial responsibility and altruistic orientation among nursing interns when discussing mortality. This inclination resonates deeply with traditional Chinese cultural values that prioritize familial bonds 25 and aligns with prior research on Chinese end-of-life attitudes. 26 The interns demonstrated multidimensional consideration of death - while contemplating their own mortality, they predominantly focused on mitigating potential emotional and financial impacts on their families. Their reflections exhibited nuanced understanding of familial emotions: they simultaneously acknowledged anticipated grief while hoping relatives could transcend sorrow to cherish shared memories. This complex, family-centered thanatological perspective, rooted in a collectivist cultural context, offers valuable insights for developing culturally sensitive death education programs.
Nursing Interns’ Focus on End-of-Life Autonomy and the Significance of Advanced Care Planning
The findings revealed that nursing interns demonstrate heightened concern regarding end-of-life autonomy, with a prevailing expectation to independently make decisions pertaining to terminal care. This observation not only underscored the prevalent deficiencies in respecting patient autonomy within clinical practice, 27 but also aligned with research by Bovero et al, 28 further emphasizing the critical importance of safeguarding autonomous decision-making during terminal stages. Moreover, this study highlights the value and necessity of Advanced Care Planning (ACP) as a crucial mechanism for preserving patient autonomy. ACP refers to the process whereby competent individuals predetermine their medical preferences for potential future incapacity, demonstrating significant efficacy in reducing physician-patient decision conflicts, enhancing quality of life for terminal patients, and alleviating psychological burdens on families.29,30
In contemporary society, although the significance of ACP has gained widespread recognition, ACP education within palliative care curricula remains underdeveloped due to cultural avoidance of death-related topics in public settings. 31 Most courses in China only provides a basic definition of ACP and then simply encouraged students to complete “My Five Wishes,” which is insufficient for helping students deeply understand ACP and may lead to unmet educational goals.32-34 Against this background, the Heart to Heart Tea House offers a novel solution. It creates a relaxed, open, and non-judgmental space, using Heart to Heart cards to guide discussions. 35 This approach encourages participants to deeply explore ACP-related topics. During the activity, participants shared personal experiences and studied the concept of “good death,” expressed their ACP preferences, and enhanced their understanding of autonomy. This provides a practical reference model for advancing and implementing ACP education within palliative care in China.
Limitations
This study has several limitations. Firstly, the use of convenience sampling from five tertiary hospitals in Hangzhou limits the transferability of the findings to nursing interns in other regions or healthcare settings. Secondly, the predominantly female and Han Chinese sample may not fully represent the perspectives of male interns or those from diverse ethnic and cultural backgrounds. Additionally, as a qualitative study, these findings reflect the perspectives of these specific students and may not be representative of all nursing interns.
The facilitators’ presence during the Heart to Heart Tea House, although trained, may have influenced participants’ responses despite efforts to maintain a neutral and supportive environment. Finally, the self-reported nature of the data may be subject to social desirability bias, particularly regarding culturally sensitive topics such as death and familial obligations.
To enhance the rigor of the study, we adhered to a systematic approach for data collection and analysis. Despite this, the self-reported data poses a limitation. Confirmability was strengthened through iterative discussions and cross-checking during coding and thematic analysis by multiple researchers, which served to mitigate individual bias.
Conclusion
Based on nursing interns’ participation in the Heart to Heart Tea House, this study demonstrates that the activity can overcome cultural death taboos by creating a safe discussion space. Interns defined “good death” through three core priorities: effective symptom management, preserved autonomy in end-of-life decisions, and maintained dignity. Their views were distinctly shaped by Chinese familial values, emphasizing minimizing emotional/financial burdens on families and achieving emotional expression. The activity also prompted reflections on life’s meaning and death’s natural acceptance. These findings highlight critical implications for hospice care education in China: integrating practical ACP, family-centered communication strategies, and enhanced symptom management skills. This research provides an empirical foundation for the culturally nuanced “good death” concept among Chinese nursing trainees and a practical framework for optimizing palliative care education.
Footnotes
Acknowledgments
The authors gratefully acknowledge the financial support provided by the Zhejiang Provincial Education Department [grant numbers Y202454808]. The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author Contributions
Funding
The authors gratefully acknowledge the financial support provided by the Zhejiang Provincial Education Department [Grant Numbers Y202454808].
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.