
Abstract
Comfort care measures have become synonymous with end-of-life care. A previous study published in 2013 showed that there was little agreement on when or how comfort care measures should be initiated and what constituted comfort care measures. We conducted our own survey among doctors of various ranks and specialities in a local tertiary hospital to obtain a better understanding of their perception of comfort care. A total of 92 doctors responded. There was still lack of agreement on what comfort measures meant despite advances in palliative care. Our survey revealed that many doctors felt that initiation of comfort measures was not dependent on the patient’s prognosis. Many were also willing to offer treatment of infections and reversible conditions in patients on comfort measures. Views were split over the extent of oxygen support, nutrition and hydration, level of care facility, blood draws and opioid use in patients on comfort measures. Many doctors felt that do-not-resuscitate and comfort-measures-only orders were linked, and knowing that patients were on comfort measures and the reason for it were useful in management. A better approach when addressing plans for comfort measures would be to discuss the expected symptoms and its management, and tailor an individual care plan for each patient.
Introduction
Comfort care is usually offered as an alternative plan for patients whose response to definitive treatment of a life-limiting illness is anticipated to be poor, and are approaching the end of life. Occasionally, the ill patient may choose conservative treatment with no medical or surgical interventions, and a goal for comfort care. Comfort care as such refers to care that helps or soothes a person who is dying, to prevent or relieve suffering as much as possible, and to improve quality of life while respecting the dying person’s wishes. 1
Multiple distressing symptoms affect hospitalised patients who have advanced, life-threatening illnesses, and the meticulous management of these symptoms becomes the primary focus near the end of life. 2 A previous study by Zanartu et al in 2013 showed that there was little agreement among medical practitioners on what constituted comfort measures and when or how it should be initiated. 3 The study’s conclusion redefined what comfort measures should encompass – “the level of care offered to a patient when life expectancy is weeks to months or less, consisting of: oxygen per nasal cannula, oral nutrition and hydration as tolerated, no blood draws regardless of indication, no transfer to critical care unit, optional case-based antibiotics therapy, opioids for maximal symptom relief and ideally do-not-resuscitate/do-not-intubate.” 3
Nearly a decade later, we were unsure if there would be a better understanding of the definition of comfort care. The aim of this paper is to investigate if there is a consensus among doctors practising in a Singapore hospital on the timing and extent of care encompassed by comfort measures only (CMO), given the progress and advancement of palliative care in Singapore.
Methods
Our study was based on the original survey by Zanartu et al. 3 For our survey, the questions were adapted to the local context, with a total of 12 multiple choice questions, one of which allowed for multiple answers.
Our hospital in Singapore is a 1000-bed regional tertiary hospital consisting of 23 clinical services including medical, surgical and emergency disciplines. After receiving a waiver for ethical approval from the Institutional Review Board, a cover letter embedded with a QR code was emailed to 531 doctors of various ranks (interns, residents, fellows, attending physicians) and specialties, inviting them to participate in the survey. The cover letter explained the rationale and application of the survey and its outcome. The QR code provided a link to a secure online questionnaire hosted by our government agency. Publicity posters about the survey were placed in the hospital’s staff-only elevators as reminders. Email reminders were also sent to the doctors at 3-monthly intervals during the survey period. The duration of the survey period lasted one year from January 2022 to December 2022. Participation was voluntary and the responses were anonymised. Consent was implied when participants opted to complete the survey. The information from the survey was consolidated and analysed by the authors.
Results
Demographics of Respondents
A total of 531 doctors from the medical and surgical specialties received the invitation to complete the survey, out of whom 92 (17.3%) responded. Fifty-one of the respondents (55.4%) were Attending Physicians who were senior doctors, 15 (16.3%) were Fellows who were doctors in training to become Attending, and 26 (28.3%) were junior doctors (Residents and Interns). Out of the 92 respondents, 24 were from the Medical Department, 23 were from the Surgical Department, 15 were from the Emergency Department and the remaining were not specified (Figure 1). Demographics by rank/position.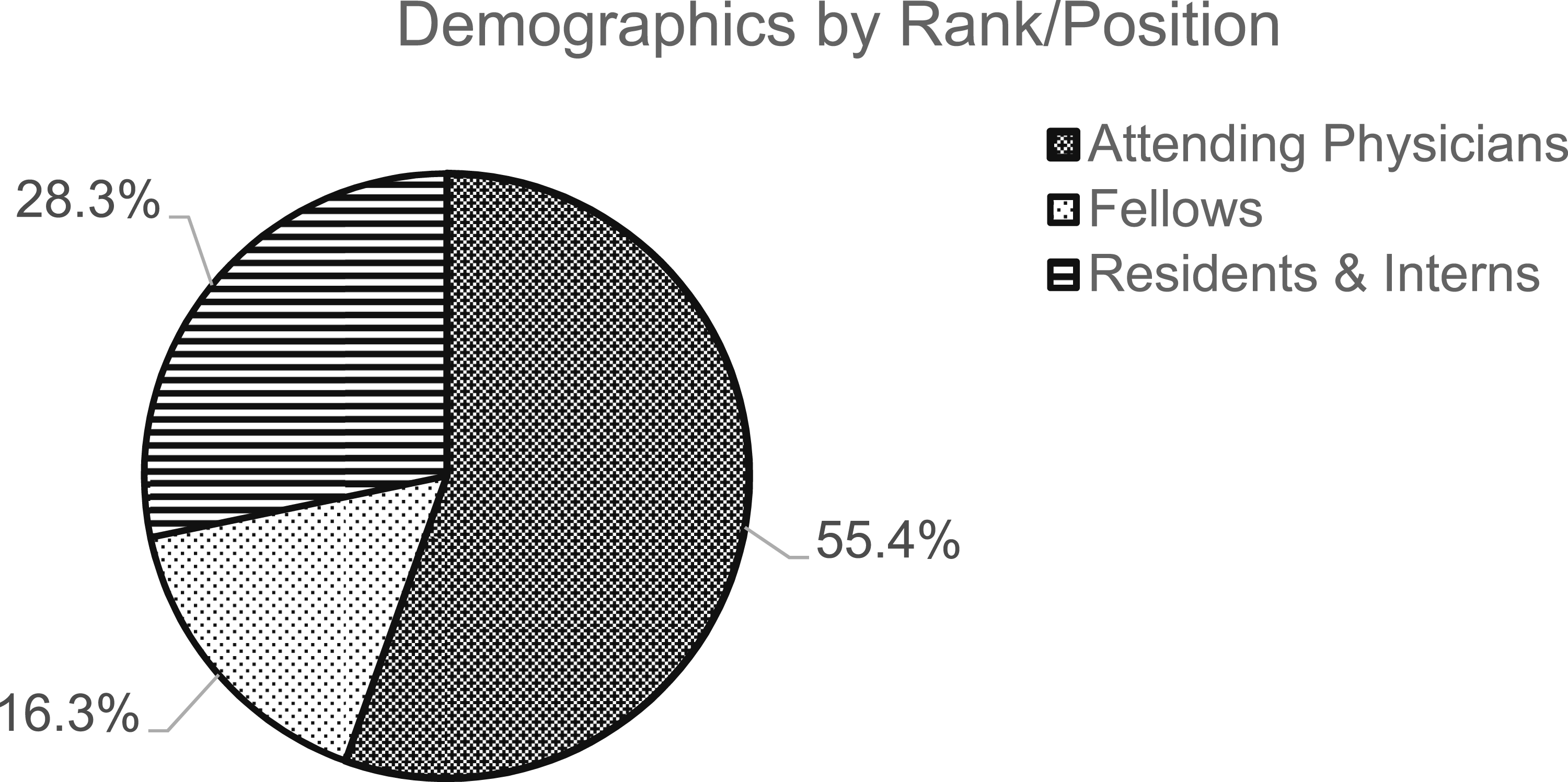
Timing of CMO Initiation
There was no agreement on the optimal time to initiate CMO. Out of the 59 (64.1%) doctors who would offer CMO based on prognosis, 15 (16.3%) would do so if the prognosis was in terms of weeks to months, as would 12 (13.0%) if the prognosis was hours to days. Thirty-two (34.8%) doctors would initiate CMO when the prognosis was days to weeks, but a similar number of 33 (35.9%) doctors felt that prognosis did not affect the decision to offer CMO.
Extent of Respiratory Support
Ninety respondents (97.8%) would offer oxygen therapy to various extent. Of these, 13 (14.1%) would give oxygen via nasal cannula, 12 (13.0%) via face mask, 54 (58.7%) via non-rebreather mask (which delivers 100% oxygen at 15 litres per minute), and 10 (10.9%) via non-invasive ventilation (NIV) such as continuous positive airway pressure (CPAP) or bilevel positive airway pressure (BiPAP). One (1.1%) respondent would offer mechanical ventilation via intubation, and 2 (2.0%) would not offer any supportive oxygen.
Extent of Nutrition and Hydration Support
Forty (43.5%) respondents were keen for oral intake as tolerated, while 17 (18.5%) would support intravenous fluid, and 32 (34.8%) would offer feeding via nasogastric tube (NGT) or gastroenterostomy (PEG) feeding. Total parenteral nutrition (TPN) would be supported by 3 (3.3%) respondents (Figure 2). Extent of nutrition and hydration support.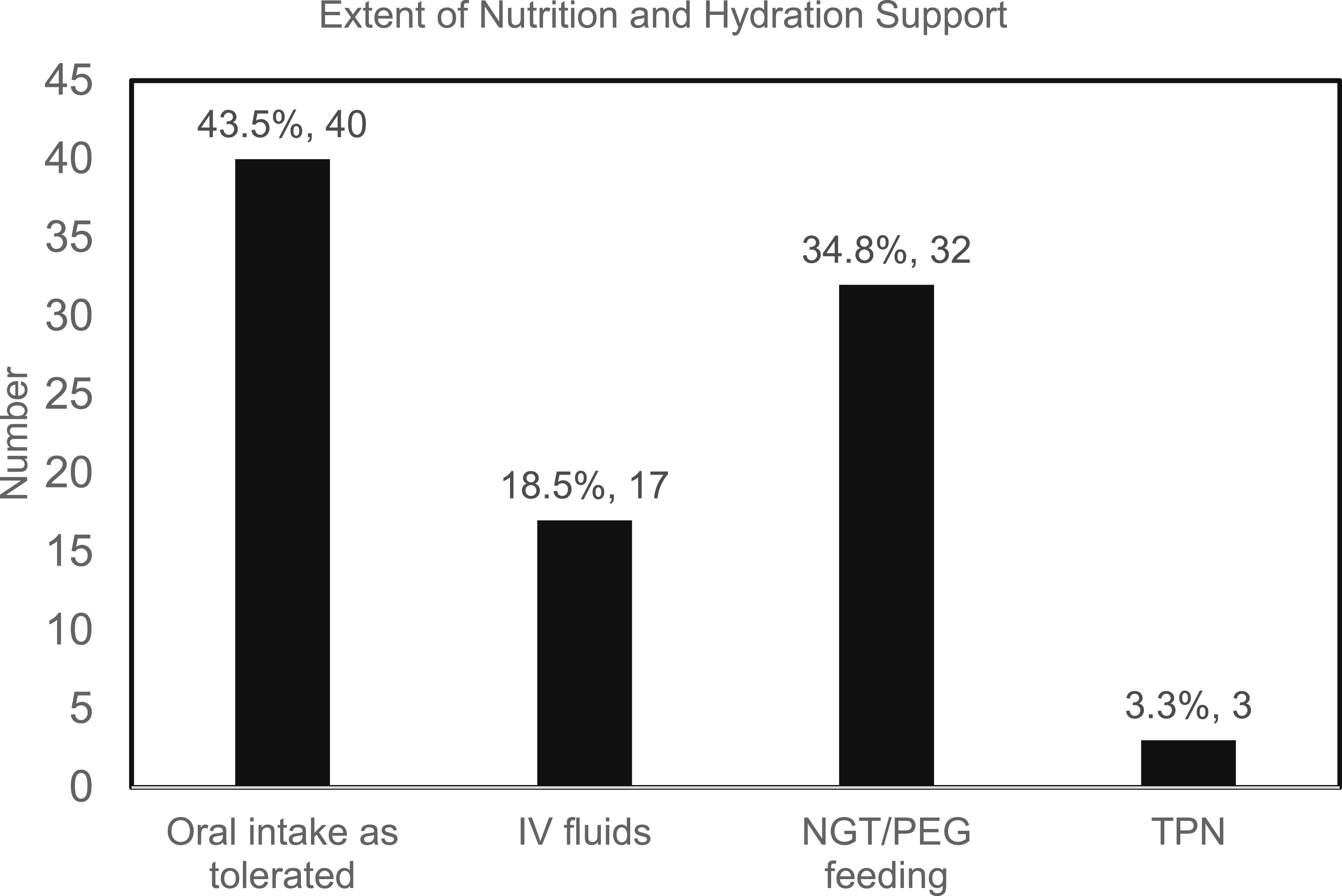
Blood Draws
For this survey question, respondents were allowed multiple responses pertaining to blood draws for a patient on CMO status. There was a total of 152 responses, out of which 32.2% felt blood investigations were not indicated if a patient was on a CMO order. Of the 63.1% who felt blood investigations should be offered, 19.7% would do so in the presence of fever or suspected sepsis, 23.0% in suspected severe electrolyte imbalance, 9.2% in suspected acute coronary syndrome, and 11.2% in suspected drug toxicity (11.2%). A small number, 4.6%, declined comment.
Antibiotic Use for Infection
Twenty nine (31.5%) of the respondents felt that only oral antibiotics should be started on patients on CMO status, and 33 (35.9%) would be offered antibiotics via oral or intravenous routes. Fifteen (16.3%) doctors would manage the CMO patient just like a non-CMO patient, and an equal number (15, 16.3%) would withhold antibiotics (Figure 3). Antibiotic use for infection.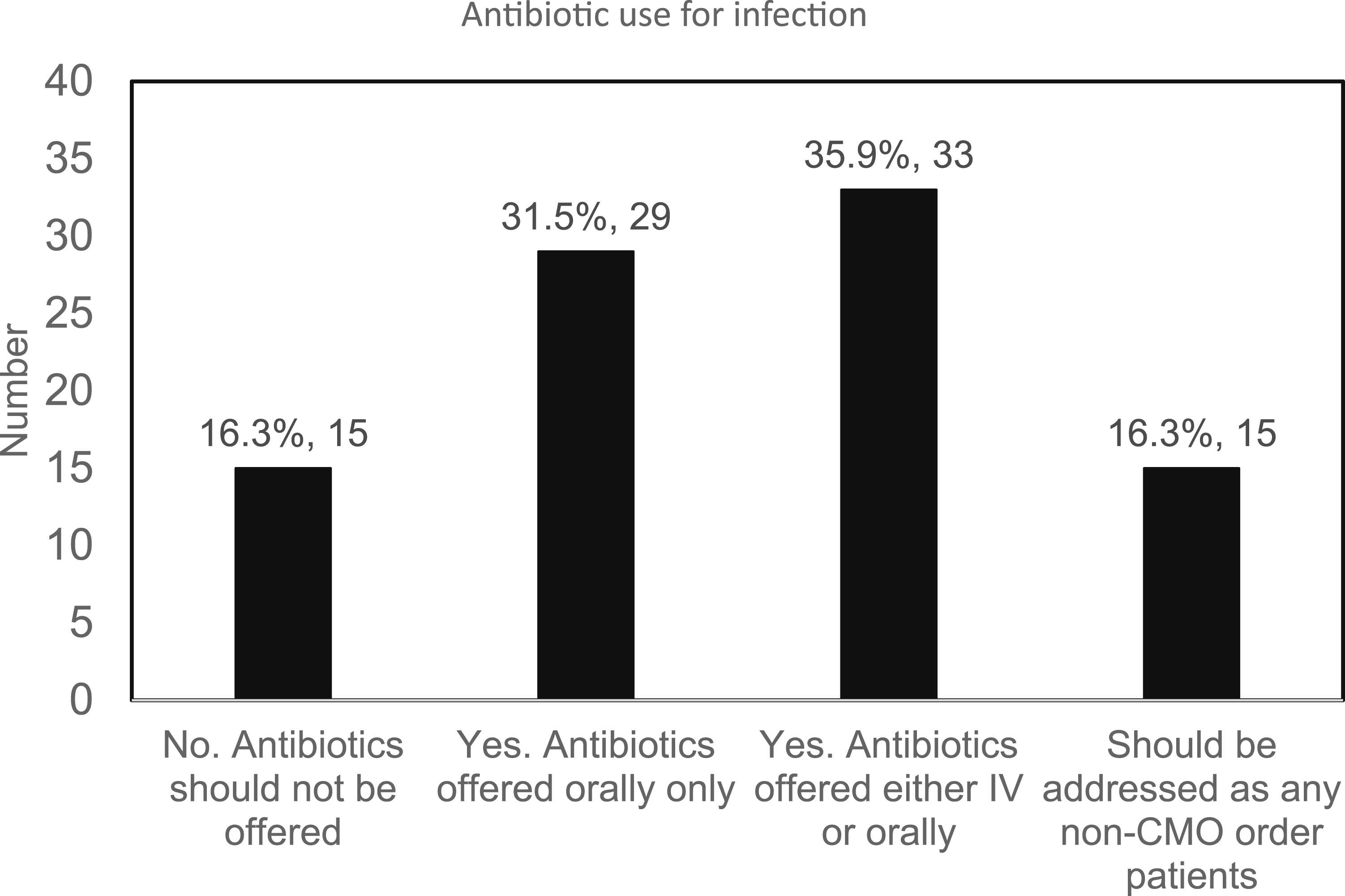
Opioid Use in CMO Patients
Forty four (47.8%) respondents felt that opioids should be used more aggressively if the patient was on CMO status, while 48 (52.2%) did not think opioid use should change despite the patient’s CMO order.
Treatment for Potentially Reversible Conditions
Fourteen (15.2%) respondents would not treat potentially reversible conditions, but would manage for symptoms only. Twenty five (27.2%) would offer a trial of oral medications, and 41 (44.6%) would escalate to invasive procedures to palliate symptoms. The remaining 12 (13.0%) felt there should be no difference in management regardless of their CMO status.
Level of Care in CMO Status
Although 61 (66.3%) respondents felt that patients on CMO status should not be transferred to wards with a higher level of care, the remaining 31 (33.7%) were willing to consider each patient’s siting of care on a case-by-case basis. With more granular questioning, 49 (53.3%) doctors felt that CMO patients should remain in the hospital general ward, 14 (15.2%) felt that patients could be transferred to the high dependency ward, and none felt that escalation to the intensive care unit (ICU) was appropriate. Twenty nine (31.5%) respondents were willing to consider the siting of each patient on a case-by-case basis.
CMO Status and DNR Status
Seventy three (79.3%) respondents felt there was a relationship between CMO status and “do-not-resuscitate (DNR)” status, out of whom 53 (57.6%) believed that a patient on CMO should have a concurrent DNR status, and 20 (21.7%) felt that a patient could not have a CMO order without being on DNR status. Nineteen (20.7%) respondents felt there both CMO and DNR were independent of each other.
Usefulness of CMO status
Eighty eight (95.7%) respondents thought that putting patients on CMO status was useful for patient management, while 4 (4.3%) felt otherwise.
Knowing the Reason for CMO Order
Forty seven (51.1%) respondents felt that knowing the reason for the CMO order would be useful in the management planning, and 42 (45.7%) believed that if the condition necessitating the CMO order had improved, the management goals should also change accordingly. Only 3 (3.3%) respondents did not think it would change management.
Discussion
In hospital settings, “comfort care”, “comfort measures” or “making [him/her] comfortable” have become synonymous with end-of-life care. 1 The term “comfort care” describes basic palliative care interventions that provide relief of symptoms to achieve comfort for a patient who is very close to death. Diagnostic or therapeutic manoeuvres that might be appropriate in earlier stages of the illness are usually not considered in this context, and comfort is a high priority with troubling symptoms expertly treated. 2
Our survey took the cue from Zanartu’s study, which associated comfort care with the care of a patient with life expectancy of less than weeks to months, using only oxygen per nasal cannula, oral nutrition and hydration as tolerated, optional case-based antibiotics therapy, opioids for maximal symptom relief, with no blood draws, intubation, resuscitation or transfer to a critical care unit. 3 Despite a lapse of nearly 10 years, ambiguity over what comfort care entailed continued to persist among clinicians as shown in our survey.
None of the respondents were trained in palliative and hospice care. The majority of the respondents in our study were senior clinicians, hence it was presumed that most of the respondents were clinically experienced, and understood what comfort measures were and the degree of intervention it involved. Nonetheless, our survey yielded interesting findings to the contrary.
In our survey, there was no consensus to the timing of CMO initiation, as previously validated by Zanartu. 3 This could stem from the lack of shared meaning for the label of CMO. 1 Our findings showed that almost two thirds of the respondents felt that prognosis played a role in the initiation of CMO, especially when the prognosis was in terms of days to weeks. For the one third who did not think that prognosis affected the decision for CMO initiation, we postulated that it could be because of the patient’s autonomy taking precedence – whereby the patient’s own preference for CMO overrode the issue of prognosis. This was in line with the recommendation that physicians base their decisions about therapeutic interventions and the type of care (including CMO) on the preferences and expectations of patients and their care givers. 4
Views were split over the extent of supplemental oxygen offered. Most of the respondents were keen to offer oxygen for patients on CMO, ranging from nasal cannula to face mask to non-rebreather mask, all of which were easily accessible in the hospital general ward. These methods of oxygen delivery were generally well-tolerated by most patients. Non-invasive ventilation such as CPAP and BiPAP were less favoured by the respondents, likely due to poor tolerability, the need for repeated investigations including blood draws, and more intensive monitoring outside of the hospital general ward. In a meta-analysis of NIV in patients with CMO orders, it was shown that the relief of dyspnea was only mild, and likely better achieved by palliative measures other than NIV, 5 which supports the survey findings.
Many respondents supported enteral nutrition over parenteral nutrition. Less than half of the respondents felt that “oral intake as tolerated” was more relevant to the goals of comfort measures. Although no significant literature backs up the idea of providing artificial nutrition and hydration to extend life, 3 one third of the doctors were keen to offer NGT or PEG feeding for maintaining nutritional and hydration status, and up to 20% were open to intravenous fluids or total parenteral nutrition in CMO patients. This could be attributed to the cultural beliefs of Singaporeans, most of whom have Asian roots which emphasise the importance of satiety, as demonstrated by the common salutation “have you eaten” in lieu of “hello”. 6 Singapore’s Advance Medical Directive (AMD) Act 2008 which allows individuals to refuse extraordinary life-sustaining treatment if they are terminally ill and unconscious, nonetheless calls for “reasonable provision of food and water” even at a terminal stage of illness. 7 The inference here is that feeding (per orally or tube-fed) is expected to be implemented by physicians even in the face of overwhelming scientific data to the contrary. 7 A study exploring the factors influencing Singapore Chinese caregivers to continue feeding at the end of life showed that feeding was a manifestation of filial piety (a cultural value that emphasises respect and care for one’s elders), source of hope, and expression of affection – views that were shared by both patients and caregivers. 8
The respondents were split in their decision for blood investigations in patients on CMO status – approximately half were ambivalent or did not support any blood draws, while the other half were keen for phlebotomy for various reasons. In a study done at an inpatient specialist palliative care unit, the top three reasons for venipuncture were to manage medications, establish the need for blood transfusion, and guide management of sepsis. The outcome was that 30% changed management, 40.7% ruled in an important diagnosis, and 86% ruled out an important diagnosis. 9 Although the palliative care setting is not synonymous to having a CMO status, it reflected the struggle faced by clinicians with the decision to conduct blood investigations, as was mirrored by our survey.
More than 80% of the respondents were keen to manage infections in patients on CMO in the same way as an infected non-CMO patient, or were willing to offer antibiotics for treatment of infection. Among these respondents, nearly half were keen for oral antibiotics only, and the other half were open to offer oral or intravenous options. In an audit carried out in a Singapore tertiary hospital, 44.9% of terminally ill patients in the hospital general ward received antibiotics in the last 24 h of life. 10 On the other hand, an audit on antibiotic use at the end of life in a Singapore inpatient hospice revealed that only 17.3% of patients were given antibiotics during their stay, with a very low use of antibiotics in the last 1 week of life (3.1%) and in the last 24 h (2.3%); indications for antibiotics were clear, and its use was rational and not excessive, and majority of patients showed symptomatic response. 11 Antibiotics use in end-of-life patients is controversial as clinical benefits have not been clearly established, thus international guidelines have recommended using the antibiotic stewardship program (ASP) in decisions involving the use of antibiotics for palliative care patients. 12 However it has been shown that the main reason for rejection of the ASP intervention, and hence antibiotic continuation, was due to the clinician’s personal preference. 12 A similar finding reported in a survey of Korean medical staff highlighted that physicians continued antibiotics as they were not confident in determining when the patient was facing imminent death, and preferred to continue antibiotics to avoid being perceived as “giving up”, 13 as was a similar survey done among American physicians. 14 Our survey done among tertiary hospital clinicians likely reflected the prevailing opinion that antibiotics should not be withheld in the background of inadequate outcome data.
Similar to the management of infections, more than 80% of the respondents were keen to treat potentially reversible conditions, probably on the premise that a patient who was responsive to treatment would have symptom improvement and life may be prolonged.
Despite the fact that half the respondents believed that opioid use should be similar to that of non-CMO patients, it was worrying that the other half felt that aggressive use of opioid was necessary. This finding unveiled a potential for inappropriate use of opioids, and it was shown in a study done on hospital-based palliative care providers, who opined that a continuous infusion of morphine should be the standard order set for those on CMO although the indications were absent. 15
Although more than half of the respondents felt that the level of care of the CMO patient should remain in the hospital general ward, nearly half would either escalate patients up to the high dependency ward (but not to ICU) or decide on a case-by-case basis, which seemed contradictory to the CMO order. Most of the respondents felt that CMO and DNR status were linked, but one fifth seemed to be in a dilemma in managing CMO and DNR in the same patient. Nonetheless the vast majority felt that having a CMO status and knowing the reason for it were useful, because it helped to align the goals of care and treatment plans.
Limitations
This survey has several limitations. A large proportion of the respondents were from unspecified specialties and subspecialties, such as General Medicine, Psychiatry, Rheumatology, Rehabilitation Medicine, Geriatric Medicine, Orthopaedics etc, hence their exposure to terminally ill patients were varied. The respondents were from a single tertiary hospital in Singapore, which may not be representative of other institutions locally, regionally or internationally. The response rate was less than 20%, hence there could be selection bias. The questions asked in the survey were non-specific and without contextual information, thus the survey responses may not reflect actual medical decision-making in individual patients.
Conclusion
There is still lack of agreement on what comfort measure entails despite advances in medical and palliative care more than 10 years after Zanartu’s initial survey. A better approach when addressing comfort care would be to involve the multidisciplinary team for discussion with the patient and loved ones about the expected symptoms and individualised management centred on patient preference, rather than instituting a blanket CMO order set. This could reduce the ambiguity of the timing of CMO initiation, and the type of treatment implemented. The busy clinician would then need to set aside time to holistically assess the patient’s values, beliefs and concerns, so that a unique plan encompassing physical, psychological and spiritual aspects can be tailored for the individual patient.
Footnotes
Acknowledgments
The authors sincerely thank all participants for participating in this study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.