
Abstract
Background
Emergency department (ED) presentations by patients with cancer are increasing globally. Policy frameworks often classify these as “potentially preventable emergency department visits” (PPEDVs) using administrative coding, yet the validity of this approach is contested. No qualitative systematic review of clinician perspectives on avoidable oncology ED use currently exists.
Objective
To synthesise multidisciplinary clinician perspectives on avoidable ED use in oncology and identify the barriers and facilitators that must be addressed to support alternatives to emergency attendance.
Methods
We searched CINAHL, PsycINFO, PubMed, and Scopus from inception to April 2026 for qualitative studies on clinician perceptions of avoidable oncology ED use. Data from 7 included studies (n = 180 clinicians) were synthesised using a three-stage thematic synthesis approach. Quality was assessed using the CASP Qualitative Checklist and GRADE-CERQual.
Results
Four analytical constructs were identified: (1) professional risk aversion under diagnostic uncertainty makes ED escalation a rational choice; (2) fractured communication across professional silos acts as a structural driver of attendance; (3) the ED serves as an organisational proxy for inaccessible 24/7 specialist care; and (4) clinicians contest policy-based definitions of “avoidability,” particularly at the end of life.
Conclusions
Avoidable ED use in oncology is primarily a product of system failures rather than clinical misuse. Reducing these visits requires concurrent investment in 24/7 specialist-led pathways, shared information infrastructure, anticipatory patient guidance, cross-specialty training, and accountable care coordination models.
Keywords
Introduction
Emergency department (ED) presentations by patients with cancer are increasing internationally, driven by rising cancer incidence, expanding outpatient systemic therapies, and persistent gaps in community oncology infrastructure.1,2 Patients present throughout the cancer trajectory with concerns spanning treatment toxicity, disease progression, and acute symptom crises. 3 This growing demand raises legitimate questions about the quality and appropriateness of care delivered in environments not designed for this population.
Health policy has responded by classifying a proportion of these visits as “potentially preventable emergency department visits” (PPEDVs). In the United States, the Centers for Medicare & Medicaid Services Oncology Patient Experience (CMS OP-35) measure operationalises this through predefined diagnosis codes applied retrospectively to discharge records. 4 However, the validity of this approach is increasingly contested. 5 Clinicians act prospectively under diagnostic uncertainty, often in a population where immunosuppression can transform an apparently minor symptom into a life-threatening emergency.3,5 What administrative algorithms label preventable, clinicians frequently experience as rational and necessary.
At the oncology-emergency interface, 2 distinct professional logics operate. Emergency medicine prioritises risk aversion and rapid stabilization, while oncology emphasises specialist-led continuity and structured outpatient management. 6 When these logics intersect, ED clinicians often lack pathways to oncology teams, training in treatment-related triage, and awareness of specialist alternatives within their own institutions.5,7 The result is that visits labelled “avoidable” by policy may be experienced as clinically rational by every professional involved.
A growing body of qualitative work is beginning to examine these questions,5–11 but no systematic review of clinician perspectives exists. This review synthesises the evidence to develop a thematic account of how avoidability is defined and contested across the acute oncology care interface, and to identify system barriers that must be addressed to support clinician-facing alternatives to emergency attendance.
Methods
This systematic review was registered with PROSPERO (CRD420261365992), an international register of systematic reviews which is recognised as a marker of methodological transparency and rigour, conducted and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. A completed PRISMA checklist is provided as a supplemental file. We searched CINAHL, PsycINFO, PubMed, and Scopus from inception to April 2026 using terms spanning cancer/oncology, emergency care, avoidability/preventability, and qualitative methods. Additional studies were identified via forward and backward citation searching and grey literature.
Inclusion criteria were: (1) primary qualitative or mixed-methods studies with extractable qualitative data; (2) participants comprising multidisciplinary healthcare professionals involved in the care of patients with acute complications of cancer or its treatment; and (3) studies available in English. Exclusion criteria were: (1) studies focusing solely on patient or caregiver perspectives; (2) studies lacking primary qualitative data; and (3) studies not available in English.
Title and abstract screening was performed independently by 2 reviewers (CC, EC), with discrepancies resolved through discussion. Full-text eligibility assessment followed the same process. Data extraction and thematic coding were conducted by the primary reviewer (CC) and reviewed by the second author (EC); interpretive disagreements were resolved by consensus.
Qualitative data were synthesised using the three-stage thematic synthesis approach of Thomas and Harden 12 : (1) line-by-line inductive coding of findings and participant quotes; (2) development of descriptive themes by grouping codes hierarchically; and (3) generation of analytical third-order constructs through interpretive comparison across studies. Risk of bias was assessed using the CASP Qualitative Checklist. 13 Confidence in each finding was evaluated using GRADE-CERQual. 14
Results
Search Results and Study Selection
Characteristics of Included Studies
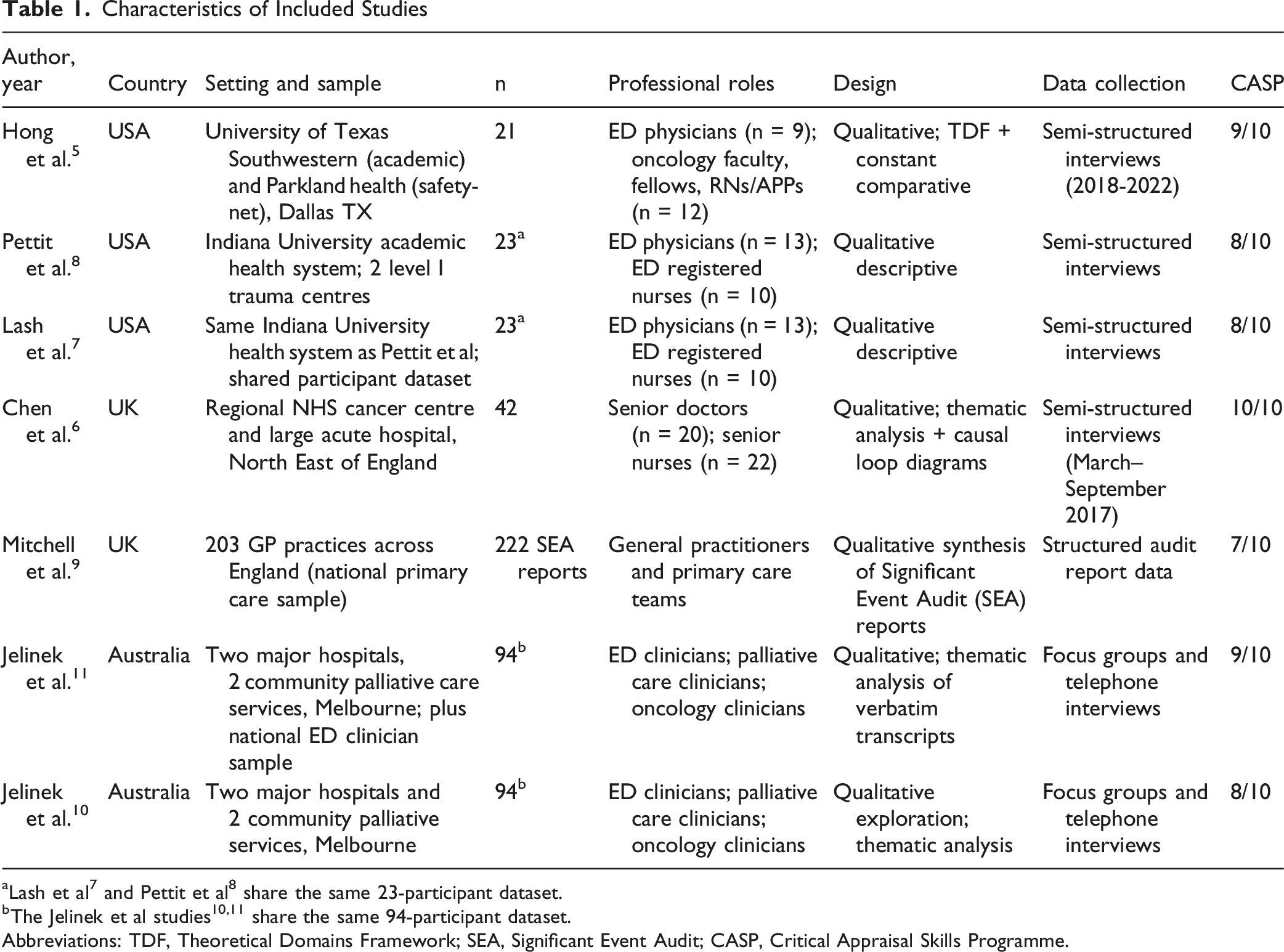
Abbreviations: TDF, Theoretical Domains Framework; SEA, Significant Event Audit; CASP, Critical Appraisal Skills Programme.
GRADE-CERQual Summary of Confidence in Analytical Constructs
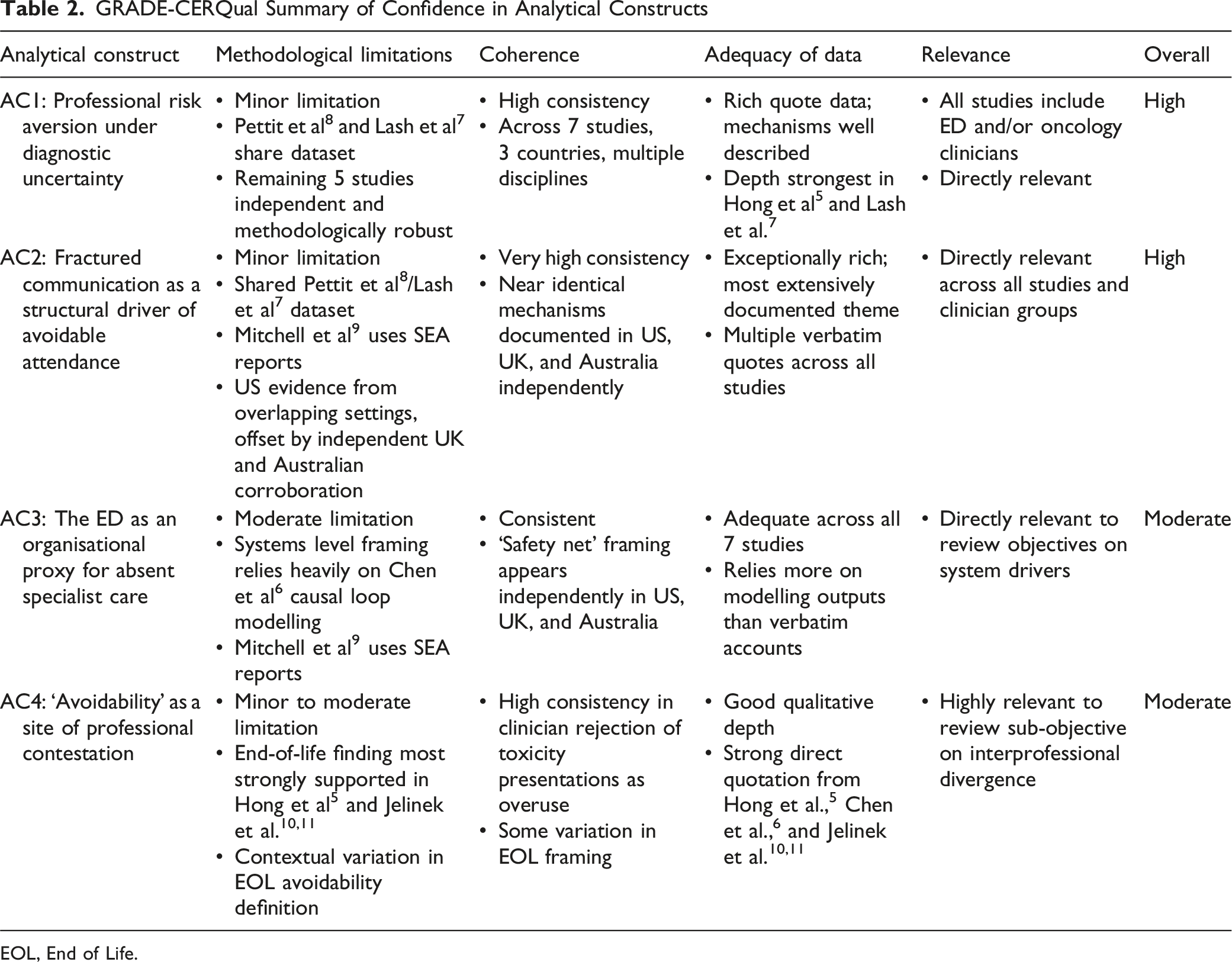
EOL, End of Life.
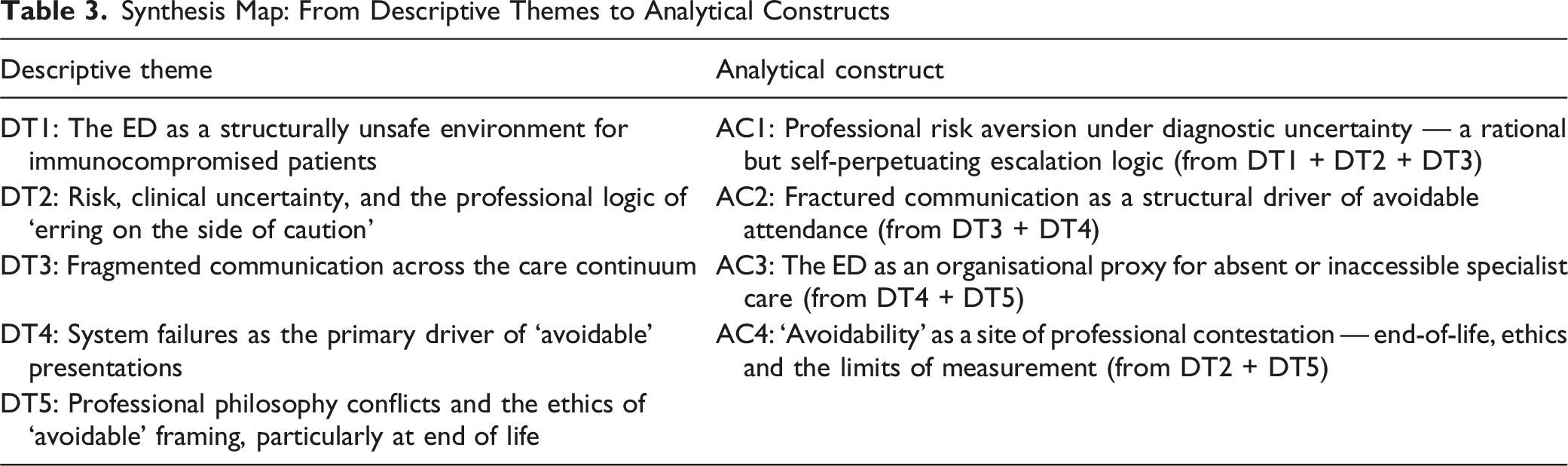
Synthesis Map: From Descriptive Themes to Analytical Constructs
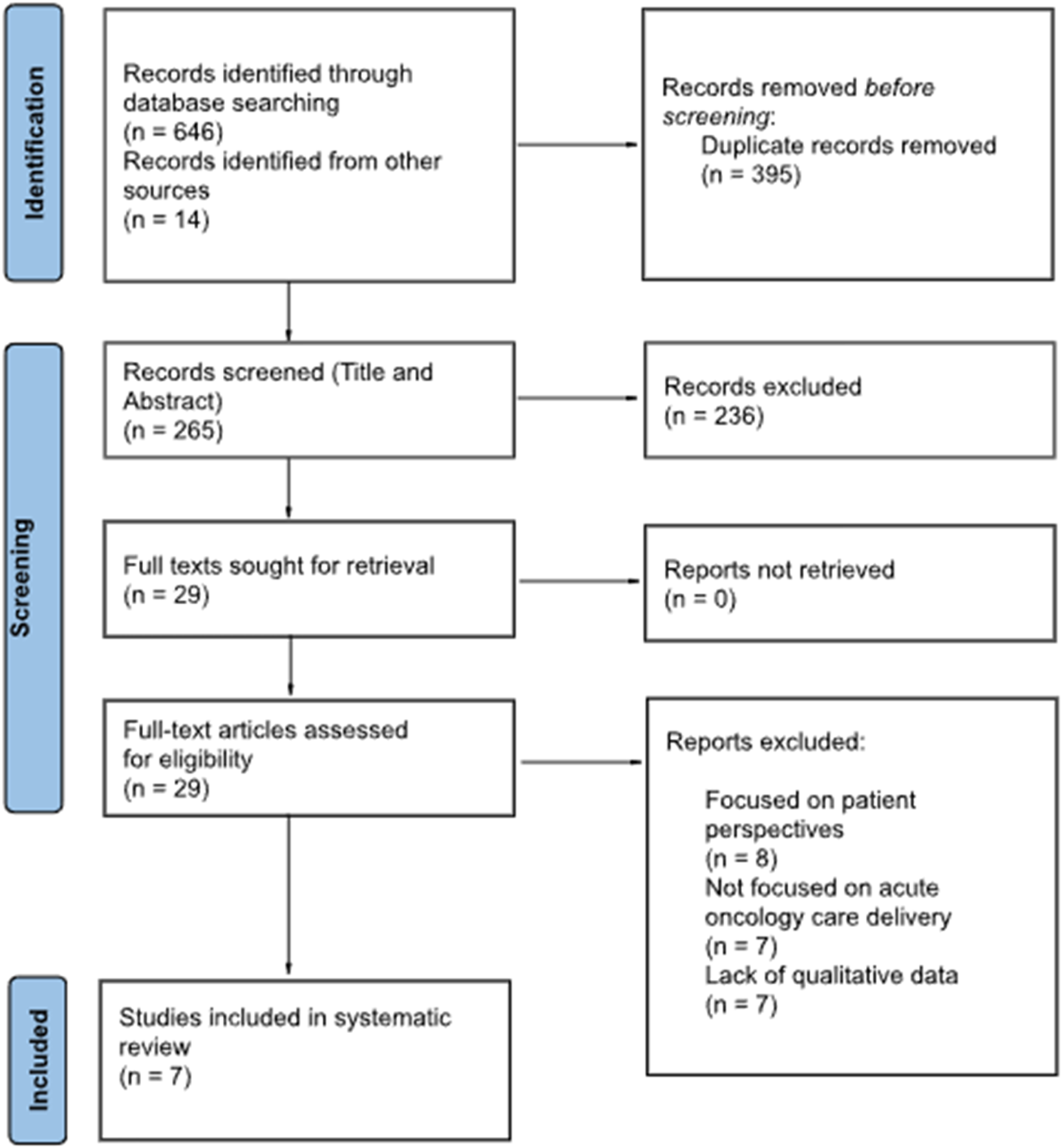
PRISMA flow diagram
Analytical Constructs
AC1: Professional Risk Aversion Under Diagnostic Uncertainty
Across multiple studies and settings, clinician decision-making at the acute oncology interface was dominated by fear of missing a diagnosis, particularly in the context of treatment-related immunosuppression. ED physicians described a risk stratification process in which the presence of cancer, rather than the presenting symptom, elevated perceived acuity. One participant in Hong et al 5 described this as clinical gestalt: “Sometimes you can just walk into the room and go, ‘There’s no way this person’s going home.’” Fear of liability further lowered the threshold for admission: “Almost any patient I send home, [I] always worry.” 5
Lash et al 7 documented ‘diagnostic expansion,’ in which a symptom that would be low-acuity in the general population becomes high-acuity in the context of cancer, with clinicians describing patients routinely receiving full work-ups for minor complaints. Jelinek et al 10 added an end-of-life dimension, finding that ED training and institutional culture created a strong bias toward action that persisted even when palliation was the appropriate response: “We tend to be very keen on making diagnoses. We tend to be terrified about missing diagnoses.” 10
Critically, this pattern reflects structurally compelled caution rather than individual anxiety: clinicians escalate because the outpatient alternatives that would make conservative management safe are simply not available.
AC2: Fractured Communication as a Structural Driver of Avoidable Attendance
Communication failure was the most extensively documented finding, identified in all 7 included studies and spanning 3 relational interfaces: between ED and oncology teams; between oncology teams and their patients; and between ED clinicians and patients.
In Lash et al, 7 17 of 23 participants described poor communication with outpatient oncology teams as a primary challenge. ED clinicians described difficulty reaching oncologists, who were frequently unavailable or reluctant to engage with acute problems. A striking example: an oncologist responding to an ED consultation by asking “Well, why are you calling me? I’m not going to do anything acutely”. 7 Hong et al 5 found that ED physicians were often unaware of oncology urgent care clinics within their own health system, meaning that even when alternatives existed, informational barriers prevented their use.
Oncology-to-patient communication failures were equally significant. Seven participants in Lash et al 7 described patients arriving at the ED unable to reach their oncology team, not knowing what else to do. Pettit et al 8 documented patients presenting because they lacked basic supplies such as antiemetics: “[The patient] didn’t have Zofran® at home… and the only thing they knew what to do is come to the emergency department”. 8 These presentations reflect failures of anticipatory communication in outpatient oncology settings rather than failures of clinical acuity.
AC3: The ED as an Organisational Proxy for Absent Specialist Care
Across all 7 studies, clinicians identified system-level failures as the dominant explanation for presentations labelled avoidable. The 24/7 availability of the ED, contrasted with restricted hours of specialist oncology services, was consistently identified as a structural driver. Jelinek et al 10 characterised patients as falling “into a void between a community service and a hospital that did not want them,” with the ED becoming the only available option.
Pettit et al 8 documented the patient-level internalisation of this dynamic: patients choosing the ED because they felt they would be a nuisance to contact their oncologist directly. One participant reported a patient stating: “I don’t want to bug them, they’re busy. I’m just going to go to the ER and get this taken care of”. 8 This is not overuse; it is the predictable behaviour of patients navigating a care environment in which the ED is the most dependable option available.
Chen et al 6 documented that a significant proportion of acute oncology admissions in the NHS were attributable not to clinical deterioration but to the absence of adequate home and community support. Financial barriers, work schedule conflicts, and limited social support further shaped care-seeking in ways entirely invisible to diagnosis-code-based preventability measures. 8
AC4: ‘Avoidability’ as a Site of Professional Contestation
This review reveals an epistemological mismatch between how policy frameworks operationalise avoidable ED use and how clinicians construct it at the bedside. Policy measures such as CMS OP-35 assign avoidability through discharge diagnosis codes, treating presenting complaints such as pain, nausea, and fever as inherently manageable outside the ED. Clinicians across multiple studies reject this framework.
ED physicians in Hong et al 5 did not view chemotherapy toxicity presentations as overuse: “Overuse? I don’t think so. Most of the time, when they’re there, they’ve got something going on”. 5 Instead, clinicians defined avoidability specifically in relation to end-of-life presentations where hospital care was unlikely to provide meaningful benefit. This clinician-defined conception maps directly onto the palliative care literature’s framework of value-concordant care. 15
The Jelinek studies10,11 and Chen et al 6 document a consistent dynamic: the failure to initiate advance care planning early in the disease trajectory, combined with a cultural ‘fight at all costs’ orientation within oncology, produces end-of-life ED presentations that clinicians across all 3 specialties understand as avoidable through earlier palliative engagement, not through administrative coding. Notably, Jelinek et al 10 offered an important counter-narrative: several participants described delivering compassionate end-of-life care in the ED as a source of professional satisfaction, resisting a simple framing of the ED as an inherently inappropriate setting.
Discussion
This qualitative systematic review, drawing on 180 clinician participants from 7 studies across 3 health systems, converges on a consistent finding: ED presentations by patients with cancer are not primarily a product of patient misuse or clinical overuse, but of system failures that make the ED the only reliably available option when specialist care is inaccessible, communication is fragmented, and community support is insufficient.
The evidence challenges the validity of administrative preventability measures such as CMS OP-35. CMS OP-35 was developed to provide a scalable, nationally standardised accountability measure for hospital outpatient quality which is a legitimate administrative purpose that diagnosis-code approaches are well suited to serve at population level. Its limitations emerge at the clinical interface where the retrospective application of diagnosis codes cannot account for the uncertainty under which clinicians act. Clinicians do not regard chemotherapy toxicity presentations as overuse; they identify end-of-life presentations where hospital care provides no meaningful benefit as the true site of avoidability - a distinction that current coding-based measures cannot capture. Holding health systems accountable for PPEDV rates without investing in the upstream conditions that would make avoidance genuinely feasible risks misattributing responsibility to frontline clinicians and patients navigating the consequences of system failures they did not create. We recommend that CMS OP-35 be revised to incorporate clinician-defined avoidability criteria, particularly at the end of life, and supplemented with prospective clinical audit data rather than relying solely on retrospective discharge coding. Administrative measures of this kind are most useful as population-level screening tools; they should not be used as the primary basis for institutional accountability without validation against clinician and patient-defined outcomes.
Risk-averse escalation, the most prominent individual-level driver identified in this review, is better understood as structurally compelled caution than as defensive medicine in the conventional liability-focused sense. Clinicians escalate because the specialist support and safe community alternatives that would enable conservative management are not reliably available. This has direct implications for intervention design: creating urgent care alternatives does not automatically recalibrate escalation behaviour if clinicians remain uncertain about their reliability and accessibility - a finding documented explicitly by Hong et al 5 who found that ED physicians were largely unaware of oncology urgent care services within their own health system.
Communication failure, the most extensively evidenced finding across all 7 studies, represents a structural configuration of cancer care organisation across professional and institutional boundaries, not simply a quality deficit in individual encounters. Oncology teams fail to prepare patients for predictable symptom trajectories; ED clinicians cannot reliably access real-time specialist advice; and the absence of shared records means goals-of-care decisions are initiated for the first time in the least appropriate environment. Each failure independently generates avoidable attendance; together they constitute a system in which avoidance is structurally precluded at every interface.
Service Implications
The analytical constructs developed in this review converge on 6 areas requiring concurrent investment. First, specialist-led acute oncology capacity outside the ED and outside standard outpatient hours, including 24/7 triage lines and rapid-access assessment clinics, is the most consistently identified requirement.7,8 Service creation and service integration are not the same problem; the latter is the harder and more important one. 5 Second, a shared information architecture accessible at the point of emergency presentation - including treatment summaries, advance care plans, and flagged high-risk patient lists with pre-established management plans - is a practical interim measure while full electronic record integration is achieved.5–7,11 Third, structured anticipatory guidance for patients at the point of treatment initiation is a low-cost intervention that addresses a correctable upstream gap.7,8 Fourth, cross-specialty training deficits require deliberate curricular intervention: ED clinicians lack training in oncology-specific risks; oncology trainees receive no formal preparation for acute triage; and both groups lack confidence in palliative communication.5,10,11 Fifth, designated clinical accountability for cancer patients in transit between settings, operationalised through oncology medical home models, has shown promise in reducing ED utilisation by eliminating the jurisdictional void in which neither ED nor oncology claims responsibility. 16 Sixth, the findings of this review have direct implications for palliative care integration across the acute oncology pathway. Early goals of care discussions, initiated at the point of diagnosis or treatment commencement rather than at crisis, represent a low-cost upstream intervention with consistent support across the included studies. This could be rectified through hybrid palliative models, evidenced by the Jelinek studies10,11 and Hong et al 5 study, in which specialist palliative input is embedded within oncology outpatient settings rather than confined to inpatient or hospice contexts to address the jurisdictional gap that drives end-of-life ED presentations. Community-based symptom control programmes, providing nurse-led or pharmacist-supported management of predictable treatment toxicities in the home setting, represent a further alternative to ED attendance that evidence supports but existing service configurations rarely provide. These approaches are not supplementary to the 5 service priorities identified above; they are the mechanism through which anticipatory guidance, cross-specialty training and accountable care coordination are operationalised at the patient level.
Limitations
The evidence base comprises 7 studies yielding 180 independent clinician participants. The geographic distribution is concentrated in 3 high-income, English-speaking health systems, limiting transferability to low- and middle-income settings. General practitioner and community-based clinician perspectives are substantially underrepresented, likely underweighting the primary care contribution to avoidable escalation. Mitchell et al 9 contributes data from Significant Event Audit reports rather than primary interview transcripts, constraining the depth of participant voice. Publication bias may amplify the universality of the system-failure narrative. As a qualitative synthesis, this review generates explanatory insights rather than quantifiable estimates and should be read alongside quantitative evidence on the prevalence and distribution of oncology ED use.
The 2 instances of shared participant datasets, Pettit et al 8 and Lash et al 7 drawing on the same 23 participants and Jelinek et al10,11 drawing on the same 94 participants, mean that findings from these studies cannot be treated as independent corroboration. This is acknowledged in the GRADE-CERQual ratings for AC1 and AC2, where shared datasets contributed to minor methodological limitation gradings. The analytical constructs are nonetheless supported by convergent evidence from the remaining independent studies across 3 health systems.
Mitchell et al 9 differs from the remaining 6 studies in 2 respects: it draws on primary care rather than acute/emergency settings, and it uses Significant Event Audit reports rather than primary interview transcripts. These distinctions are acknowledged in its CASP score (7/10) and in the GRADE-CERQual ratings for AC2 and AC3, where its methodological contribution is weighted accordingly. Its inclusion reflects a decision to capture the full multidisciplinary pathway through which avoidable escalation occurs; general practitioners are often the clinicians whose community management decisions determine whether an ED presentation takes place and their perspectives are systematically absent from acute-setting research. Excluding this qualitative data would render the synthesis blind to this upstream decision point.
As a two-author review, the possibility of interpretive bias cannot be excluded; the authors’ clinical backgrounds may have oriented the synthesis toward system-level explanations over individual clinician factors.17,18
Conclusion
This qualitative systematic review demonstrates that avoidable ED use in oncology is a product of system failures rather than individual misuse. Clinicians experience risk-averse escalation, fractured communication, and absent specialist alternatives as structural conditions that make ED attendance the rational choice. They define avoidability not by administrative diagnosis codes but by whether hospital care can provide meaningful clinical benefit - a definition particularly important at the end of life. Reducing avoidable oncology ED visits requires concurrent investment in 24/7 specialist pathways, shared information infrastructure, anticipatory patient guidance, cross-specialty training, and accountable care models. Future qualitative research should prioritise general practitioner and community clinician perspectives, low- and middle-income health system contexts, and the experiences of clinicians working within recently established acute oncology service models.
Supplemental Material
Supplemental Material - What Makes an Emergency Visit ‘Avoidable’? A Qualitative Systematic Review of Multidisciplinary Clinician Perspectives on Acute Oncology Care Delivery
Supplemental Material for What Makes an Emergency Visit ‘Avoidable’? A Qualitative Systematic Review of Multidisciplinary Clinician Perspectives on Acute Oncology Care Delivery by Calum Connolly and Euan Connolly in American Journal of Hospice and Palliative Medicine®
Supplemental Material
Supplemental Material - What Makes an Emergency Visit ‘Avoidable’? A Qualitative Systematic Review of Multidisciplinary Clinician Perspectives on Acute Oncology Care Delivery
Supplemental Material for What Makes an Emergency Visit ‘Avoidable’? A Qualitative Systematic Review of Multidisciplinary Clinician Perspectives on Acute Oncology Care Delivery by Calum Connolly and Euan Connolly in American Journal of Hospice and Palliative Medicine®
Footnotes
Acknowledgments
The authors received no writing or editing assistance from any third party in the preparation of this manuscript.
Ethical Considerations
This study is a qualitative systematic review based on previously published studies. It did not involve the direct participation of human subjects or the collection of new data. Ethics approval was not required.
Consent for Publication
All authors have given consent for the manuscript to be submitted in its current form.
Author Contributions
CC: Conceptualisation, Methodology, Data Curation, Formal Analysis, Writing – Original Draft, Writing – Review and Editing. EC: Methodology, Data Curation, Formal Analysis, Writing – Review and Editing. All authors approved the final version for submission.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
This is a qualitative systematic review of previously published studies. No new primary data were collected. All data are derived from the included studies, which are fully cited in the reference list. The PROSPERO registration (CRD420261365992) is publicly accessible.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.