
Abstract
Background
Gynecological cancers are among the leading causes of cancer-related deaths, which makes it important to focus on the end-of-life (EOL) quality and its improvement among gynecological cancer patients. Several indirect indicators have been developed to assess poor EOL quality among gynecological cancer patients, and these indicators can be used to assess EOL quality across different settings.
Objectives
(1) To assess the EOL quality and its improvement; and (2) to assess the EOL care and its changes among gynecological cancer patients at Oulu University Hospital by quality care measures.
Design
We conducted a retrospective study, comparing 2 cohorts. Patient data were obtained from the records of Oulu University Hospital.
Setting/Subjects
We compared 2 cohorts of gynecological cancer patients who died between 1.1.2018 and 30.6.2020 (Cohort 1) and between 1.1.2021 and 30.6.2023 (Cohort 2).
Results
In the latter cohort (Cohort 2), more patients were referred to palliative care (81% vs 94%, respectively). Additionally, there was a significant decrease in the proportion of patients receiving chemotherapy during the last 3 months of life in Cohort 2 (44% vs 25%). The time between the EOL discussion and death was longer in Cohort 2 (median 57 vs 125 days, respectively).
Conclusion
Based on these indicators, the EOL quality of patients with gynecological cancer at Oulu University Hospital may have improved in recent years. However, there remains room for improvement, particularly in the earlier initiation of palliative care.
Keywords
Background
Combined, ovarian, peritoneal, and fallopian tube cancers represent the 10th most common cancer and the fifth leading cause of cancer-related death among Finnish women. Thus, ovarian cancer has a higher mortality rate relative to its incidence compared with many other cancers. The golden standard treatment of ovarian cancer is cytoreductive surgery and chemotherapy. Although most ovarian cancer cases respond well to chemotherapy at first, many of the cases relapse later. After recurrence, disease progression occurs at shorter intervals in the natural history of the disease. 5-year survival for ovarian cancer patients is under 30%. 1 Endometrial cancer is the most common gynecological cancer, with approximately 900 new cases diagnosed each year in Finland. However, the number of deaths is relatively low, at about 200 per year. 2 The 5-year relative survival rate for endometrial carcinoma during 2000-2007 was 83.2% in Northern Europe. Treatment options for endometrial cancer include surgery, radiation therapy, chemotherapy and immunotherapy. 3
Several indirect indicators have been developed to assess poor-quality end-of-life (EOL) care for cancer patients. One of the indicators is the initiation of new anticancer therapies or the continuation of ongoing treatments close to death. Additionally, frequent emergency room visits, hospital admissions, or prolonged stays in intensive care units near death indicate poorer EOL care. Other indicators of poor-quality EOL care are first enrollment in hospice only during the last few days of life and dying in an acute-care setting. 4 Additionally, administration of chemotherapy close to death may lead to unnecessary patient suffering and increased societal costs. Furthermore, early referral to palliative care has been associated with a reduced risk of receiving chemotherapy in the last 30 days of life. 5 Palliative care can be defined as services that offer the patient and their family medical, emotional and spiritual care near the end-of-life. 6 Additionally, EOL discussions at least 30 days before death have been associated with a lower incidence of chemotherapy, hospitalization, intensive care unit admissions, and dying in an acute care setting. 7 As gynecological cancers, especially ovarian cancer, are among the most common causes of cancer-related death, it’s very important to focus on the quality of life in EOL care for gynecological patients. Previous research has shown that chemotherapy late in life, delayed referrals to palliative care, and late EOL discussions can harm the quality of life in women with gynecological cancer during their final stages.
Our study aims to examine, using quality-of-care measures, how EOL care influences the quality of life of women with gynecological cancer, and to assess whether patterns of palliative and EOL care have changed in recent years at Oulu University Hospital.
Methods
STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines for cohort studies were followed (Supplement Table 1).
Patients’ data were collected from Oulu University Hospital records. We searched from the database for patients who had an International Classification of Diseases, 10th revision (ICD-10) diagnosis code of ovarian cancer (C56.71, C56.79, C56.74, C56.72, C56.98, C56.00), fallopian tube cancer (C57.0), peritoneal cancer (C48.89, C48.19, C48.80), endometrial cancer (C54.11, C54.14, C54.19, C54.23, C54.13, C54.29), or malignant neoplasm of overlapping sites of female genital organs (C57.8), and died between 1.1.2018 - 30.6.2020 (cohort 1) or 1.1.2021 - 30.6.2023 (cohort 2).
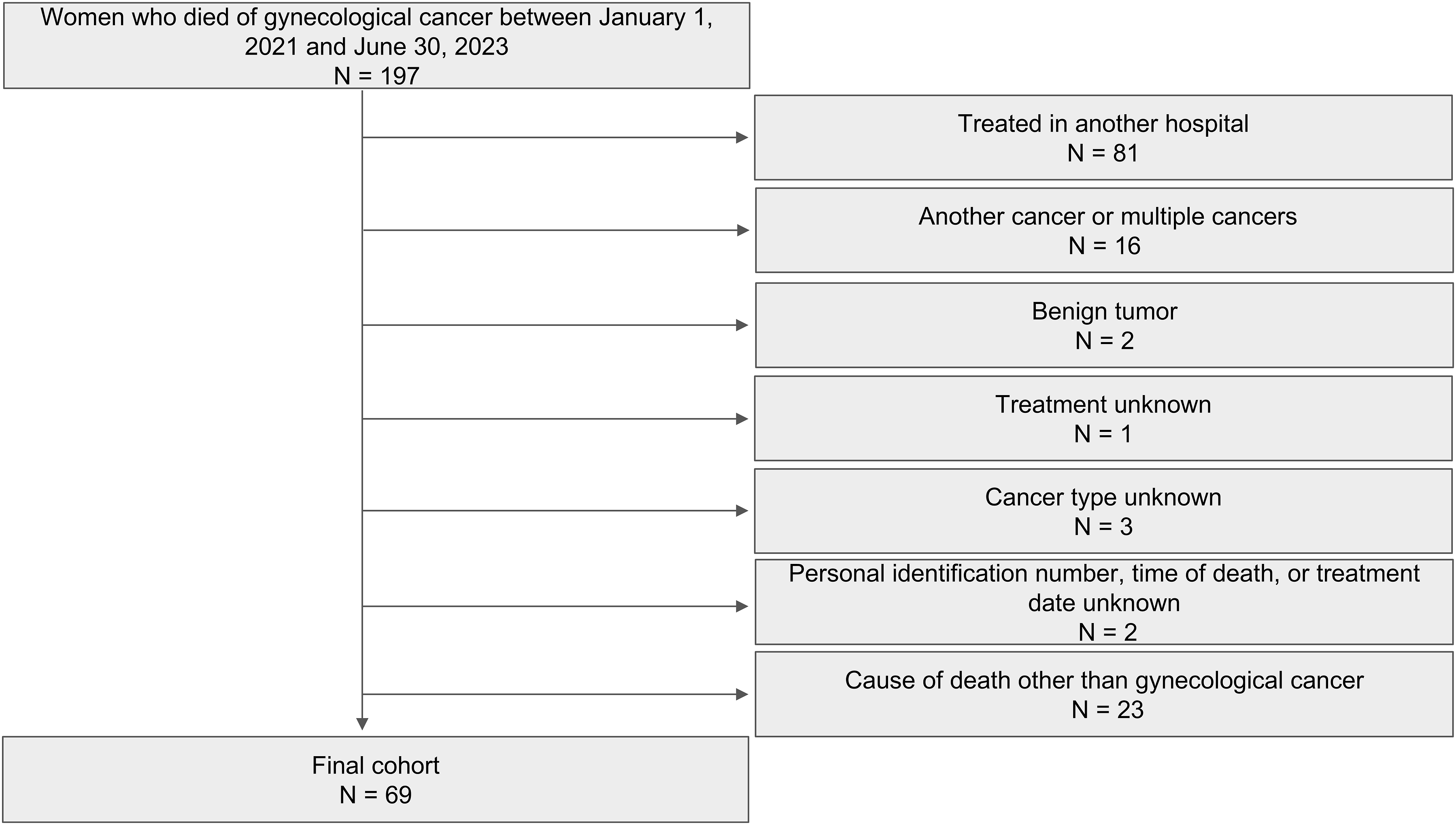
Exclusion criteria included treatment in another hospital; cancer other than gynecological cancer or multiple cancers; benign tumor; unknown treatment; unknown cancer origin; unknown personal identification number, time of death, or treatment date; or cause of death other than gynecological cancer.
The following information was extracted from the patient data: cancer type, cancer histology, cancer grade, ICD-10 code, date of diagnosis, time of death, cause of death, FIGO stage, central hospital, age at diagnosis, initial treatment, last initial treatment day, status after first line treatment, date of relapses, relapse treatments, status after relapses, number of previous chemotherapy lines, date of last chemotherapy, date of Do-Not-Resuscitate (DNR) order, whether the patient received palliative care, the initiation date of palliative care, whether an EOL discussion was held with the patient, date of EOL discussion, the date of last visit to the gynecology ward, received therapies in the last 3 months of life, the last therapy received during the last 3 months of life, date of last medical procedure in the last 6 months of life, admission date of the patient’s final gynecology ward stay and location of death.
Data Analysis
The data was analyzed by R version 4.3.2. For categorical variables, P values were calculated using the chi-squared test or the Fisher’s exact test if the assumptions for chi-squared test were not satisfied. For numerical variables, means and standard deviations were calculated for variables with a symmetrical distribution and their P values were calculated using the Student’s t-test. For numerical variables with a skewed distribution, medians and quartiles were calculated, and their P values were calculated using the Mann-Whitney U test.
Results
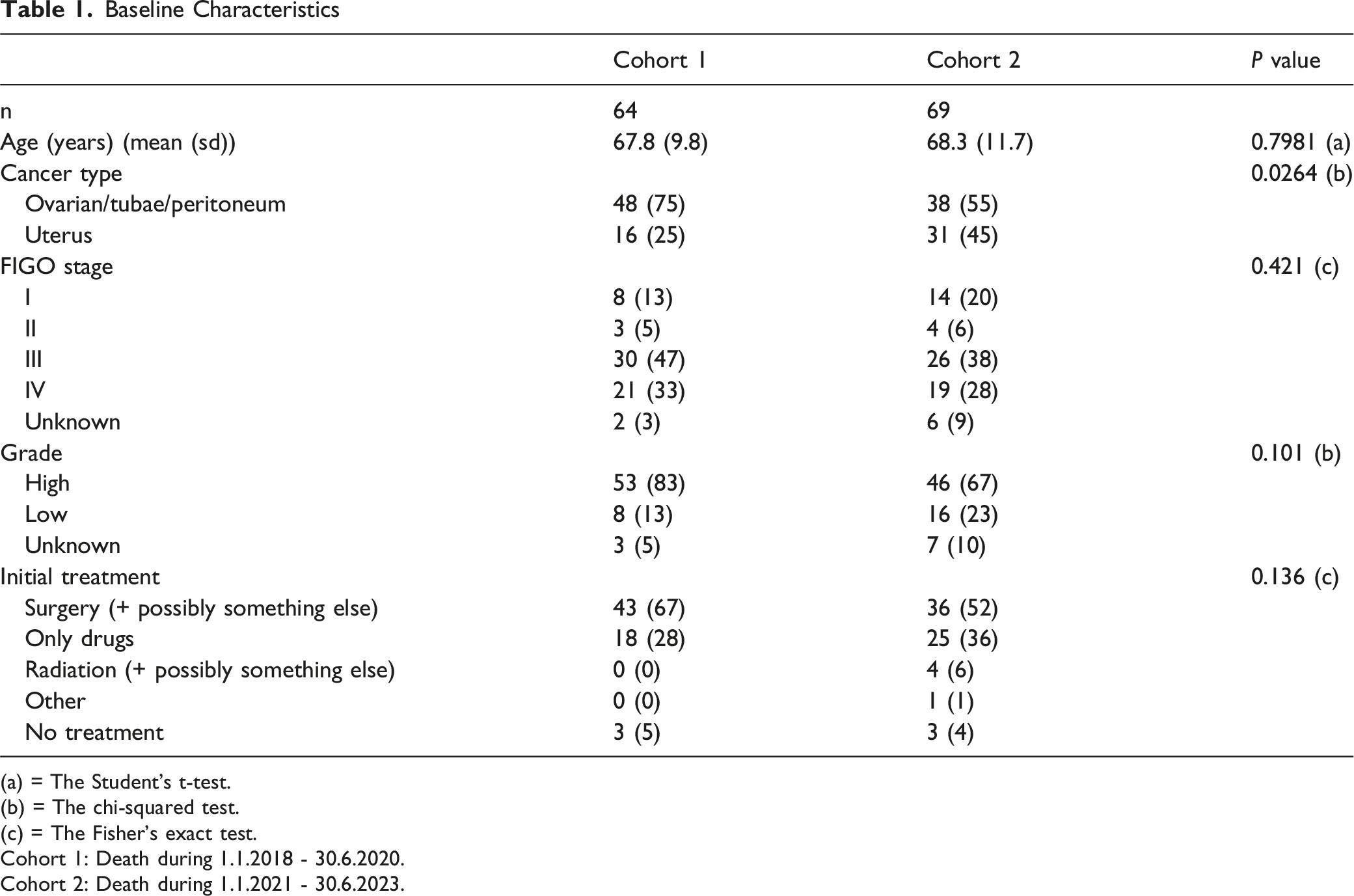
There were altogether 64 patients in cohort 1 (Figure 1) and 69 patients in cohort 2 (Figure 2). In both cohorts, most patients were ovarian cancer patients (75 % and 55 %, respectively), while overall, more ovarian cancer patients were in the earlier cohort (Cohort (1) and more endometrial cancer patients were in the latter cohort (Cohort (2) (Table 1). The distributions of age, cancer grade, stage, and histology were similar in both cohorts (Table 1, Supplement Table 2). Cancer treatment from first-line therapy to treatment of the fifth relapse was similar in both cohorts, with the only difference being the management of the fourth relapse (Supplement Table 2). Flowchart of cohort 1 Flowchart of cohort 2 Baseline Characteristics (a) = The Student's t-test. (b) = The chi-squared test. (c) = The Fisher’s exact test. Cohort 1: Death during 1.1.2018 - 30.6.2020. Cohort 2: Death during 1.1.2021 - 30.6.2023.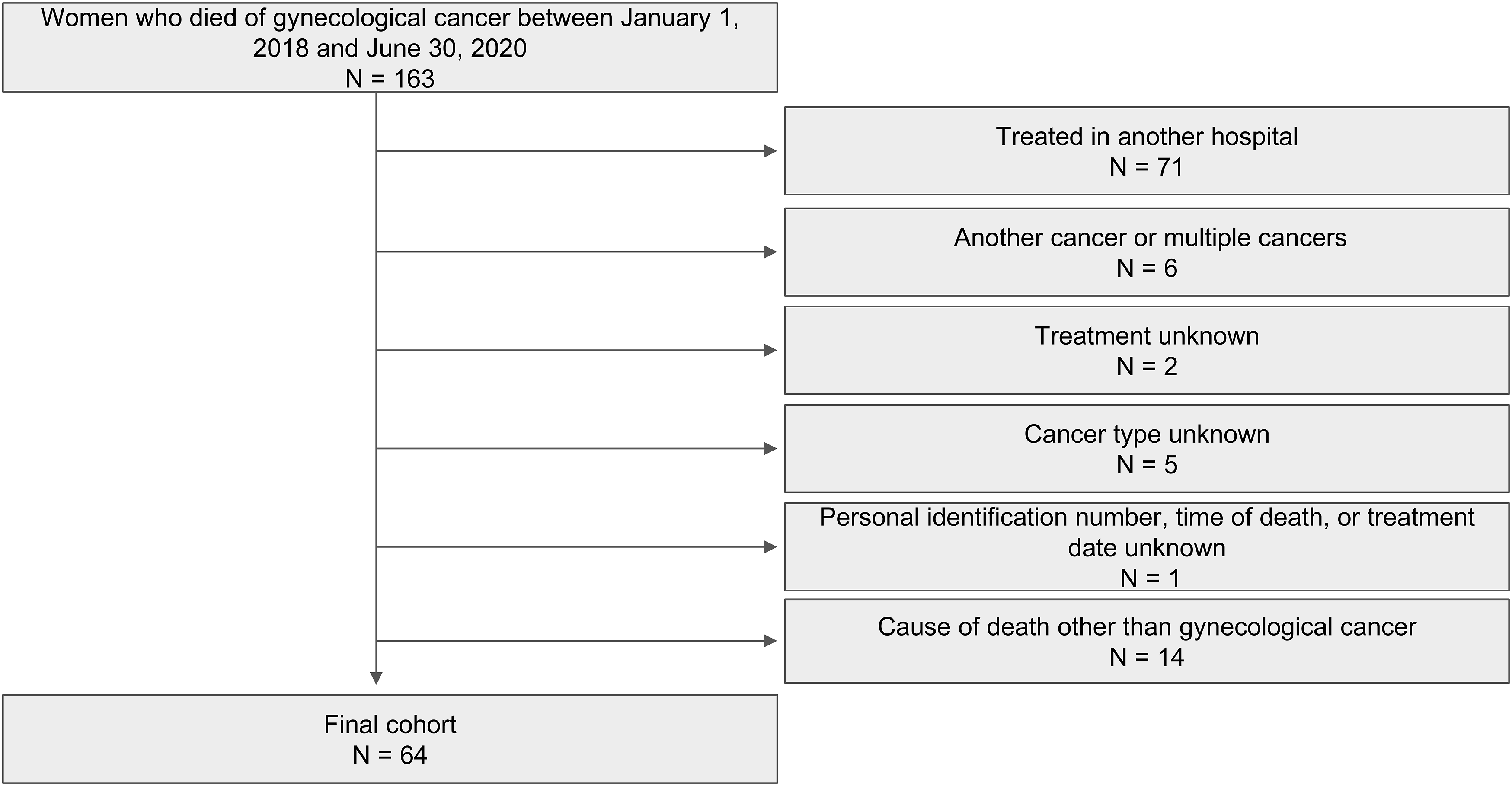
Treatments During the Last 3 months of Life
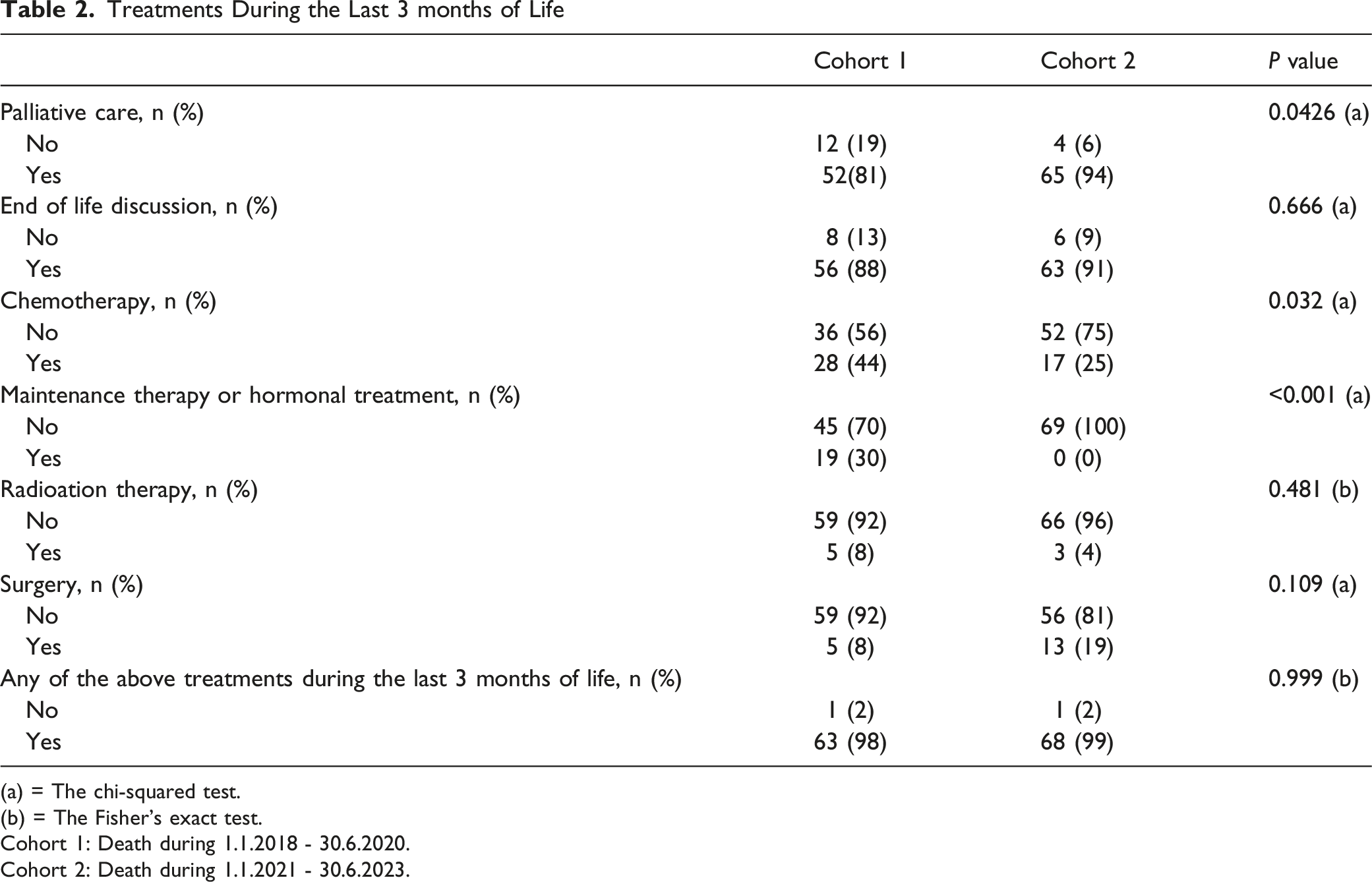
(a) = The chi-squared test.
(b) = The Fisher’s exact test.
Cohort 1: Death during 1.1.2018 - 30.6.2020.
Cohort 2: Death during 1.1.2021 - 30.6.2023.
Procedures During the Last 3 months of Life
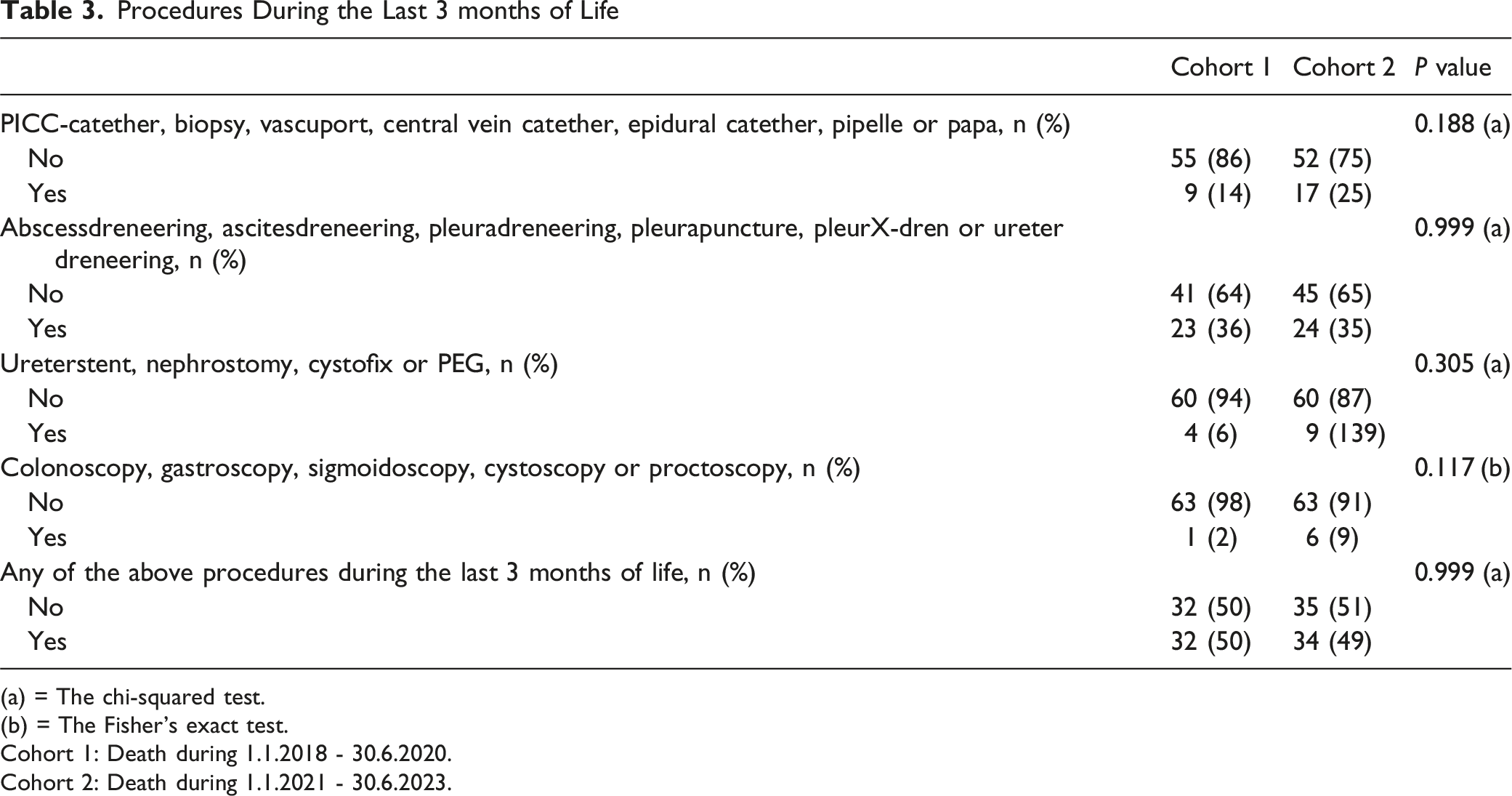
(a) = The chi-squared test.
(b) = The Fisher’s exact test.
Cohort 1: Death during 1.1.2018 - 30.6.2020.
Cohort 2: Death during 1.1.2021 - 30.6.2023.
Time Distributions of Certain Events to Death
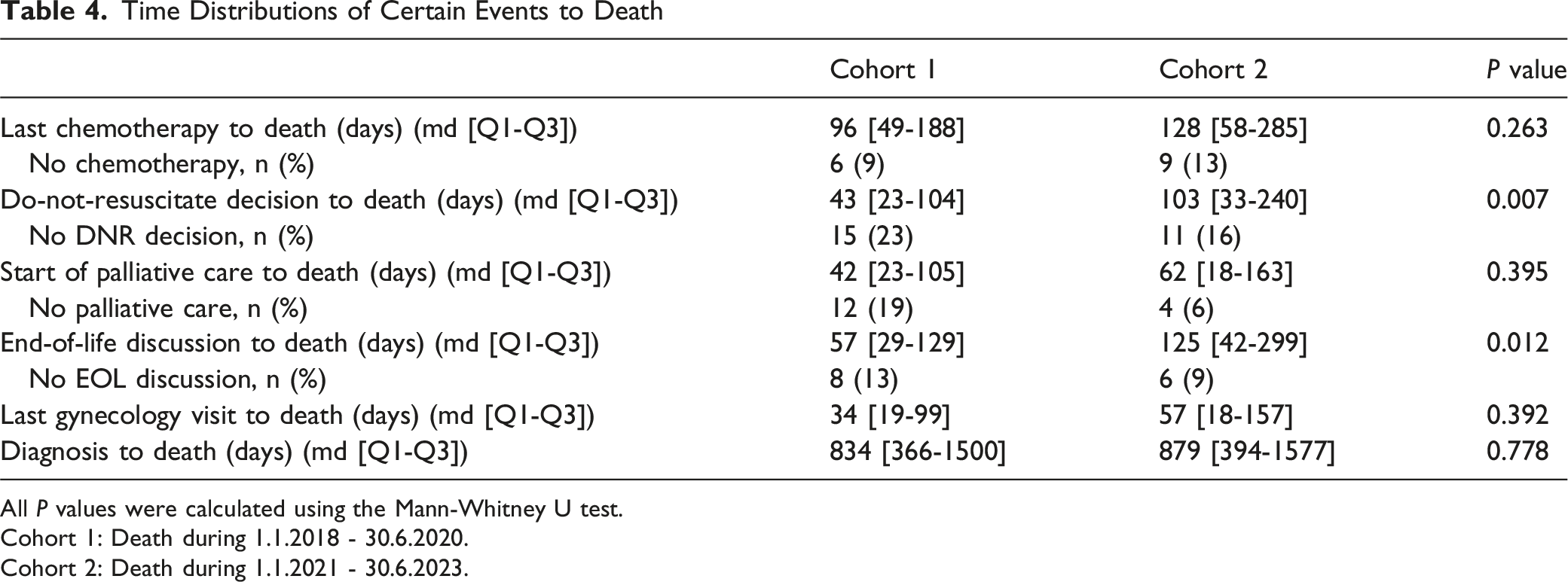
All P values were calculated using the Mann-Whitney U test.
Cohort 1: Death during 1.1.2018 - 30.6.2020.
Cohort 2: Death during 1.1.2021 - 30.6.2023.
We conducted the same analysis separately for ovarian and endometrial cancers. The main findings were similar regardless of whether the cancers were analyzed separately or combined. However, fewer significant findings were observed when the analyzes were conducted separately (Supplement Table 3, 4, 5 and 6).
Discussion
In our study, more patients were referred to palliative care (81% vs 94%) in the latter years (cohort (2) than in previous years (cohort 1), suggesting that quality of life may have in this regard. However, the duration from diagnosis to death was similar in both groups (Table 4). According to a previous study, most patients with gynecologic cancer spend fewer than 30 days in hospice. 6 Earlier referrals for palliative care could reduce hospital admissions and procedures near the EOL. Earlier palliative care referral has been associated with improved EOL quality by various indicators, such as reduced high-intensity care.8,9 In a previous study, the median time from palliative care consultation to death was 2.3 months in cervical cancer patients. 9 In another study, most of the ovarian cancer patients received palliative care 238 days before death. 10 In our study, the time from initiation of palliative care to death was similar in both cohorts, a median of 62 days in cohort 2 and 42 days in cohort 1. In this regard, although palliative care referrals have increased notably in the last 3 months of life across both cohorts, referrals should still occur earlier in the disease process.
A previous study by Prigerson et al found that chemotherapy use near the EOL in patients with end-stage cancer may worsen the quality of life, including patients with good performance status. 11 Lee et al found that in recurrent ovarian cancer, chemotherapy palliated symptoms in less than half of the symptomatic participants, and improvements in quality of life were reported by approximately 1 in 6 patients receiving chemotherapy. 12 In our study, there was a decrease in the number of patients receiving chemotherapy during the last 3 months of life (44% vs 25%, respectively) (Table 2). According to this indicator, the EOL quality may have improved. In another study, 62% of advanced ovarian cancer patients received chemotherapy in the last 3 months of life. 7 Hashimoto et al identified the factors affecting the interval between the last chemotherapy and death in breast cancer, gynecological cancer, primarily unknown cancer, and in other cancer patients, and they found that nearly 50% of patients received chemotherapy during the final 3 months of life. 13 This suggests that in our study, the number of patients receiving chemotherapy in the last 3 months of life has greatly decreased, even compared to other studies. In contrast, one study by Srisuttayasathien et al differed from previous studies by suggesting that in ovarian cancer patients, quality of life did not differ in patients who received salvage chemotherapy compared to patients receiving palliative care. 1 14
Although the number of patients receiving chemotherapy in the last 3 months of life has decreased in our study, there has been no significant increase in the time from last chemotherapy to death (median 96 vs 128 days, respectively) (Table 4). However, the median duration from last chemotherapy to death remains relatively long, particularly in Cohort 2, compared with Hashimoto et al, who reported a median of 100 days. 13
In our study, we found that even though the aggressiveness of chemotherapy treatment close to death has decreased, the time from diagnosis to death has not decreased. This may suggest that aggressive chemotherapy in EOL care does not prolong survival. Similar findings were made in another study, where they suggested that chemotherapy use near death does not provide benefit. 15
Time between EOL discussion and death was significantly longer in cohort 2 (median 57 vs 125 days, respectively) (Table 4). In previous studies, earlier EOL discussions have been associated with better EOL quality. 77,16 Patients who have earlier EOL discussions receive care that is more likely to meet EOL quality measures. 16 Lopez-Acevedo et al found that the median time between EOL discussion and death was 29 days. 7 In another study, they found that in an outpatient setting, the median time between EOL discussion and death was 64 days. 16 This suggests that, in our study, EOL discussions occur early in the disease process, particularly in Cohort 2, compared with previous studies.
Time between DNR decision and death was longer in cohort 2, compared to cohort 1 (median 43 vs 103 days, respectively) (Table 4). No studies have assessed the impact of earlier DNR decisions on EOL quality in gynecological cancer patients. However, patients who had a palliative care consultation in metastatic pancreatic cancer were more likely to have a DNR decision and were significantly less likely to receive aggressive care. 17 A study that described trends of EOL care quality factors of gynecological cancer patients at a tertiary care center, found that the interval time between DNR order and death was 49.6 days during the years 1995-1997. 18 This suggests that in our study, the time between DNR order and death has increased pleasingly.
These findings suggest that the quality of EOL care for gynecological cancer patients at Oulu University Hospital may have over recent years. There remains room for improvement, particularly in the earlier initiation of palliative care. Although no specific procedures were implemented at our hospital to improve palliative care, discussion of its quality increased both nationally and regionally during and between those cohorts. For example, national guidelines on palliative care were published in October 2019. 19 Additionally regional multi-professional palliative care education was conducted in May 2020 and national pilot education for Special Competence in Palliative Care was launched in August 2020. We believe that these things may have affected the increase in palliative care in our hospital.
The major strength of this study was its single-center design at a tertiary care center, which enabled systematic data collection from a consistent source. However, the findings of this study should be interpreted in light of its limitations. Firstly, this is a retrospective review of medical records, which may not reflect all medical interventions performed. We didn’t use validated questionnaires to assess EOL quality; instead, we used indirect measures. Additionally, EOL discussions may not have been adequately documented in the patient’s records, potentially underestimating the number of patients who have EOL discussions. Similarly, the time between EOL discussion and death may have been underestimated or overestimated. We may also have underestimated some EOL quality indicators, such as treatments administered in the last 3 months of life, because patients could have received care at another hospital. Our record settings couldn’t locate these outpatient documents unless there was a separate notation of them in the Oulu University Hospital records. Additionally, we were unable to specify the type of palliative care the patients received. Palliative care was defined as a mention of transitioning to a palliative care approach in the patient records. The location of death was also collected from the patient data, which may have led to an underestimation of the number of patients dying at home or at other wards than the university hospital ward. Our study population is small, which may affect the study’s reliability. Unfortunately, we were unable to include more recent years in the latter cohort because we lack data on the date of death in our hospital records after June 2023. We acknowledge the limitations of this study, including potential selection and misclassification bias.
In our study, more patients were referred to palliative care in the latter years. Additionally, fewer chemotherapies were administered during the last 3 months of life, potentially suggesting that the quality of life may have improved without compromising survival time. In addition, EOL discussions occur earlier in the disease process, which may indicate improved EOL quality by this measure.
Supplemental Material
Supplemental material - Chemotherapy and Palliative Care at the End of Life in Patients With Ovarian and Endometrial Cancer: A Retrospective Study
Supplemental material for Chemotherapy and Palliative Care at the End of Life in Patients With Ovarian and Endometrial Cancer: A Retrospective Study by Angelika Oksa, BM, Heikki Huhtamäki, BSc, Suvi Turunen, PhD and Elina Urpilainen, PhD in American Journal of Hospice and Palliative Medicine®
Supplemental Material
Supplemental material - Chemotherapy and Palliative Care at the End of Life in Patients With Ovarian and Endometrial Cancer: A Retrospective Study
Supplemental material for Chemotherapy and Palliative Care at the End of Life in Patients With Ovarian and Endometrial Cancer: A Retrospective Study by Angelika Oksa, BM, Heikki Huhtamäki, BSc, Suvi Turunen, PhD and Elina Urpilainen, PhD in American Journal of Hospice and Palliative Medicine®
Supplemental Material
Supplemental material - Chemotherapy and Palliative Care at the End of Life in Patients With Ovarian and Endometrial Cancer: A Retrospective Study
Supplemental material for Chemotherapy and Palliative Care at the End of Life in Patients With Ovarian and Endometrial Cancer: A Retrospective Study by Angelika Oksa, BM, Heikki Huhtamäki, BSc, Suvi Turunen, PhD and Elina Urpilainen, PhD in American Journal of Hospice and Palliative Medicine®
Supplemental Material
Supplemental material - Chemotherapy and Palliative Care at the End of Life in Patients With Ovarian and Endometrial Cancer: A Retrospective Study
Supplemental material for Chemotherapy and Palliative Care at the End of Life in Patients With Ovarian and Endometrial Cancer: A Retrospective Study by Angelika Oksa, BM, Heikki Huhtamäki, BSc, Suvi Turunen, PhD and Elina Urpilainen, PhD in American Journal of Hospice and Palliative Medicine®
Supplemental Material
Supplemental material - Chemotherapy and Palliative Care at the End of Life in Patients With Ovarian and Endometrial Cancer: A Retrospective Study
Supplemental material for Chemotherapy and Palliative Care at the End of Life in Patients With Ovarian and Endometrial Cancer: A Retrospective Study by Angelika Oksa, BM, Heikki Huhtamäki, BSc, Suvi Turunen, PhD and Elina Urpilainen, PhD in American Journal of Hospice and Palliative Medicine®
Supplemental Material
Supplemental material - Chemotherapy and Palliative Care at the End of Life in Patients With Ovarian and Endometrial Cancer: A Retrospective Study
Supplemental material for Chemotherapy and Palliative Care at the End of Life in Patients With Ovarian and Endometrial Cancer: A Retrospective Study by Angelika Oksa, BM, Heikki Huhtamäki, BSc, Suvi Turunen, PhD and Elina Urpilainen, PhD in American Journal of Hospice and Palliative Medicine®
Footnotes
Acknowledgments
We want to express our gratitude to MD Päivi Vuolo-Merilä for guidance in palliative care in our hospital, as well as for updating the causes of death in the hospital records.
Ethical Considerations
This study was granted hospital research approval as well as a separate permit for the use of registry data by Oulu University Hospital (99/2024, date April 15, 2024).
Author Contributions
A.O: conceptualization, data collection, writing–original draft, reviewing, editing; H.H: data analysis, writing–original draft, reviewing; S.T: writing–original draft, reviewing, editing; E.U: conceptualization, writing–original draft, reviewing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Finnish government research funds granted to Oulu University Hospital.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.