
Abstract
Background
Advance care planning documentation allows individuals to communicate preferences for medical care and designate surrogate decision-makers. It is unknown if comprehensive documentation confers additional benefits.
Objectives
This study examined additive associations between comprehensive advance care planning (ACP) documentation and end-of-life care (EOL) outcomes among older adults in the United States.
Setting/Subjects
Data from the Health and Retirement Study exit interviews (2010-2022) indicated ACP documentation status, based on proxy-reported completion of a living will (LW) and/or durable power of attorney (DPOA) for 5622 decedents representing 23.2 million individuals.
Measurement
Documentation was operationalized as a binary variable (any document, no document) and an ordinal variable (no documentation, one document, two documents). EOL outcomes included binary indicators of intensive care unit use in the last two years of life, use of life-sustaining treatments, hospice utilization prior to death, and location of death (out-of-hospital, hospital).
Results
About 42.7% decedents had two documents and 28.9% had none, documentation increased substantially around 2014. Compared with no documentation, having any documentation was associated with lower likelihood of life-sustaining treatment (aRR = 0.85, 95% CI: 0.74-0.98) and higher likelihood of hospice utilization (aRR = 1.43, 95% CI: 1.28-1.60) and out-of-hospital death (aRR = 1.11, 95% CI: 1.06-1.18), but not ICU use. Having two documents showed similar patterns. Associations were stronger among decedents with expected death and attenuated among those with unexpected death.
Conclusions
ACP is associated with less aggressive EOL care and greater hospice use, although the incremental benefits of having both documents are modest.
Key Message
Advance care planning documentation is associated with less aggressive end-of-life care and greater hospice use among older adults. However, having multiple documents offers only modest additional benefit, suggesting that communication and care processes, rather than documentation alone, are central to achieving goal-concordant end-of-life care.
Introduction
Advance care planning (ACP) is central to align end-of-life care with patient preferences. ACP allows individuals to articulate their future medical treatment and designate surrogate decision-makers, thereby promoting care aligned with patients’ values and goals.1-4 Two key components of ACP include living wills, which usually document healthcare preferences such as life-sustaining treatments, and durable power of attorney (DPOA) for healthcare, which appoints a surrogate decision-maker to act on the patient’s behalf. 5 Together, these comprehensive ACP documentations are intended to support shared decision-making and reduce uncertainty during critical clinical situations when patients may lack decisional capacity.5-7
Despite longstanding policy and clinical emphasis on ACP, evidence regarding its effectiveness in improving end-of-life outcomes remains mixed.8-10 Earlier studies suggested that ACP is associated with reduced use of aggressive interventions (eg, intensive care unit [ICU] admission, mechanical ventilation, cardiopulmonary resuscitation) and increased hospice utilization.11-16 However, more recent research highlights substantial heterogeneity in these associations, with some studies finding limited or context-dependent effects, particularly after adjusting for patient preferences, illness trajectories, and healthcare system factors.17-19 For example, recent analyses using nationally representative datasets have shown that ACP documentation is associated with greater hospice use and a higher likelihood of dying in their preferred setting (eg, outside of a hospital), but not with reductions in potentially burdensome care such as gastrostomy tube insertion, intubation/mechanical ventilation. 10 One factor contributing to this heterogeneity is that most prior studies have operationalized ACP documentation as a binary construct (any vs none), potentially obscuring important differences between partial and comprehensive ACP documentation.20-22 Emerging evidence emphasizes that ACP is an ongoing process rather than a one-time event, and that effective ACP requires integration of documentation with communication and clinical decision-making processes.23-27 In this context, having both a living will and a DPOA may represent a more complete and actionable form of ACP, potentially leading to more goal-concordant end-of-life care. 15
Additionally, whether these additive associations differ by the anticipated trajectory of death is further unresolved question. 28 When death is anticipated, there may be a greater opportunity for ACP to influence care decisions through communication and planning. In contrast, in cases of unexpected death (eg, sudden death from a heart attack), the opportunity for ACP to shape care may be more limited, and the presence of a surrogate decision-maker may play a more critical role than documented preferences alone. However, to our knowledge, few prior studies explicitly examined whether the associations between ACP and end-of-life care differ by the expectedness of death.
Conceptually, this study is guided by contemporary models of ACP that view ACP as a multistep process rather than a discrete documentation event. The Advance Care Planning Process Framework posits that formal documents, such as living wills and durable powers of attorney for healthcare, serve as mechanisms through which patient preferences are communicated, surrogate decision-makers are prepared, and shared decision-making can occur when decisional capacity is lost.4,27 In this framework, documentation alone does not directly determine end-of-life care; rather, its influence is mediated through communication, surrogate engagement, and the accessibility of patient preferences during clinical decision-making. Consequently, more comprehensive ACP documentation may facilitate goal-concordant care by strengthening these underlying processes. We further posit that these mechanisms may operate differently depending on whether death is anticipated, as expected illness trajectories provide greater opportunity for communication and care planning than sudden or unexpected deaths.
To address these gaps, we used nationally representative data from the Health and Retirement Study (HRS) to examine additive associations between comprehensive ACP documentation (living wills and DPOA) and end-of-life care outcomes among U.S. older adults. We evaluated whether having both documents is associated with differences in intensive care use, life-sustaining treatment, hospice utilization, and location of death, compared with having one or no documents. We further examined whether these associations vary by the expectedness of death and assessed temporal trends in ACP documentation. By distinguishing between partial and comprehensive ACP documentation, this study aims to provide new insights into the mechanisms by which ACP documentation may influence end-of-life care and to inform policies and interventions that promote goal-concordant end-of-life care.
Methods
Data Source and Study Population
Guided by the Advance Care Planning Process Framework, ACP documentation was conceptualized as a structural component of advance care planning that may facilitate communication, surrogate preparedness, and goal-concordant decision-making at the end of life. To embody this framework, we conducted a retrospective cross-sectional study using HRS data, a nationally representative longitudinal survey of U.S. adults aged 50 years and older.29,30 We analyzed exit interview data collected from 2010 to 2022, generally covering decedents who died one to three years before the interview. The interviews were administered to proxy respondents following a participant’s death and provide detailed information on end-of-life experiences, healthcare utilization, and advance care planning. 31 The analytic sample included decedents aged 50 years or older with complete information on ACP documentation (living will and/or DPOA) and having positive sampling weights (n = 6986). After excluding respondents with missing data on sociodemographic and death-related variables, the main analytic sample consisted of 5622 decedents, representing approximately 23.2 million individuals nationwide. The University of Florida Institutional Review Board determined that this study involved non-human subjects research using publicly available, de-identified data and was therefore exempt from review. This study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline for cross-sectional studies.
Measures
The primary exposure was the comprehensive ACP documentation completion status, based on proxy-reported information on whether the decedent had a living will and/or a DPOA for healthcare. We operationalized it using two approaches. First, a binary indicator distinguished individuals with any documentation (living will and/or DPOA) from those with none. Second, an ordinal variable categorized individuals into three mutually exclusive groups to ensure adequate cell sizes for multivariable regression analyses: no documentation, one document (either a living will or DPOA), and two documents (both a living will and DPOA). This categorization allowed examination of the additive associations of having both components of ACP documentation.
We examined four end-of-life care outcomes reported in the exit interview: ICU use in the last two years of life, use of life-sustaining treatments, hospice utilization prior to death, and location of death categorized as out-of-hospital vs hospital death. All outcomes were treated as binary variables (yes, no).
We examined four end-of-life care outcomes reported in the exit interview: ICU use in the last two years of life, use of life-sustaining treatments, hospice utilization prior to death, and location of death categorized as out-of-hospital vs hospital death.
Demographic characteristics included age at death (50-64, 65-84, ≥85 years), sex (male, female), race/ethnicity (non-Hispanic White, non-Hispanic Black, Hispanic, non-Hispanic Other), educational attainment (GED or lower, high school graduate, some college, college graduate or above), marital status (married or living with a partner, divorced or separated, widowed, never married), income categorized into quartiles (Q1–Q4), with Q1 representing the lowest income group, cause of death (cancer, cardiovascular disease, or other causes), and whether the death was expected at about the time it occurred (yes/no). These variables were selected based on prior literature demonstrating their associations with advance care planning and end-of-life decision-making.32,33
Statistical Analysis
We first compared decedents’ characteristics by ACP documentation status using chi-square tests. We then estimated the annual prevalence of ACP documentation completion by year of death from 2008 to 2021 and assessed linear trends over time. These analyses were additionally stratified by expectedness of death to examine potential differences in temporal patterns. To further characterize trends, we conducted joinpoint regression analyses to estimate annual percent change (APC) in ACP documentation completion and to evaluate the statistical significance of changes in trend slopes across distinct time periods. 34
Next, we calculated the prevalence of each end-of-life outcome across ACP documentation groups. To examine associations between ACP documentation and end-of-life care outcomes, we used modified Poisson regression models with robust variance estimation to estimate adjusted risk ratios (aRRs) and 95% confidence intervals (CIs) adjusting for aforementioned covariates. This approach was selected to provide valid and interpretable estimates of relative risk for common binary outcomes. 35 Models were specified using both binary (any vs none) and ordinal (none, one document, two documents) exposure definitions, with no ACP documentation as the reference category. We further conducted stratified analyses by expected vs unexpected death to assess whether associations varied by the anticipated nature of death.
All analyses accounted for the HRS complex survey design, incorporating last wave interview sampling weights, strata, and primary sampling units to generate nationally representative estimates. Statistical analyses were performed using SAS version 9.4 (SAS Institute Inc.) and Stata version 19 (StataCorp), and statistical significance was defined as a two-sided P-value less than 0.05.
Results
Respondent-Reported Characteristics of Decedents by Dementia Status Before Death (n = 5622, Weighted n = 23,194,490)
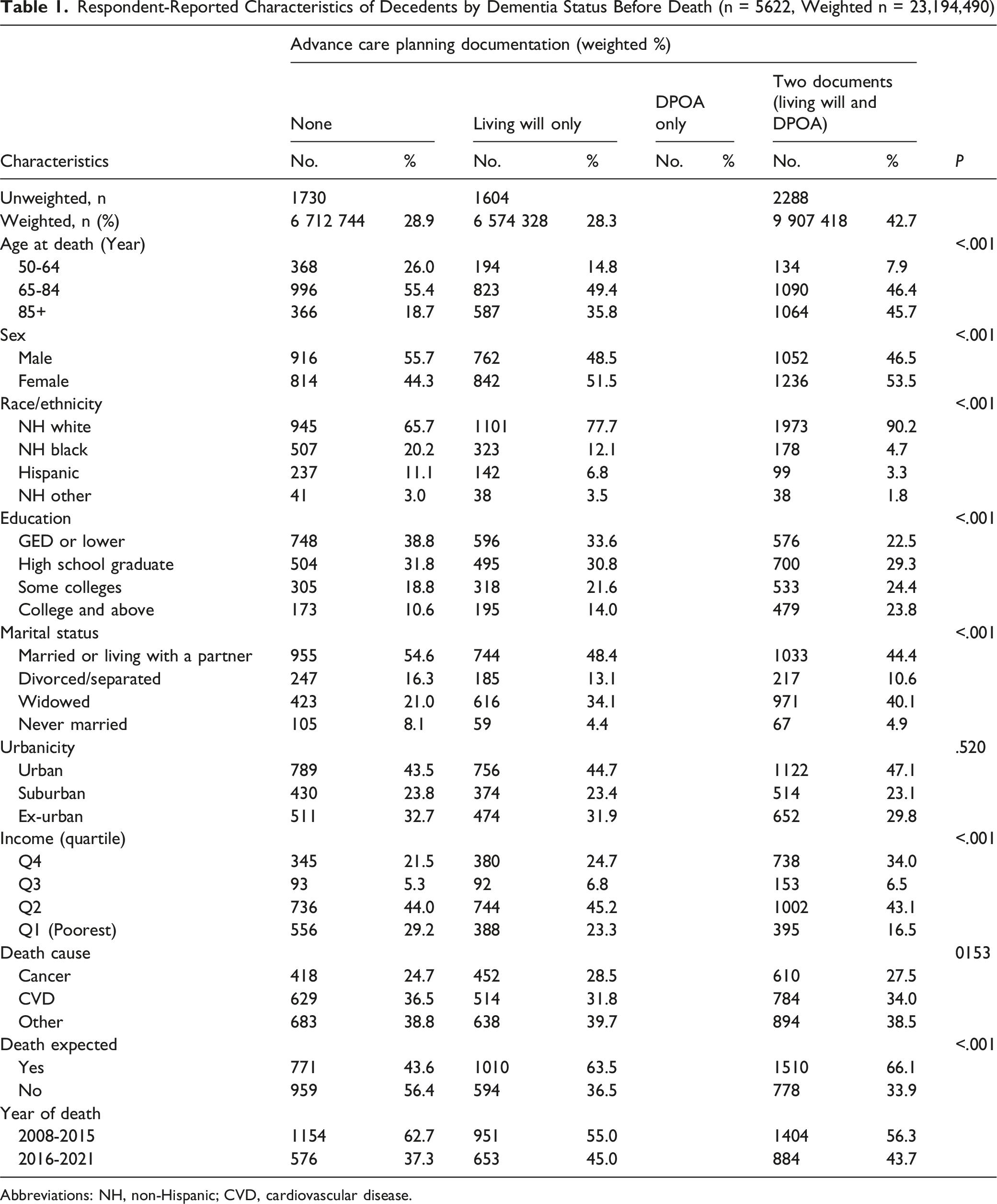
Abbreviations: NH, non-Hispanic; CVD, cardiovascular disease.
Prevalence and Relative Risks of End-of-Life Care Outcomes Among Decedents Using Survey-Weighted Modified Poisson Regression
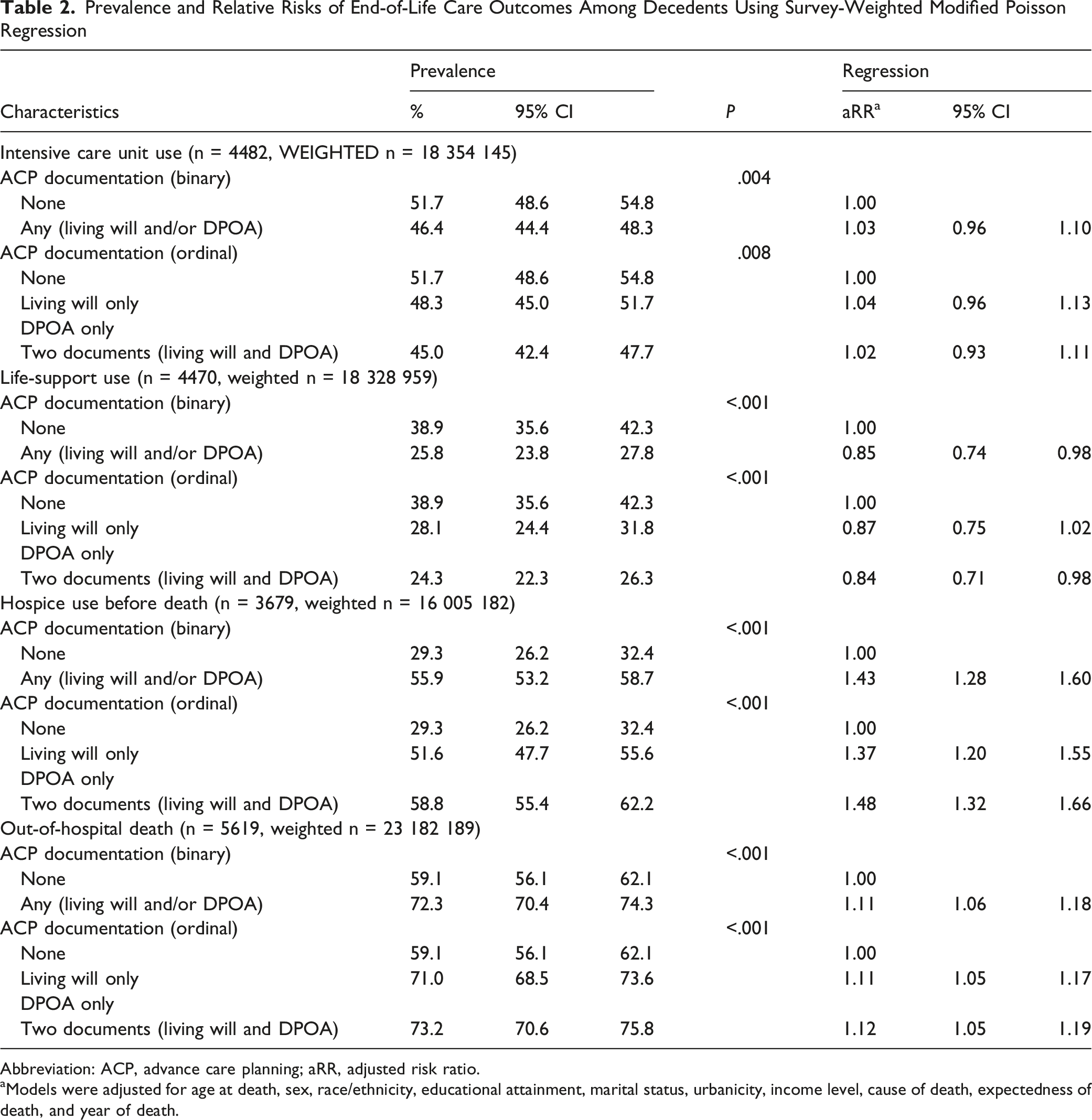
Abbreviation: ACP, advance care planning; aRR, adjusted risk ratio.
aModels were adjusted for age at death, sex, race/ethnicity, educational attainment, marital status, urbanicity, income level, cause of death, expectedness of death, and year of death.
Relative Risks of End-of-Life Care Outcomes Estimated via Modified Poisson Regression, Stratified by Death Expectedness
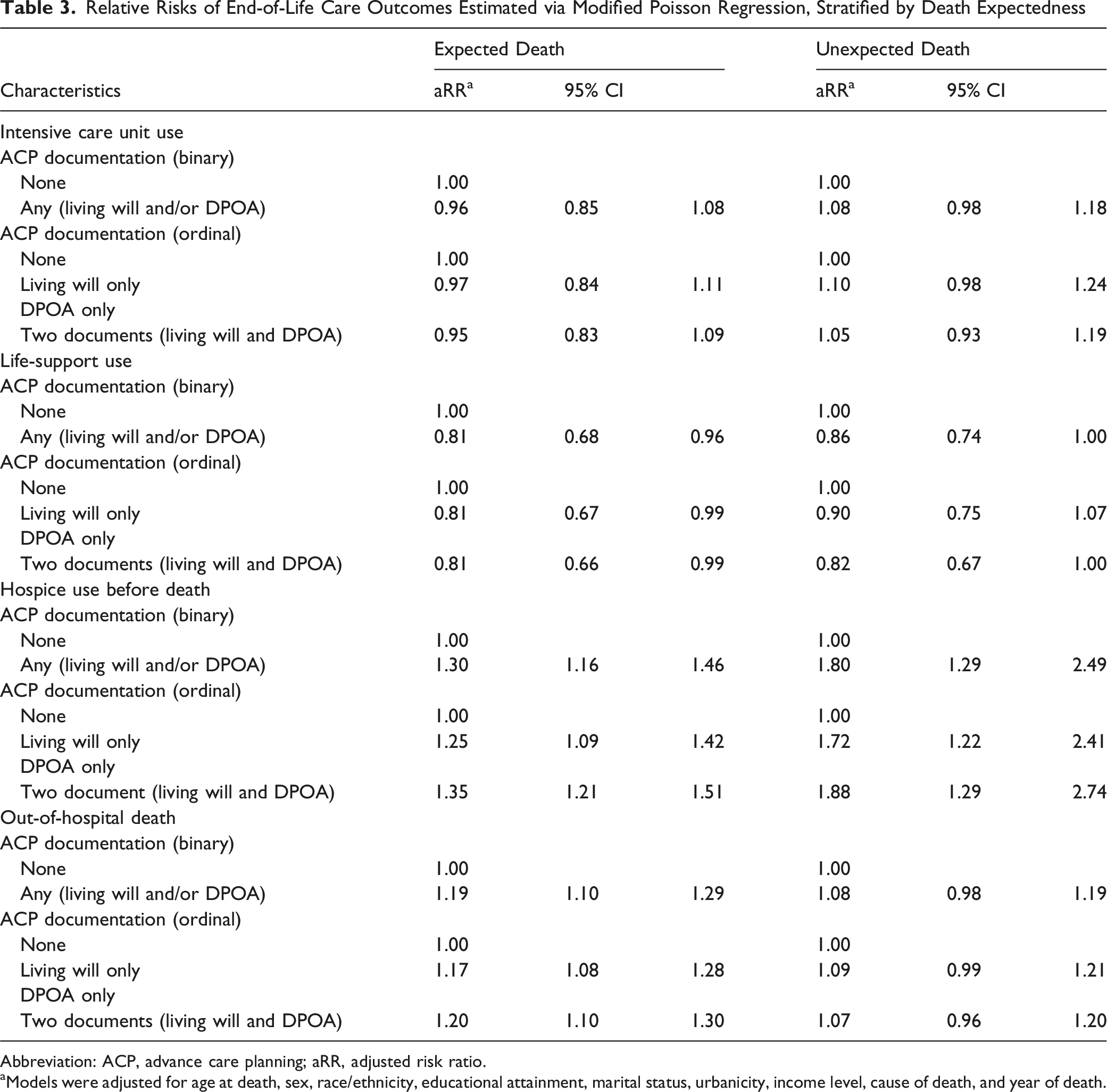
Abbreviation: ACP, advance care planning; aRR, adjusted risk ratio.
aModels were adjusted for age at death, sex, race/ethnicity, educational attainment, marital status, urbanicity, income level, cause of death, and year of death.
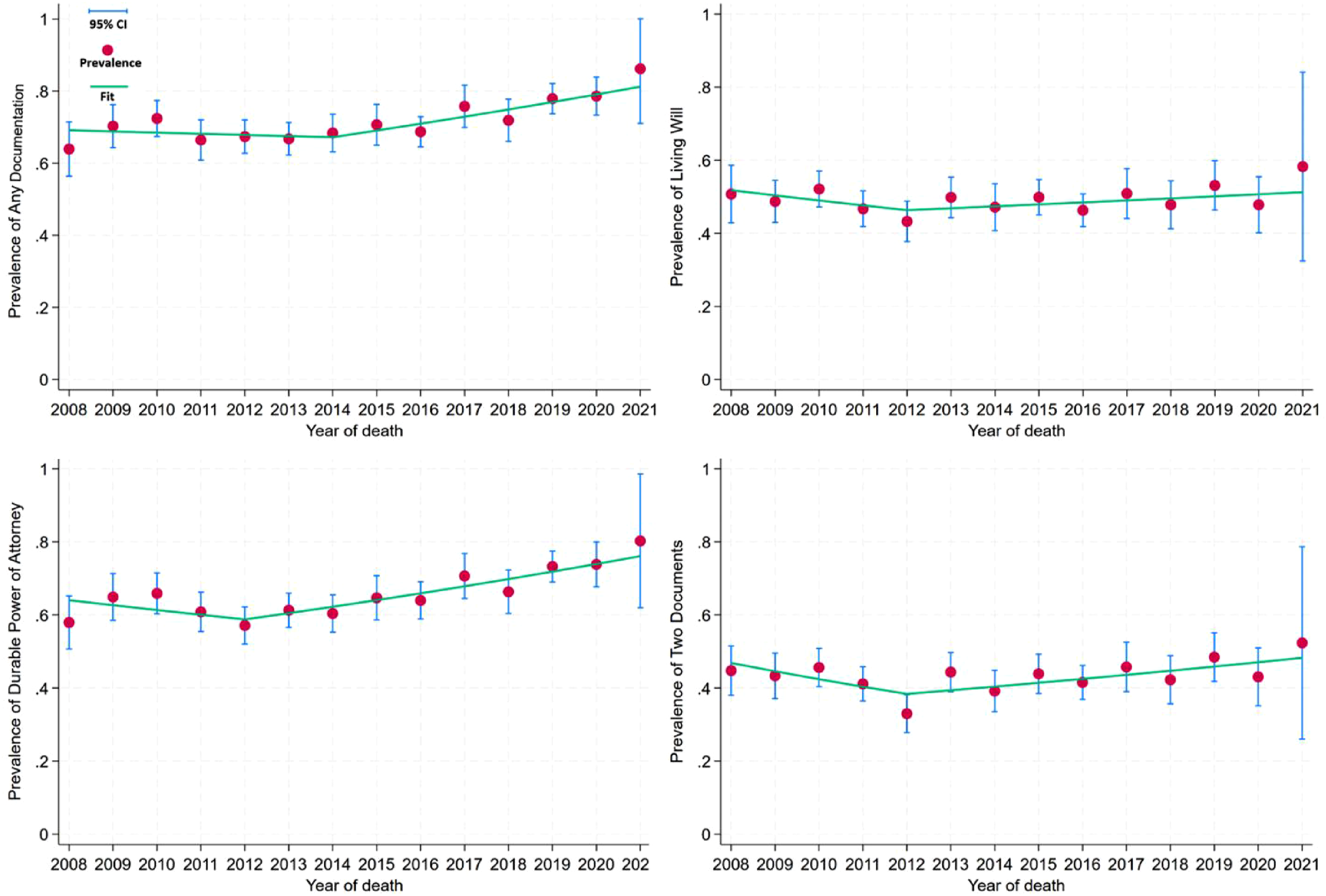
Temporal trends indicated a substantial increase in any ACP documentation, either Living will or DPOA, and two documents over time (P < .05), with overall higher prevalence in the expected death group than unexpected death group (Figure 1). The prevalence of any ACP documentation remained relatively stable between 2008 and 2016 but increased significantly thereafter, reaching more than 86% by 2021. Joinpoint analysis identified a significant inflection point around 2014, after which the prevalence increased at an annual rate of approximately 2.7% (Figure 2). Similar patterns were observed for durable power of attorney and completion of both documents, with evidence of a reversal from declining or stable trends prior to approximately 2012 to significant increases thereafter. These findings suggest a growing uptake of advance care planning, particularly comprehensive documentation involving both treatment preferences and surrogate designation. Trends in advance care planning documentation (living wills and durable power of attorney [DPOA]) before death among decedents, 2008-2021. Jointpoint analysis of any advance care planning documentation (living wills and/or durable power of attorney [DPOA]), living will, DPOA, and two documents (living will and DPOA) before death among decedents, 2008-2021.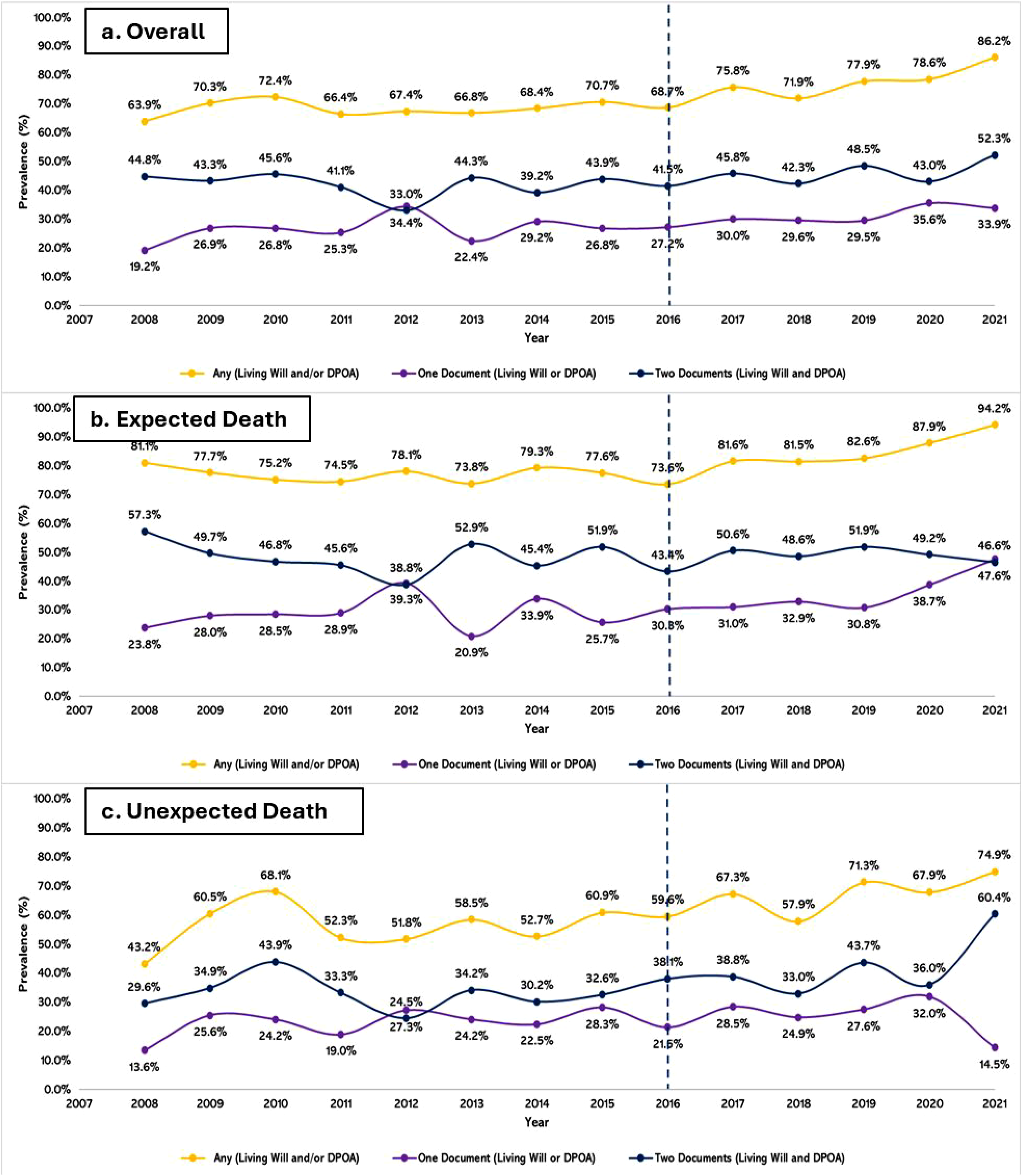
Discussion
In this nationally representative study of U.S. older adult decedents, we observed a substantial increase in ACP documentation over time, particularly after a joinpoint inflection around 2014. Having any ACP documentation was associated with more favorable end-of-life outcomes compared with having no documentation, though the incremental benefit of having both a living will and a DPOA relative to a single document was modest after covariate adjustment. In stratified analyses, associations with life-sustaining treatment and out-of-hospital death were more pronounced among individuals with expected death and attenuated among those with unexpected death; however, ACP documentation remained strongly associated with hospice utilization regardless of death expectedness. Together, these findings suggest that while ACP documentation is associated with less aggressive end-of-life care patterns, much of the observed benefit may be driven by broader processes underlying ACP rather than the accumulation of documents alone.
Temporal Trend in ACP Documentation
These findings are consistent with contemporary conceptual models that distinguish ACP documentation from the broader ACP process. Under this framework, living wills and durable powers of attorney function as tools that support communication, surrogate activation, and preference implementation rather than as independent determinants of care. The relatively modest incremental benefit observed for dual documentation suggests that the pathways linking ACP to end-of-life outcomes may depend more heavily on the quality of communication and preparedness generated by the ACP process than on the number of documents completed.
The observed increase in ACP documentation prevalence over time, particularly the acceleration identified by joinpoint analysis around 2014, likely reflects a confluence of policy, clinical, and cultural shifts that have elevated the prominence of advance care planning in routine care. The introduction of Medicare reimbursement for ACP discussions in 2016, alongside growing emphasis on patient-centered care and serious illness communication, may have incentivized clinicians to engage patients in these conversations and formalize documentation.23,25 In addition, broader public awareness of end-of-life planning, driven by initiatives such as The Conversation Project and increased attention to goal-concordant care may have contributed to rising uptake. Despite these encouraging trends, prior work suggests that disparities in ACP completion persist across racial, socioeconomic, and educational groups, 22 which is consistent with the sociodemographic gradients observed in our sample. Taken together, these findings suggest that while ACP is becoming more common, equitable access to and engagement in ACP remain important areas for intervention.
Modest Incremental Benefit of Having Both Documents
Although having both a living will and a durable power of attorney represents a more comprehensive form of ACP, our findings indicate that the incremental benefit of dual documentation (beyond having a single document) is modest after adjustment for sociodemographic and clinical factors. This pattern aligns with emerging conceptualizations of ACP as a dynamic, communication-driven process rather than a static documentation event.27,36,37 The presence of any documentation may serve as a proxy for underlying patient engagement, preferences for less aggressive care, or prior discussions with clinicians and family members, which may be the primary drivers of observed differences in end-of-life outcomes. In this context, the marginal gains associated with additional documentation may reflect diminishing returns when preferences are already known or when surrogate decision-makers are sufficiently prepared. These findings are consistent with prior studies demonstrating that ACP’s effectiveness depends not only on the existence of documents but also on their integration into clinical workflows and real-time decision-making.10,17,38 Accordingly, interventions focused solely on increasing documentation rates may have a limited impact unless paired with efforts to enhance communication quality, surrogate preparedness, and accessibility of ACP information at the point of care.
Variation by Expectedness of Death
The stronger associations between ACP documentation and life-sustaining treatment, hospice utilization, and out-of-hospital death observed among decedents with expected death are consistent with the premise that anticipated dying trajectories create greater opportunity for iterative discussions, prognostic awareness, and alignment of care with patient preferences.39,40 In cases of unexpected death, such as acute events or rapid clinical deterioration, the window for ACP to influence care may be limited, and decisions may be driven more by emergent clinical circumstances than by previously documented preferences. A notable exception to the general attenuation pattern was hospice utilization, for which ACP documentation showed its strongest association in those with unexpected death. One interpretation is that among decedents whose deaths were expected, hospice utilization is relatively common regardless of documentation status, leaving less room for documentation to differentiate care patterns. In contrast, when death is unexpected, documented preferences or a designated surrogate may function as a more decisive signal that redirects care toward hospice even in acute clinical situations where extended deliberation is not feasible. Our findings suggest that the mechanisms through which ACP documentation influences hospice referral differently from other end-of-life care decisions; surrogate activation and the documentation signaling may be more important than preference specification alone when death is not expected. 41 Further investigation of these pathway-specific effects is warranted.
Policy Implications
Our findings suggest that future ACP initiatives should move beyond document completion as the primary marker of success. While recent policy efforts such as Medicare reimbursement for advance care planning have likely contributed to increased documentation,23,39,42,43 our results suggest that expanding documentation alone may be insufficient to meaningfully improve end-of-life care. Policies should therefore move beyond document-completion metrics and promote systems that support ongoing communication about patient goals, values, and treatment preferences across care teams and care transitions. Ensuring that ACP information is routinely reviewed, updated, and accessible across settings may be particularly important for translating preferences into care decisions during serious illness.
Our findings also highlight persistent sociodemographic differences in ACP documentation. Targeted outreach and education efforts focused on historically underserved populations, including racial and ethnic minority groups and individuals with lower educational attainment, may help reduce disparities in ACP engagement. In addition, clinician-facing interventions, including structured communication training, decision aids, and technology-supported ACP programs, have demonstrated success in improving ACP engagement and documentation and may represent scalable approaches for health systems seeking to improve goal-concordant care. Collectively, these strategies may enhance patient-centered decision-making, improve care quality, and promote more efficient use of healthcare resources near the end of life.
Although documentation was associated with less aggressive end-of-life care and greater hospice utilization, the modest incremental benefit of having multiple documents indicates that communication and decision-making processes may be more important than documentation quantity alone. Health systems should prioritize interventions that improve communication among patients, families, surrogate decision-makers, and clinicians, while ensuring that ACP information is readily accessible across care settings. Future research should identify which components of the ACP process—including surrogate preparedness, communication quality, and timing of discussions—most effectively promote goal-concordant care.
Limitations
These findings should be interpreted in light of the following limitations. First, the use of proxy-reported exit interview data may introduce recall bias or misclassification, particularly for ACP documentation and end-of-life care experiences. Although proxy reports are widely used in end-of-life research and are often the only feasible source of information after death, their accuracy may vary depending on the respondent’s knowledge and involvement in care. Second, our measures of ACP documentation capture the presence of living wills and durable power of attorney but do not reflect the content, quality, timing, or accessibility of these documents, nor whether they were available or adhered to at the point of care. As a result, we were unable to assess whether care was truly goal concordant. Third, outcomes were measured as broad indicators of healthcare utilization and may not fully capture the complexity of end-of-life decision-making or the appropriateness of care in specific clinical contexts. Fourth, stratification by expectedness of death was based on proxy assessment and may be subject to misclassification, particularly in cases with uncertain illness trajectories. Finally, the observational study design precludes causal inference. Individuals with ACP documentation may differ systematically from those without in ways not fully captured by measured covariates, such as health literacy, preferences for care, or engagement with the healthcare system, potentially leading to residual confounding. Despite these limitations, this study leverages a large, nationally representative dataset and robust analytic methods to provide new insights into the role of ACP documentation components in shaping end-of-life care.
Conclusions
Comprehensive ACP documentation was associated with less aggressive end-of-life care and greater hospice utilization among U.S. older adults, although the additional benefit of having both a living will and durable power of attorney was modest. These findings suggest that ACP effectiveness may depend less on the accumulation of documents and more on the communication, surrogate preparation, and decision-making processes that documentation facilitates. Efforts to improve end-of-life care should therefore focus on strengthening the quality and implementation of ACP conversations, as well as on promoting documentation completion.
Footnotes
Ethical Considerations
The HRS is a publicly available, de-identified dataset, the Institutional Review Board (IRB) determined that this study was non-human subject research.
Author Contributions
ZX: Conceptualization; methodology; software; formal analysis; original draft; writing – review and editing.
MJ: Conceptualization; original draft; supervising; writing – review and editing; corresponding author.
JL: Conceptualization; writing – review and editing.
BP: Conceptualization; writing – review and editing.
YH: Conceptualization; methodology; supervising; writing – review and editing; senior author.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.