
Abstract
Context
Hospice care is intended for the final phase of life, but trajectories after admission vary widely. Some patients die within days, whereas others stabilize and live longer than expected. Very short stays may limit comprehensive care, while prolonged stays may involve socio-existential concerns and practical challenges. Early symptom profiles may reveal differences between trajectories.
Objectives
To describe multidimensional symptom profiles at admission and during the first month of hospice care among patients with short, average, and prolonged survival.
Methods
Patient-completed Utrecht Symptom Diary–4 Dimensional (USD-4D) data from 15 Dutch hospices (2017-2025) were analyzed. Survival was grouped as short (0-3 days), average (4-93 days), or prolonged (≥94 days). Physical/psychological prevalence (>0) and clinically relevant prevalence (>3) were calculated, and intensity (0-10) was summarized for all items at admission and across five predefined 3-day windows during the first month.
Results
Among 2112 patients, 82 had short survival, 1825 had average survival, and 205 had prolonged survival. Physical and psychological burden were highest in short survival, intermediate in average survival, and lowest in prolonged survival; in prolonged survival, physical symptoms improved within two weeks and then stabilized. Socio-existential concerns were more prominent in the short and prolonged survival groups than in the average-survival group.
Conclusion
Multidimensional symptom and concern profiles differed across survival groups, with differences visible at admission and more pronounced within two weeks. Routine multidimensional evaluation within two weeks may help identify emerging prolonged trajectories and align care with changing physical and socio-existential needs.
Keywords
Introduction
Hospices provide palliative care to patients with a limited life expectancy due to terminal illness. This care focuses on symptom management and quality of life and is multidimensional, addressing symptoms and concerns across the physical, psychological, and socio-existential dimensions.1-3 Hospice patients report an average of six to seven symptoms on admission, and one in four has needs in at least three of the four dimensions.4,5
Physical symptoms are known to affect both prognosis and quality of life during the palliative phase.6-10 Studies using patient-reported outcome measures have also shown correlations between socio-existential concerns and reduced quality of life, as well as associations with increased physical and psychological symptoms.11-13 This underlines the importance of assessing symptoms across all dimensions in palliative and hospice care.
The Utrecht Symptom Diary-4 Dimensional (USD-4D) was developed to assess multidimensional symptoms in a single patient-reported outcome measure. 14 The Utrecht Symptom Diary (USD) originated as an adaptation of the Edmonton Symptom Assessment System, which includes commonly reported physical and psychological symptoms in palliative care. 15 The USD was later expanded to include concerns in the socio-existential dimensions, reflecting the five polarities of the Diamond Model. 16 This resulted in the 19-item USD-4D, which consists of twelve items related to physical and psychological symptoms, five items addressing socio-existential concerns, and two items focusing on overall well-being and perceived value of life. Both the USD and USD-4D have been validated and are commonly used in various settings, including hospices.12,17
In the Netherlands, patients have access to hospice care with an estimated life expectancy of three months or less. Dutch hospice data show that 14% of patients die within three days of admission, while 6% survive beyond three months. 18 Admission may not be appropriate in both cases, which poses problems for hospices. Short hospice stays may come too late for effective care to be started, while prolonged hospice stays can prevent hospices from making optimal use of their resources. Prolonged survival can also create emotional, social, and financial strain for patients and families. 19 Given that physicians tend to overestimate rather than underestimate life expectancy in the palliative phase,20,21 patients who outlive their prognosis remain infrequently studied.
Hospices indicate that a comprehensive, multidimensional intake takes about two weeks. This moment offers a first opportunity to evaluate the admission and signal, among others, the potential for extended survival. Earlier identification of such cases could help patients and hospices better tailor care and prevent later problems.
This study aims to describe multidimensional symptom profiles among hospice patients with short, average, and prolonged survival to better inform patient evaluation during the first month of hospice care. To this end, it will compare baseline characteristics and admission symptoms across these groups and examine weekly trajectories of multidimensional symptom and concern scores during the first month in patients with short, average, and prolonged survival.
Methods
Study Design and Setting
This retrospective observational study used clinically collected data from the SYMPAL database, which contains data from 15 high-care hospices in the Netherlands that are members of the Dutch Association of Hospice Care (Associatie Hospicezorg Nederland, AHzN). Data were collected between 2017 and 2025 from patients admitted to these hospices during this period and who had completed at least one USD-4D. Analysis was conducted retrospectively in May and June of 2025. This study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement for cohort studies. 22
Inclusion Criteria
Patients in the database were divided into three groups based on the known survival time. Short survival was defined as 0 to 3 days, average survival as 4 to 93 days, and prolonged survival as 94 days or more, following the definitions used in the HOPEVOL trial and Dutch regulations. 18 Patients known to be alive beyond 94 days after admission were classified as prolonged survivors, irrespective of whether they remained in hospice. Patients with a confirmed death before day 4 were classified as short survivors, and those dying between days 4 and 93 as average survivors, regardless of place of death. To best reflect patients’ experiences, only USD-4Ds completed by patients themselves were included.
Study Size
Given the descriptive design, no a priori sample size calculation was performed; the study size was determined by the number of eligible patients available in the SYMPAL database.
Outcome Measurements
The primary outcome was the prevalence, clinical relevance, and intensity of multidimensional symptoms and concerns across the three survival groups at admission, and across the average and prolonged survival groups during the first month after admission.
Multidimensional symptoms and concerns were assessed using the USD-4D, a 19-item instrument scored from 0 to 10, with higher scores indicating greater symptom burden or concern. The instrument covers physical symptoms (pain, sleeping problems, dry mouth, dysphagia, appetite loss, altered bowel habits, nausea, dyspnea, and fatigue), psychological symptoms (feeling different than usual, anxiety, and depressed mood), and socio-existential concerns (‘taking time for yourself’, ‘bearing what happens’, ‘letting loved ones go’, ‘perceived balance in life’, and ‘thinking about the end of life gives peace of mind’). Two additional items, well-being and perceived value of life, are assessed separately from these dimensions. The USD-4D is typically completed twice weekly as part of standard hospice care but, can be completed more frequently if needed. Dutch and English versions of the USD-4D are provided in Supplemental Appendix 1.
For physical and psychological items, prevalence was defined as an item score greater than zero, reflecting the presence of any reported symptom, and clinical relevance as an item score greater than three, indicating symptoms that were more pronounced and likely to require clinical attention. Prevalence and clinical relevance were not calculated for well-being, perceived value of life, or the socio-existential USD-4D items, as these items concern social and spiritual aspects of patients’ values, wishes, and sense-making rather than discrete medical symptoms. Intensity was defined as the item score (0-10) for all USD-4D items.
In addition, patient characteristics were collected to describe the study population. Age (years), sex (female or male), primary diagnosis (cancer, organ failure, degenerative disease, infectious disease, frailty, or other), marital status (married/partnered, widowed, divorced, or never married), living situation (alone or not alone), and accommodation prior to hospice admission (home, hospital, nursing home, or other) were included.
Analysis
Patient characteristics were described per survival group. Categorical variables were presented as counts and percentages, and continuous variables as median with interquartile ranges, based on distribution, which was assessed using Q–Q plots and the Shapiro-Wilk test.23-26
To capture patient status at predefined time points and reduce variation in the timing of assessment, five 3-day windows were specified: the first 72 hours after admission and 3-day periods centered on days 7, 14, 21, and 28. Only patient-completed USD-4Ds within these windows were included. When multiple USD-4Ds were available within a window, the most complete questionnaire was selected. Missing responses were handled per item using available-case analysis (each statistic was based on available responses for that item).
For physical and psychological USD-4D items, symptom prevalence and clinical relevance were calculated and reported as percentages, with the corresponding number of available responses. Symptom prevalence and clinical relevance were defined as the percentage of patients reporting a score greater than zero and greater than three, respectively. Item intensity scores were analyzed as continuous variables and summarized as median with interquartile range. 17 USD-4D scores at admission were analyzed for all survival groups; for patients with average and prolonged survival, the same analyses were repeated at the predefined time points.
All analyses were performed using IBM SPSS Statistics, version 30.0.27. 27
Results
Patient Characteristics
Data were available for 2342 unique patients, of whom 2112 could be classified into a survival group. In 230 cases, patients left hospice within 93 days, and no date of death was recorded; these patients could not be classified. Of the 2112 classified patients, 82 (3.9%) had short survival, 1825 (86.4%) had average survival, and 205 (9.7%) had prolonged survival. Across the five predefined time windows, 1120 patients completed one or more USD-4Ds and were therefore included in the week-by-week analyses.
Median age was highest in the short survival group and lowest in the prolonged survival group. Cancer was the predominant diagnosis across all groups, particularly in the average survival group, whereas organ failure was more common in the short survival group. Most patients were living at home prior to hospice admission, followed by hospital care, with similar distributions across survival groups. Sex distribution and social characteristics were largely comparable between groups.
Baseline Demographic and Clinical Characteristics of Hospice Patients in the Full Cohort and Week-By-Week Cohort, Stratified by Survival Category
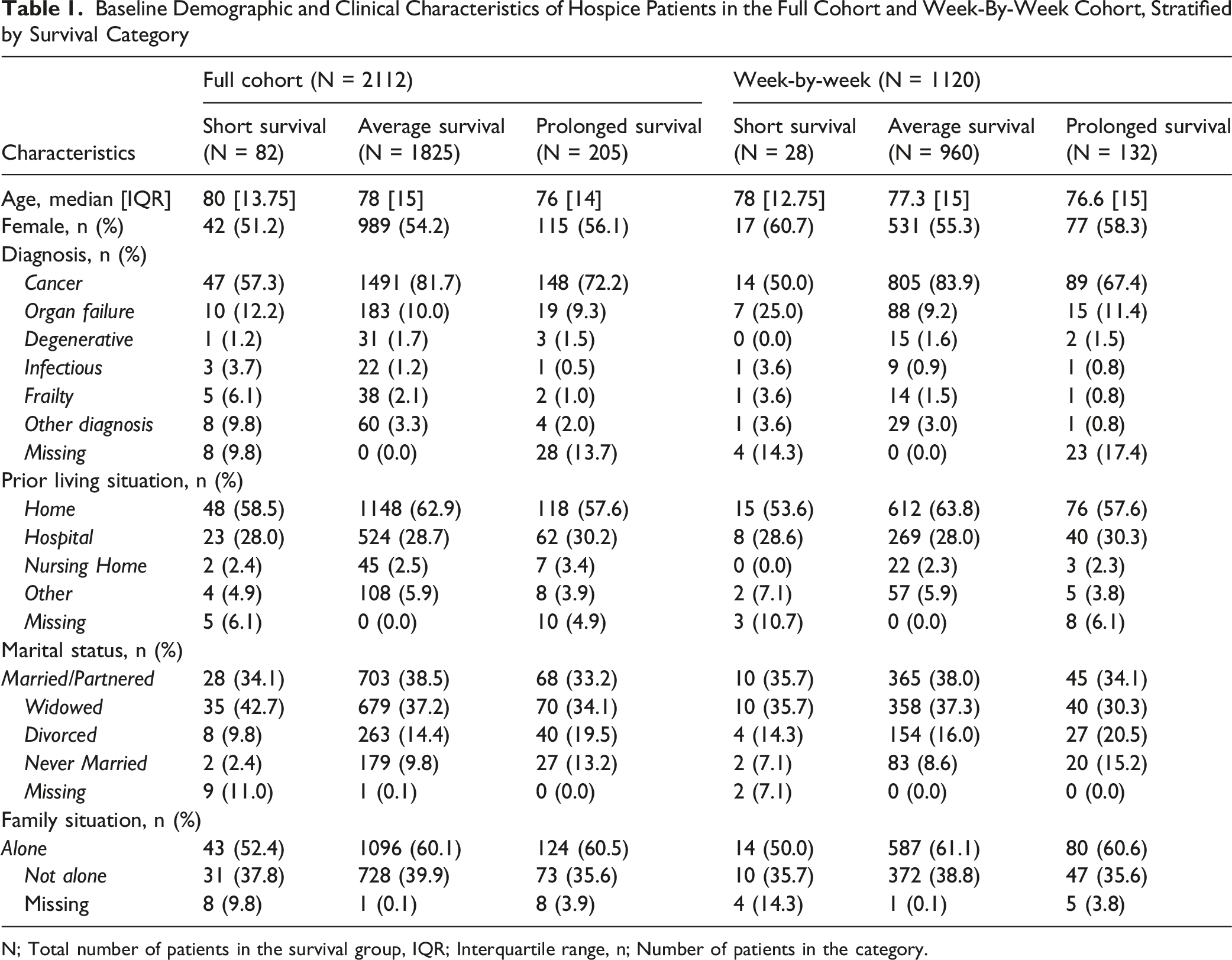
N; Total number of patients in the survival group, IQR; Interquartile range, n; Number of patients in the category.
Prevalence and Clinical Relevance of Physical and Psychological Symptoms
Prevalence (%) Reported in Percentage of Physical and Psychological Symptoms at Different Moments During the First Month of Hospice Care for Groups With Short, Average and Prolonged Survival. Prevalence Defined as a Score Greater Than 0 on the Corresponding Item of the Utrecht Symptom Diary – 4 Dimensional (USD-4D). Percentages Were Calculated Based on Available Responses per USD-4D Item and Time Point
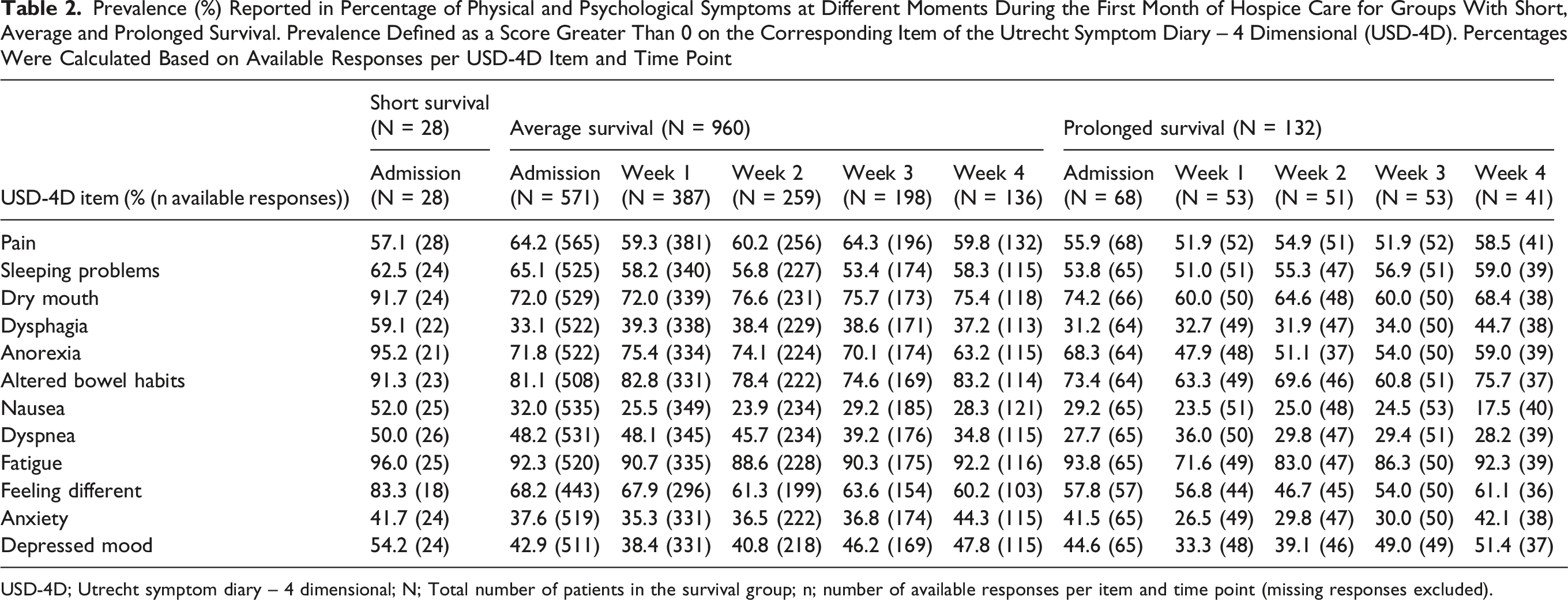
USD-4D; Utrecht symptom diary – 4 dimensional; N; Total number of patients in the survival group; n; number of available responses per item and time point (missing responses excluded).
Many symptoms had a relatively constant prevalence across all weeks, although some symptoms changed. In the prolonged survival group, the prevalence of fatigue, anorexia, and dry mouth decreased by 22, 20, and 14 percentage points, respectively, between admission and week 1. These were the only symptoms showing such a decrease. No comparable decreases were observed in the average survival group.
Clinical Relevance (%) Reported in Percentages at Clinically Relevant Level of Physical and Psychological Symptoms at Different Moments During the First Month of Hospice Care for Groups With Short, Average and Prolonged Survival. Clinical Relevance Defined as a Score Greater Than 3 on Corresponding Item of the Utrecht Symptom Diary – 4 Dimensional (USD-4D). Percentages Were Calculated Based on Available Responses per USD-4D Item and Time Point
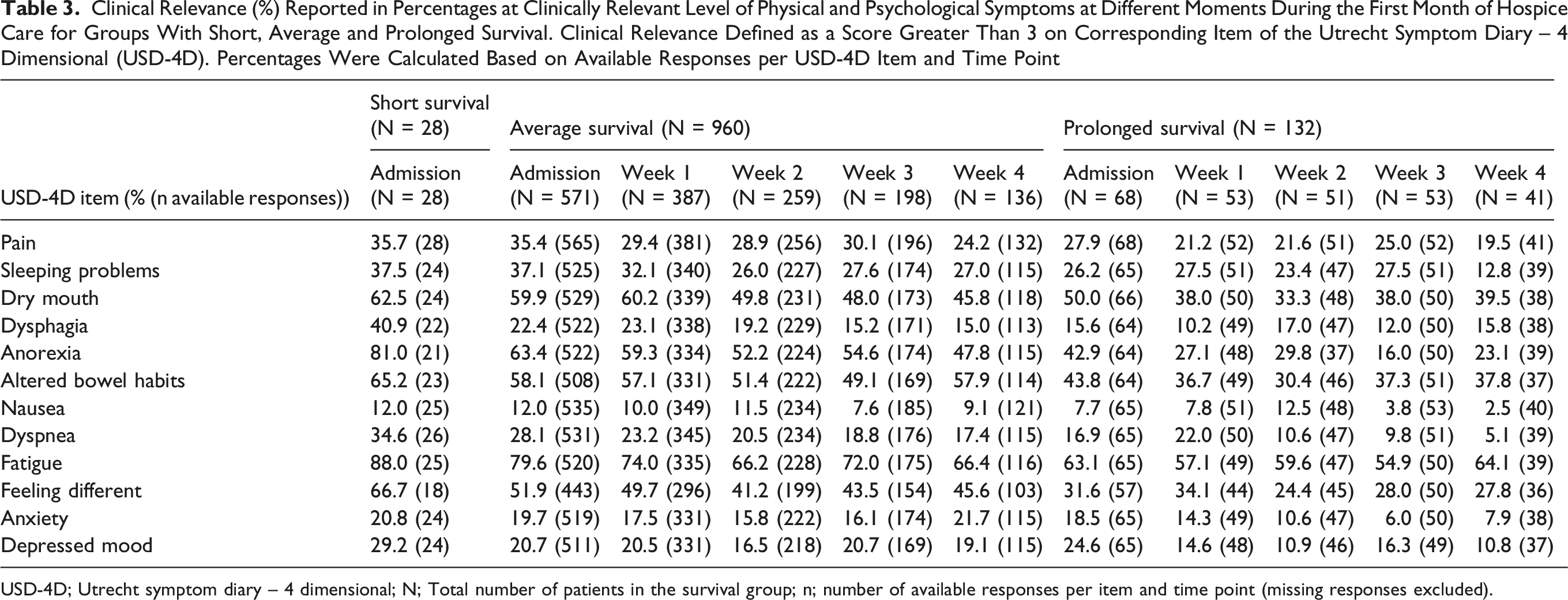
USD-4D; Utrecht symptom diary – 4 dimensional; N; Total number of patients in the survival group; n; number of available responses per item and time point (missing responses excluded).
A clear difference was observed between overall prevalence and clinical relevance. Several symptoms were frequently reported but less often clinically relevant, particularly pain, sleeping problems, and feeling different. In contrast, fatigue, anorexia, dry mouth, and altered bowel habits remained prominent when considering clinical relevance.
Intensity of Multidimensional Symptoms and Concerns
Median Item Scores of the Utrecht Symptom Diary – 4 Dimensional (USD-4D) at Different Time Points During the First Month of Hospice Care in the Short, Average, and Long Survival Groups
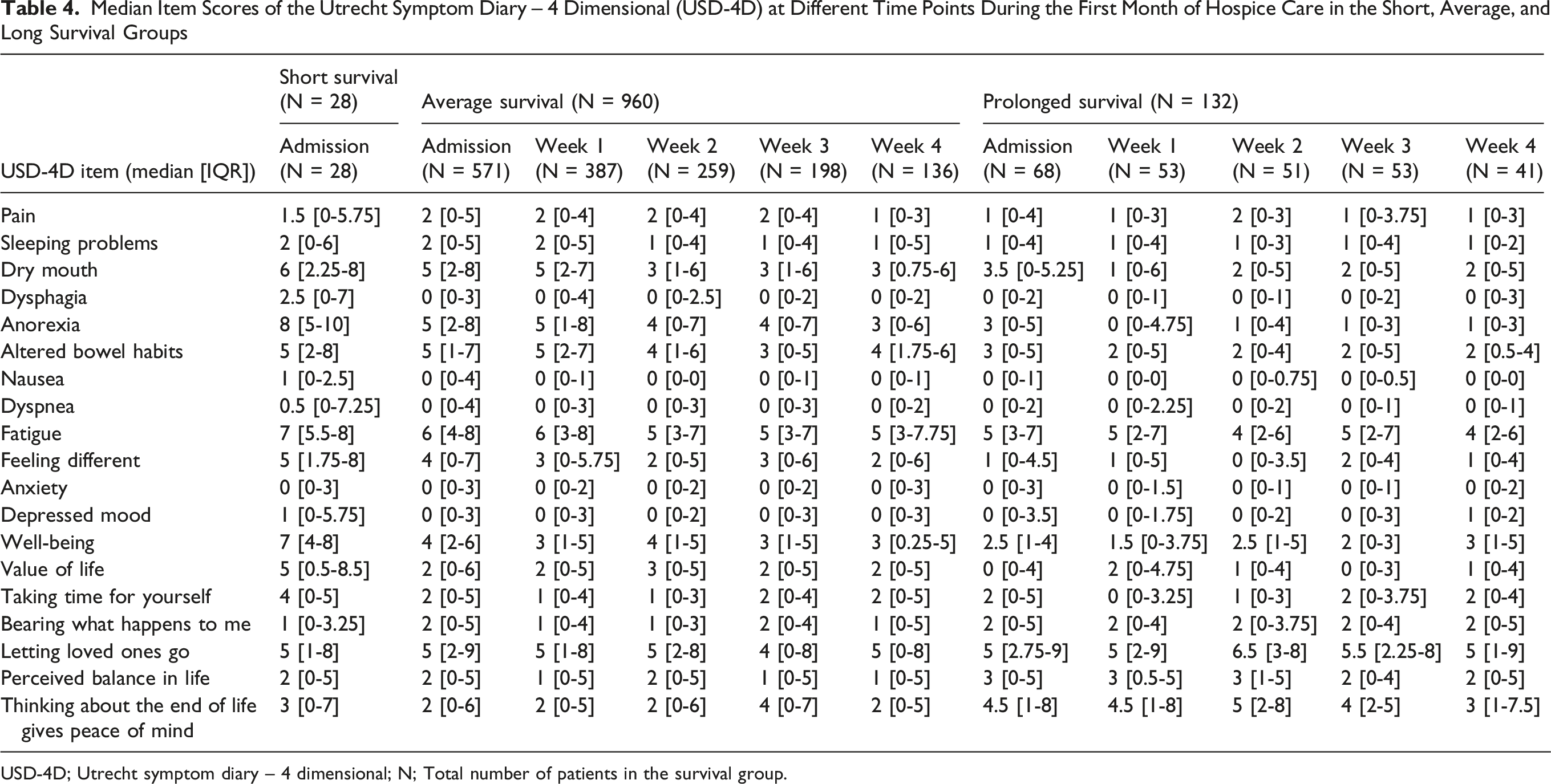
USD-4D; Utrecht symptom diary – 4 dimensional; N; Total number of patients in the survival group.
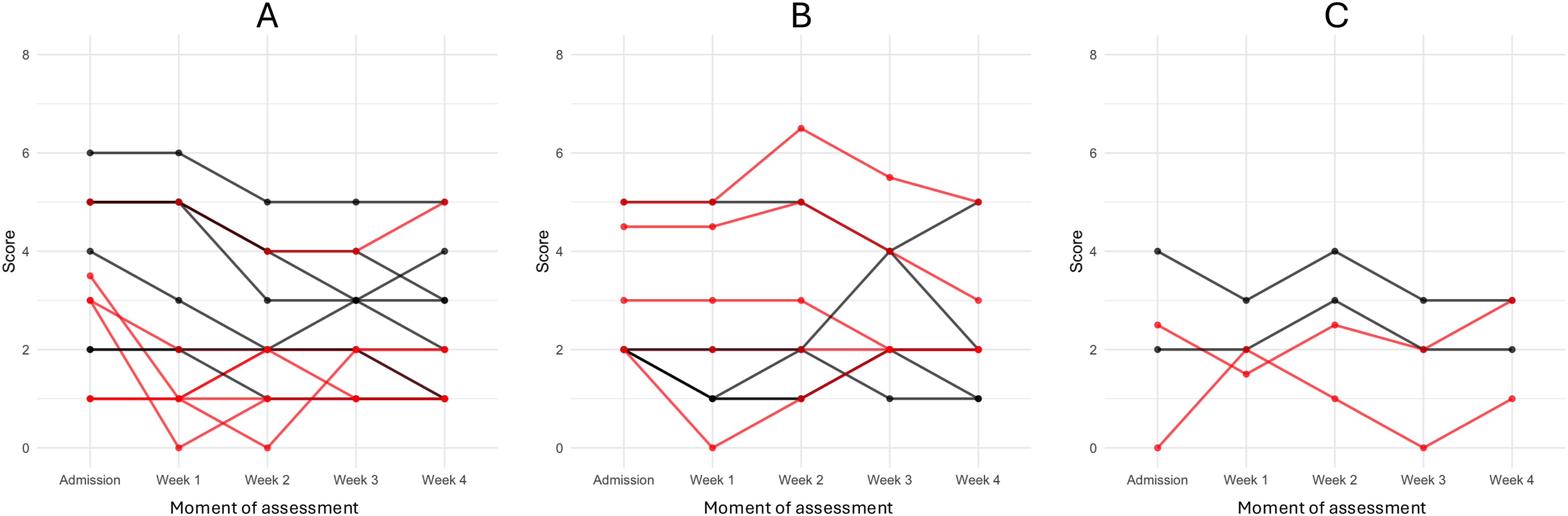
Median scores per item of the Utrecht Symptom Diary–4 Dimensional (USD-4D) at different moments during the first month of hospice care for groups with average and prolonged survival for three domains. Panel A shows physical and psychological scores, Panel B presents socio-existential scores, and Panel C represents well-being and perceived quality of life. The horizontal axis indicates the moment of assessment (Admission to Week 4), and the vertical axis represents the score. Each line reflects a median score of a USD-4D item over time. Red lines denote patients with prolonged survival (> 93 days), while black lines denote patients with average survival (3–93 days)
Overall, physical and psychological symptom scores were highest at admission in the short-survival group. During follow-up, the average survival group reported higher mean scores for many physical and psychological symptoms than the prolonged survival group. In contrast, socio-existential concerns were relatively more prominent in the prolonged survival group, with two items scoring higher than in the average survival group. ‘Letting loved ones go’ and ‘thinking about the end of life gives peace of mind’ were the socio-existential items that reached the highest scores in the prolonged survival group at any time point, while well-being and value of life remained lower in this group at admission.
Consistent with the prevalence analyses, mean scores showed a decrease in anorexia and dry mouth between admission and week 1 in the prolonged survival group. These were the only symptoms showing such a decline. After week 2, median scores remained largely stable in the prolonged survival group. In the average survival group, no similar decrease was observed, and scores showed greater variability over time.
Discussion
This study aimed to describe profiles of multidimensional symptoms and concerns in hospice patients with short, average, and prolonged survival. Comparing groups showed a clear contrast across the dimensions. Physical symptom burden was high in both the short and average survival groups. In contrast, the prolonged-survival group started with a lower burden that decreased further for up to two weeks and then stabilized. Socio-existential concerns showed a different pattern, with higher levels in the short and prolonged survival groups than in the average-survival group. Against this background, fatigue, anorexia, dry mouth, and altered bowel habits were the most prevalent and most intense symptoms across all survival groups. This is consistent with findings of previous research using the USD-4D.4,28
Previous research found that physical symptoms tend to increase towards the end of life.29-31 Among these symptoms, anorexia is particularly relevant because of its relationship with prognosis. Anorexia or poor appetite is associated with mortality risk. 32 In a study using repeated Edmonton Symptom Assessment Scale (ESAS) assessments, appetite was among the worst symptoms the week before death. 33 In the short survival group, anorexia severity was high. In the prolonged survival group, anorexia severity started lower and improved after admission, with most change occurring in the first week. This improvement was not observed in the average survival group. Improvement in appetite after initiation of hospice care has been associated with longer survival, 34 suggesting that early change in anorexia severity after admission may be a relevant observation when comparing survival groups.
This study identified two specific socio-existential concerns that were rated more severely by patients with longer survival, namely ‘perceived ability to let loved ones go’ and ‘thoughts about the end of life give peace of mind’. In the prolonged survival group, these concerns were perceived as worse on average than any physical or psychological symptoms. Research indicates that existential well-being and existential concerns are linked to outcomes for both patients and informal caregivers. Patient socio-existential distress is associated with informal caregiver decreased quality of life and increased distress, highlighting the relevance of the social system.35-38 Murray et al identified peaks in socio-existential distress at key moments in the palliative phase, including diagnosis, discharge, disease progression, and the terminal stage. 39 The higher levels of socio-existential concerns observed among patients with prolonged survival suggest that these concerns may have contributed to the decision to admit. This may point to a critical transition preceding hospice admission, although the factors driving such transitions remain unclear. In these cases, admission may initially seem appropriate, while a prolonged stay may later suggest that the trajectory did not align with the expected end-of-life course.
Strengths and Limitations
This study, to our knowledge the first, explored and compared multidimensional symptoms reported by patients with short, average, and prolonged survival trajectories in hospice care. This study examined multidimensional symptoms and concerns during the first month of hospice admission, specifically, providing insight into early signals of prolonged survival. These insights can help evaluate the suitability of hospice care, as this initial evaluation typically occurs two weeks after hospice admission.
Several limitations should be considered. First, the study was conducted within Dutch hospice care, which may differ from other countries due to regulatory and cultural factors. In particular, the 3-month cut-off used to define prolonged survival was based on Dutch regulations. Future studies should examine the clinical relevance of this threshold and identify when the symptom differences observed here begin to emerge. Second, to align with routine admission evaluation, we included only USD-4D assessments completed at or near weekly intervals when modeling symptom trajectories. While this choice increases practical relevance, it reduced the analyzable sample because assessments were often not completed at exact weekly intervals in practice, which may limit generalizability. Finally, interpretation of the short survival group requires caution due to the small subgroup size and substantial missing assessments. Missingness may be systematic if patients were too unwell to complete questionnaires, potentially biasing estimates for this group.
Clinical Implications
This study shows that profiles of multidimensional symptoms and concerns differ across short, average, and prolonged survival, with differences already evident at admission and becoming more pronounced within two weeks after admission. Although these profiles are not definitive indicators of survival duration, awareness of them may help hospice staff recognize when a patient’s trajectory differs from expectations. This may be particularly relevant in patients with prolonged survival.
Routine evaluation at two weeks after hospice admission may therefore be a suitable moment to reassess whether hospice admission remains appropriate. This evaluation should consider the patient’s multidimensional symptoms and concerns, as well as the broader care context. Patients whose admission is mainly driven by socio-existential distress may follow a different trajectory, as the factors prompting admission can improve over time with support and stabilization. As a result, continued hospice admission may not always remain the most appropriate setting, and care at home may become a feasible alternative.
The findings also highlight the need for further research into the factors underlying socio-existential distress at the time of admission. Such research should consider both the care situation before hospice admission and the support provided during the hospice stay. This could help determine whether the benefits achieved during admission could also be provided in the home setting, or whether a model of temporary hospice admission may be particularly suitable for these patients.
These findings are currently being disseminated through a national education program for hospice professionals, delivered five times annually, in which reflection on multidimensional symptoms and concerns forms a core component. The findings are also incorporated into training on the use of the USD-4D.
Conclusion
This study aimed to describe profiles of multidimensional symptoms and concerns in hospice patients with short, average, and prolonged survival, and found contrasts across dimensions during the first month after admission. The results show that symptom and concern trajectories after admission differ between survival groups and that these differences can already be observed early in the admission period. These findings suggest that hospice care needs should be understood as multidimensional and situated within a broader care context. In the Dutch context, these findings are particularly relevant given the regulatory and practical constraints on the length of hospice admissions. This underscores the importance of routine evaluation at two weeks after admission, as it captures the evolving care context during this early phase.
Supplemental Material
Supplemental Material - Exploring Multidimensional Symptoms of Hospice Patients With Different Lengths of Survival
Supplemental Material for Exploring Multidimensional Symptoms of Hospice Patients With Different Lengths of Survival by Twan Meulenbeld, Nina Stoks, Dorien Zwart, Saskia Teunissen, Everlien de Graaf in American Journal of Hospice and Palliative Medicine®.
Footnotes
Ethics Considerations
The study was conducted in compliance with the principles of Good Clinical Practice and in accordance with the principles of the Declaration of Helsinki and the General Data Protection Regulation. The Medical Research Ethics Committee Utrecht confirmed that the Medical Research Involving Human Subjects Act did not apply to this study (number 11-113/C).
Consent to Participate
All participants have been adequately informed about the use of clinical data in research during admission into the hospice. Consent was obtained digital and was documented in the patients’ electronic health record. Only data of patients who gave consent was used in this study.
Consent for Publication
With consenting to participate to this research, all participants consented to the publication of the results of this research.
Author contributions
Twan Meulenbeld: Formal analysis; Writing – original draft; Writing – review & editing. Nina Stoks: Formal analysis; Methodology; Writing – review & editing. Saskia Teunissen: Conceptualisation; Writing – review & editing; Funding acquisition; Resources; Supervision. Dorien Zwart: Resources; Writing – review & editing. Everlien de Graaf: Conceptualisation; Project administration; Formal analysis; Methodology; Writing – review & editing; Supervision.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the Cini de Wind foundation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Primary data used in this research can be acquired by contacting the last author of this paper.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.