
Abstract
Background
Palliative care is an essential component of high-quality cancer care; however, limited research has examined the multilevel barriers to and facilitators of social workers’ ability to deliver palliative care for patients with cancer. Guided by ecological systems theory, this qualitative study identifies such barriers and facilitators perceived by social workers providing palliative cancer care in the United States.
Methods
Using an exploratory qualitative design, we conducted semi-structured Zoom interviews with 10 social workers practicing in palliative cancer care settings. We identified themes in participant responses using reflective thematic analysis and interpreted those themes within an ecological systems framework.
Results
Participants identified barriers and facilitators across societal, organizational, interpersonal, and individual levels. Societal barriers included stigma, misunderstandings about palliative care, and financial constraints, whereas integration into care teams and continuity across care settings facilitated coordinated care. Organizational barriers included excessive workload demands and delayed referrals; social workers’ community connections facilitated enhanced resource access and care coordination. Interpersonal barriers centered on unclear role delineation, while interprofessional collaboration, proactive role education, and positive patient experiences strengthened social work practice in palliative care settings. At the individual level, insufficient role preparation and administrative burden constrained patient-centered care; however, a strong sense of professional meaning and clinical competence supported social workers’ practice in these settings.
Conclusion
Enhancing role clarity, palliative care education, interprofessional collaboration, and organizational support may strengthen social workers’ integration within palliative care settings and advance person- and family-centered cancer care.
Keywords
Introduction
Palliative care is an essential component of high-quality cancer care, 1 aimed at addressing the physical, psychological, social, and spiritual needs of patients with cancer and their families across the disease trajectory to enhance quality of life. 2 Despite its growing integration into cancer care, palliative care is often misunderstood and conflated with hospice care. Hospice care is typical intended for patients in the final phases of illness when curative treatment is no longer the primary focus. In contrast, palliative care can be provided at any stage of cancer and provided alongside curative or life-prolonging treatments. Growing evidence demonstrates that integrating palliative care into early stage of cancer care can improve patients’ symptom management, 3 quality of life, 4 satisfaction with care, 5 and use of health care-related resources. 6 As integral members of interprofessional palliative care teams, 7 social workers provide specialized psychosocial care as identified by the U.S. National Palliative Care Guidelines. 2 However, social workers are often excluded from debates regarding which psychosocial services are most essential to effective palliative care, 8 and limited evidence has documented the key outcomes and effectiveness of social workers’ contributions in this field to date. 9
Although prior studies have delineated the present roles and capacities of social workers in palliative care in the U.S.,10,11 less attention has been paid to the barriers of and facilitators to effective practice that they encounter in these settings, particularly when working with patients with cancer. International studies have already identified barriers to social work practice in palliative care, including role ambiguity, limited resources, and systemic constraints12,13; however, it remains unclear how these barriers manifest within the U.S.’s distinct healthcare structures and practice environments, thereby preventing U.S. policymakers and administrators from optimizing social workers’ contributions to palliative care by leveraging the latest available evidence.
Ecological systems theory 14 conceptualizes professional practice as a domain shaped by multiple interacting levels of influence, including individual, interpersonal, organizational, and societal systems. Understanding the multilevel barriers and facilitators that shape social work practice – both within and across professional contexts – is an essential prerequisite for strategically guiding workforce development, institutional policy, and interprofessional collaboration. As a step toward filling this knowledge gap via a qualitative study grounded in ecological systems theory, 14 we examined the perceived multilevel barriers and facilitators faced by social workers providing palliative care to patients with cancer in the United States.
Methods
Study Design
We used an exploratory qualitative design to identify the perceived barriers and facilitators among social workers providing palliative cancer care in the United States. This study was reviewed and approved by the Syracuse University Institutional Review Board.
Participants and Recruitment
Participants were recruited using convenience sampling through an announcement sent via a national listserv managed by the Social Work Hospice and Palliative Care Network and through a local cancer center. Inclusion criteria included: (1) being a social worker currently practicing with cancer patients in the United States; and (2) engaging in the provision of palliative care.
Data Collection
From November 2023 to January 2024, two team members with social work backgrounds conducted semi-structured interviews via Zoom using an interview guide (available in Supplement 1). Interview questions included “What are some of the challenges you face as a social worker in your practice setting (personal barriers, institutional barriers)” and “How have you overcome these challenges? What are a few examples?” Individual interviews lasted from 18 to 43 min, with a median duration of 32 min. All participants provided informed oral consent before participating and received a $30 Amazon e-gift card upon completion of the interview.
Data Analysis
Interviews’ audio recordings were automatically transcribed using Zoom, and three team members reviewed all transcripts for accuracy and completeness. We then analyzed the data using reflective thematic analysis.15,16 Data were coded and analyzed using inductive and deductive approaches. First, four team members independently familiarized themselves with the data and generated initial codes inductively. The full team then compared codes, refined the codebook, and consolidated codes into overarching themes. To strengthen methodological rigor and trustworthiness, we held regular debriefing meetings to examine interpretations, as well as ongoing reflexive discussions to address potential biases. Themes were then defined, refined, and classified deductively into barriers or facilitators operating at societal, organizational, interpersonal, and individual levels (Figure 1). Multilevel barriers and facilitators of social work practice in palliative cancer care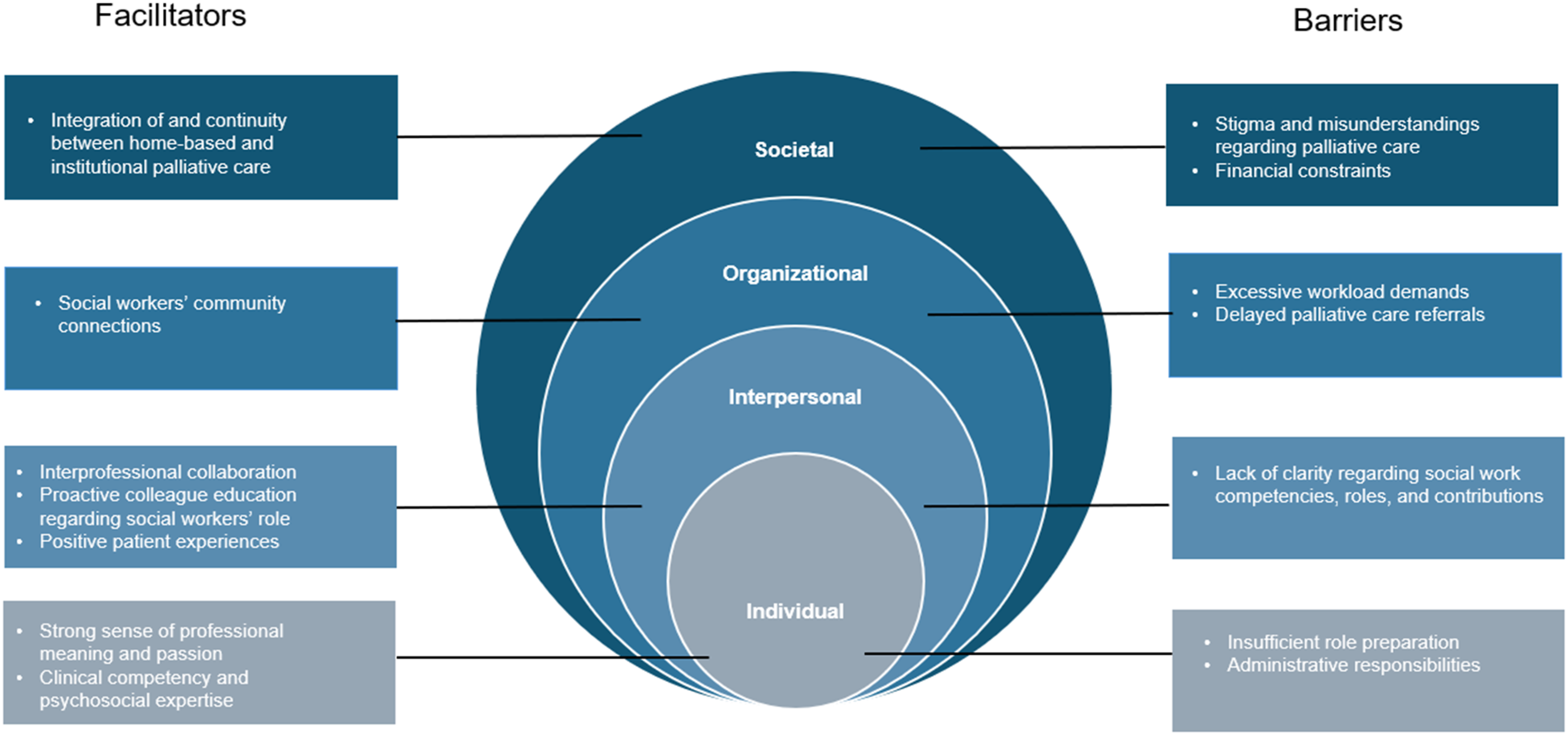
Results
Participants
Ten social workers working in palliative cancer care were interviewed, including eight clinical social workers and two in supervisory roles. Eight participants provided demographic information. Among them, 63% were more than 50 years old; these participants were predominantly female (88%) and White (63%). Additionally, 88% held full social work licenses (eg, Licensed Master Social Worker, Licensed Clinical Social Worker), and 25% had advanced palliative and hospice social work certification (APHSW-C). Participants reported working in their current roles for between 2 and 40 years.
Barriers to Palliative Social Work Practice
Societal Barriers
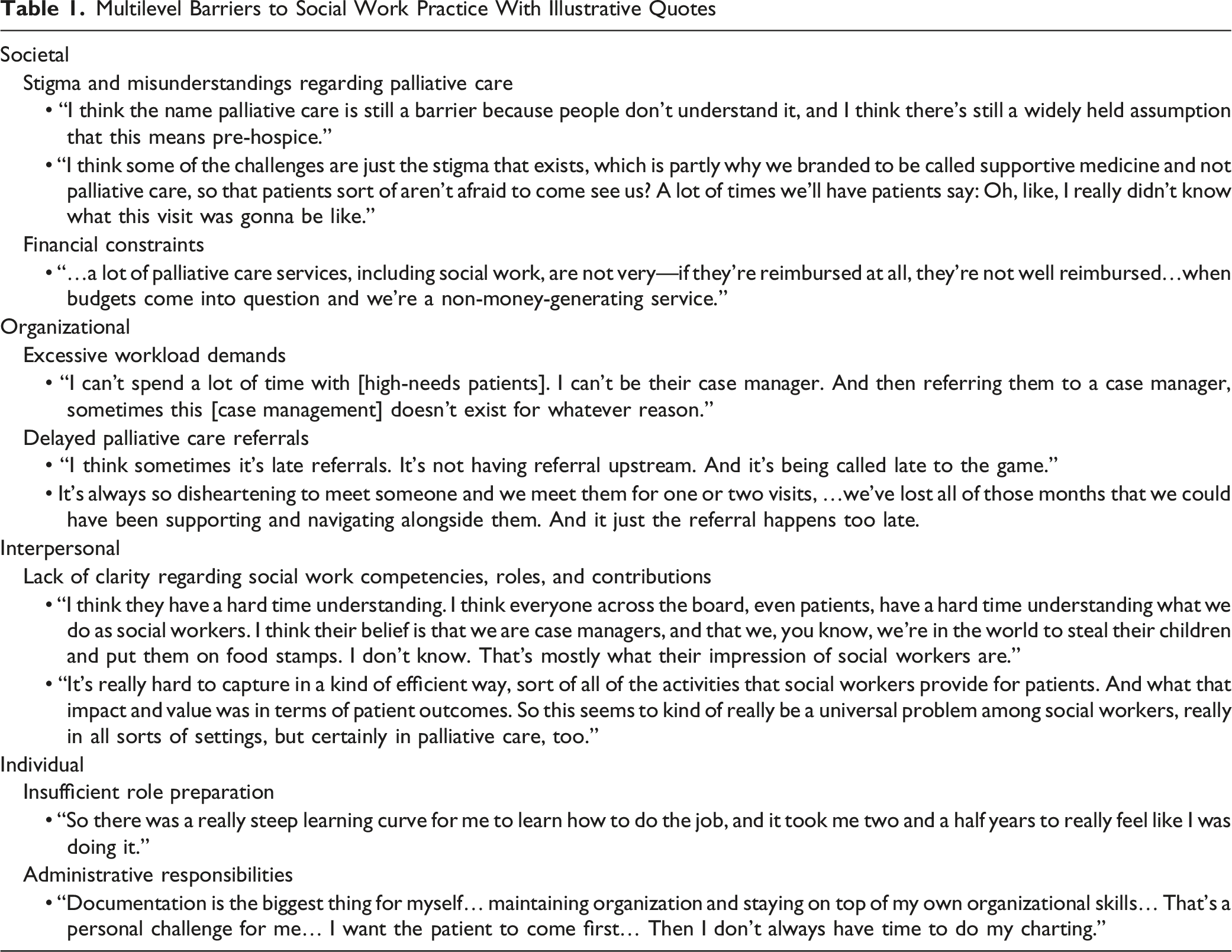
Multilevel Barriers to Social Work Practice With Illustrative Quotes
Organizational Barriers
The two most salient organization-level barriers included excessive workload demands and delayed palliative care referrals. Regarding workload demands, one participant explained, “I can’t spend a lot of time with [the high needs patients]. I can’t be their case manager. And then referring them to a case manager, sometimes this [case management] doesn’t exist for whatever reason.” Participants reported that limited resources and insufficient staffing directly affected their ability to care for patients and deliver services and emphasized that late or absent referrals further hindered their ability to provide adequate support. One participant attributed frequent referral delays to “not having referral upstream. And […] being called late to the game.” Indeed, several participants expressed that, without timely referrals, they often became involved in a patient’s care plan too late to offer meaningful services before patients required hospice care.
Interpersonal Barriers
Participants described a lack of clarity among patients regarding social workers’ competencies, roles, and contributions, which created interpersonal challenges when participants attempted to explain social workers’ functions on care team. One participant noted that patients often held narrow or inaccurate perceptions of social work, frequently equating social workers with case managers or associating them with negative stereotypes, such as believing they are “in the world to steal their children and put them on food stamps”. These misconceptions impeded social workers’ ability to effectively communicate the full scope of their practice to patients. One participant further emphasized that even other health care providers often have a limited understanding of the full scope of social workers’ roles, particularly their capacity to provide therapeutic interventions. This lack of role clarity can delay referrals and restrict social workers’ ability to engage patients and families early in the care trajectory. As the participant explained, physicians and nurses sometimes assume that “only the psychologists can provide the therapy,” reflecting a misconception that narrows perceptions of social work practice and, in turn, limits opportunities for comprehensive psychosocial support.
Individual Barriers
Participants identified individual-level barriers related to insufficient role preparation and the challenge of managing administrative demands. One participant described a “steep learning curve” in the profession, noting it took them more than two years to feel confident as a social worker serving in palliative care settings. Others emphasized the challenge of balancing documentation requirements with patient care, with one stating, “Documentation is the biggest thing for myself… I want the patient to come first, and I spend so much time [with documentation].” Their experiences illustrate a continual tension between social workers’ administrative workload and patient-centered practice.
Facilitators of Palliative Social Work Practice
Societal Facilitators
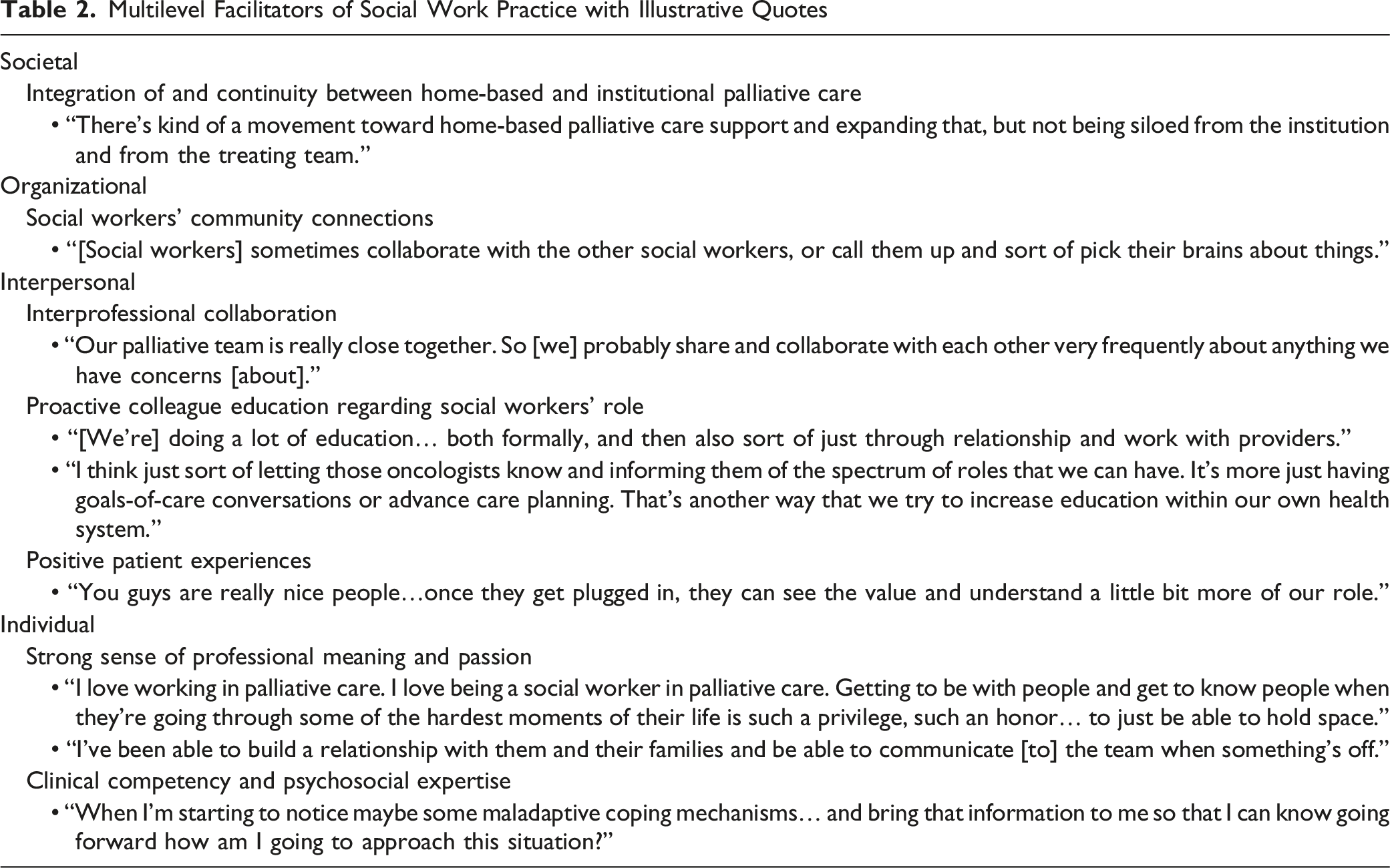
Multilevel Facilitators of Social Work Practice with Illustrative Quotes
Organizational Facilitators
Social workers’ community connections reportedly served as valuable resources for accessing local knowledge and coordinating services. For example, one participant described drawing on colleagues’ experience working in nursing homes and assisted living facilities, noting that they often “collaborate with other social workers or call them up and pick their brains about things.”
Interpersonal Facilitators
Participants noted that close collaboration among multidisciplinary team members in palliative care facilitated palliative social work practice and further emphasized that this practice was strengthened by social workers’ proactive education of colleagues regarding their broad scope of practice. One participant described the benefits of “letting those oncologists know and informing them of the spectrum of roles that we can have. It’s more just having goals-of-care conversations or advance care planning. That’s another way that we try to increase education within our own health system.” In addition, positive patient experiences reinforced the value of social work involvement. As one participant shared, patients often initially expressed apprehension but later reflected, “You guys are really nice people… once they get plugged in, they can see the value and understand a little bit more of our role.”
Individual Facilitators
At the individual level, participants described a strong sense of professional meaning and passion for their work as key facilitators of their practice in palliative cancer care. Many characterized their work as a privilege and emphasized the importance of “holding space” for patients and families during difficult moments. As one participant noted, “I love working in palliative care […], it’s such a privilege, such an honor […] to just be able to hold space.” Clinical competence and psychosocial expertise also emerged as salient practice facilitators, with participants describing their ability to identify maladaptive coping and relational shifts. For example, one participant reported “starting to notice maybe some maladaptive coping mechanisms” in a patient and adjusting their approach accordingly. Together, these qualities facilitated participants’ integration within interdisciplinary teams and strengthened patient-centered care.
Discussion
Guided by ecological systems theory, this study identified barriers and facilitators across societal, organizational, interpersonal, and individual domains among social workers providing palliative cancer care. Although the benefits of integrating palliative care at early stage of cancer care are well established, our findings indicate that palliative care often occurs late in the cancer trajectory, creating substantial barriers to effective social work practice by limiting social workers’ ability to engage earlier in the care trajectory and provide comprehensive psychosocial support. Such delays are frequently linked to patients’ and caregivers’ lack of awareness of and misconceptions about palliative care. For example, only a small fraction of U.S. adults reports having accurate knowledge of palliative care, with national survey data showing that approximately 89% of respondents have an inadequate understanding of palliative care and that many automatically associate it with death or hospice care. 17 Additionally, oncologists’ misconceptions about palliative care are related to late referrals to that care. Indeed, national survey of oncologists revealed that only 17% refer patients to palliative care once they have received a metastatic cancer diagnosis, while 10% reported offering referrals only at patients’ end of life. 18 These low or delayed referral rates are partly driven by oncologists’ concerns that patients may equate palliative care with end-of-life or hospice care, leading to distress or diminished hope.19,20 Addressing this gap will require strategies that promote earlier integration of palliative care within oncology and clarify its value beyond end-of-life care. Improved interdisciplinary understanding – particularly of social workers’ psychosocial expertise and scope of practice – may facilitate more timely referrals and sustained engagement across the cancer care continuum.
Unclear role definitions and misunderstandings of social work by other team members hindered social worker participants’ ability to leverage their full professional skill set in palliative cancer care settings. This finding is consistent with prior findings on social work within multidisciplinary health teams 21 as well international studies of palliative care social work.12,13 Our prior study found that social workers in palliative cancer care play a multifaceted role in supporting patients and families, including addressing psychosocial needs, facilitating communication, and supporting decision making across the cancer trajectory. 22 Similarly, O'Donnell and colleagues’ study found that physicians, nurses, chaplains, and other members of palliative care teams viewed social workers as essential contributors to patient-centered care, recognizing their expertise in psychosocial assessment, family support, communication facilitation, and care coordination. 23 However, the breadth and variability of social work practice in palliative care present both a strength and a challenge. While this flexibility allows social workers to respond effectively to complex patient and family needs, it can also impede palliative care social workers’ ability to clearly articulate and justify their roles to patients or fellow care team members. 24 In addition, this lack of role clarity may limit other disciplines’ ability to fully recognize social work as a source of distinct value within interprofessional teams, 25 rather than perceiving it as a “blurred profession”. 21 Consistent with this concern, Giamportone’s qualitative study of physicians, nurses, and social workers found that role confusion, inconsistent expectations across professions, and limited awareness of social workers’ competencies hindered the effective integration of social workers within healthcare teams. 26 As a result, social workers may be considered “able to do anything” yet remain overlooked by team members and organizational leadership. 21 When social workers lack a clearly defined role, they risk being underutilized and excluded from early involvement. These dynamics can lead to delayed or fragmented psychosocial support, weakened interdisciplinary collaboration, and heightened professional strain, ultimately compromising the quality and equity of palliative cancer care.
While identifying these persistent multilevel barriers to high-quality palliative care social work practice, our study also identifies opportunities to address them. The strong integration of and continuity between home-based and institutional palliative care, facilitated by coordinated communication, is a crucial facilitator of effective palliative social work practice and enhances patient and caregiver experiences and health outcomes. Palliative care’s interprofessional and collaborative nature enhances social work practice by fostering holistic, team-based approaches to addressing the complex physical, emotional, social, and spiritual needs of cancer patients and families. At the same time, our findings join prior studies in emphasizing that facilitating social work practice in palliative cancer care requires proactively educating both patients and providers (eg, oncologists) to clarify different professions’ roles, responsibilities, and core competencies. 9
However, the work of optimizing social workers’ contributions to palliative care settings far precedes social workers’ interactions with patients or other providers in those settings. Social work education programs should intentionally integrate palliative care into their curricula to strengthen students’ competencies in palliative care settings. Beyond receiving training in foundational psychosocial assessment and support, students need to be prepared to facilitate goals-of-care discussions, engage in advance care planning, and navigate end-of-life care conversations associated with serious illness-all essential competencies for effectively serving patients in palliative care. Students must also be equipped to function effectively within interprofessional teams. Interprofessional education (IPE) interventions – defined as educational approaches in which “students from two or more professions learn about, from, and with each other” 27 – offer a promising, structured mechanism to build this competency. A robust body of literature substantiates IPE’s value and its association with enhanced team communication, 28 greater collaborative practice readiness, and improved patient outcomes. 29 Educators can further enhance future social workers’ preparedness for interprofessional palliative care settings through seminars, workshops, and case-based learning experiences. Incorporating serious illness-focused case simulations, IPE-based learning opportunities, and palliative care-focused field placements may further build clinical confidence and strengthen professional identity among future social workers in palliative cancer care.
The strength of this study is its grounding in ecological systems theory, which structured our comprehensive examination of the individual, interpersonal, organizational, and societal factors that both enable and constrain social workers providing palliative cancer care in the United States. However, this study exclusively analyzes social workers’ self-reported perspectives. Although social workers provided valuable insights into the barriers to and facilitators of their practice in palliative care settings, the study did not include viewpoints of other interprofessional team members. Future research should incorporate the perspectives of additional key stakeholders – including oncologists, palliative care physicians, and nurses – to develop a more comprehensive understanding of the multilevel barriers and facilitators influencing social work practice in palliative cancer care and develop solutions that improve service delivery and coordination across all care team members.
Conclusions
This study provides valuable insights into the multilevel barriers and facilitators encountered by social workers in palliative cancer care in the United States. As social workers will continue to play essential roles serving clients in this setting, care systems, policymakers, and educational institutions must pursue initiatives to strengthen social work’s integration within palliative cancer care. By achieving clearer role delineation, ongoing palliative care education among patients and families, enhanced interprofessional collaboration, and organizational support to address structural and workflow-related barriers to palliative social work practice, these efforts will help optimize the delivery of person- and family-centered palliative cancer care.
Supplemental Material
Suppplemental Material - Multilevel Barriers and Facilitators of Social Work Practice in Palliative Cancer Care
Suppplemental Material for Multilevel Barriers and Facilitators of Social Work Practice in Palliative Cancer Care by Ting Guan, Jamie Hill, Xiafei Wang, Karlynn BrintzenhofeSzoc in American Journal of Hospice and Palliative Medicine®
Footnotes
Acknowledgements
We would like to acknowledge the Social Work Hospice and Palliative Care Network for assisting with participant recruitment. We also thank all participating social workers for their time and valuable contributions to this study. In addition, we thank research assistants Ava Marion Henderson, Shameem Varikkodan, and Sadaf Sedaghatshoar for their support with data collection, data cleaning, and analysis. We also extend our gratitude to Jordan Wingate for his editorial assistance.
Ethical Considerations
This study was approved by Syracuse University’s Institutional Review Board (Protocol # 23-266).
Consent to Participate
All participants provided informed oral consent before participating in the study.
Author Contributions
TG and KB designed the study. TG, JH, XW, and KB analyzed the data. All authors interpreted the data. TG, JH, and XW drafted the manuscript. All authors contributed to revisions and approved the final manuscript.
Funding
This work was supported by funds provided by the David B. Falk College of Sport and Human Dynamics, Syracuse University.
Declaration of Conflicting Interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data are currently being used for other studies and manuscript development. Data supporting the findings of this study may be made available upon reasonable request, with permission from the researchers who collected the data.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.