
Abstract
Background
People with cancer often experience strong emotions at the time of diagnosis and when informed that their cancer has metastasized. Whereas the expression of emotions is often healthy, the fear of emotional expression can impede adaptation by undermining motivation and social support and contributing to pain and somatic symptoms.
Aim
This study aimed to assess the relevance of fear of emotional expression to cancer-related pain and somatic complaints, particularly as the disease progresses.
Design
This cross-sectional secondary analysis examined the association between fear of emotional expression and somatic symptoms. Moderation analysis tested whether the association between fear of emotional expression and somatic symptoms was more pronounced among patients with metastatic cancer than among patients with remitted or localized cancer.
Setting/Participants
Data were collected online from 633 participants with remitted, localized, and metastatic cancer diagnoses.
Results
Models indicated significantly stronger associations between fear of emotional expression and somatic symptoms among patients with metastatic cancer compared to those with localized or remitted cancer. These results held after adjusting for depression and other putative confounders.
Conclusions
Taken together, these findings suggest that difficulties expressing emotions could impede quality of life if physical manifestations of stress layer upon other metastatic cancer-related symptoms and side effects.
Patients with cancer experience fear, sadness, and anger,1,2 and may find benefit in expressing emotions throughout the cancer continuum from diagnosis to palliative care and survivorship.1,3,4 Expressed emotions can be better understood, soothed, and harnessed so that individuals can pursue their needs for safety, closeness, and dignity, whether in the context of personal relationships, psychotherapy, or supportive care.1,5,6 Indeed, expression of emotion appears to be a critical mechanism of action across psychosocial treatments.7,8 Although emotional expression can be valuable for dealing with the many emotions triggered by serious illness,3,9,10 individuals vary greatly in the degree to which they express emotions, and some people experience substantial fear of disclosing or expressing such feelings to others.11-13 Rigid avoidance of emotional expression is linked to physical manifestations of stress, such as pain and fatigue, and overcoming such avoidance can ease physical symptoms including chronic pain.14-16 However, the linkages between emotional expression and somatic symptoms are understudied among patients with cancer, particularly as the disease metastasizes and its emotional impact becomes more salient, 17 while distressing symptoms such as pain, fatigue, and nausea often grow in intensity.
Emotional expression is one facet of broader and highly contextualized emotional regulation processes that are shaped across the decades of development preceding an adult cancer diagnosis.18,19 In some cases, salient high-stress events and psychological trauma couple with punitive responses of others to cultivate fears that expressing emotions will result in a loss of control over one’s emotions or lead to rejection or abandonment by others.20-22 In other cases, emotional suppression may unfold more subtly when familial or cultural norms discourage expression of normative distress.23,24 Individuals who habitually suppress emotional expression to manage these fears are vulnerable to psychiatric symptoms such as depression and PTSD.6,14,25 Furthermore, analysis of emotional suppression in the laboratory and daily life provides strong evidence that withholding emotional expression augments pain and physical symptoms.14-16,26,27 There is debate as to how this occurs; for example, emotional non-expression may activate fear-based pain neural circuitry, or lead to preferential attention to somatic rather than emotional experiences, or stimulate the sympathetic nervous system, creating peripheral changes.6,8,18,26,28 Regardless of the underlying mechanism, people who are fearful about confronting their emotional reactions to stressful cancer-related experiences may be less inclined to attend to and express the somatic symptoms of their distress and illness.
Although understudied, the fear of emotional expression likely complicates the management of cancer-related symptoms and treatment side effects such as pain, fatigue, and nausea. Drawing from the literature on avoidance and denial in cancer, cancer status may be key to understanding the impact of emotional expression on these physical complaints. 29 During the early stages of cancer, such as work-up, diagnosis, and initial treatment, the tendency to minimize, avoid, or inhibit emotional expression could be adaptive for sustaining routines and role performance. By contrast, the emotional impact of cancer metastasis may be driven by a heightened salience of mortality and accompanying perceptions of unfinished business, particularly as curative outcomes become less likely.17,30 At this stage of illness, fear of expressing one’s feelings could impede the processing of other fears surrounding mortality and undermine opportunities to discuss and shape one’s legacy.10,30 At a more practical level, individuals also tend to become increasingly dependent upon the support of others as cancer progresses, and fears of emotional expression may undermine the ability to assert one’s independence and needs. 3 The increased intensity and urgency of emotion as cancer advances, combined with a fear of expressing them, could contribute to physical symptoms such as pain, fatigue, and nausea, which patients often feel safer disclosing to others.
This analysis aimed to understand the intersection of fear of emotional expression, cancer status, and somatic symptoms in a large sample of individuals with varied cancer histories. It was hypothesized that fear of emotional expression would be associated with more somatic symptoms, and that this association would be stronger among participants with metastatic disease than those with localized cancers or cancers in remission. Furthermore, it was hypothesized that the association of fear of emotional expression and somatic symptoms in patients with advanced disease would remain after accounting for plausible confounders such as gender, disease site, and depressive symptoms. These hypotheses were tested using a series of moderation analyses. Evidence of moderation by cancer status would suggest that metastatic cancer constitutes a unique context that may amplify the association between fear of emotional expression and somatic symptoms.
Methods
Participants
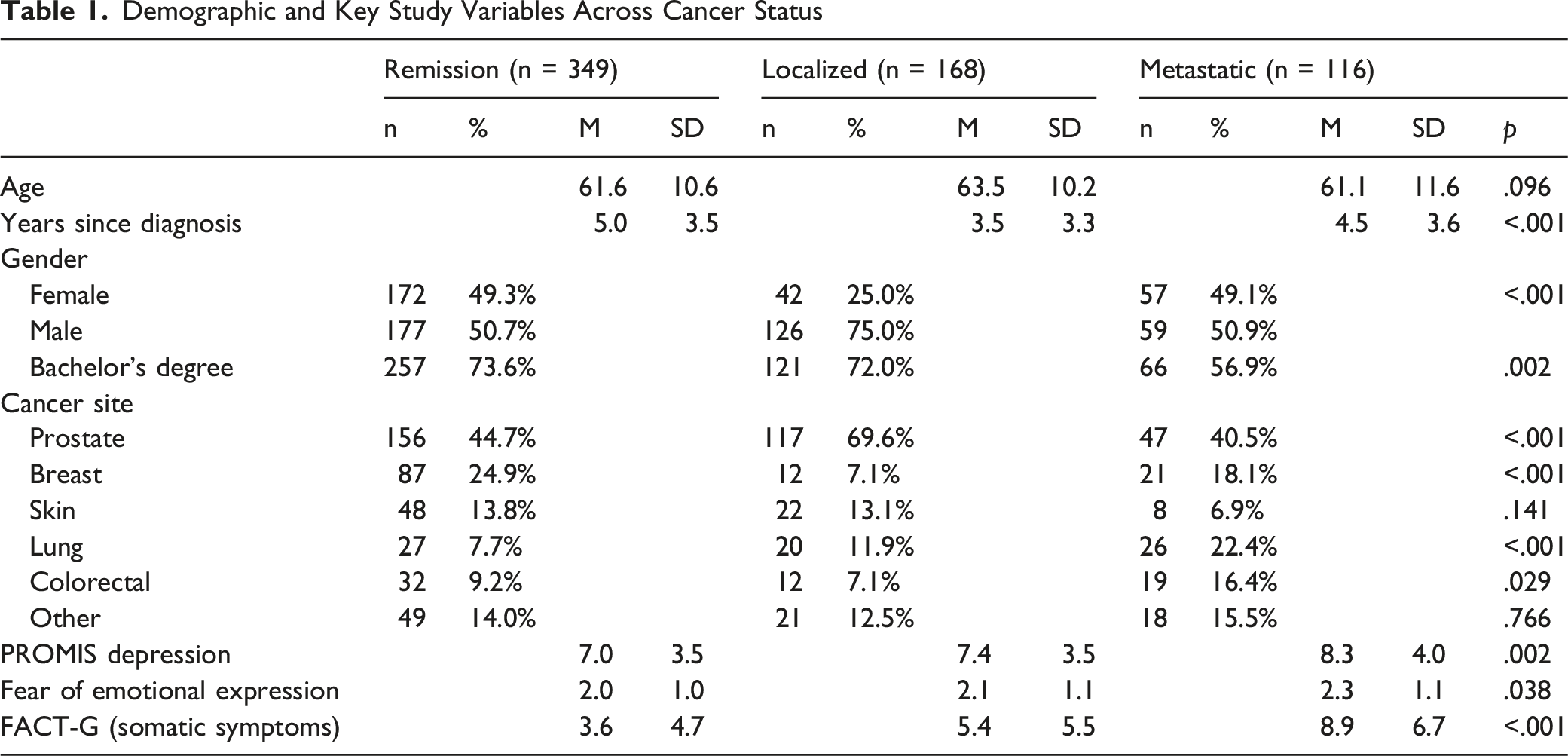
Demographic and Key Study Variables Across Cancer Status
Measures
Statistical Analyses
Descriptive statistics, bivariate correlations, and regression models were computed using SPSS version 28. The primary study hypothesis was tested using the PROCESS Macro. 34 Model 1 was used to test the interaction of fear of emotional expression and cancer status in predicting somatic symptom scores. Fear of emotional expression was entered as a continuous predictor, and cancer status was entered as a categorical predictor with categories for cancer in remission, localized disease, and metastatic disease. The predictors and their interaction were entered into an unadjusted model and a fully adjusted model. In these models, an interaction term coefficient with a probability value below .05 was considered evidence of a significant interaction. Significant interactions were then characterized by computing and plotting the simple slopes for fear of emotional expression with somatic symptoms across each of the 3 cancer statuses. These steps were repeated after adjusting for plausible confounders of age, gender, education (ie, yes/no college degree), cancer type, time since diagnosis, and depression that might account for the relationship between fear of emotional expression and somatic symptoms.
Results
Analysis of variance revealed differences in demographic characteristics and key study variables across cancer status groups (See Table 1). Participants with different cancer statuses differed in depression (F(2,630) = 6.11, P < .01), fear of emotional expression (F(2,630) = 3.30, P < .01), and somatic symptom scores (F(2,630) = 43.62, P < .05). Participants with metastatic disease reported higher levels of depression compared to participants in remission (P = .005), but not participants with localized disease (P = .148). Participants with metastatic disease reported greater somatic symptoms (M = 8.9 SD = 6.7) than participants with localized disease (M = 5.4 SD = 5.5, P < .001), who in turn reported greater somatic symptoms than participants with cancer in remission (M = 3.6 SD = 4.7, P < .001). Although the 3 cancer status groups differed fear of emotional expression, post-hoc comparisons did not reveal specific significant group differences.
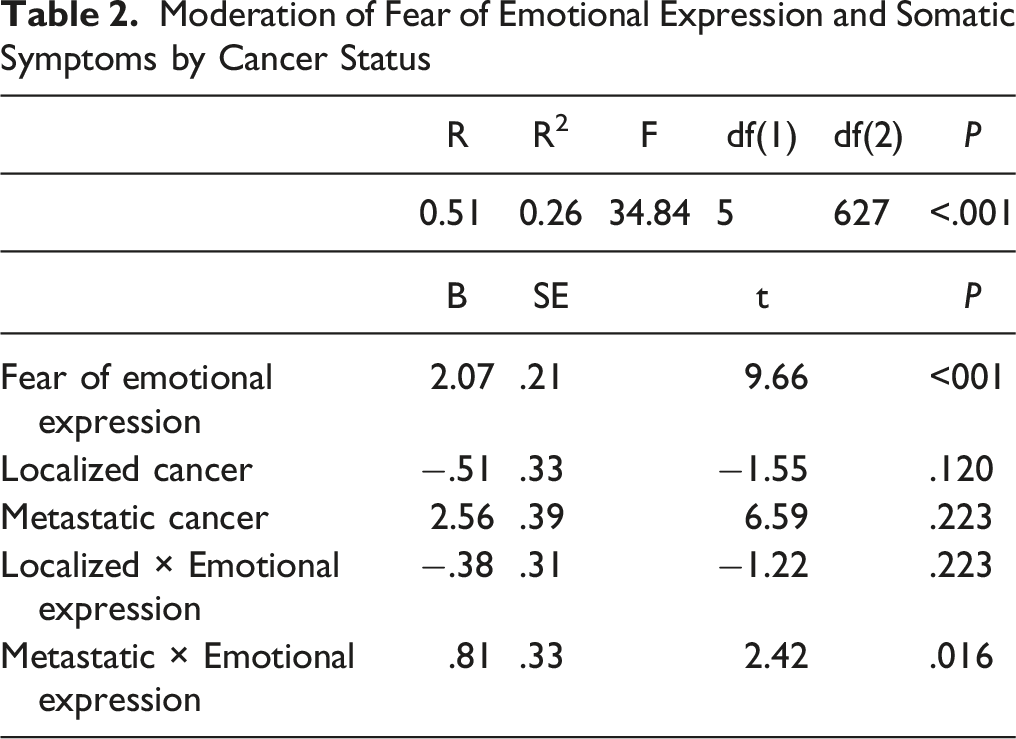
As hypothesized, fear of expressing emotions was positively related to higher somatic symptom scores (r = .39, P < .001) for the full sample. Results of moderation tests were consistent with the hypothesis that fear of emotional expression would be most strongly related to somatic symptoms among participants with metastatic disease. In the initial unadjusted model, fear of emotional expression interacted with disease status to predict higher somatic symptom scores (R2 Change = .01, F(2, 627) = 3.07, P = .047; see Figure 1). Although the slope of association between fear of emotional expression and somatic symptoms was significant for all 3 cancer statuses, the association was substantially stronger among participants with metastatic disease (B = 2.88 SE = 0.44, P < .001), than among those with localized disease (B = 1.70 SE = 0.38, P < .001), or those with cancer in remission (B = 1.64 SE = 0.27, P < .001). Thus, as expected, fear of emotional expression was positively associated with more somatic symptoms across cancer status, but the association was strongest among patients with metastatic cancer. Interaction plot of the unadjusted moderation model. Fear of emotional expression is more strongly positively associated with somatic symptom burden (FACT-G) among people with metastatic cancer than those with localized cancer or cancer in remission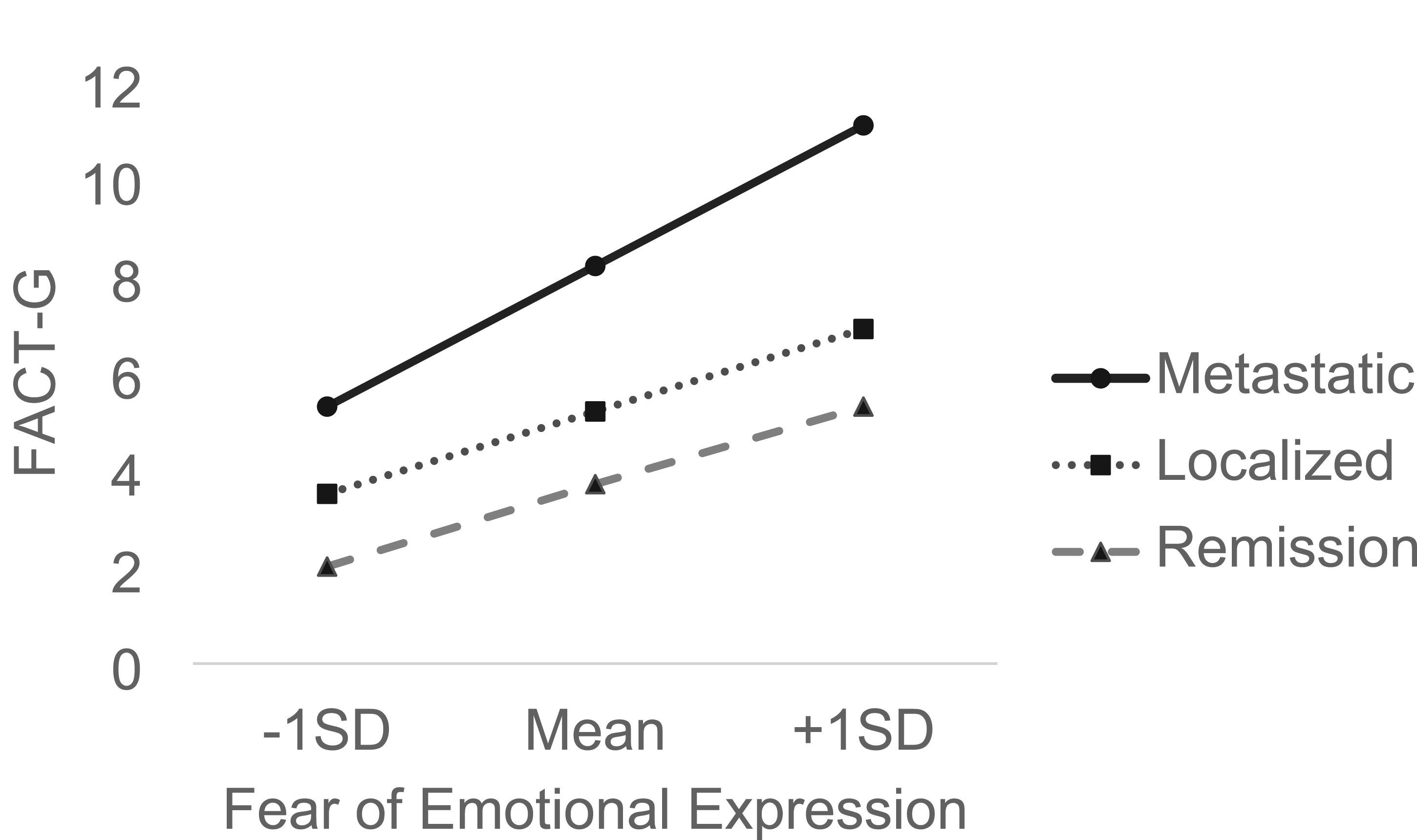
Moderation of Fear of Emotional Expression and Somatic Symptoms by Cancer Status
Discussion
As hypothesized, the fear of emotional expression was positively associated at a medium to large magnitude (r = .39) with the severity of somatic symptoms in the full sample of people with varying cancer status—metastatic, localized, or in remission. More interestingly, the linkage between fear of emotional expression and severity of somatic symptoms varied based on participant cancer status such that the association was strongest among patients with metastatic disease. Furthermore, after adjusting for covariates, this association remained among participants with metastatic disease, but not among participants with localized disease and with cancer in remission.
These findings lend credence to the possibility that the emotional weight of metastatic cancer may be distinct from other cancer stages so that fear of emotional expression is more tightly coupled to physical complaints such as pain and fatigue. Importantly, this coupling was not simply explained by the greater burden of depressive symptoms among patients with metastatic cancer. Taken together, these findings imply that it is not simply the level of distress that may matter for understanding somatic symptoms, but the broader context of individuals’ orientation toward expressing emotion in combination with their status of cancer progression.
Implications for Practice
Metastatic cancer has historically reflected a transition in care where curative outcomes are less likely, and patients face the threat of mortality with growing psychological salience. 10 At this stage of illness, individuals may confront strong emotions as their mortality becomes more difficult to ignore, and they experience a greater burden of pain and other somatic symptoms. 35 As individuals with metastatic cancer approach the end of life, they may benefit from opportunities to actively shape how others view their legacy through life reviews, emotional disclosures to loved ones, and other meaning-making activities.10,30,36 The heightened emotional challenges of metastatic cancer may contribute to physical symptoms such as pain, fatigue, and nausea if individuals are fearful of expressing their emotional needs and concerns. Whereas individuals who are more confident or comfortable in expressing emotions may be able to process their feelings with others, unexpressed emotions may paradoxically produce a heightened state of physiological arousal and tension. Expressing emotion provides opportunities for rallying social support, connecting with others, and asserting one’s autonomy and agency in therapeutic and lay contexts.6,14,15,37 Having identified the increased potency of fear of emotional expression in metastatic cancer, targeted assessment and support during later stages of cancer may be needed, particularly as physicians have noted that emotional expression is critical to advance cancer care planning and goals of care. 38 Spontaneously expressed emotions can be attended to and acknowledged as part of routine care. For patients who appear more reticent to express emotions, clinicians can consider whether making statements that normalize and invite emotional expression are helpful on a case-by-case basis.
Limitations
Several limitations qualify the study findings. The reliance on a single-item measure of fear of emotional expression may limit its reliability, albeit this likely leads to statistical underestimates in the current study regarding the full range of participant attitudes regarding emotional expression and their relationships to somatic symptoms. Additional measurement of specific feared emotions is needed. Although the analysis was able to account for important and potentially confounding differences in participants across their cancer status, the study did not include measures specific to the needs of patients with metastatic cancers and those approaching the end of life. While a diverse population of people with cancer was surveyed, findings may not represent the cancer population at large. Finally, the data are cross-sectional, limiting causal inferences.
Conclusions
In conclusion, these findings indicate that metastatic cancer is a unique and important context for emotional processing and expression. Although patients with metastatic disease endorse higher levels of psychiatric symptoms such as depression, these symptoms do not explain a heightened association between fear of emotional expression and somatic symptoms once cancer has spread. More exploratory work is needed to identify the content and process of emotional avoidance in late-stage cancer, and how emotional processing and expression can be facilitated through informal and professional supports.1,5 Further mechanistic research is needed to ascertain whether existing psychosocial and supportive care treatments for malignant pain exert their impacts through emotional processing and expression, 39 and whether targeted interventions for emotional awareness and expression can maximize impacts.6,14
Footnotes
Author Contributions
This manuscript was approved for submission by all authors and is original work prepared for Palliative Medicine. All authors were involved in the drafting and critical revision of the document. JG was involved in the conceptualization, analysis, interpretation, drafting, and revision of the article. MAL was involved in the conceptualization, interpretation, drafting, and revision of the article. KH was involved in the interpretation, drafting, and revision of the article. AH was involved in the interpretation, drafting, and revision of the article. MH was involved in conceptualization, design, data acquisition, interpretation, drafting, and revision of the article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported with funds U54GM104940 from the National Institute of General Medical Sciences and R01CA168387 from the National Cancer Institute.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The study data are available from the authors upon reasonable request.