
Abstract
Objective
To identify and synthesize the available evidence on the impact of advance care planning on decision-making and end-of-life care.
Design
A scoping review was conducted following the Joanna Briggs Institute methodology. The results were grouped into thematic categories and presented in accordance with the PRISMA-ScR guidelines.
Inclusion Criteria
Documents published between 2006 and 2026 in English, Spanish, and Portuguese were included, provided they were available in full text and addressed the research question.
Information Sources
The PubMed, Scopus, Web of Science, and BIREME databases were used. Additionally, the snowball sampling method was employed to expand the search.
Results
A total of 2816 records were identified through database searches and secondary tracking, of which 30 were selected for the final review. The identified impacts were organized into a conceptual framework comprising five interrelated dimensions: care congruence, healthcare utilization, economic and cost outcomes, family and caregiver impact, and patient quality of life. Each category is enriched by a set of interrelated components that describe various clinical, psychosocial, and financial outcomes reported in the literature.
Conclusions
Although advance care planning is not a new concept, this review provides an updated and integrated framework that highlights five interrelated domains of impact fundamental to the quality of end-of-life care. These findings suggest the potential value of considering ACP within patient-centered and value-based care models, while underscoring the relevance of future research aimed at informing the sustainability and humanization of end-of-life care.
Introduction
End-of-life decision-making represents one of the most significant and complex challenges in contemporary medicine, grounded primarily in the ethical principle of patient autonomy. 1 With technological and medical advances, clinical situations have arisen in which individuals lose the ability to express their wishes precisely when critical decisions must be made. A study by Silveira et al, which collected data through surveys of older adults who died between 2000 and 2006 to determine the prevalence of the need for decision-making and the loss of decision-making capacity, revealed that 42.5% required decision-making, of whom 70.3% lacked the capacity to do so. 2 This reality underscores the need to establish guidelines to optimize the process of implementing care in line with the patient’s preferences. 1
Advance directives are legal documents grounded in the principle of autonomy that express the patient’s wishes regarding future medical treatments when the patient lacks decision-making capacity. These tools are typically presented in formats such as a Living Will or the designation of a health care representative or proxy. 1 However, the concept has evolved into Advance Care Planning (ACP), understood as a complex, reflective, communicative, and dialogic process that is not only individual but also requires institutional and regional implementation. Additionally, its implementation seeks not only to document wishes but also to promote shared decision-making and improve legal protection for physicians when acting in accordance with the patient’s wishes. 3
Current knowledge regarding the impact of these tools is substantial and encompasses both clinical and psychological dimensions. Some authors note a high degree of agreement between the preferences documented in advance directives and the medical care patients actually receive before death. 1 Furthermore, evidence has shown that early discussions, especially those occurring more than 30 days before death, are associated with a lower likelihood of receiving aggressive measures, such as last-minute chemotherapy or admission to intensive care. 4 On a psychological level, advance planning has been associated with lower levels of stress, anxiety, and depression in both patients and their families, reducing the risk of experiencing symptoms of post-traumatic stress or pathological grief following the loss. 1 Furthermore, economic benefits have been observed through reductions in costs associated with futile treatments. 5
Despite these benefits, ACP implementation remains heterogeneous across healthcare systems; its effectiveness is hindered by persistent barriers, such as a lack of communication skills among healthcare staff and cultural factors that inhibit conversations about death. 1 Challenges persist in interpreting the documents and applying them in uncertain clinical scenarios, which often lead to conflicts between the medical team and family members. 5 Therefore, this review is essential because it aims not only to synthesize evidence but also to provide an integrated understanding of the multidimensional impact of ACP on decision-making and the care received by patients at the end of life.
Methods
A scoping review was conducted based on the guidelines outlined in the Joanna Briggs Institute (JBI) Evidence Synthesis Manual 6 to answer the following research question: What evidence is available regarding the impact of advance care planning on decision-making and end-of-life care? To ensure alignment between the research question and the selection criteria, the study was guided by the PCC framework as follows: Population: patients and their family caregivers involved in end-of-life care; Concept: multidimensional impact of advance care planning on decision-making and care; Context: diverse healthcare settings, including primary care, hospitals, and community care. The protocol was previously developed and registered in the Open Science Framework (OSF) to ensure transparency and traceability.
Comprehensive Search Strategy
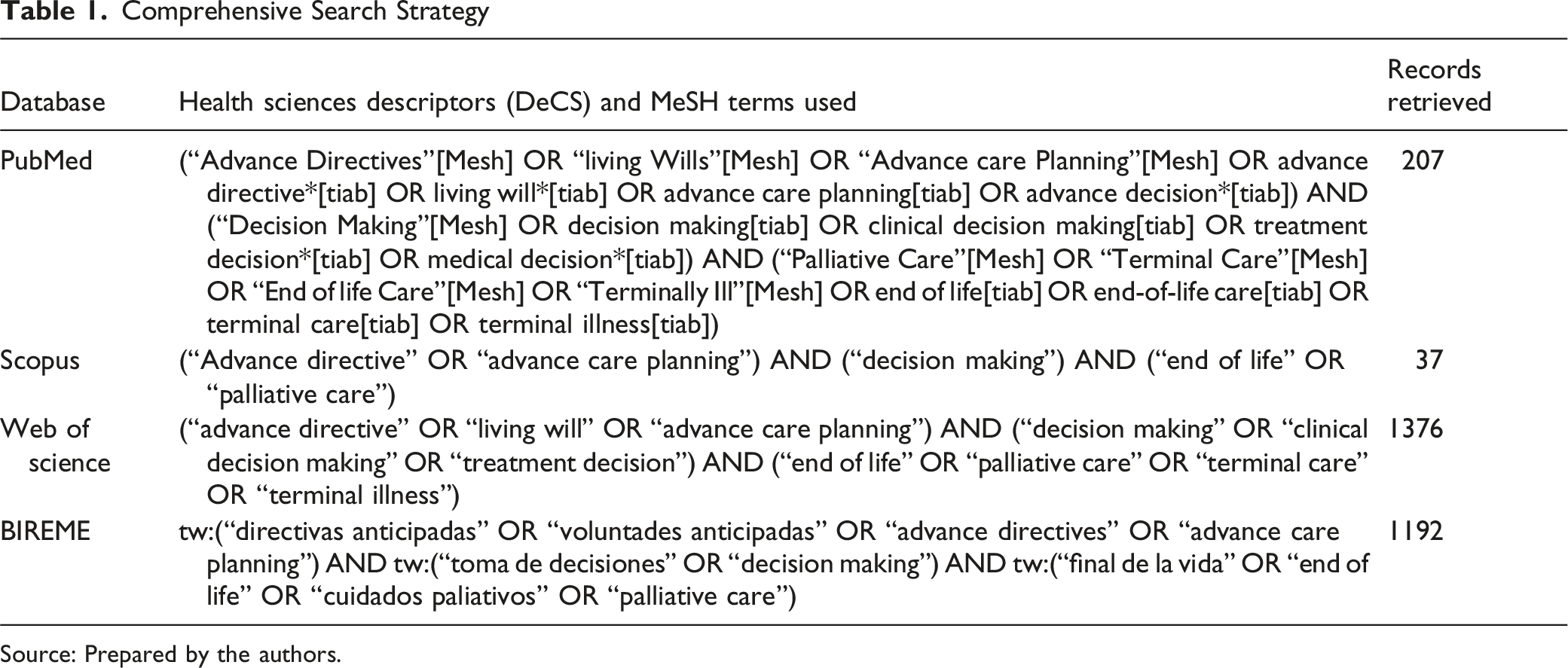
Source: Prepared by the authors.
Regarding database-specific syntax variations, the search string implemented in Scopus was intentionally more concise and centered on core conceptual terms compared to the multi-layered strings used in PubMed and Web of Science. While this focused approach avoided field tags and specific indexing descriptors (such as MeSH terms), Scopus was utilized primarily as a complementary data source to ensure regional cross-referencing. The potential risk of omission was mitigated by the comprehensive and highly sensitive syntaxes deployed across the other primary medical databases, which included comprehensive synonyms such as ‘living will’ and ‘terminal care'.
Inclusion and Exclusion Criteria
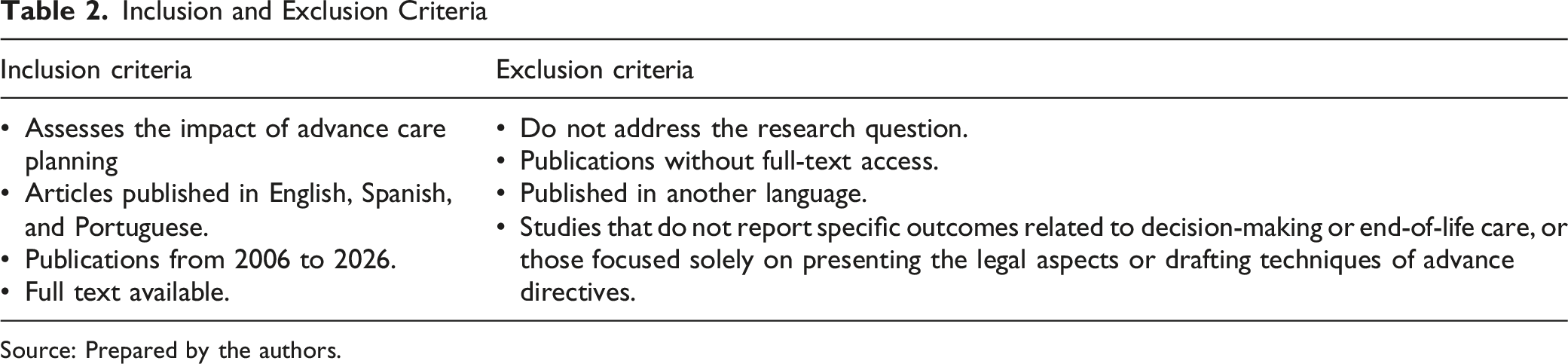
Source: Prepared by the authors.
Regarding language management, documents retrieved in English and Spanish were fully reviewed and analyzed in their original languages by the research team, who possess native and professional proficiency in both languages. For papers published in Portuguese, an advanced digital translation tool was utilized for initial text retrieval and data extraction to overcome language barriers. To prevent machine translation bias and ensure conceptual equivalence, all translated findings, clinical metrics, and core outcomes were subsequently subjected to a rigorous qualitative cross-verification and manual refinement process performed directly by the bilingual investigators before final thematic synthesis.
Subsequently, a database was created in Microsoft Excel®, where the articles were recorded. Before the formal screening, a pilot test was conducted on 5% of the initial records to calibrate the reviewers and ensure consistent application of the inclusion criteria. Two independent reviewers screened titles and abstracts. Disagreements were resolved by consensus. The selected articles were read in full to determine their relevance to the review. The document search and selection process was conducted in accordance with the PRISMA-ScR methodology. Figure 1 presents the process in detail. PRISMA-ScR flowchart for study inclusion. Source: Prepared by the authors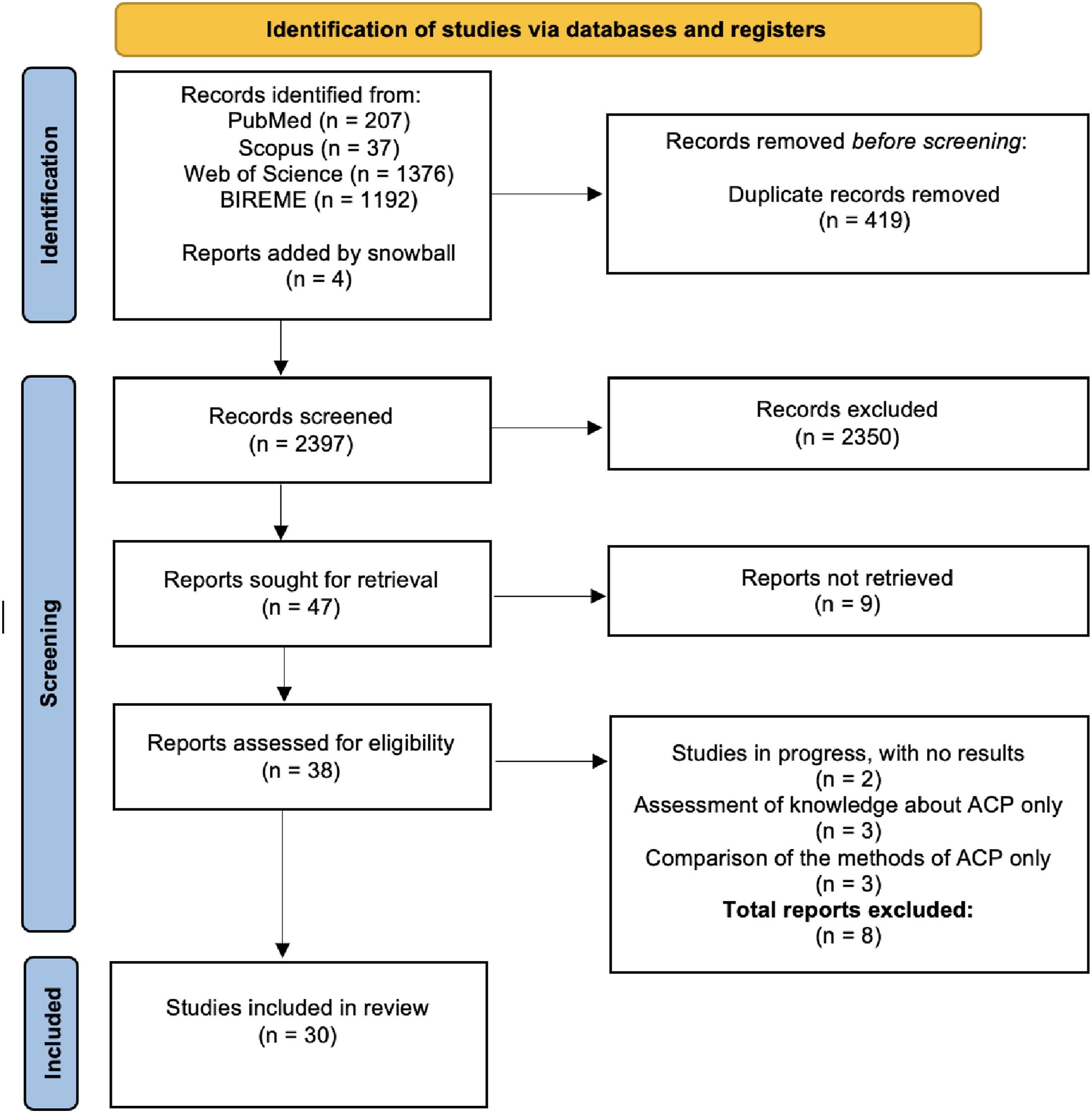
Given the inclusion of both primary studies and secondary evidence syntheses, potential overlap and duplication of evidence were carefully addressed. During the screening and selection process, a cross-referencing evaluation was conducted to map primary studies embedded within the retrieved systematic reviews against the individually selected primary articles. When overlapping evidence was identified, it was approached through a narrative and conceptual lens; rather than treating them as separate isolated sources, the data were integrated textually to capture a comprehensive overview of the reported outcomes.
Data Synthesis
Data synthesis was structured directly within the Microsoft Excel® database following the formal screening and selection process. The two independent reviewers extracted the reported outcomes, clinical metrics, and textual conclusions from the 30 included studies. These extracted data points were categorized into initial descriptive subthemes based on the specific indicators reported in the literature. Disagreements regarding data extraction or subtheme classification were resolved through the same consensus-driven approach used during the initial screening phases to ensure internal consistency and prevent interpretation bias.
Through this iterative classification process, the validated subthemes were synthesized into a conceptual framework comprising five distinct, interrelated impact dimensions: care congruence, healthcare utilization, economic and cost outcomes, family and caregiver impact, and patient quality of life and psychological well-being. This structured synthesis enabled the transition from the extracted bibliographic metrics to an integrated profile, mapping how advance care planning operates as a system-level intervention across diverse healthcare experiences.
Patient and Public Involvement
No patients or members of the public were involved in the design, conduct, reporting, or dissemination plans for this exploratory review.
Results
A total of 2812 initial records were identified through a search of the following databases: PubMed (n = 207), Scopus (n = 37), Web of Science (n = 1376), and BIREME (n = 1192). Concurrently, secondary manual searches utilizing the snowball sampling method yielded 4 additional relevant studies from the citation tracks of the retrieved literature, which were directly integrated alongside the database-derived records for subsequent eligibility evaluation. After removing 419 duplicates, 2397 titles and abstracts were analyzed, of which 2350 were excluded for failing to meet the inclusion criteria.
Forty-seven reports were selected for full-text retrieval, of which 9 could not be retrieved in full text due to institutional repository access limits and database subscription constraints at the authors’ participating institution. To maintain methodological transparency and minimize omission bias, exhaustive secondary searches were conducted across open-access databases, institutional mirrors, and public academic repositories (such as Google Scholar and ResearchGate) to locate alternative digital copies. Despite these thorough retrieval attempts, full-text access could not be secured; therefore, these nine records were definitively excluded from the final review due to the lack of complete data required for comprehensive thematic synthesis.
Summary of the Included Evidence
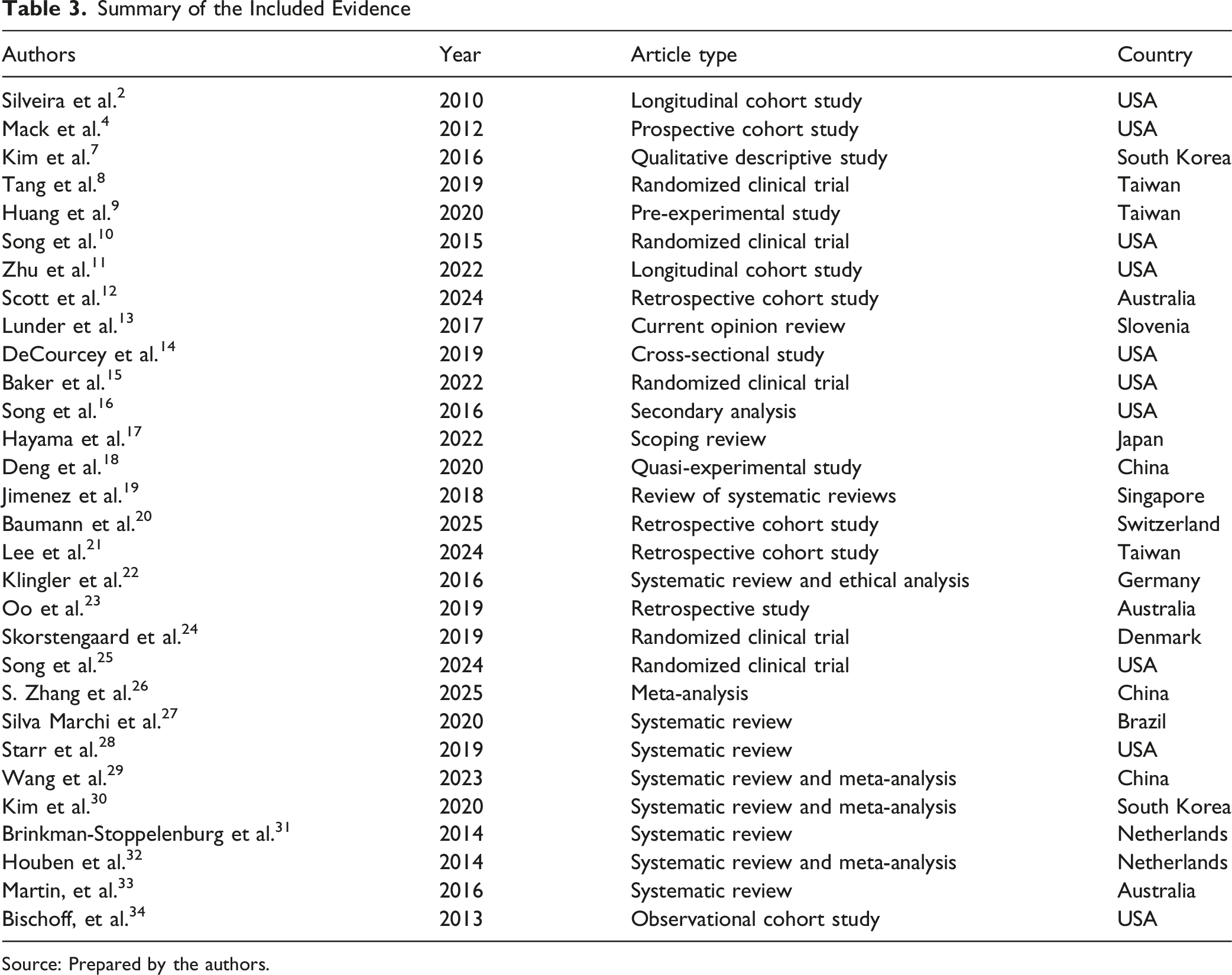
Source: Prepared by the authors.
Figure 1 shows the PRISMA-ScR flowchart for systematic reviews and meta-analyses, covering the following stages: identification, selection, and inclusion of articles. Ten reviews (including systematic reviews, meta-analyses, and scoping reviews), seven cohort studies (longitudinal, prospective, and retrospective), five randomized clinical trials, two quasi-experimental or pre-experimental studies, and one study of each type were identified for the following: qualitative descriptive, secondary analysis, cross-sectional, observational, retrospective, and opinion studies. This methodological diversity reflects a robust, multifaceted body of evidence that seeks to capture the complexity of advance care planning from diverse clinical and observational perspectives.
The literature originated from various regions of the world; however, most studies were conducted in the United States (10 publications), followed by Taiwan (n = 3), China (n = 3), and Australia (n = 3). Additionally, two studies were identified from South Korea and two from the Netherlands; and one study each from Slovenia, Japan, Singapore, Switzerland, Germany, Denmark, and Brazil. Geographically, the distribution of the evidence indicates a strong leadership of North American and Asian contexts in the investigation of ACP practices. These details are summarized in Table 3 and illustrated graphically in Figure 2. Geographic distribution of the scientific output included in the review. (n = number of studies included). Source: Prepared by the authors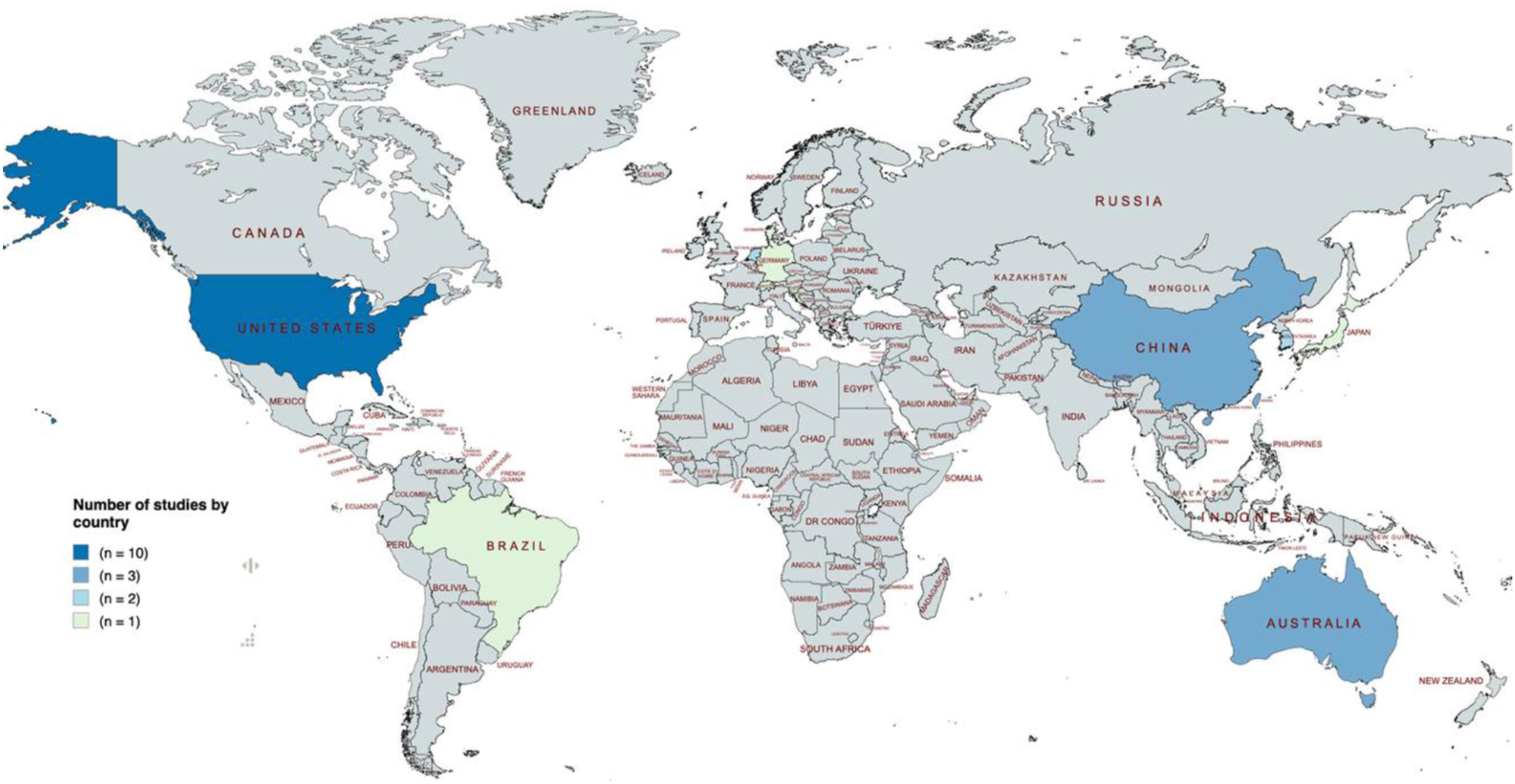
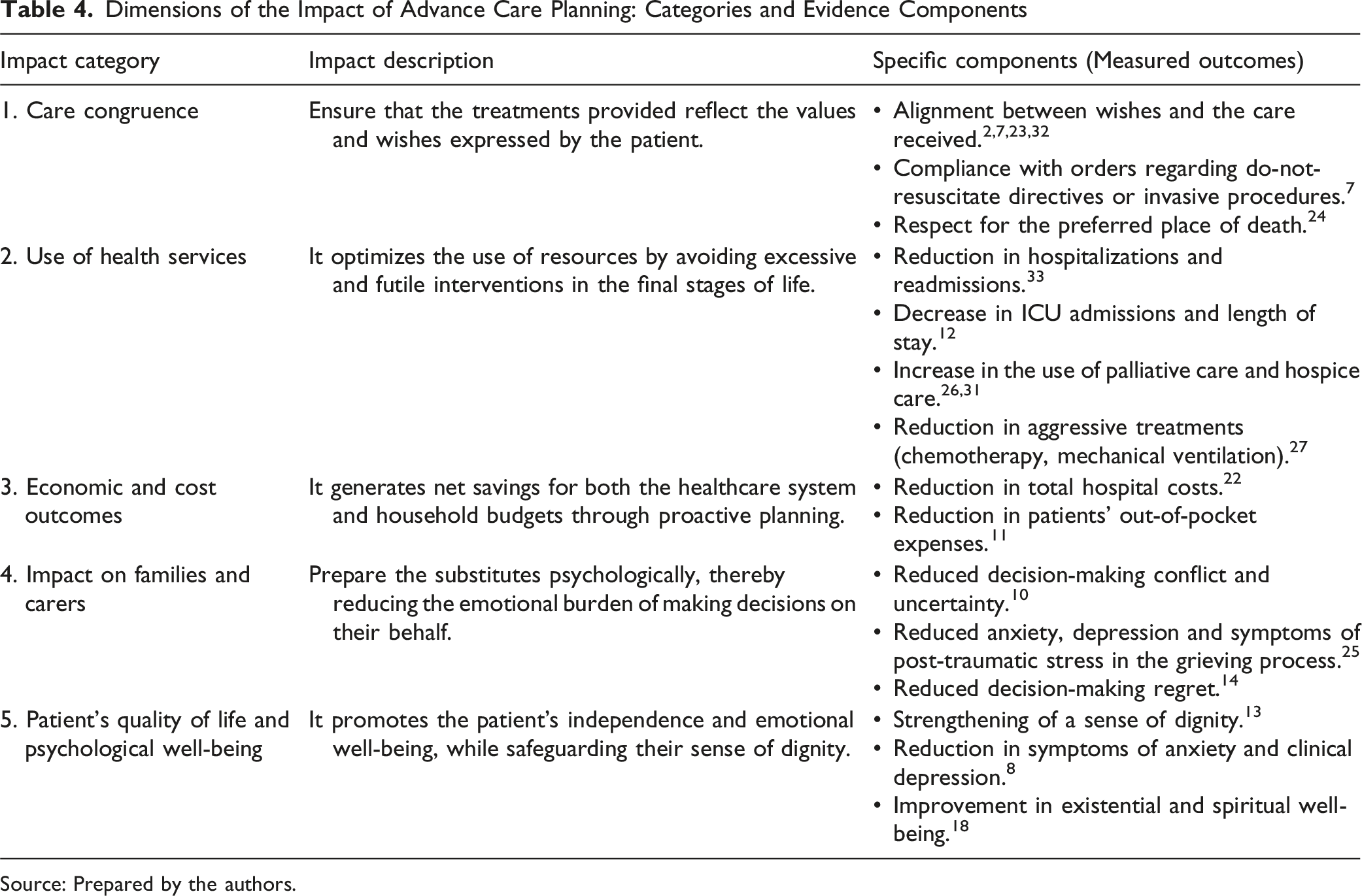
A wide range of impacts of advance care planning (ACP) was identified and grouped into five categories. Twenty-five articles (83.33%) addressed care congruence, a dimension that emerges as the most consistently reported, assessing the alignment between patients’ wishes and the treatments they received. Closely related to clinical outcomes, fifteen studies (50.00%) focused on the utilization of health services, analyzing hospitalization rates and ICU admissions. Beyond operational metrics, ten articles (33.33%) explored the impact on quality of life and psychological aspects of the patient. Six studies (20.00%) reported effects on family and caregivers, particularly regarding decision-making and grief. Finally, four articles (13.33%) focused on economic outcomes and costs associated with care, identifying an emerging but still developing interest in the financial sustainability of these programs. It is worth noting that some studies addressed more than one impact category.
Dimensions of the Impact of Advance Care Planning: Categories and Evidence Components
Source: Prepared by the authors.
Discussion
This discussion section summarizes the findings from the literature to map the multidimensional impact of Advance Care Planning. While previous studies have often emphasized individual benefits, such as patient autonomy, our findings highlight the systemic implications of ACP as a dynamic process of communication and knowledge management that fundamentally redefines the quality of end-of-life care. 13 Through the systematization of the evidence, it is observed that the effectiveness of advance directives extends beyond mere legal documentation, directly impacting patient autonomy, the optimization of healthcare system resources, and the psychosocial well-being of families. 19 Mapping these results allows us to identify a shift towards a preventive, person-centered approach, which is fundamental to addressing the challenges posed by complex chronic diseases. 30
To systematize the complexity of the identified results and facilitate a comprehensive understanding of the evidence, we have structured the analysis into five critical impact dimensions. This classification responds to the need to map advance care planning not merely as a documentary act, but as a multidimensional intervention that transforms the clinical and emotional experience of the end of life. This shift towards a preventive and person-centered approach is particularly relevant in primary care settings, where early ACP discussions can be integrated into longitudinal care to manage the trajectory of complex chronic diseases proactively. Below, we explore each category in depth to examine the components that define ACP’s scope in decision-making. The interrelationships among these dimensions and their overall impact are illustrated in Figure 3. Dimensions of the multidimensional impact of advance care planning. Source: Prepared by the authors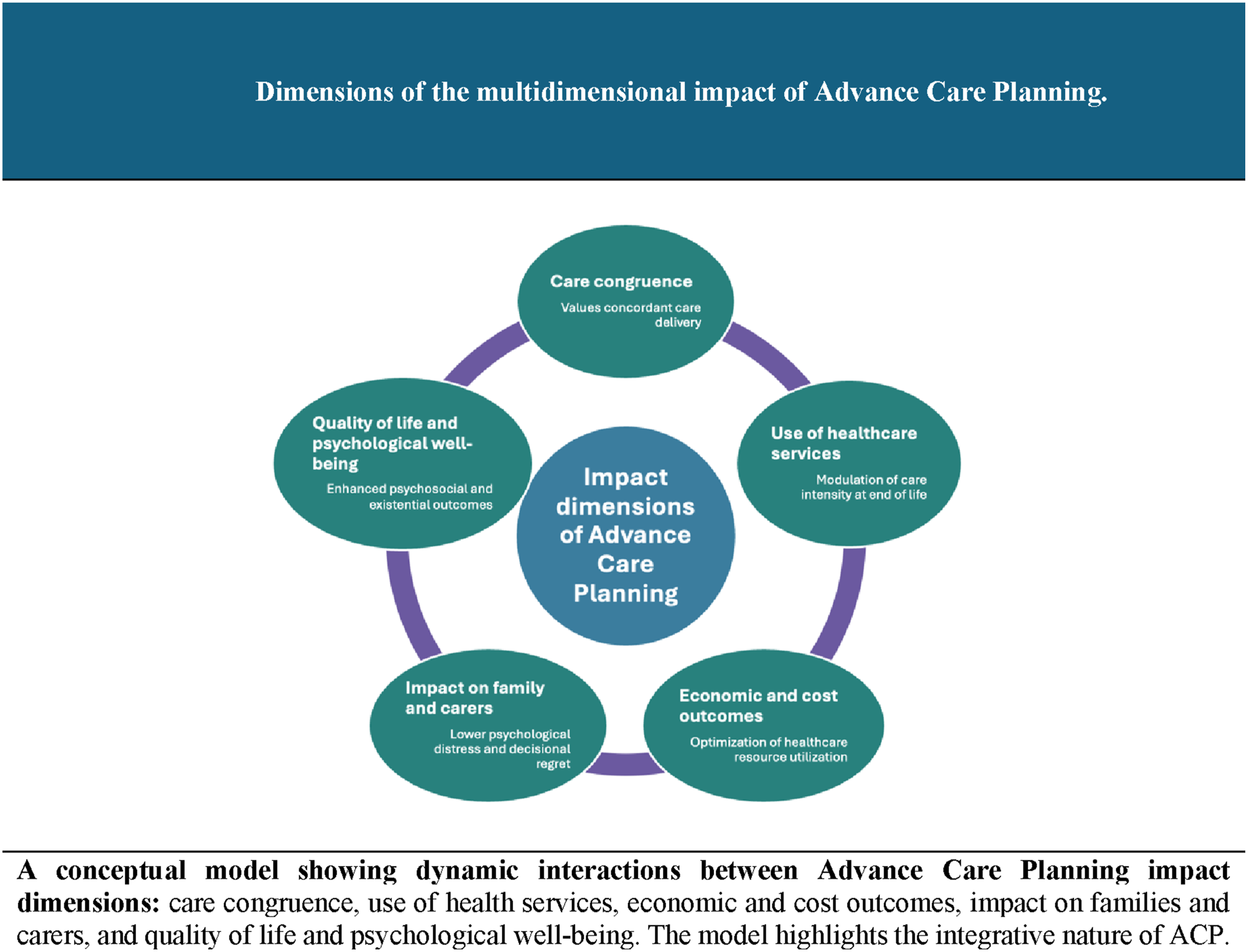
Care Congruence
Advance care planning’s ability to ensure that the treatment received aligns with the patient’s values is the most robust indicator of success, as evidenced by high concordance in resuscitation orders. 7 In this regard, the evidence suggests that ACP helps to stabilize the patient’s preferences throughout the course of the illness, ensuring that their care goals remain consistent. 32 Furthermore, it has been shown that interventions that use an iterative, reflective process better align hospital care with previously expressed wishes. 23 Specifically in older adults, the presence of advance directives is associated with a higher probability of receiving limited or comfort care rather than invasive interventions. 2
However, the literature also reveals that the effectiveness of advance directives is deeply mediated by relational and cultural complexities; factors such as the family member’s emotional distress in the face of the patient’s deterioration can lead to disagreements, particularly in cultures where family decision-making is predominant. 21 Furthermore, consistency is enhanced when the patient formally designates a representative, thereby reducing uncertainty in surrogate decision-making. 16 Similarly, in adolescents with serious illnesses, facilitated communication significantly increases the accuracy of parents’ reporting of their children’s treatment preferences. 15 Despite these advances, the impact of discussions at the actual place of death remains mixed in some clinical trials, Skorstengaard et al reported mixed outcomes, demonstrating that a structured ACP intervention did not significantly alter the proportion of patients dying at home compared to standard care, 24 highlighting an opportunity for improvement and the need to identify the barriers to achieving this care goal.
Use of Healthcare Services
Our analysis suggests that ACP acts as a key regulator mechanism for medical interventions, significantly reducing unplanned hospitalizations and admissions to intensive care units. 12 Closely related to this, studies in patients with advanced cancer confirm that the use of advance directives reduces the use of aggressive measures such as futile chemotherapy in the final days of life. 27 Consequently, this shift in resource use leads to an increase in referrals to palliative care and hospice, facilitating death in the place of choice. 31 Furthermore, in care homes, ACP interventions have been shown to reduce unnecessary hospital transfers during acute episodes. 33
It is essential to note that timing is key and has emerged as a decisive factor; conversations occurring more than 30 days before death are strongly linked to lower-intensity care near the end of life. 4 Furthermore, recent meta-analyses reinforce the finding that advance directives increase the use of palliative care, although their effect on ICU length of stay may vary. 26 Among older adults, all components of ACP, from discussion to documentation, are associated with higher-quality care received. 34 Even in critical settings such as the ICU, advance care planning support can help clarify decisions regarding life-sustaining treatment and avoid unwanted treatments. 17 Finally, documenting specific medical orders ensures that life-sustaining interventions align with care goals. 20
Economic Outcomes and Healthcare System Costs
From an economic perspective, ACP is an effective strategy for reducing total hospital costs through proactive planning. 22 In this context, it has been observed that the early completion of advance directives – drawn up more than 3 months before death – is associated with lower direct out-of-pocket costs for the patient, as it avoids procedures of low clinical benefit. 11 Finally, it is noted that these savings are particularly evident in regions with high levels of end-of-life medical expenditure. 28
Impact on the Family and Carers
Beyond individual autonomy, advance care planning is a dual intervention of high therapeutic value, as it not only benefits the patient but also prepares family members for their role as decision-makers, significantly reducing their emotional burden during the process. 10 Particularly in the pediatric setting, it has been shown that ACP discussions that include family goals succeed in reducing parental decision regret following the loss of a child. 14 Concerning adult survivors, the evidence indicates that advance planning is associated with a reduction in anxiety and post-traumatic stress during the grieving process. 25 Finally, it is worth noting that the joint participation of the patient-caregiver dyad in the ACP process improves the family’s overall satisfaction with the care received by their loved one. 29
Quality of Life and Psychological Well-Being of the Patient
In evaluating psychological parameters, Tang et al demonstrated that advance care planning significantly improves depressive and anxiety symptoms among patients with cancer. However, it is critical to note their concurrent null findings regarding overall quality of life and the fulfillment of preferred end-of-life care. 8 In this regard, it has been observed that structured programs enable patients with degenerative conditions, such as mild dementia, to participate actively in their care planning while they still have the capacity to do so. 9 Complementarily, the use of interviews based on the patient’s life story reduces existential distress among frail older adults. 18 Finally, it is important to highlight that these facilitated communication processes not only reduce clinical anxiety but also strengthen the individual’s sense of dignity at the end of life.
Limitations
This study has several limitations that should be considered when interpreting its results. Firstly, the potential exclusion of relevant literature due to language barriers, restricted access to full-text articles, database selection, the search period, and indexing criteria may have limited the analysis’s comprehensiveness. Additionally, potential publication bias must be acknowledged, as studies with negative or neutral results are less likely to be available in the indexed literature. Language bias is also relevant, as only articles published in English, Spanish, and Portuguese were included. Also, the heterogeneity in the methodological quality of the included studies constitutes another limitation, given that no critical assessment of internal or external validity was conducted, which may affect the robustness of the conclusions.
Furthermore, in accordance with scoping review guidelines, a formal critical appraisal of the methodological quality or risk of bias of the included evidence was not performed. The analyzed literature spans a broad methodological spectrum-ranging from randomized controlled trials and systematic reviews to retrospective analyses and descriptive reports. Consequently, the strength of the conclusions varies across the analyzed dimensions. Particularly, the economic and cost outcomes dimension must be interpreted with caution, as it is supported by a limited subset of only four studies, highlighting the need for more rigorous economic evaluations in future research.
Finally, the external validity of these findings is constrained by the geographical and cultural concentration of the reviewed evidence. Most of the included studies originated from the United States, Taiwan, China, and Australia. These regions operate under substantially different legal structures governing healthcare proxies, variations in institutional funding for palliative care, and distinct cultural attitudes regarding death and familial autonomy. Consequently, the synthesized dimensions may not directly translate to healthcare systems with alternative regulatory frameworks or different sociocultural norms.
Conclusions
This review provides an integrative multidimensional framework that maps the existing literature on Advance Care Planning, suggesting its role as a potential system-level intervention. The identification of five dimensions -care congruence, use of health services, economic and cost outcomes, impact on families and carers, and quality of life and psychological well-being- offers a preliminary conceptual structure through which the varied impacts of ACP on patients’ end-of-life experiences can be organized and further evaluated.
These categories may be understood as interrelated elements that form a comprehensive care profile, instead of isolated compartments. The cross-cutting nature of these components suggests ACP’s comprehensive impact across diverse clinical settings, from community care and care homes to intensive care units, potentially guiding a shift from isolated, crisis-driven interventions to a proactive, reflective management of the disease trajectory.
Furthermore, this categorization aligns with ACP’s recognition as a strategic component and highlights the relevance of examining evolving frameworks in palliative care. Its observed capacity to align treatments with the patient’s values, optimize the use of institutional resources, and provide support centered on the person and their context points toward its potential role in supporting the transition of healthcare systems towards more sustainable, equitable, and humane models.
Finally, the systematization of evidence across these five dimensions offers a potential conceptual framework for evaluating clinical interventions and may serve to inform the integration of advance care planning into standard medical practice. Likewise, it is imperative to continue research in this area to more precisely identify the specific elements that underlie the effectiveness of ACP across different clinical settings, aimed at responding comprehensively to the needs of patients and their families, and to the sustainability of healthcare systems.
Footnotes
ORCID iDs
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Universidad de La Sabana, Colombia, through the MED-342-2023 project (Permanent professional development in Primary Health Care through the Virtual Campus for Public Health in Colombia).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.