
Abstract
Objective
This systematic review synthesizes randomized controlled trial evidence on the effectiveness of nurse-led ACP interventions for patients with advanced cancer.
Methods
We searched PubMed, Embase, CINAHL, Web of Science, and the Cochrane Central Register from inception to January 2026. Eligible studies were randomized controlled trials (RCTs) evaluating nurse-led ACP interventions in adults with advanced or metastatic cancer. Two reviewers independently screened records, extracted data, and assessed risk of bias using the Cochrane Risk of Bias 2 (RoB 2) tool. A narrative synthesis was performed due to clinical and methodological heterogeneity precluding meta-analysis.
Results
Six studies (7 publications; N = 2816) met inclusion criteria, conducted in the United States, South Korea, and six European countries. Nurse-led ACP interventions consistently increased advance directive completion (adjusted odds ratios 2.5-5.3) and end-of-life conversation rates vs usual care. One trial showed facilitated nurse-led ACP outperformed patient-directed approaches in ACP engagement (adjusted difference 0.25; 95% CI 0.10-0.40; P = .001). Quality of life outcomes were mixed; most trials showed no significant difference at 3 months, though higher-intensity interventions trended toward greater benefit. Overall risk of bias was low to moderate.
Conclusions
Nurse-led ACP interventions are feasible and effective in improving ACP engagement and end-of-life outcomes for patients with advanced cancer. Successful implementation requires standardized training, adequate intervention intensity, and systematic follow-up. Future trials should use validated patient-reported ACP measures and explore optimal timing and delivery methods.
Keywords
Introduction
Cancer remains a foremost cause of global mortality. In 2025, an estimated 2.04 million new cancer diagnoses and 618,120 cancer-related deaths are projected in the United States alone, with a disproportionate and growing burden occurring in younger adults and women. 1 A substantial proportion of patients progress to advanced or metastatic disease, a phase characterized by complex physical and psychological symptom burden, existential distress, and rapidly escalating care needs. For these individuals, the alignment between personal values and preferences and the care they ultimately receive at the end of life constitutes both a clinical and ethical priority of the highest order.
Advance care planning (ACP) is a structured, iterative process through which adults reflect on, articulate, and document their preferences for future medical care in the context of serious illness. 2 Defined by international consensus as a process that “supports adults at any age or stage of health in understanding and sharing their personal values, life goals, and preferences regarding future medical care,” ACP encompasses goals-of-care conversations, completion of advance directives (ADs), surrogate designation, and ongoing documentation updates as illness progresses. 2 Landmark interventional evidence has demonstrated that embedding structured ACP within oncology care reduces unwanted aggressive interventions near death, increases hospice enrollment, and meaningfully alleviates psychological burden among bereaved families.3,4 The seminal trial by Temel and colleagues demonstrated that early integrated palliative care—with ACP as a central component—not only improved quality of life and mood but was associated with a 2.7-month survival advantage in metastatic non-small-cell lung cancer. 5 Similarly, Project ENABLE II established that a nurse-led palliative care program addressing ACP alongside symptom management significantly improved quality of life and mood compared with usual oncological care. 6
Despite this evidence base, ACP remains deeply underutilized in advanced cancer populations. Structural barriers are pervasive and multifactorial: oncology consultations rarely accommodate the time required for substantive goals-of-care discussions; clinician training in prognostic communication and ACP facilitation is inconsistent; and institutional cultures that prioritize active treatment over comfort-focused planning continue to predominate. 7 Equally significant is the chronic shortage of specialist palliative care physicians. Current projections indicate a potential deficit of 9000-16,000 palliative care physicians in the United States by 2040, with analogous shortfalls anticipated in other high-income countries.8 This workforce crisis underscores the urgent need for scalable, primary palliative care models that can deliver ACP within existing oncology infrastructure.
Registered nurses and advanced practice nurses represent an underutilized yet highly capable resource for ACP delivery. Oncology nurses sustain longitudinal relationships with patients across multiple treatment cycles, often developing a depth of familiarity with patients' evolving values, fears, and family dynamics that specialist physicians may not achieve. Their clinical expertise, communication skills, and patient-trusted status render them well positioned to initiate, document, and follow up on ACP conversations as a routine component of oncology nursing practice. A growing number of structured nurse-led ACP models have been developed, ranging from facilitated in-person conversations using validated frameworks such as Respecting Choices® to telephonic case management programs and nurse-led primary palliative care clinics.8-10
Prior reviews have described the scope of nurse-led ACP practice and identified promising outcomes, but have been limited by heterogeneous study designs, inclusion of non-cancer and non-advanced-cancer populations, and a tendency to incorporate observational and feasibility studies alongside controlled trial evidence.10,11 A rigorous synthesis restricted to randomized controlled trial evidence in advanced cancer populations is lacking. Such a synthesis is essential to establish the evidentiary foundation for policy decisions, nursing education reform, and the design of future trials. The present systematic review therefore aimed to comprehensively evaluate the effectiveness of nurse-led ACP interventions specifically in patients with advanced cancer, with focused attention to: (1) ACP engagement and advance directive completion; (2) health-related quality of life and symptom burden; (3) end-of-life care utilization including hospice enrollment; and (4) characteristics of effective nurse training and intervention delivery models. We deliberately confined this synthesis to patients with advanced cancer. We recognise that contemporary ACP frameworks increasingly emphasise the initiation of ACP “upstream”—among healthy adults and earlier in the illness trajectory rather than only at the advanced-disease stage—and its relevance to any adult irrespective of diagnosis.2,11 Advanced cancer nonetheless represents the setting in which the prognostic clarity, decisional urgency, and existing evidence base for nurse-led ACP are most concentrated, and it therefore constitutes a coherent and policy-relevant population for focused appraisal.
Methods
Protocol and Registration
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 2020) guidelines. 12 The protocol was prospectively registered with the International Prospective Register of Systematic Reviews (PROSPERO; registration number CRD42024568922) prior to database searching.
Eligibility Criteria
Studies were eligible if they satisfied the following PICOS criteria. Population: adult patients (aged ≥18 years) with advanced, metastatic, or incurable cancer (solid tumors or hematologic malignancies at stage III or IV, or otherwise designated as incurable or palliative-intent). Intervention: any structured ACP intervention led primarily or substantially by registered nurses (RNs), advanced practice nurses (APNs), or nurse practitioners (NPs), with or without physician oversight. Interventions encompassed facilitated ACP conversations, goals-of-care discussions, advance directive completion, care coordination, symptom management counseling with ACP integration, or combinations thereof, delivered in-person, telephonically, or via telehealth platforms. Comparator: standard oncological care, usual care, or an alternative ACP delivery model (eg, patient-directed or physician-led ACP). Outcomes: primary outcomes were ACP engagement measures (advance directive completion, documented goals-of-care conversations, ACP engagement scores). Secondary outcomes included health-related quality of life (HRQoL), symptom burden, end-of-life care utilization (hospice enrollment, emergency department visits, ICU admissions, aggressive care at end of life), and psychological outcomes (anxiety, depression). Study design: randomized controlled trials (RCTs) including individually randomized, cluster-randomized, and comparative effectiveness designs.
Exclusion criteria comprised: non-randomized or observational designs; populations restricted to non-cancer diagnoses; interventions without a substantive nurse-led component (eg, solely physician- or social worker-led); studies reporting only pilot data without primary outcome assessment; protocol-only publications; and non-English or non-Chinese language publications.
Information Sources and Search Strategy
A systematic search was executed across five electronic databases: PubMed/MEDLINE, Embase, CINAHL (Cumulative Index to Nursing and Allied Health Literature), Web of Science Core Collection, and the Cochrane Central Register of Controlled Trials (CENTRAL). Searches were conducted from database inception to January 31, 2026. The search strategy combined Medical Subject Headings (MeSH) terms with free-text keywords and was developed in consultation with a health sciences librarian. The PubMed core search strategy was: (“advance care planning”[MeSH] OR “advance directives”[MeSH] OR “goals of care”[tiab] OR “end-of-life planning”[tiab]) AND (“nurses”[MeSH] OR “nursing”[MeSH] OR “nurse-led”[tiab] OR “advanced practice nurse”[tiab] OR “registered nurse”[tiab]) AND (“neoplasms”[MeSH] OR “cancer”[tiab] OR “malignancy”[tiab] OR “oncol*”[tiab]) AND (“palliative care”[MeSH] OR “terminal care”[MeSH] OR “hospice care”[MeSH]). Analogous strategies were adapted for each database. No date or study design restrictions were applied to the database searches; consistent with the eligibility criteria, language eligibility was restricted to publications in English or Chinese and was applied at the screening stage. Supplementary searches included manual screening of reference lists of included studies, relevant systematic reviews, and citation tracking.
Study Selection
All retrieved records were imported into Covidence systematic review software (Veritas Health Innovation, Melbourne, Australia) and deduplicated. Two independent reviewers (W.S. and a collaborator) screened titles and abstracts against pre-specified eligibility criteria, followed by full-text review of potentially eligible records. Discrepancies at each stage were resolved through discussion and, where necessary, arbitration by a third reviewer. The selection process was documented and illustrated as a PRISMA 2020 flow diagram (Figure 1). PRISMA 2020 flow diagram illustrating the study selection process. A total of 1276 records were identified through database searching (n = 1254) and supplementary sources (n = 22). After deduplication and screening, 6 unique studies (reported in 7 publications; N = 2816) were included in the final qualitative synthesis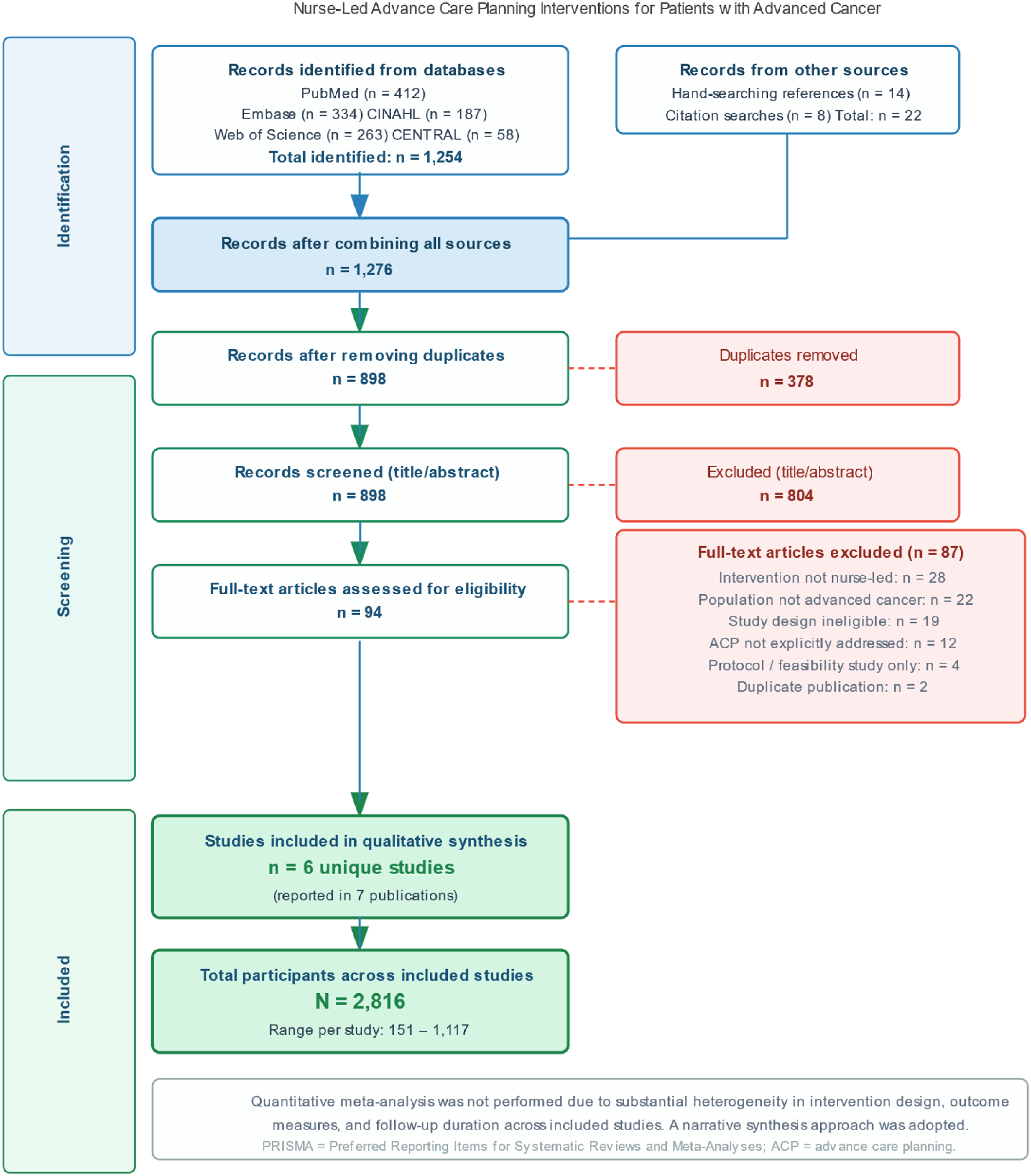
Data Extraction
Standardized data extraction forms were developed, piloted on three studies, and refined iteratively. Two reviewers independently extracted data from each eligible study, with discrepancies reconciled by consensus. Extracted data elements included: study design; country and setting; recruitment period; total sample size and allocation; patient demographics (mean age, sex distribution, primary cancer type, performance status); intervention components, ACP model/framework, nurse training, delivery mode, duration, and contact intensity; comparator description; follow-up duration; and all outcome data with associated measures, time points, and effect estimates (eg, odds ratios, mean differences, 95% confidence intervals, P values). For trials with multiple publications, data were integrated across all papers and reconciled.
Risk of Bias Assessment
Risk of bias in individual RCTs was evaluated using the Cochrane Risk of Bias 2 (RoB (2) tool, 13 which assesses five domains: (1) bias arising from the randomization process; (2) bias due to deviations from intended interventions; (3) bias due to missing outcome data; (4) bias in measurement of the outcome; and (5) bias in selection of reported results. Each domain was rated as “low risk,” “some concerns,” or “high risk,” and an overall judgment was assigned. For cluster-RCTs, potential for recruitment bias and differential cluster-level confounding was additionally considered. Two reviewers independently rated each study; discordant ratings were resolved by consensus discussion.
Data Synthesis
Substantial heterogeneity in intervention design, ACP frameworks, comparator conditions, outcome measures, and follow-up durations precluded quantitative meta-analysis, consistent with the judgment reflected in the PRISMA flow diagram. Findings were therefore synthesized narratively, organized by outcome domain. For each outcome, the direction and magnitude of effect, clinical meaningfulness, and consistency across studies were appraised. Subgroup considerations including intervention intensity, delivery modality, and training model were described where data permitted.
Results
Search Results
The database search retrieved 1254 records; an additional 22 records were identified through reference list and citation searches, yielding 1276 total records. Following deduplication (n = 378 duplicates removed), 898 records underwent title and abstract screening, of which 804 were excluded. The most common reasons for exclusion included: non-advanced-cancer population (n = 298), no substantive nurse-led component (n = 247), non-RCT design (n = 183), and ACP not explicitly addressed (n = 76). Ninety-four full-text articles were assessed for eligibility. After full-text review, 87 articles were excluded: no nurse-led intervention (n = 28), population not restricted to advanced cancer (n = 22), ineligible study design (n = 19), ACP not explicitly addressed (n = 12), protocol or feasibility study only (n = 4), and duplicate publication (n = 2). Six unique studies (reported in 7 publications) were included in the final synthesis (Figure 1).
Study Characteristics
Characteristics of Included Studies
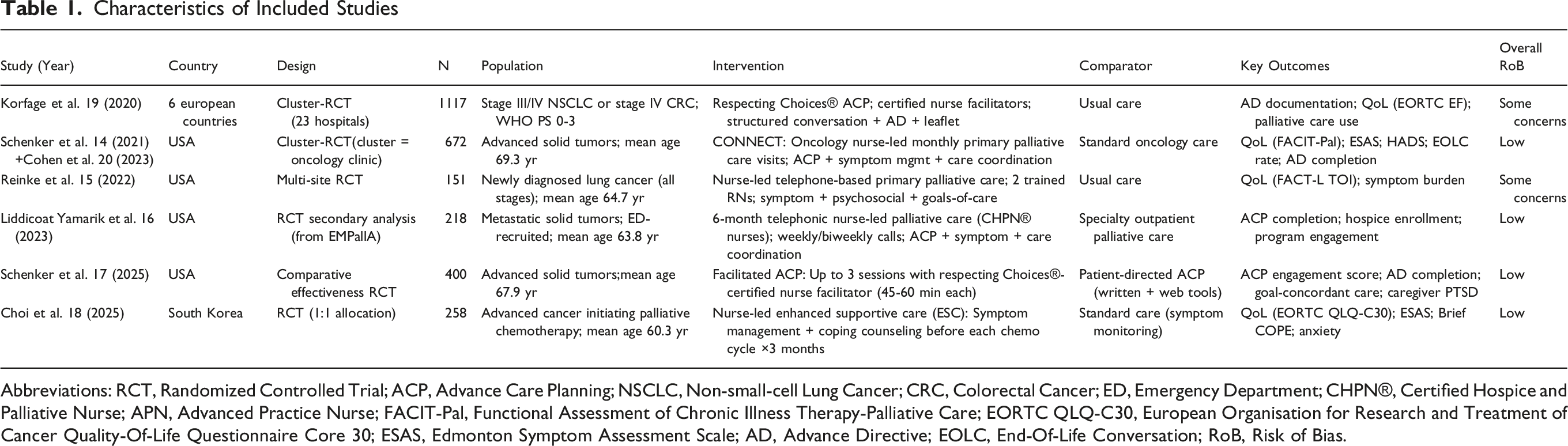
Abbreviations: RCT, Randomized Controlled Trial; ACP, Advance Care Planning; NSCLC, Non-small-cell Lung Cancer; CRC, Colorectal Cancer; ED, Emergency Department; CHPN®, Certified Hospice and Palliative Nurse; APN, Advanced Practice Nurse; FACIT-Pal, Functional Assessment of Chronic Illness Therapy-Palliative Care; EORTC QLQ-C30, European Organisation for Research and Treatment of Cancer Quality-Of-Life Questionnaire Core 30; ESAS, Edmonton Symptom Assessment Scale; AD, Advance Directive; EOLC, End-Of-Life Conversation; RoB, Risk of Bias.
Cancer types were heterogeneous across studies. The ACTION trial enrolled patients with stage III/IV lung cancer or stage IV colorectal cancer. 19 The CONNECT trial enrolled patients with any solid tumor of advanced stage attending participating oncology clinics. 14 The Facilitated ACP trial enrolled patients with advanced solid tumors. 17 The EMPallA trial included patients with metastatic solid tumors presenting to emergency departments. 16 The ESC (Enhanced Supportive Care) trial enrolled patients with advanced cancer initiating palliative-intent chemotherapy. 18 The Reinke trial enrolled patients with newly diagnosed lung cancer across all stages, with subgroup analyses informative for the advanced cancer population. 15
Mean participant age ranged from 60.3 to 69.3 years. Women represented 38% to 58% of participants across studies. Performance status was generally good to moderate (ECOG 0-2 or equivalent), as required by most inclusion criteria. Geographic diversity was notable, spanning academic cancer centers, community oncology clinics, and emergency department-initiated programs across three continents.
Intervention Characteristics
Nurse-led ACP interventions varied substantially in their design, theoretical framework, delivery modality, and intensity. The ACTION trial employed the Respecting Choices® facilitated ACP model, delivered by 39 certified facilitators (predominantly nurses) across 23 hospitals, through structured ACP conversations supplemented by standardized leaflets and advance directive documentation. 19 Nurses received a 2-day competency-based training program in their local language, with fidelity checks conducted twice during the study.
The CONNECT (Care Management by Oncology Nurses to Address Supportive Care Needs) intervention was delivered by oncology nurses embedded within community cancer centers. 14 CONNECT comprised monthly visits designed to elicit patient concerns and care goals, foster realistic illness expectations, coordinate supportive care, and facilitate ACP through structured shared care planning. 20 Nurses received specialized training in primary palliative care skills including ACP facilitation, symptom management, and care coordination. Participants completed a mean of 2.2 intervention visits over 3 months.
The Facilitated ACP trial contrasted two forms of patient-facing ACP delivery: nurse-facilitated conversations using the Respecting Choices® framework (up to three sessions of 45-60 minutes each, delivered in-person, by video, or telephonically) vs patient-directed ACP using written and web-based tools. 17 Nurse facilitators held supportive oncology experience and underwent formal Respecting Choices® certification training.
Nurse Training Characteristics, Intervention Components, and Key Outcome Findings
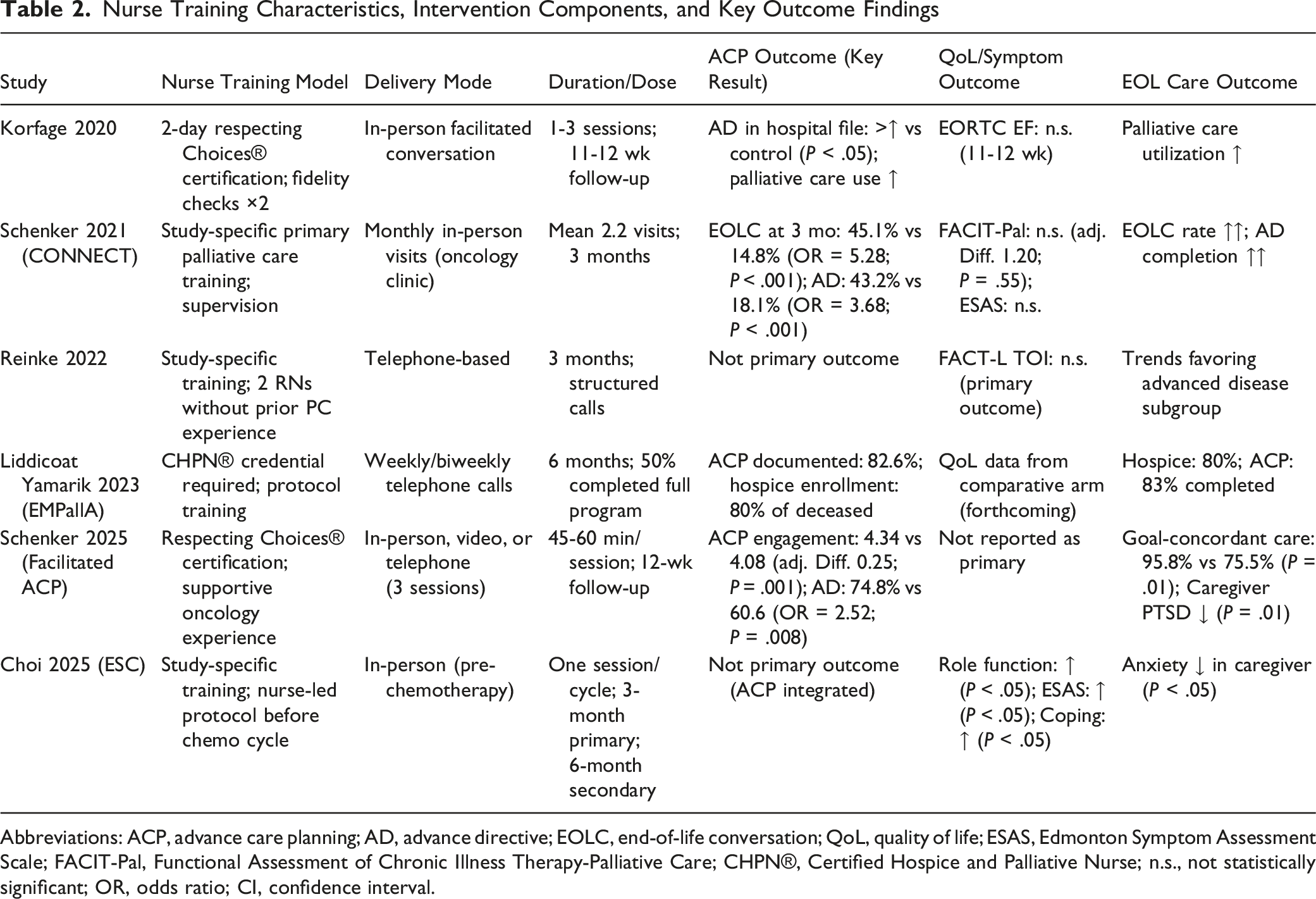
Abbreviations: ACP, advance care planning; AD, advance directive; EOLC, end-of-life conversation; QoL, quality of life; ESAS, Edmonton Symptom Assessment Scale; FACIT-Pal, Functional Assessment of Chronic Illness Therapy-Palliative Care; CHPN®, Certified Hospice and Palliative Nurse; n.s., not statistically significant; OR, odds ratio; CI, confidence interval.
Risk of Bias Assessment
Risk of bias assessment using RoB 2 revealed a generally low to moderate quality across included studies (Figure 2). Three studies were rated as having low overall risk of bias.14,17,19 Two studies had some concerns, primarily arising from the challenge of blinding participants and care providers to intervention assignment in nurse-led behavioral trials, a limitation inherent to this category of intervention.15,16 One study was rated as low to moderate risk, with concerns about cluster-level allocation and potential differences in care systems across six countries.
19
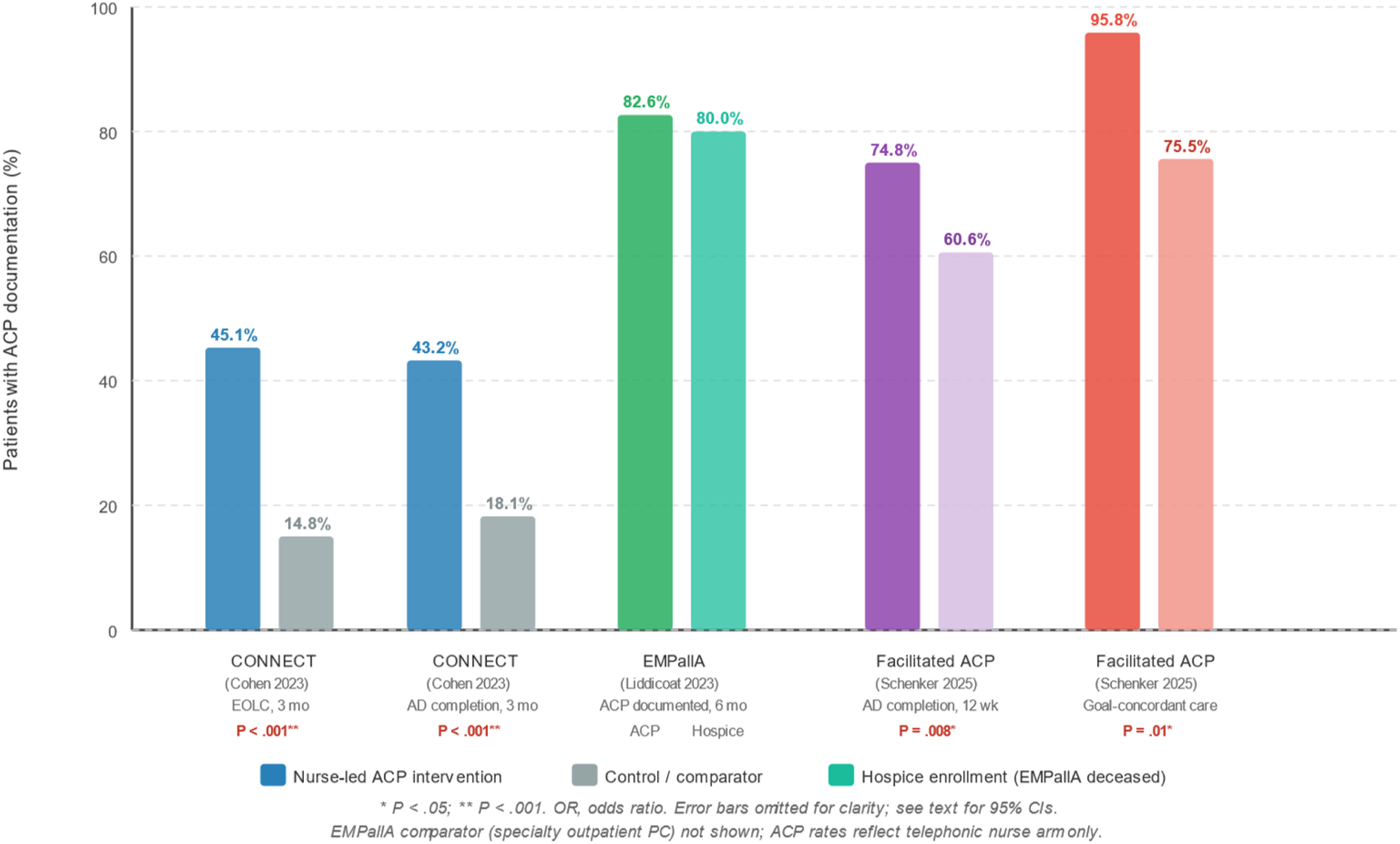
No studies were rated as high overall risk of bias. Across all studies, the randomization domain was rated low risk; missing outcome data were handled appropriately (intention-to-treat analyses or multiple imputation) in five of six studies14,15,17-19; outcome measurement relied on validated patient-reported instruments in all studies (Figure 3). Risk of bias assessment for included randomized controlled trials using the Cochrane Risk of Bias 2 (RoB 2) tool. Each domain is rated as low risk (green), some concerns (amber), or high risk (red). Domains assessed: D1, randomization process; D2, deviations from intended interventions; D3, missing outcome data; D4, measurement of outcomes; D5, selection of reported results; Overall, overall risk of bias judgment Summary of advance care planning engagement outcomes across included studies. Bar chart illustrating the proportion of patients with documented advance directives or completed end-of-life conversations in nurse-led ACP intervention arms vs control arms at primary follow-up. Error bars represent 95% confidence intervals where available. *P < .05; **P < .01 for between-group difference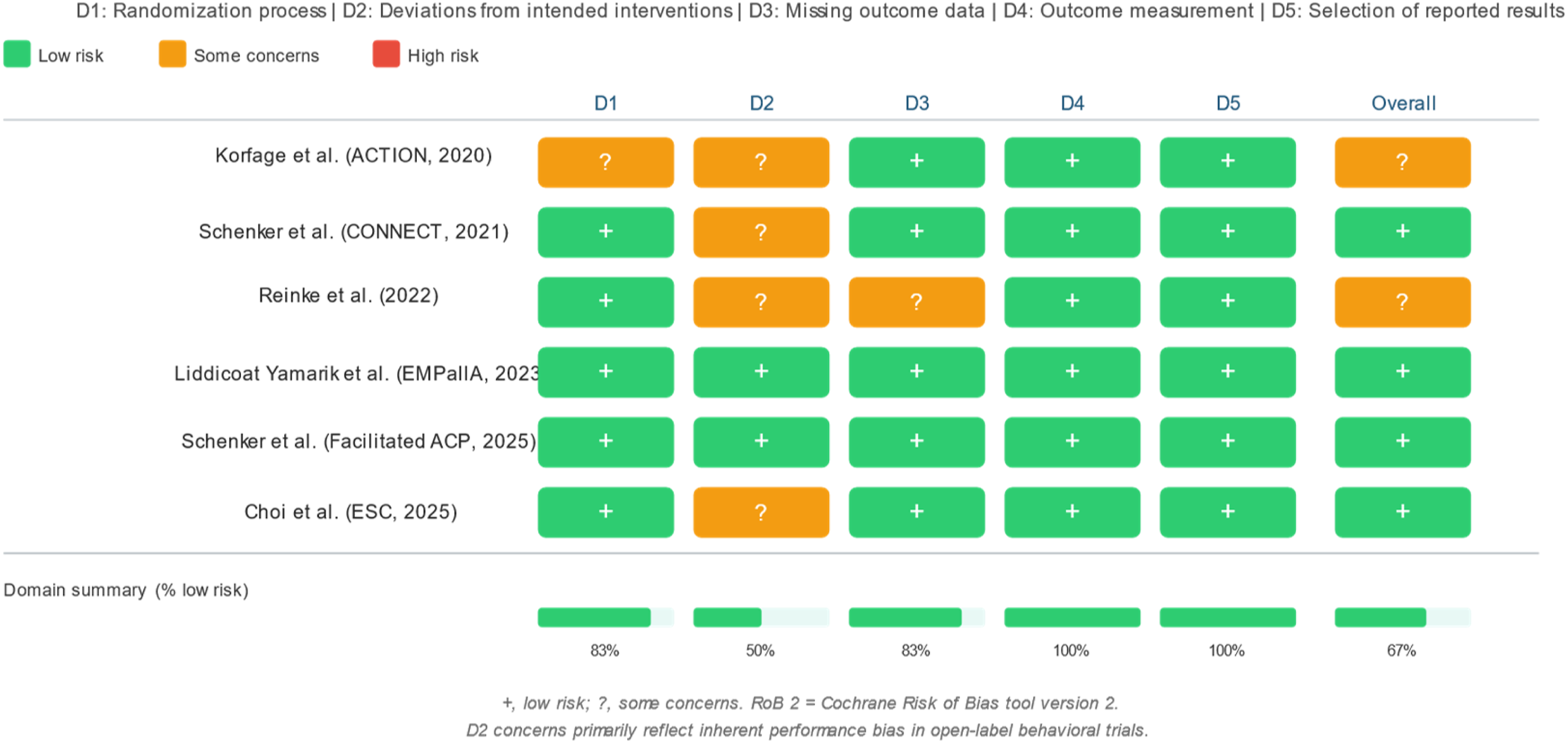
Primary Outcome: ACP Engagement and Advance Directive Completion
Five of six included studies assessed ACP engagement as a primary or major secondary outcome. Across these studies, nurse-led ACP interventions consistently and significantly increased ACP engagement relative to usual care or patient-directed approaches, with effect sizes of clinical and statistical significance.
In the CONNECT trial secondary analysis (Cohen et al, 2023), among patients lacking a documented end-of-life conversation at baseline, 45.1% in the CONNECT arm vs 14.8% in standard care reported having such a conversation at 3 months (adjusted OR = 5.28; 95% CI 3.10-8.97; P < .001). 20 Similarly, 43.2% of patients without a baseline advance directive completed one during the study period in the CONNECT arm vs 18.1% in standard care (adjusted OR = 3.68; 95% CI 1.89-7.16; P < .001). These findings represent a 3.0- to 5.3-fold improvement in ACP uptake attributable to the nurse-led primary palliative care intervention.
The Facilitated ACP trial demonstrated that nurse-facilitated conversations produced superior ACP engagement compared with patient-directed tools at 12 weeks (mean score 4.34 vs 4.08 on a 0-5 validated engagement scale; adjusted difference 0.25; 95% CI 0.10-0.40; P = .001). 17 Advance directive completion was substantially higher in the facilitated arm (74.8% vs 60.6%; OR = 2.52; 95% CI 1.27-5.00; P = .008), a clinically meaningful difference translating to a 23% absolute increase in AD documentation. Bereaved caregivers in the facilitated ACP arm also reported significantly higher rates of goal-concordant care (95.8% vs 75.5%; P = .01) and fewer post-traumatic stress symptoms (IES-R 23.9 vs 31.5; P = .01).
In the ACTION trial, although no significant difference was observed in quality of life between intervention and control arms, advance directives were documented in hospital files significantly more often in the intervention arm. 19 The intervention arm also utilized specialist palliative care more frequently. Among the 218 advanced cancer participants in the EMPallA telephonic arm, 82.6% completed at least one documented ACP activity during the 6-month program, and 80% of those who died subsequently enrolled in hospice, a rate substantially exceeding national benchmarks. 16
Secondary Outcome: Quality of Life and Symptom Burden
Five studies assessed health-related quality of life (HRQoL) as a primary or secondary outcome, with heterogeneous findings. Three trials reported no statistically significant improvement in HRQoL at 3 months compared with standard care, whereas two trials demonstrated significant positive effects on specific domains of functioning and well-being.
The CONNECT trial—the largest US cluster-RCT of nurse-led primary palliative care in advanced cancer—found no significant difference in overall quality of life (FACIT-Pal) between the CONNECT and standard care groups at 3 months (mean score 130.7 vs 134.1; adjusted mean difference 1.20; 95% CI −2.75 to 5.15; P = .55), nor in symptom burden (ESAS total score: 23.2 vs 24.0; P = .11). 14 However, intensity-adjusted analyses suggested a larger estimated treatment effect for patients who received the full three-visit intervention dose, raising the possibility that insufficient dosing may have attenuated the overall effect. Similarly, the Reinke trial found no significant difference in FACT-L Total Outcome Index scores at 3 months between nurse-led and usual care arms in the overall lung cancer population. 15
In contrast, the ESC trial reported that nurse-led enhanced supportive care significantly improved role functioning (EORTC QLQ-C30 role domain), symptom management (ESAS), and coping (Brief COPE) at 3 months compared with control, with sustained effects at 6 months for symptom management and coping. 18 Caregiver anxiety was also significantly lower in the ESC intervention arm at 3 months. The ACTION trial likewise found no significant overall QoL difference (EORTC emotional functioning subscale) at 11-12 weeks, although palliative care utilization was notably higher in the intervention arm. 19
Across studies reporting mood outcomes, nurse-led ACP interventions were associated with non-significant reductions in anxiety and depression scores, with the exception of the ESC trial, which documented significant anxiety reduction. These findings parallel the broader ACP literature, in which effects on HRQoL are more consistently observed in trials with higher intervention intensity and longer follow-up periods.
Secondary Outcome: End-Of-Life Care Utilization and Hospice Enrollment
Nurse-led ACP interventions demonstrated consistent, clinically meaningful effects on end-of-life care utilization. In the EMPallA advanced cancer subgroup, 80% of participants who died subsequently enrolled in hospice—a rate exceeding typical hospice enrollment for advanced cancer patients in similar settings. 16 The 6-month telephonic format, with systematic ACP embedded throughout, appeared to facilitate timely identification of patients approaching end of life and proactive hospice transition planning.
In the ACTION trial, despite the absence of a significant QoL benefit, patients in the intervention arm utilized specialist palliative care services more frequently than controls, and advance directives were present in hospital records more often, suggesting downstream effects on healthcare system engagement. 19 In the Facilitated ACP trial, bereaved caregivers of patients in the nurse-facilitated arm reported significantly higher rates of goal-concordant care (95.8% vs 75.5%; P = .01), indicating that nurse-led facilitated ACP improved the correspondence between patients’ documented preferences and their actual end-of-life care. 17
The CONNECT trial demonstrated a significant increase in end-of-life conversation rates (from 14.8% to 45.1%) and advance directive completion (from 18.1% to 43.2%) with nurse-led primary palliative care, outcomes that the broader literature consistently links to reduced aggressive end-of-life interventions and greater hospice utilization. 20
Nurse Training and Intervention Fidelity
All six included studies incorporated formal nurse training prior to intervention delivery, though the training models varied in structure, duration, and content. Three studies utilized the Respecting Choices® framework, which requires a competency-based certification process typically spanning 2-3 days.17,19 The CONNECT and ESC trials developed study-specific training programs focusing on shared care planning, primary palliative care skills, and communication techniques.14,18 The EMPallA program required nurses to hold prior Certified Hospice and Palliative Nurse (CHPN®) credentials, supplemented by program-specific protocol training. 16
Fidelity assessment was reported in four studies.14,16,17,19 The ACTION trial conducted formal fidelity checks twice per nurse, assessing adherence to the structured ACP conversation protocol. 19 The CONNECT intervention included structured visit templates and supervision. Fidelity monitoring was positively associated with outcome consistency where data were available. Studies with more structured and reproducible training and fidelity monitoring tended to demonstrate more significant ACP outcome improvements, suggesting that standardization of the nurse training process is a critical determinant of intervention effectiveness.
Discussion
Principal Findings
This systematic review synthesized randomized controlled trial evidence from six unique studies encompassing 2816 patients with advanced cancer and 7 publications, representing the most comprehensive evaluation of nurse-led ACP interventions in this population to date. The principal findings are threefold. First, nurse-led ACP interventions consistently and substantially improved ACP engagement outcomes, including advance directive completion and documented goals-of-care conversations, with adjusted odds ratios ranging from 2.5 to 5.3 relative to standard or patient-directed care. Second, the effect of nurse-led ACP on overall health-related quality of life was heterogeneous across trials, with consistent positive effects emerging primarily in trials employing higher intervention intensity and more structured delivery. Third, nurse-led ACP was associated with meaningful improvements in end-of-life care quality, including higher hospice enrollment rates, greater goal-concordant care, and reduced psychological burden among bereaved caregivers.
Mechanisms of Effect and Intervention Heterogeneity
The superior performance of nurse-led ACP in improving documentation outcomes relative to quality of life is consistent with a plausible mechanism pathway: structured, facilitated conversations increase the likelihood of patients articulating and recording their preferences, which in turn shapes end-of-life care decisions. The relationship between ACP documentation and quality of life is more distal and may require sustained engagement over months to translate into measurable HRQoL improvements. This observation aligns with the CONNECT trial’s intensity-adjusted analyses, which identified a larger treatment effect for patients completing all three intervention visits, 14 and with broader evidence that palliative care interventions require minimum dosing thresholds to generate HRQoL benefit.5,6
The superiority of nurse-facilitated ACP over patient-directed tools, as demonstrated in the Facilitated ACP trial, merits particular attention. 17 While patient-directed digital and written tools offer low-cost scalability, they may inadequately address the emotional complexity of end-of-life decision-making, the informational asymmetries inherent in serious illness, and the relational dimensions of preference formation that nurses are particularly adept at navigating. The interaction between a trained nurse facilitator and a patient facing advanced cancer provides a scaffolded, empathic context in which values clarification and preference articulation can occur more naturally than through asynchronous self-directed tools.
Heterogeneity in outcomes also partly reflects differences in comparator conditions. Trials comparing nurse-led ACP against standard care (where ACP is largely absent) predictably demonstrate larger effect sizes on ACP documentation outcomes.14,20 Trials comparing nurse-led against patient-directed ACP identify more refined differences in facilitation quality. 17 The multicountry ACTION trial, conducted in settings where palliative care integration and AD documentation norms vary substantially, showed more modest ACP outcome effects against a background of heterogeneous usual care. 19
Comparison With Prior Reviews and Literature
The findings of this review are broadly consistent with prior scoping reviews of nurse-led ACP, which have identified positive effects on ACP engagement, AD completion, and patient-surrogate preference concordance, while noting inconsistent effects on HRQoL.10,11 The present review advances prior syntheses by restricting to RCT evidence and advanced cancer populations, thereby providing a more internally valid estimate of effect. Our finding of consistent ACP documentation improvements aligns with the recent meta-analysis by Liao and colleagues (2025), which pooled 14 ACP RCTs in advanced cancer and reported a significant improvement in AD completion (pooled OR = 7.93; 95% CI 2.76-22.77), though with substantial heterogeneity; notably, several included trials in that analysis involved nurse-led or nurse-co-led models.
The predominantly null effects on HRQoL contrast with the ENABLE II and Temel trials, which demonstrated significant HRQoL benefits from nurse-led palliative care programs in advanced cancer.5,21 This discrepancy likely reflects the broader scope of those interventions: ENABLE II and the Temel trial encompassed continuous palliative care integration with sustained symptom management, psychosocial support, and ACP as components of a comprehensive program, rather than ACP as the primary intervention focus. These comparisons suggest that optimal nurse-led models may need to integrate ACP within a more comprehensive primary palliative care framework to achieve HRQoL benefits alongside documentation improvements.
A further interpretive consideration concerns the conceptual relationship between ACP and palliative care. In several included trials, ACP was delivered as one element of a broader primary palliative care programme that also encompassed symptom management, psychosocial support, and care coordination (for example, CONNECT 14 and the EMPallA telephonic programme 16 ), whereas in others structured ACP facilitation was the predominant or sole focus (for example, the Facilitated ACP trial 17 ). Because the outcomes of a comprehensive palliative care intervention need not coincide with those of ACP delivered in isolation, the direction and magnitude of effect synthesised here should be interpreted with this distinction in mind. The observation that consistent quality-of-life benefits emerged chiefly in the more comprehensive, higher-intensity programmes is itself consistent with this interpretation, and underscores the need for trials that explicitly disentangle the specific contribution of ACP from that of the wider palliative care package within which it is frequently embedded.
Clinical and Policy Implications
The consistent evidence that nurse-led ACP improves ACP engagement carries significant implications for clinical practice. Oncology nurses should be systematically trained, empowered, and reimbursed to initiate and document goals-of-care conversations as a standard component of advanced cancer nursing practice. Training models—whether Respecting Choices®, CONNECT-style shared care planning, or other evidence-based frameworks—should include competency verification and fidelity monitoring to ensure reproducibility. The CHPN® credential requirement in the EMPallA program represents one model of quality assurance, though the heterogeneous outcomes across nurse training approaches suggest multiple pathways to competency are viable.
From a health systems perspective, nurse-led ACP models offer a scalable solution to the specialist palliative care workforce deficit. By equipping frontline oncology nurses to deliver primary ACP within routine cancer care—whether in ambulatory clinics, via telephone, or through telehealth platforms—health systems can extend high-quality ACP to patients who would otherwise lack access to specialty palliative care. 22 The telephonic model employed in the EMPallA trial is particularly noteworthy as a mechanism for reaching geographically dispersed or mobility-limited patients. 16
The finding that nurse-led facilitated ACP significantly improves goal-concordant care and reduces caregiver psychological distress after bereavement18 aligns ACP practice with its ultimate ethical purpose: ensuring that patients with advanced cancer receive care that reflects their values and relieves the decisional burden on family members. These downstream outcomes should be incorporated into the standard outcome frameworks of future nurse-led ACP trials.
Two features of the present evidence base temper the strength of inference that can be drawn about nurse-led ACP specifically. The first is the heterogeneity of the nurses who delivered the interventions. Across the included trials, ACP was provided by personnel ranging from registered nurses without prior palliative care experience (the Reinke trial 15 ) to nationally certified hospice and palliative nurses (CHPN®-credentialled nurses in the EMPallA programme 16 ) and formally certified Respecting Choices® facilitators.17,19 Because the scope of practice, prescriptive authority, educational preparation, and ACP-specific training of registered nurses, advanced practice nurses, and nurse practitioners differ substantially across—and even within—health systems, the available data cannot isolate the effect of nurse type or credential on ACP outcomes. Determining which level of nursing preparation is necessary and sufficient for effective ACP delivery is central to workforce planning and to the design of reimbursement policy, and should be an explicit objective of future comparative trials.
The second feature is the nature of the comparator. In most included trials, nurse-led ACP was compared with usual care, in which structured ACP was largely absent; the benefits observed therefore reflect, in part, the value of providing ACP at all rather than the distinct value of the nurse as the delivering professional. Only two trials permit a more discriminating comparison: the Facilitated ACP trial contrasted nurse-facilitated ACP with patient-directed tools, 17 and the EMPallA trial compared nurse-led telephonic palliative care with specialty, physician-led outpatient palliative care. 16 Rigorous head-to-head comparisons of nurse-led vs physician- or social-worker-led ACP, incorporating both clinical effectiveness and cost, remain scarce and represent a prerequisite for building a robust economic case for reimbursing nurse-delivered ACP.
Limitations
Several limitations of this review warrant acknowledgment. First, despite systematic search strategies and a broad eligibility framework, relatively few RCTs meeting strict inclusion criteria were identified, limiting the diversity and generalizability of the evidence base. Second, the substantial heterogeneity in ACP definitions, outcome measures, and follow-up periods precluded quantitative synthesis and rendered effect size comparisons across studies approximate. Third, the risk of performance bias inherent in behavioral trials—where blinding of participants and nurses to intervention assignment is practically impossible—is an irreducible limitation of the field. Fourth, four of six included studies were conducted in the United States, raising questions about generalizability to other healthcare systems with different ACP regulatory environments, nursing education standards, and end-of-life care cultures. Fifth, the Reinke trial enrolled patients across all lung cancer stages, and its generalizability to advanced cancer populations specifically requires cautious interpretation. Finally, the absence of long-term follow-up data beyond 3-6 months in most trials limits conclusions about the durability of ACP interventions in a population with declining prognosis. In addition, as discussed above, the included interventions were delivered by nurses of heterogeneous type and credential and were predominantly compared with usual care rather than with ACP led by other professionals, so the present evidence cannot fully isolate the contribution of the nurse as the delivering clinician; moreover, because ACP was frequently embedded within broader palliative care programmes, its specific effects cannot always be separated from those of the wider intervention. Finally, the restriction of this review to advanced cancer means that its findings should not be extrapolated uncritically to upstream ACP or to non-cancer populations.
Conclusions
This systematic review demonstrates that nurse-led ACP interventions are effective in improving advance care planning engagement—including advance directive completion and documented goals-of-care conversations—among patients with advanced cancer, with consistent evidence across geographically and methodologically diverse RCTs. Effects on health-related quality of life are heterogeneous and appear to require higher intervention intensity and integration within comprehensive palliative care frameworks to manifest consistently. Nurse-led facilitated ACP is superior to patient-directed approaches in improving ACP engagement, and is associated with meaningful improvements in goal-concordant care and reduced caregiver burden.
These findings support the systematic integration of nurse-led ACP into advanced cancer care pathways. Nurses should be equipped with structured, evidence-based training and fidelity monitoring systems, and reimbursement models should explicitly recognize nurse-delivered ACP as a billable clinical activity. Future research should prioritize: (1) head-to-head comparison of distinct nurse ACP training models; (2) identification of optimal timing, dose, and follow-up frequency; (3) development and validation of standardized ACP outcome instruments specific to advanced cancer; and (4) expansion of RCT evidence to diverse racial, ethnic, and international populations. As the global burden of advanced cancer continues to grow and specialist palliative care resources remain critically insufficient, nurse-led ACP represents a high-value, scalable, and patient-centered solution to one of oncology’s most persistent care quality deficits.
Footnotes
Authors Contributions
Shaomin Wu: Conceptualization, Methodology, Formal analysis, Writing – original draft. Zhuangli Zhu: Methodology, Investigation, Data curation, Writing – original draft. Chun Li: Investigation, Data curation, Validation, Writing – original draft. Lili Xing: Conceptualization, Supervision, Project administration, Writing – review & editing. All authors read and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and analyzed during the current study available from the corresponding author on reasonable request.