
Abstract
Background
Older adults living with serious illnesses face challenging decisions with illness progression. Advance Care Planning (ACP) presents an opportunity to explore values and goals, absent the pressure of time-sensitive decisions.
Participants
Community-dwelling adults ≥65 with an estimated 33% mortality risk, and if invited by the participant, the person who would serve as their surrogate decision maker (SDM).
Setting
Primary care practices in a Midwest metro area. Interviews occurred in the patient’s home or other preferred location.
Methods
Qualitative, descriptive study analyzing ACP conversations that used the Respecting Choices Advanced Steps (RCAS) framework, which includes the opportunity to complete an Indiana POST form. Interviews were conducted at baseline and 1 year later. Interviews were digitally recorded, transcribed, and then analyzed using an inductive content analysis approach.
Findings
Participants included 22 patients and 8 potential surrogates. Themes included reasons for ACP, living well, and impact of serious illness. When expressing preferences for future treatment, many participants selected limited interventions until they realized this did not include cardiopulmonary resuscitation. After learning this, participants often selected full intervention and full code because they wanted a chance to re-establish an acceptable quality of life.
Conclusion
Some older adults with a high mortality risk desire resuscitation and ICU care because they want a chance at getting back to a preferred state of living well. If a patient survives these interventions, SDMs are likely to encounter decisions about whether further life-sustaining treatment can achieve a patient’s goals and values and their perspectives on what living well means.
Keywords
Introduction
Older adults living with one or more serious illnesses often face challenging decisions as the burdens of life prolonging treatment increase and the benefits decrease.1,2 Advance care planning (ACP) is a process that prepares people and surrogate decision makers for future communication and medical decision making. 3 One goal of ACP is to identify a patient’s values and goals and ensure that the treatments they receive are consistent with them.4-6 When surrogates are included in the ACP process, it reduces decision making related distress and improves their ability to make decisions on behalf of the patient. 7 Moreover, patients are more likely to receive their preferred treatment at the end-of-life.7,8
Effective ACP features high quality communication to support values-based informed preferences that are documented and integrated into the healthcare system, so information is available when there is a need to make treatment decisions.3,7,9 POLST, a portable medical order form is often used to document treatment preferences for older adults living with serious illness. 10 When signed by a licensed clinician, POLST medical orders are valid in the community and across the healthcare system. The Indiana version of POLST is the Physician Orders for Scope of Treatment (POST) form. Research suggests that POLST is associated with numerous positive ACP outcomes. 11 Due to the time required to conduct robust ACP discussions, initial POLST conversations may be facilitated by trained individuals and then reviewed by a licensed clinician before signing. 12 Respecting Choices® Advanced Steps TM (RCAS) is one training program developed to prepare non-clinicians to take on the ACP facilitator role using a standardized, structured approach. 13
The Planning Ahead randomized trial sought to determine if ACP discussions conducted by a trained nurse facilitator using RCAS would improve outcomes among community dwelling older adults. We conducted qualitative analysis of transcribed digital audio recordings of the initial RCAS conversation intervention and a RCAS conversation 1 year later to explore factors that may influence preferences for treatment.
Methods
Setting
Participants were recruited from primary care practices in a Midwest metro area. The intervention was conducted at a location specified by the patient. The study was reviewed and approved by the Indiana University Institutional Review Board (protocol # 1905850231). Written informed consent to participate was obtained for all participants in the study. The informed consent included a statement of voluntariness for participation and the assurance that published results would be anonymized.
Participants
A convenience sample of 22 patients and 8 study partners from the larger Planning Ahead study provided data for this qualitative research. 14 The research team selected the first 22 study participants that were randomized to receive the RCAS intervention and were alive at 1 year following the initial intervention due to the longitudinal nature of the project and funding resources. Eligible participants for the Planning Ahead parent study were living in the community, receiving primary care from a participating provider, and did not have a POST at baseline. Eligibility was restricted to participants with an estimated 1 year 33% mortality risk assessed using the Gagne index calculated with ICD-10 codes present in the medical record(≥7)15-17 or a similar estimated 1-year mortality using disease specific indices. Exclusion criteria included acute illness, current hospice enrollment and an inability to complete study activities in English. Participants had the opportunity to include the person they would want to be their healthcare decision maker in the interview. Although individuals who lacked decision making capacity were included in the parent study, only participants with capacity are included in this analysis.
Procedures
The study began in May 2020 and completed enrollment in 2024. Study procedures have been published elsewhere. 14 After enrollment, participants who were randomized into the intervention group participated in an RCAS interview. As part of the study, and consistent with the RCAS model, participants were encouraged to and given the opportunity to formally designate a surrogate decision maker as their legal representative and invite that person to participate as a study partner. 14 As in the initial intervention, participants agreeing to complete a 1-year follow-up interview were invited to include a study partner.
Nurses with >10 years of experience (SK critical care and MC geriatrics) completed a VitalTalk mastering tough conversations course, RCAS facilitator training and conducted all the RCAS interviews. They were unknown to the participants prior to the RCAS interviews. The RCAS structured conversation first provides patients an opportunity to explore their values and goals in a broad sense before moving to discussion about specific preferences for future treatments. When discussing specific preferences, the RCAS conversation focuses on three treatment options (Full treatment, selective treatment and comfort focused treatment) that support patient’s goals of care and that align with options available on POST orders for medical interventions. Full Treatment/No Limitations on Medical Interventions are recommended when prioritize living longer. Selective Treatment/Limited Medical Interventions are recommended when participants prioritize maintaining their current health and want to avoid intensive care and intubation. Comfort-Focused Treatments are recommended when participants prioritize comfort-focused care.
After summarizing what is learned, the facilitator reviews each section of the POST form with the participant and moves to a discussion about goals of treatment. Only after priorities are addressed does the facilitator offer to document decisions about treatment options on a POST form. Participants are told that completion of the POST form is optional. Written decision aids created by the Respecting Choices program are available to share with the participant and their study partner. In the POST model, limited interventions/maintaining function and comfort care are inconsistent with Full Code because a person with serious illness whose heart and breathing stop will most likely require intubation and ventilation which are part of full treatment orders. Participants were approached about engaging in an interview about their experience 1 year after the initial interview.
Data Collection
Initial RCAS interviews and follow-up interviews were digitally recorded and later transcribed. All transcripts were checked against the recording by a member of the research team. Both interviews followed the RCAS framework and additional questions were designed to explore factors that influenced patient preferences for treatment and any factors that contributed to changes in preferences over time.
Qualitative Analysis
The RCAS interview structure provided a framework for analysis of the interview data. The research team hoped to explore factors that influenced preferences for treatment. Data analysis included content from the initial and 1-year follow up interviews. The research team used qualitative inductive content analysis. 18 The process began with line-by-line open coding of transcripts to inductively identify and label ideas. After a sample of transcripts was independently read and coded by the research team (AMT, LDW, SEH, SK, MC) to identify themes, the team met to develop a preliminary list of codes and establish consistency. Three of the researchers (AMT, SEH, LDW) have extensive experience with qualitative research. The remaining transcripts were independently coded by 3 coders (SK, MC, LDW) before meeting as a group to refine the code book as additional interviews were coded. Differences in interpretation of data were discussed until the coders achieved consensus. The team created and maintained a coding dictionary and used memos to track coding decisions. This process continued until all transcripts were coded, though thematic saturation was achieved after 15 interviews. 18 After coding individual cases, the research team used constant comparative analysis across cases to group, categorize, and abstract themes. Data was managed using NVivo. 19 After coding, lists of generic categories were generated to collapse the codes that were similar through an interpretive process and finally categories were abstracted to create themes as a means of describing the phenomenon. 18 To enhance the holistic interpretation of the data, throughout the data gathering process, intervention nurses maintained notes, tracking impressions, ideas and early interpretation of the data that were reviewed and discussed with the other authors. 20
Findings
Participant Characteristics
Patient and Study Partner Demographics
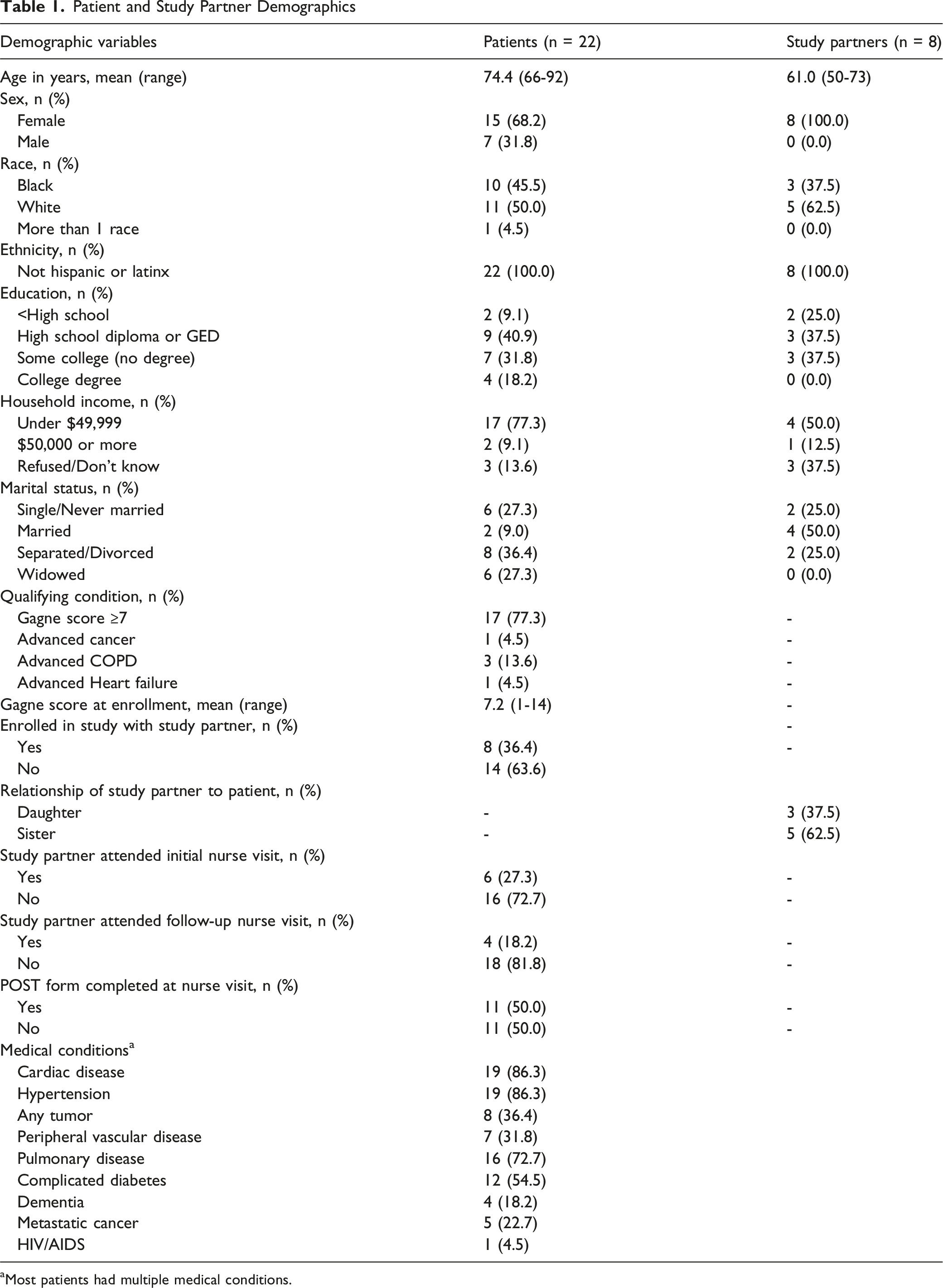
aMost patients had multiple medical conditions.
Themes
Initial analysis yielded 20 codes which were collapsed into 11 categories. Five themes will be reported here using the RCAS interview guide as an organizing structure. The selected themes relate to patient preferences about ACP, including decisions about CPR and medical interventions. All example quotes provided are from participants and not from study partners.
Reasons for ACP
Participants expressed many reasons for wanting to participate in ACP. Many indicated they were interested in ACP primarily due to a desire to protect themselves from receiving medical treatment they did not want or being in a state of health they found unacceptable. Participants also expressed concern that a surrogate would choose something that they did not want for themselves. Prior negative experiences (either their own or of other people close to them), reinforced this rationale for wanting their surrogate to be part of ACP, although few patients (6/22) had potential surrogates participate in the RCAS conversation. Prior conversations with their chosen surrogate about preferences promoted confidence in their choice of surrogate. Patients’ responses illustrated how important it was to them to share their values with a future surrogate.
Understanding of Current Medical Condition
Although all participants in the study had an estimated 33% mortality, many did not describe their illness as being serious and viewed illness progression as a future event they have not yet had to face. There was an acceptance that many medical issues are not curable but are treatable, allowing participants to still enjoy life. Many participants provided comments that illustrate how uncertainty impacted their thinking, especially when pressed to make a choice about preferences for future medical treatments. When presented with the opportunity to express preferences for future treatments, particularly setting limits on treatments, participants would often state they needed more time to process the situation, despite in many cases having lived for years with chronic progressive illnesses.
Living Well
The RCAS uses a framework to support participants in reflecting on what “living well” means to them. Two themes emerged relevant to this topic: getting back to normal and quality of life.
Getting Back to Normal
When asked to clarify what “getting back to normal” meant, participants expressed an appreciation for the way life used to be when they were more independent. Even in the face of advanced, serious illness, participants talked about hoping for restoration. In some cases, treatment preferences were predicated on the expectation that they would be able to return to their existing level of function and remain in their home.
What Gives Life Meaning
Maintaining relationships inspired a sense of purpose for living and was a priority. Participants described that it was the connection with others (family, faith, community and pets) that brought meaning to their life in good and difficult times. Staying active, particularly in ways that reinforced independence, was also central to many patients’ statements about what gave their life meaning. Part of independence was expressed as valuing their cognitive abilities over their physical abilities. They described not wanting medical interventions if they lost the ability to appreciate those around them and even a desire to stop burdensome interventions if their mind was irreversibly impaired.
Impact of Serious Illness Experiences
Participants used their serious illness experiences to inform their thoughts about their own future illness trajectory. Some participants described previous experiences with their own and others’ serious illness and how it motivated them to participate in some form of ACP (complete an advance directive, have conversation with family). The impact these experiences on them often motivated them to identify limits to what they would consider for their own care as their illness progressed. In some cases, when asked about serious illness experiences, a participant did not initially report experience with serious illness. However, later in the interview they would spontaneously describe an experience that a healthcare provider would likely consider serious illness (eg, previous hospitalization, family member who was treated for cancer, etc.).
This quote exemplifies the impact of serious illness on future treatment preferences. At the 1-year follow-up RCAS interview, when the patient was reminded of preferences identified at the initial interview (full interventions), after acknowledging significant illness progression and a current preference to avoid CPR she offered clarification of her preferences.
The Moment of Truth - Stating a Treatment Preference
As part of the RCAS framework, the facilitator introduced three overall goals of medical care described previously. Based on what they had learned from listening to the patient describe their preferences and experiences the ACP facilitator would suggest one of the three goals to the participant. Because many participants had acknowledged that their medical problems could not be cured, the overall goal of maintaining current health was often suggested and affirmed by participants. However, when asked to decide about preferences for future treatment, several participants selected full interventions and full code status, despite acceptance of the non-curative nature of their current condition and describing wanting to avoid negative outcomes. They maintained their preference even when they were provided with additional information about CPR, including that patients who survive CPR would be admitted to the ICU, need a ventilator, and have a low likelihood of recovery, including a low likelihood of returning to their current cognitive and physical function after the resuscitation event. Participants who expressed a preference for CPR indicated that they wanted a chance to return to their current life and level of activity, even if it was unlikely.
Some patients expressed wanting life-sustaining treatment only if it would be effective:
Facilitator Field Notes
The experiences of the intervention nurses facilitating these conversations provide some additional insight into the themes that emerged during these interviews. As noted above, the intervention nurses would, after summarizing the patient’s values and goals, often suggest a treatment goal consistent with maintaining current health, a choice that precludes CPR in the POST framework. Invariably, participants initially affirmed the intervention nurses’ reflection that they preferred a plan of care focused on maintaining function until they learned that “maintaining current health” did not include CPR. At this point, many changed their mind and instead expressed a preference for full interventions. The intervention nurses perceived that the opportunity to set limits on future treatments seemed to make participants uneasy. Even when participants identified limits to what they would accept and affirmed the intervention nurse’s understanding of their values, if participants wanted a chance at returning to normal, the selection of full interventions was their only option.
Discussion
This analysis of structured ACP discussions found that older adults with serious illness value living well, can imagine future states of illness that they would consider unacceptable, and can specify limits to what they would find an acceptable quality of life. Participants were motivated to participate in ACP, underscoring the importance of sharing their values with a future surrogate. Most felt that their current quality of life was acceptable, while acknowledging the ongoing need for medical treatments and their functional limitations. If they were to need treatments in the future, an important goal would be to get back to “normal.”
These findings reinforce outcomes from studies of other populations that describe the value of ACP as protecting participants from experiencing treatments that would be highly burdensome and that would be unlikely to lead to outcomes that the participant would find acceptable. 21 Like the findings of others, participants in this study were focused on living well, valued relationships and those relationships influenced preferences for future medical treatment. 22
A surprising finding was that among this population of older adults with increased mortality risk, many who believed that the overarching goal of their healthcare was to maintain current health rather than be cured still desired life sustaining treatments including CPR and ICU care. Many of the participants who acknowledged their serious illness and voiced an acceptance of death stated that their overall goal of treatment was to maintain their current health but were unwilling to give up on a chance of their lives being saved, despite being presented with statistics about the complications for survivors of CPR. This suggests it may be helpful for ACP interventions and decision aids to detail changes in quality-of-life outcomes for older adults who survive ICU admissions rather than just provide survival statistics that may have less relevant meaning for older adults. 23
However some patients who preferred CPR and full interventions could identify circumstances under which they would not want continued life-sustaining therapies. Honoring a patient’s underlying values and goals depends on their surrogate’s knowledge of the person’s limits so this finding underscores the importance of revisiting preferences when a person’s condition changes and the importance of focusing on the conversation 24 and documentation of reasons and values behind the chosen treatment options. At least one study demonstrated that when participants in ACP report high quality communication around POLST, they report being more satisfied with their decisions. 25
Although the literature on ACP focuses on eliciting an individual’s preferences, our findings suggest that asking patients to state preferences about treatment where the choices are black and white led them to pick an option likely to impose aggressive treatment with little chance of satisfactory recovery and lead to the need for surrogates to make decisions for them. One participant’s comments illustrate this point very well
However, other patients expressed a desire to spare family members from the burden of decision making. When patients’ surrogates do not participate in ACP conversations with the patient, and they see the patient has elected CPR they will be exposed to burdens of difficult decisions which is a circumstance many patients want to avoid. The default choice to select full interventions is consistent with previous work that showed the flaws in a strategy that focuses on survival rather than planning for anticipated escalation of treatments as health declines. 26
Findings seem to suggest a need for the development of an alternative framework that differs from the widely accepted model that is so prevalent in modern medicine and serves as the foundation of the RCAS and POLST programs. When a patient with an underlying serious illness experiences an acute event, where recovery without significant negative impact on functionality is unlikely, providing life sustaining treatment may be considered medically inappropriate and medical teams may recommend not providing those treatments. 27 However, our study found that several patients with serious illness viewed the appropriateness of CPR and ICU level care differently. They thought these interventions were reasonable because they provided a chance of getting back to their current quality of life.
When asked about their knowledge of CPR in the present study, patients acknowledged that what they have seen on TV has influenced how they think about their preference for CPR. TV portrayals of unrealistic survival rates may misinform viewers and may influence treatment preferences for patients facing serious illness. 28 This may explain why showing patients information about statistical survivability did not influence their treatment preferences. It is also possible that these patients who were still living in the community were not ready to make decisions about treatment limitations despite being seriously ill because they were still experiencing an acceptable quality of life even in the face of declining health. Quality of life assessments are impacted by more than symptom burden. 29 Moreover, uncertainty of future health states played a role in influencing choices. The healthcare system that honors a choice to “have a chance” must do a better job of engaging patients and surrogates in identifying the meaning of chronic progressive illness (frailty). 26
In a fractured healthcare system where care provided in the hospital may be provided by people who have never met the patient prior to hospitalization, the consistency that patients desire and deserve will likely need to come from engaging potential surrogate decision makers in conversations and building trust in the information provided during an acute deterioration of a patient’s health. Consistent with previous research,26,30-32 patients in this study may have a lack of shared meaning with providers regarding terms like frailty and serious illness, or an appreciation for how these terms apply to them and impact decisions about treatment escalation.
Our finding that patients value the process of ACP, especially to prevent unwanted care and choose the appropriate surrogate, provides evidence for the continued widespread use of ACP. Patients were able to express their illness understanding, share their values and goals and incorporate these into selecting treatment preferences for future medical care. However, what serious illness means to them seems different than what it means to healthcare professionals.
Limitations
The data for this analysis was based on a convenience sample of participant interviews from a larger study. While the results are meaningful, it is not clear if they are representative of the broad range of perspectives in the overall population. Additionally, it is possible the use of a non-clinician facilitator is a limitation. Because the RCAS program prepares non-clinicians to facilitate ACP conversations, the model emphasizes neutrality in presenting treatment options. It is possible that clinicians who are accustomed to making recommendations about treatment options would be more directive (eg, advising against CPR/Full Interventions) in ways that would be acceptable to patients and surrogates.
Conclusions
This qualitative study illustrated the challenges of translating preferences into information that can guide future medical care. Many patients can imagine a future time when they would set limits, but when they assessed their current quality of life as acceptable, they were willing to accept advanced clinical life-support interventions. Even people with incurable illnesses want a chance to return to “normal”; their current health.
Given the harms of CPR and the popular myth that recovery with satisfactory quality of life is the norm,33,34 it should not be surprising that even patients with significant risk for mortality choose full code. In the absence of documentation of the reasons for patient treatment choices, a choice for full interventions may lead to outcomes that are seemingly inconsistent with patient values and preferences. Truly honoring a preference to have a chance means they need an informed surrogate, reinforcing the importance of helping patients identify a surrogate decision maker and promoting and documenting engaged discussions, not just with the patient, but with the patient and their chosen surrogate.
Footnotes
Ethical Considerations
This study received ethical approval from the Indiana University IRB (protocol # 1905850231September 9, 2020.
Consent to Participate
All participants provided written informed consent prior to participation in the study.
Consent for Publication
Part of the written informed consent included the potential for anonymized publication of study results.
Author Contributions
Removed for de-identification
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Institute on Aging (R01AG056618). ClinicalTrials.gov ID: NCT04070183. Dr. Torke is also supported by a Midcareer Investigator Awards in Participant-Oriented Research (K24AG053794). The manuscript for the Clinical Trial Number (NCT04070183) was registered on August 4, 2019 with the Clinical Trial Registry.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article’.
Clinical Trial Registration
The manuscript for the Clinical Trial Number (NCT04070183) was registered on August 4, 2019 with the Clinical Trial Registry.