
Abstract
Introduction
Hospital readmissions in the US place a considerable burden on patients and their caregivers. Our study will investigate whether spiritual intervention during a patient’s hospital stay contributes to lower rates of readmissions 30 days after hospital discharge.
Methods
Two hundred patients receiving palliative care will be randomized into control (n = 100) and intervention groups (n = 100). The control group will receive a standard spiritual support visit, while the intervention group will receive a spiritual intervention consisting of active listening, compassionate presence, assessment of post-discharge resources, and a supportive phone call 5 to 7 days after discharge. The primary outcome will be hospital readmission within 30 days of discharge. Board-certified chaplains will be allowed to use their individual skillsets but within the standardized ACA spiritual care model. Training chaplains to assess patients in the same way will help with this discrepancy as the same form will be used.
Discussion
We hypothesize that patients who receive spiritual intervention with a supportive phone call will experience fewer hospital readmissions. Spiritual intervention will instill.confidence in those patients at risk of readmission by assuring them that the hospital staff remain concerned about their well-being even after discharge.
Introduction
Hospital readmissions constitute a significant burden on hospitals and health systems and are challenging for patients and their family members. Readmissions in the US cost billions of dollars a year, 1 and approximately four million adult readmissions occur annually, with an average cost of $16,000 each. 2 Pyakuryal et al 3 and Wright 4 found that out of 76,936 total index inpatient admissions, there were 11,633 (15.1%) total 60-day hospital revisits; furthermore, of these revisits, 8456 (72.7%) were inpatient readmissions by the Hospital Readmission Reduction Program (HRRP)-targeted conditions, such as pneumonia, heart failure, and chronic obstructive pulmonary disease. Ninety-two percent of 30-day hospital revisits were attributable to just 3 of the 6 HRRP conditions, suggesting the need to include condition specific weights in the HRRP metric along with other potential reforms. 4
Reducing hospital readmissions has the potential of benefit for both the healthcare institution as well as the patient because these excess costs are passed onto future patients to help reduce financial loss. Despite the high number of patients being readmitted outside the limit, many of these readmissions may be preventable if health systems implement targeted measures to reduce them.5–11 Research shows that a key strategy for preventing readmissions is providing support to patients at home after discharge. 12 For example, telehealth and remote monitoring have been shown to allow patients to remain at home rather than being admitted to inpatient units.13,14
Similarly, outpatient interventions improve quality of life, reduce symptom burden, and enhance access to care.15–18 Palliative care (PC) also strives to reduce preventable hospitalizations and has been shown to lower cost of hospitalization and care of patients at home.11,15,19 Furthermore, PC helps to prevent escalation in hospital use.20–25
Both inpatient and outpatient palliative care offer a transdisciplinary approach to care and costs savings in reduced length of stay, especially with its emotional and spiritual arms as core elements. Other interventions have been shown to reduce readmissions, improve management of care at home,26–30 and address certain needs of patients receiving PC within the community. 31
Part of this study is to minimize readmissions from a financial perspective. However, by avoiding readmissions, hospitals are also freeing up beds for other admissions, which is especially important considering bed capacity is strained. In bed capacity limitation situations, patients would need to board to wait for a bed, which is a poor experience and could lead to poor outcomes. While no reimbursement is given for readmissions, by not readmitting those patients, beds are available for reimbursable patients.
Spiritual care clinicians also look for ways to reduce readmissions. Research shows that patients want their spiritual needs addressed to improve their quality of life.32–34 Spiritual care also contributes to increased longevity, improved emotional well-being, a stronger immune system, reduced risk of disease, improved self-confidence, healing, and ability to cope with illness, pain, and life stressor.35,36
Spiritual involvement appears to enhance recovery after illness and surgery.37–40 However, although research exists on the benefits of spiritual support, 41 studies on the effects of spiritual interventions designed to reduce readmissions are scarce, 42 despite hospital administrators recognizing that spiritual care may contribute to cost savings and reduction of readmissions. 43 Spiritual care is often hard to quantify, and this study aims to show its value by trying different approaches and tests to see how additional impacts can be garnered.
Our study will examine the efficacy of spiritual intervention conducted by spiritual care clinicians aimed at reducing readmissions of patients receiving PC occurring within 30 days of hospital discharge. The findings will contribute to the limited evidence on the role of spiritual care in reducing readmissions and the efficacy of spiritual care interventions in this area. Offering adequate support in the patient’s home and implementing a range of strategies from interdisciplinary teams can help reduce readmissions; this also alleviates discomfort and stress that patients and caregivers often experience during hospitalization. 44
Based on clinical practice, our hypothesis is, chaplains, in collaboration with other members of the interdisciplinary team, can help reduce readmissions in the same way, just as they assist patients and their caregivers in understanding treatment options and values, addressing spiritual, emotional, and social concerns, and support patients receiving PC in the decision-making process.
This hypothesis is warranted as a similar spiritual intervention had been shown to be effective in other health care settings and contributed to positive benefits. 39 Thus, the aim of our study is to measure the effectiveness of spiritual intervention on hospital readmissions, explore the benefits of checking on patient well-being and needs after discharge, and assess the impact of spiritual intervention in reducing hospital readmissions.
Methods
Design
This quantitative quasi-experimental research will be conducted over 12 months. A total of 200 patients receiving PC will be randomized into control (n = 100) and intervention group (n = 100). Our team will use Excel’s RAND function (Microsoft Corporation) to generate random sequence. Patients in both groups must be open to receiving a spiritual supportive chaplain visit. This random process has a goal of securing both non-religious and religious backgrounds.
Patients in the control group will receive a standard supportive visit from a board-certified chaplain (BCC). Patients in the intervention group will receive a visit from a BCC who will offer an intervention based on the ACA spiritual care model (active listening, compassionate presence, assessment of access to community and spiritual resources during home stay, and assurance of ongoing spiritual support). Additionally, patients in the intervention group will receive a spiritual supportive telephone call 5 to 7 days after discharge. The call will focus on the patient’s well-being and coping, sources of meaning and support (including non-faith-based resources), and any unmet social or spiritual needs.
Each chaplain encounter will be documented in the electronic health record. In the moment, triage escalation will be done as if someone were experiencing stroke symptoms. /The “I’m just the chaplain” is what we wish to avoid if we are to be considered value-added clinicians. The patient will be told by us to call 911 if they feel it is necessary to go to the emergency department.
If urgent concerns arise during the telephone call (eg, possible medical decompensation, safety concerns, severe distress, or need for same-day clinical follow-up), the chaplain will follow an established escalation pathway (in addition to documentation), which includes notifying the patient’s palliative care team or primary care team according to institutional policy. The BCC will set up a time on the same day to finish the ACA with the patient.
Study Participants
Study participants will be hospitalized adult patients who have received a PC consult at our institution. Each patient will receive a study code corresponding to their medical record number to help with HIPAA and patient privacy. Our plan recruits patients with different diagnoses, because research shows that some diagnoses more frequently cause readmission. 45 This will be considered when analyzing the data. For this study, our focus will not be on a specific illness, but the illness must be classified under PC criteria. Patients meeting inclusion criteria will be adults who return to and reside at home, have the capacity for decision making, and are able to understand and communicate in English. Patients will be excluded if they are younger than 18 years of age, are receiving end-of-life or hospice care or reside at a skilled nursing facility.
Study Procedure
Patients who meet inclusion criteria will be identified by a PC registered nurse who will receive education on the study’s aims, objectives, and participation criteria. Patients will be informed about a visit from a BCC during their first visit with PC clinicians. They will be given the opportunity to ask questions and opt out of the BCC visit. If they decline to participate, they will not be approached again about a visit from a BCC, though visits will be provided if requested. BCC visits will be scheduled at a time convenient for the patient. In addition, these chaplains will assist with palliative care patients and be trained to fill out the form in the same way to ensure continuity of care. Training protocols will be formatted and tested within research team meetings.
Spiritual Intervention
Patients in the intervention group will receive a spiritual intervention (SI) based on the ACA spiritual care model. The BCC providing the SI will attempt to create a space where patients and caregivers can freely share and process their medical journeys, their strengths and weaknesses, and their spiritual needs. The SI will focus on establishing trust, creating connections and confidence in the interdisciplinary group.
The ACA spiritual care model, recently created and introduced at Mayo Clinic, was chosen over similar models, such as the Spiritual Assessment and Intervention Model, 46 because it closely aligns with the study’s goals. Because professional chaplaincy serves patients across religious, spiritual, and non-religious identities, the ACA model in this study will be applied in a patient-centered manner.
For patients who identify as non-religious or non-theistic, the intervention will focus on sources of meaning, values, relationships, legacy, and other supportive communities and resources (rather than faith practices). The chaplain will avoid assumptions of religious affiliation and will offer prayer or other explicitly religious practices only when appropriate and desired by the patient.
Active Listening
The BCC will engage in active listening to build trust, along with creating a foundation for providing compassionate care. Through intentional and active listening, our hope is that patients and caregivers will experience and receive validation, an intentional healing presence, and an opportunity to collaboratively reflect on thoughts, feelings, and spiritual dynamics of their medical journey.
Compassionate Presence
In our research a BCC will function as a compassionate presence throughout the visit to foster a deep connection, creating a safe space for patients and caregivers to share their emotions and feelings and to reflect on their medical journeys. The BCC will also continue to provide empathic listening, offer validation, and minister to any emotions arising during the visit.
Assessment of Access to Spiritual Resources
During the visit, the BCC will gently assess and discuss the spiritual and community support available to the patient after their discharge from the hospital. The proposed assessment process is presented in Figure 1. Recent research highlights the importance of assessing and improving access to spiritual resources for hospital readmitted patients, emphasizing its impact on patient-centered care and outcomes; spiritual care is often underutilized in hospitals, despite its known benefits. Readmission research flowchart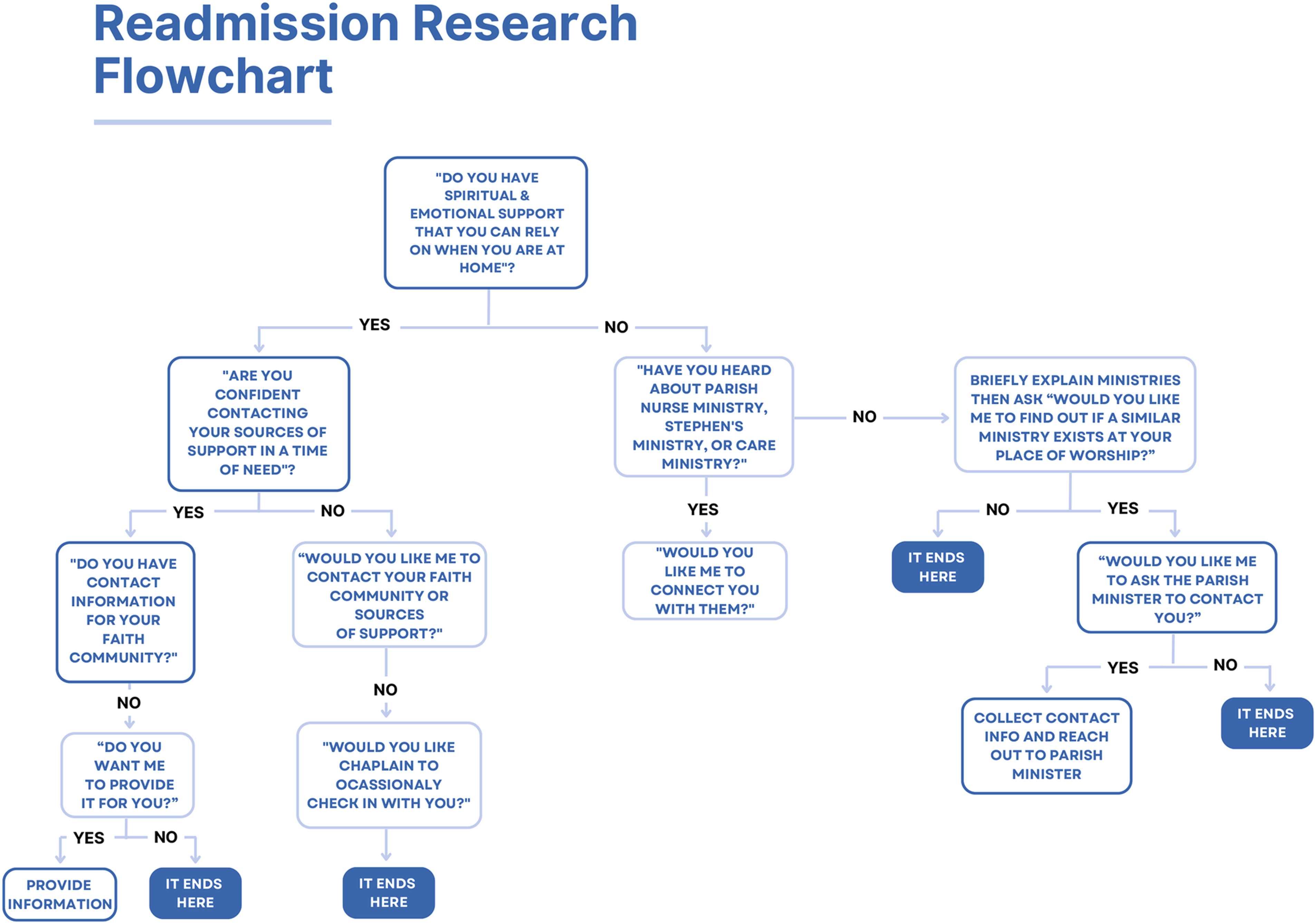
Assurance of Ongoing Spiritual Support
Finally, the BCC will assure patients of spiritual support according to their spiritual or religious needs, background, and context (eg, assurance of prayer). Through this part of the SI, our aim is to create a sense of self-efficacy and coherence in the patient for times of crisis. Spiritual care positively affects the consequences of using health care services, also reduces the duration of hospitalization and accelerates recovery,47–49 the admission and re-hospitalization of the patient,47,50 hospitalization time, and costs. 51
A unique telephone number will be provided to each patient at the end of the BCC visit. The patient will be instructed to call the number in case of distress, when contemplating possible readmission, or when needing spiritual or emotional support. The call will be answered by a BCC who will assess the patient’s needs and coordinate next steps. The same number will be included in the patient’s hospital discharge packet. Patients will also be instructed to call their routine medical emergency number (eg, 911) in case of medical need or emergency. The telephone line will be managed by the spiritual care department using institutional privacy and documentation standards, and any calls that generate a need for clinical follow-up will be routed per the escalation workflow described above. Five to 7 days after hospital discharge, a BCC will make a supportive telephone call to check on the patient’s needs, explore current coping and support (including non-religious supports), offer assurance through prayer when appropriate and desired by the patient, and offer connection to relevant community resources.
When a patient’s preferred faith community does not have identified supportive resources (eg, Stephen Ministers, parish nurses, volunteer visitor programs), the chaplain will offer alternatives from the institution’s community resource list or other community-based support aligned with the patient’s values and preferences. Additionally, an offer for an additional spiritual supportive telehealth visit will be extended.
Interventional fidelity and chaplain variability will be tracked. Following each intervention visit and follow-up call, the BCC will complete a brief structured checklist indicating which ACA components were delivered (active listening, compassionate presence, assessment of resources, assurance/ongoing support) and whether any components were only partially completed due to patient acuity, patient preference, or time constraints. Deviations from the proposed script that are clinically indicated to meet in-the-moment needs will be permitted and categorized (eg, additional crisis support, additional resource linkage). Fidelity data will be incorporated in analysis as descriptive process measures and may be included as covariates or sensitivity analyses to assess whether outcomes vary by degree of intervention completion.
Data Analysis
Thirty days after discharge, data will be extracted from the electronic health record for analysis. Data extracted for statistical analysis will include number of readmissions per patient, diagnoses, number of hospital days, age, sex, race, religious affiliation, and spiritual support patient’s faith or spiritual community or from another source. A regression analysis will be performed to identify possible correlation between variables. Readmission data of every readmitted patient will also be analyzed to investigate possible reasons for readmission. Our quality improvement IRB exempt initiative will adhere to all institutional policies for protection of human subjects.
Discussion
Studies that explore the contribution of spiritual care departments to the reduction of hospital readmissions are scarce. Although research on spiritual care has been increasing over the last few decades,52,53 the financial contribution of chaplaincy to health care has not been explored adequately. This may be because measuring the economic value of SI is challenging. However, Medicare has recently included certain selective SI as billable services, 54 meaning spiritual care departments can be involved in producing revenue for involved health care systems. Spiritual care is becoming professionally recognized as an equal and respected clinical discipline, as shown by spiritual care departments gaining field of rank as an academic discipline in evidenced-based integrated practice. 55 Benefits of spiritual care can have both a direct financial impact on an organization, as well as an indirect impact by lowering expenses through reduced readmissions. Fewer readmissions is the goal but not at the expense of patient safety.
Since the inception of PC and hospice, spiritual care has been an integral component in health care, with chaplaincy embedded as a core service.56,57 This research is situated within the context of PC, as spiritual care appears to be well integrated into practice and it plays a crucial role in an interdisciplinary model of care. The authors of this study include PC and spiritual care clinicians, as well as administrative and support staff.
While this study population may not yield statistically significant results, our aim is to capture data that can serve as a foundation for further studies at other hospitals across the US. Supported by numerous studies as stated in the Introduction, our team is confident that SI aimed at specific outcomes do produce positive results. Assuring patients upon discharge that spiritual support staff care about their well-being and that this support is available may reduce anxiety and provide them with greater confidence, knowing they are not alone. Our availability at their fingertips may be the difference between going to the emergency department or choosing spiritual options. Our goal is to not prohibit them from going to the emergency department or calling 911 if they feel like they need to go for peace of mind.
Although the ultimate goal is not to sway patients from going to the emergency department and having a potential subsequent readmission into the hospital, it is hoped that anxiety may be reduced by SI so that other options may be explored first (eg, choosing a lower level of care). Therefore, by including virtual support from BCC clinicians, readmissions may be avoided, potentially saving money for both the patient and the institution. Finally, while the primary goal is not solely focused on therapeutic benefits, it could enhance patient perception that hospital care can extend beyond its walls through outpatient virtual care offering spiritual care as an alternative to going to the emergency department.
To strengthen attribution of outcomes to chaplaincy (rather than follow-up contact alone), the intervention emphasizes chaplain-specific competencies such as non-directive listening, facilitation of meaning-making and reconciliation, whole-person integration of medical realities with values and identity, and tailored rituals or practices (including but not limited to prayer when desired). These interventions differ from generic follow-up in that they explicitly address spiritual distress, existential concerns, and value-based coping that may influence when and how patients seek acute care.
Our hypothesis that spiritual care can reduce readmissions is informed by a theoretical framework composed by the Concept of Self-Efficacy58,59 and the Sense of Coherence. 60 Self-efficacy theory has been successfully applied in various fields, including gerontology 61 and PC and end-of-life care.62–64 According to Banduras’ Social Cognitive Theory, individuals can harness their cognitive, motivational, and behavioral resources to accomplish tasks and adapt to the challenges of illness. 65 Particularly, Bandura’s concepts may enhance patient efficacy and provide reassurance during times of anxiety, uncertainty, and fear.
A sense of self-efficacy prompted by spiritual support and emotional caregiving may lead to fewer hospital admissions. Similarly, Antonovsky’s theory suggests that individuals can mobilize their resources to cope with stressors. The third component of his theory, meaningfulness, can be expressed through an individual’s spirituality and connection to a faith community. For many patients, meaningfulness and spirituality are driving forces in life. Spirituality and SI may serve as valuable resources when coping during crises. Thus, SI may be an effective tool for preventing readmissions, particularly those not related to physical emergencies, such as anxiousness related to pent up emotions that can be assisted by a chaplain to help calm patient’s breathing pattern.
Limitations
The small number of patients included in this pilot study may limit the statistical significance of the results. Furthermore, our study will enroll patients with a variety of diagnoses, which will make establishing conclusions and correlations between variables challenging. Because chaplains function as active interventionists in this study, meaningful differences in clinical style may exist even among board-certified chaplains; we will mitigate this by using a shared intervention framework (ACA model), a proposed telephone script, and fidelity tracking of the core components delivered. Additionally, patients must be willing to receive a chaplain visit, but the randomized process will help with eliminating self-selection. The intervention is designed to be inclusive of non-religious patients by focusing on meaning, values, relationships, and community supports, but differential uptake remains possible.
Finally, while the study is designed to test a chaplain-delivered intervention, it may be difficult to fully separate the effect of chaplain-specific spiritual care from the effect of follow-up attention itself. Despite these limitations, data collected during our pilot study will contribute to the growing body of knowledge on hospital readmissions and the importance and efficacy of spiritual care in this area. Chaplains track an outcome on every spiritual care visit, including patient comments, so this should capture which interventionist helped to make a difference. This siphoning out the data of who made the difference is hard to decipher but not impossible. Our study group plans to ask study participants what and who helped them the most. Other studies could address if a social worker, nurse, or other clinical professionals can do any different. In this case this study would emphasize the chaplain’s work in attempting to address hospital readmissions.
Supplemental Material
Supplemental Material - The Efficacy of Spiritual Care Intervention on Readmissions of Hospitalized Patients Receiving Palliative Care: A Quasi-Experimental Pilot Study Proposal
Supplemental material for The Efficacy of Spiritual Care Intervention on Readmissions of Hospitalized Patients Receiving Palliative Care: A Quasi-Experimental Pilot Study Proposal by Gary G. Creech, Rebecca L. Bieck, Betsy X. Bolint, Jennifer L. Derrick, April D. Lanz, Jacek T. Soroka, Sara H. Suleman in American Journal of Hospice and Palliative Medicine®
Footnotes
Acknowledgment
The Scientific Publications staff at Mayo Clinic provided copyediting, proofreading, administrative, and clerical support.
Ethical Considerations
IRB approval will be sought before beginning the study.
Consent to Participate
We will obtain patient consent during study recruitment.
Author Contributions
Conceptualization: GGC, RLB, BXB, JLD, ADL, JTS, SHS; Formal analysis: GGC, RLB, BXB, JLD, ADL, JTS, SHS; Methodology: GGC, RLB, BXB, JLD, ADL, JTS, SHS; Project administration: GGC, JTS; Supervision: ADL; Writing: GGC, JTS; Critical review: RLB.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing is not applicable to this article as no new data were created or analyzed in this study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.