
Abstract
Introduction
Dyspnea is a prevalent, debilitating, and distressing symptom in palliative care. This systematic review evaluated the efficacy of oxygen therapy and oxygen delivery modalities compared with room air, medical air (FiO2 21%), pharmacological therapy, or other respiratory support modalities for relieving dyspnea in patients with advanced, progressive, and incurable diseases.
Methods
A systematic search of PubMed and Scopus was conducted for studies published up to February 15, 2026, evaluating oxygen therapy or oxygen delivery modalities for dyspnea in palliative care. Risk of bias was assessed using the Cochrane RoB 2 tool and the Newcastle-Ottawa Scale. Data synthesis was performed narratively.
Results
Nine studies encompassing 879 participants were included. Among seven clinical trials, only one presented a low overall risk of bias. In non-hypoxemic patients, oxygen therapy was not consistently superior to medical air. In hypoxemic patients, limited evidence suggested benefit from conventional oxygen compared with room air, while high-flow nasal cannula was associated with greater short-term dyspnea relief than conventional oxygen therapy in one emergency department trial. Opioid therapy was associated with greater dyspnea reduction than oxygen alone in one prospective study.
Conclusion
Oxygen therapy should not be prescribed routinely for dyspnea in non-hypoxemic palliative care patients. Its use should be guided by baseline oxygenation status, delivery modality, expected symptomatic benefit, patient goals, and treatment burden. The certainty of evidence remains limited by small samples, heterogeneity, and risk of bias.
Keywords
Introduction
The American Thoracic Society defines dyspnea as both a physiological alteration and a subjective experience of respiratory discomfort. 1 This sensation transcends cardiac or pulmonary biology; it results from a multisystemic disorder involving neurohormonal changes and peripheral and respiratory muscle dysfunction.2,3 It is, therefore, an experience of global suffering where physical discomfort intersects with anxiety, fear, and psychological, social, and spiritual distress. 4 Its management requires a holistic perspective that prioritizes global comfort and human dignity.
Dyspnea severely impacts quality of life, psychosocial well-being, and socio-familial organization. 5 It remains one of the most prevalent, debilitating, and difficult-to-control symptoms in advanced or terminal diseases, often worsening in the final days of life.6,7 Severe dyspnea is reported in 65%, 70%, and 90% of severely ill patients with heart failure, lung cancer, and chronic obstructive pulmonary disease, respectively. 8 It is also a recognized poor prognostic factor in advanced cancer. 9
In Palliative Care (PC), dyspnea is frequently harder to control than oncological pain or nausea. 10 Often, the response is the administration of supplemental oxygen. Multiple studies demonstrate that prescribing oxygen for end-of-life patients is deeply ingrained in clinical practice and frequently viewed as a basic comfort measure.11,12 While patients and caregivers associate oxygen therapy with immediate relief, its true physiological and symptomatic benefit in patients without documented hypoxemia remains highly debated.13,14 Furthermore, this intervention carries non-negligible financial and logistical costs. In Canada, palliative oxygen therapy that did not meet hypoxemia criteria accounted for approximately 30% of oxygen therapy costs in 2000. 15
Current literature and international guidelines, such as those from the American Society of Clinical Oncology, do not support the routine use of supplemental oxygen in non-hypoxemic patients. 16 Instead, evidence favours optimizing baseline pharmacological therapy, namely through opioid titration, combined with targeted non-pharmacological interventions like facial airflow.16,17 High-flow nasal oxygen devices have also emerged, potentially alleviating dyspnea by reducing nasopharyngeal resistance and inspiratory effort.18,19
Although previous systematic reviews and meta-analyses have addressed this topic, clinically relevant uncertainties remain, particularly because available studies differ in baseline oxygenation status, oxygen delivery modality, comparator intervention, treatment duration, and dyspnea assessment tools.13,14,18,19 Therefore, an updated synthesis distinguishing hypoxemic from non-hypoxemic patients and conventional oxygen therapy from high-flow modalities is warranted.
Despite these recommendations, substantial gaps persist in clinical application. 7 Given the marked heterogeneity of populations, interventions, comparators, and outcome measures, it is essential to systematize the latest evidence. This systematic review aims to evaluate the efficacy of oxygen therapy in relieving dyspnea intensity in adult PC patients, considering baseline oxygenation status and type of oxygen delivery, to promote more rational and evidence-based prescribing.
Methods
This systematic review was conducted and reported in accordance with the PRISMA 2020 (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. 20 The study protocol was not previously registered.
Eligibility Criteria
Study selection was guided by the PICO (Population, Intervention, Comparison, Outcome) framework: • • • •
Included studies were randomized controlled trials (RCTs) and observational studies (prospective and retrospective cohorts) published in English or Portuguese. We excluded pediatric studies, acute reversible respiratory diseases (eg, acute asthma exacerbation or infection), animal models, narrative reviews, letters to the editor, and isolated case reports.
For eligibility assessment, “receiving palliative care” was defined broadly as care delivered to patients with advanced, progressive, incurable, or life-limiting disease in whom the primary therapeutic goal was symptom relief rather than disease modification. Studies were considered eligible when the population was explicitly described as receiving palliative, hospice, terminal, end-of-life, or supportive care, or when participants had advanced incurable disease and dyspnea was managed with a palliative intent.
Hypoxemia was defined according to each study’s criteria, most commonly as SpO2 <90% on room air or PaO2 ≤55 mmHg. When oxygenation thresholds differed or were not reported, this was recorded as a source of clinical heterogeneity and considered in the narrative synthesis.
Information Sources and Search Strategy
A systematic literature search was conducted in PubMed/MEDLINE and Scopus for articles published between January 1, 1989, and February 15, 2026, to capture relevant contemporary evidence. The search strategy combined controlled vocabulary, namely MeSH (Medical Subject Headings) terms in PubMed, and free-text words, adapting the syntax and Boolean operators to each database’s specificities. The final search equation used for PubMed was: (“oxygen therapy”[MeSH Terms] OR “oxygen”[All Fields]) AND (“dyspnea”[MeSH Terms] OR “breathlessness”[All Fields]) AND (“palliative care”[MeSH Terms] OR “end-of-life care”[All Fields] OR “terminal care”[All Fields]). The search equation for Scopus was: (TITLE (oxygen therapy OR oxygen) AND TITLE-ABS-KEY (dyspnea OR breathlessness) AND TITLE-ABS-KEY (palliative care OR end-of-life care OR terminal care)).
Selection Process and Data Extraction
Study selection occurred in sequential phases. Initially, results from database searches were exported, and duplicates were removed. An initial screening was performed through independent reading of titles and abstracts, excluding studies that did not meet the PICO eligibility criteria. In the second stage, potentially relevant articles underwent full-text review for final inclusion, with documented reasons for exclusion. The initial screening was conducted by one reviewer, and final inclusion decisions were collaboratively validated with a second reviewer. Data extraction was performed by the primary investigator into a standardized spreadsheet (Microsoft Excel), and all data matrices were subsequently validated by the remaining authors. Extracted data included: study identification (first author and publication year), study design, sample size, primary diagnosis, baseline oxygenation/oximetry, intervention and control group details, outcome measurement scales, and reported efficacy.
Risk of Bias Assessment
Methodological quality and risk of bias were initially assessed by the primary investigator, with results and clinical justifications independently reviewed and validated by the second investigator. RCTs were evaluated using the Cochrane Risk of Bias 2 (RoB 2) tool. 21 The analysis focused on five fundamental domains: randomization process, deviations from intended interventions (including carryover effect assessment in crossover designs), missing outcome data, outcome measurement, and selection of the reported result. The overall risk of bias for each trial was categorized as “low risk,” “some concerns,” or “high risk.” Observational cohort studies were assessed using the Newcastle-Ottawa Scale (NOS). 22 Methodological quality was quantified through a scoring system focusing on three main domains: cohort selection, comparability, and outcome assessment. The maximum possible score was 9, with studies scoring ≥7 considered as having high methodological quality (low risk of bias).
Synthesis Methods
For the primary outcome, efficacy was defined as a reduction in dyspnea intensity measured with validated instruments, including the Numerical Rating Scale (NRS), Modified Borg Scale (MBS), visual analogue scale (VAS), Respiratory Distress Observation Scale (RDOS), or Symptom Assessment Scale (SAS), according to the measure used in each study. When available, changes from baseline, between-group differences, confidence intervals, P values, patient preference, and clinically relevant response thresholds were extracted. Due to the marked clinical and methodological heterogeneity identified among the studies, evident in the diversity of validated instruments used for dyspnea measurement, the variability of oxygen therapy protocols, and the distinct methodological designs, statistical aggregation via meta-analysis was not considered appropriate. Consequently, a narrative and tabulated synthesis of the results was performed. Data were thematically structured, evaluating the symptomatic efficacy of interventions primarily based on the sample’s baseline oxygenation status (hypoxemic vs non-hypoxemic patients). Differences in oxygen dose or flow rate, delivery device, intervention duration, timing of outcome assessment, and comparator intervention were considered key sources of clinical heterogeneity and were therefore described narratively.
Certainty of Evidence
The overall certainty of evidence for the primary outcome was evaluated using the GRADE (Grading of Recommendations Assessment, Development and Evaluation) approach. 23 Evidence quality was classified into one of four levels: high, moderate, low, or very low. It was downgraded in cases identifying serious methodological limitations, outcome inconsistency, indirect evidence, statistical imprecision, or suspected publication bias.
Results
Study Selection
The initial database search identified 299 potentially relevant records (217 in PubMed, 82 in Scopus). After removing 41 duplicates and excluding 205 articles by title, 53 abstracts were screened; 43 were excluded for not meeting the predefined eligibility criteria. Ten articles underwent full-text evaluation. One was excluded due to incompatible outcomes. The final sample of this systematic review included 9 original studies (Figure 1). PRISMA flowchart detailing the identification, eligibility, and inclusion phases of articles obtained through searches in electronic databases.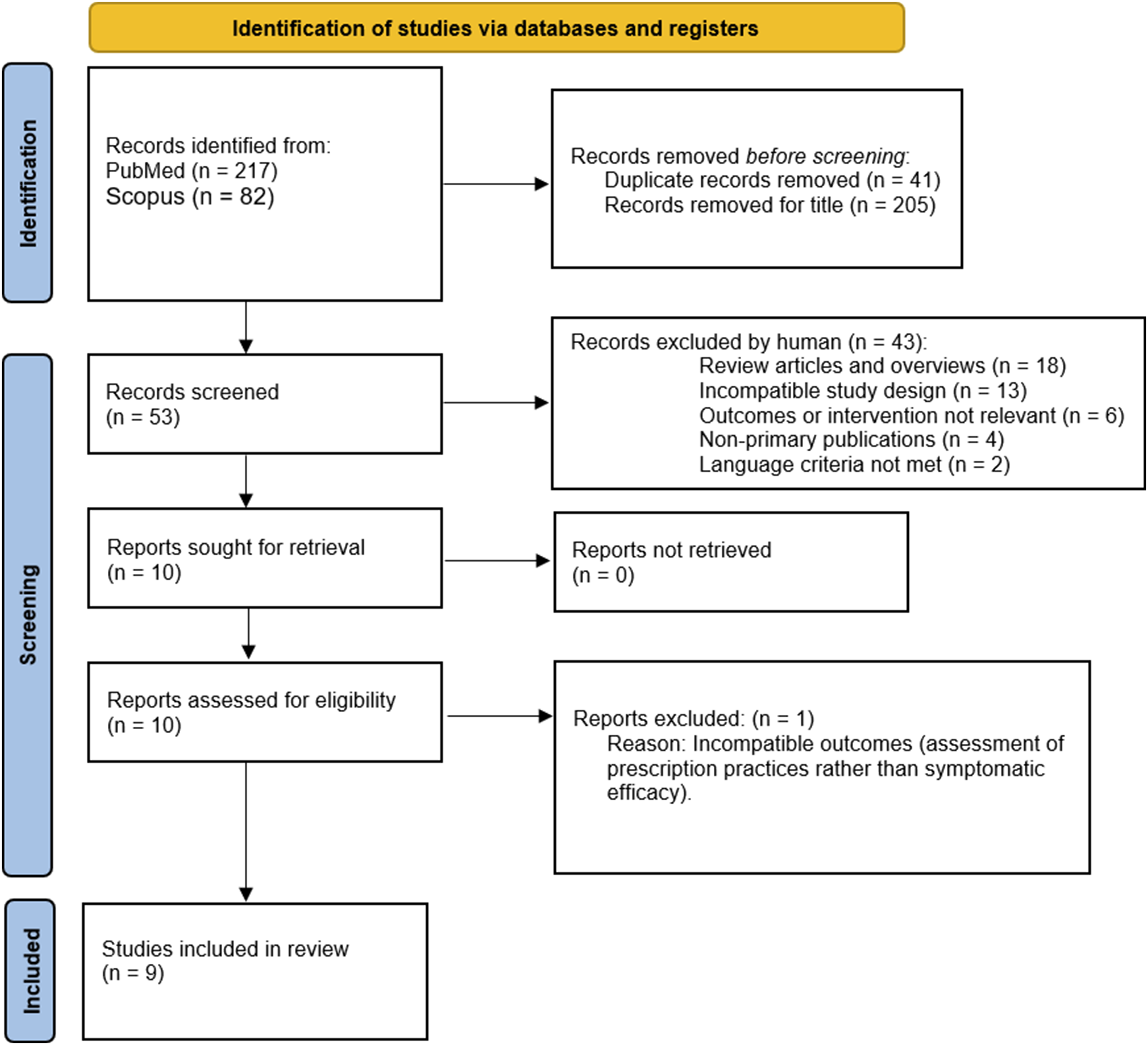
Characteristics of Included Studies
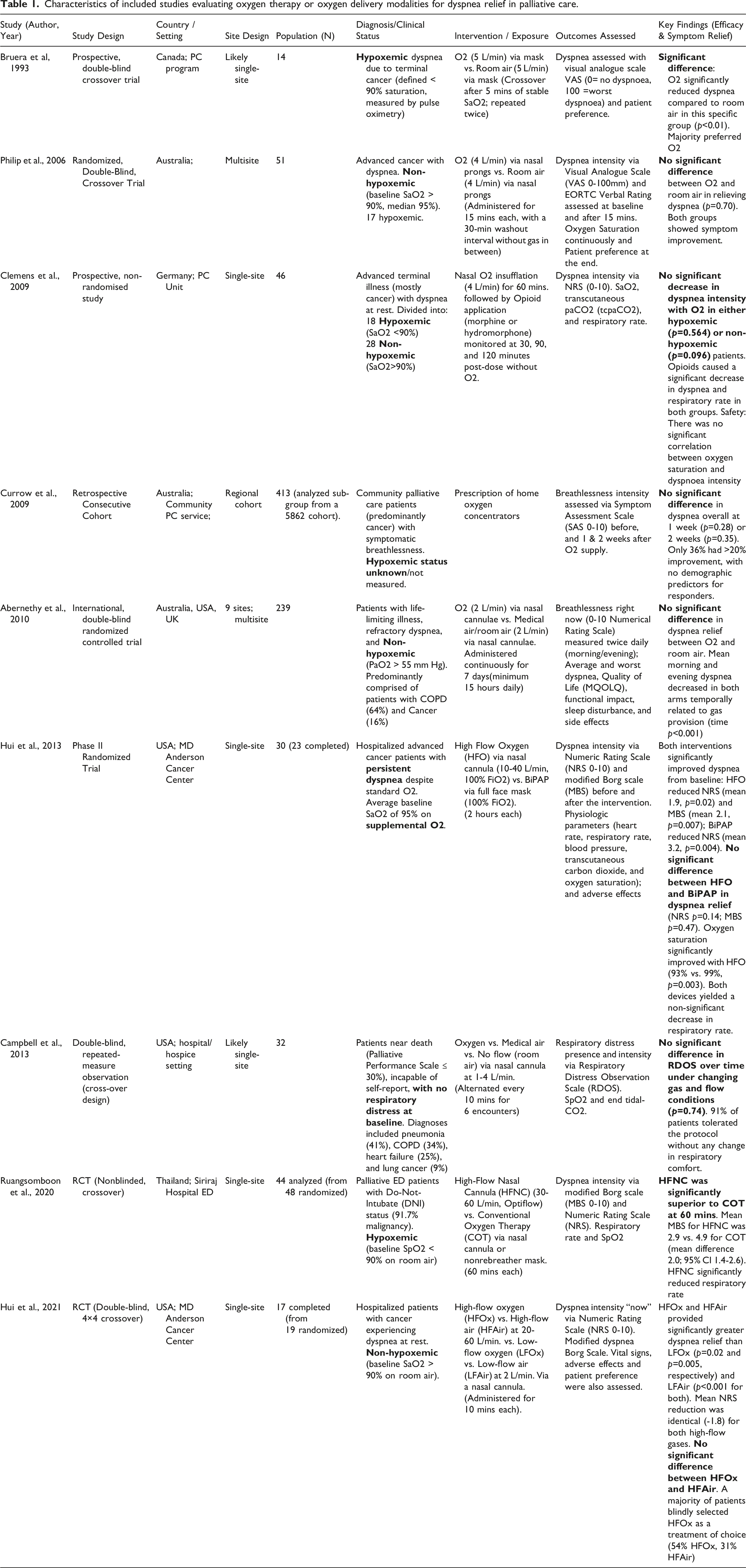
Characteristics of included studies evaluating oxygen therapy or oxygen delivery modalities for dyspnea relief in palliative care.
Oxygen Therapy for Dyspnea
Analysis of the included studies suggests that the symptomatic effect of oxygen therapy varied according to baseline oxygenation status, oxygen delivery modality, flow rate, and comparator intervention. Given the heterogeneity of study designs and small sample sizes in several trials, findings are summarized narratively by clinical subgroup and type of comparison. • • • • • • •
Methodological Quality and Risk of Bias Assessment
The primary source of bias, consistent across most trials, was concentrated in Domain 2 (deviations from intended interventions) and Domain 4 (measurement of the outcome). (Figure 2). Considering that dyspnea is a subjective, patient-reported symptom, the practical impossibility of completely blinding the physical and tactile characteristics of respiratory devices, such as the impact of airflow on the nasal mucosa, introduced an inevitable risk of expectation bias in clinical practice. In this context, the trial by Abernethy et al
24
stood out as the only one classified with a low overall risk of bias, serving as the methodological standard for ensuring a robust double-blind design by concealing air and oxygen concentrators in identical boxes in the home setting. Three trials were classified as having “some concerns.”25,30,31 Three studies presented a high overall risk.27-29 This high risk was primarily driven by the inherently open-label design in scenarios where blinding the flow rate in HFNO or non-invasive ventilation was unfeasible, or, in the case of Bruera et al,
28
by the absence of a washout period between interventions, generating a physiological carryover effect. The methodological quality of the two observational cohort studies26,32 was assessed using the Newcastle-Ottawa Scale (Table 2). Both studies demonstrated high overall methodological quality, achieving a score of 7 out of 9. The main limitations identified were the lack of rigorous control for secondary confounding variables in the comparability domain and the reliance on self-assessment scales without any form of blinding. Risk-of-bias assessment of the included randomized clinical trials using the Cochrane RoB 2 tool. The domains assessed were bias arising from the randomization process (D1), bias due to deviations from intended interventions (D2), bias due to missing outcome data (D3), bias in measurement of the outcome (D4), and bias in selection of the reported result (D5). The color classification reflects low risk, some concerns, and high risk for each domain and for the overall risk-of-bias judgment. Methodological quality assessment of the included observational studies using the Newcastle-Ottawa Scale.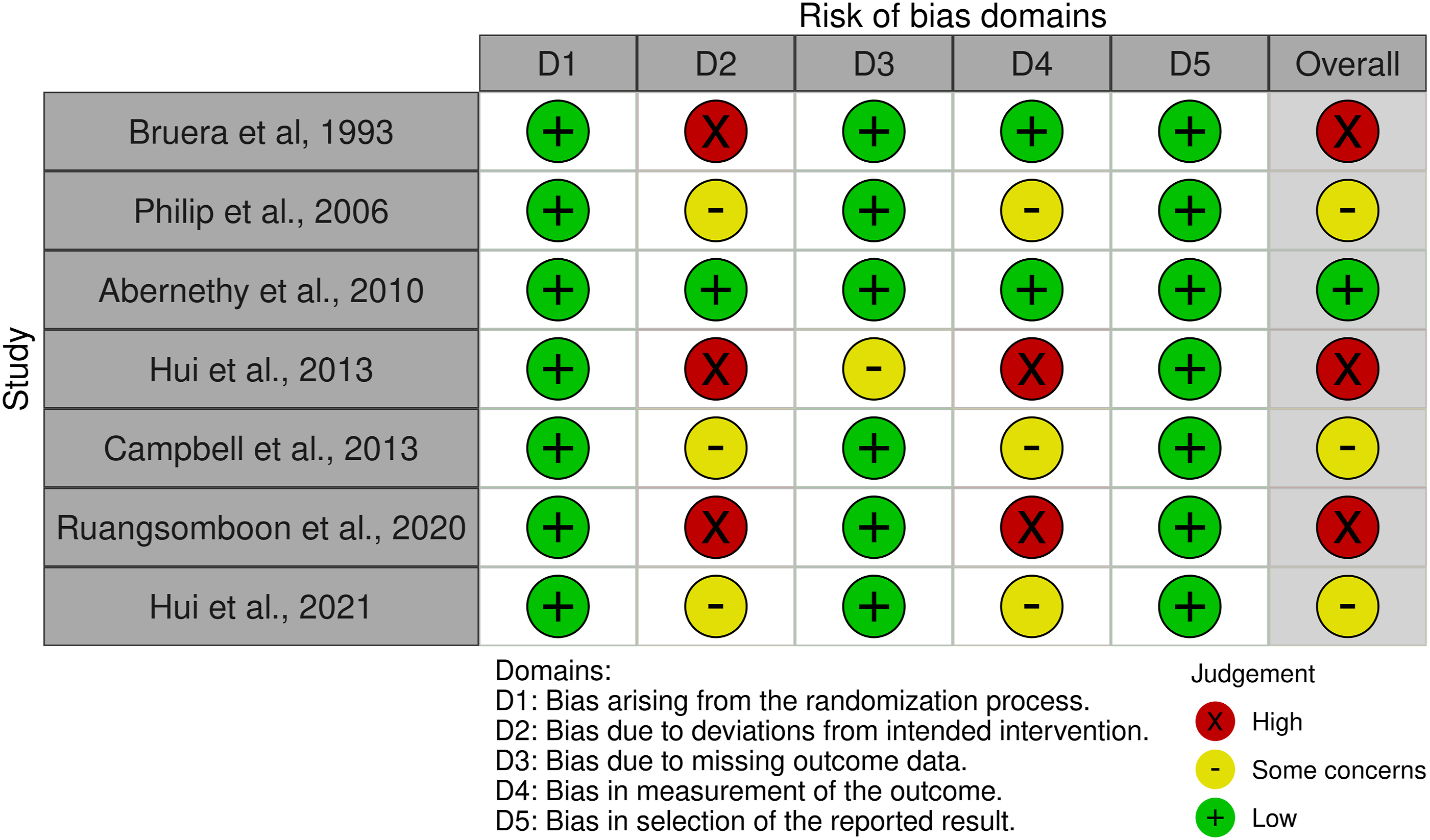

Certainty of Evidence (GRADE Approach)
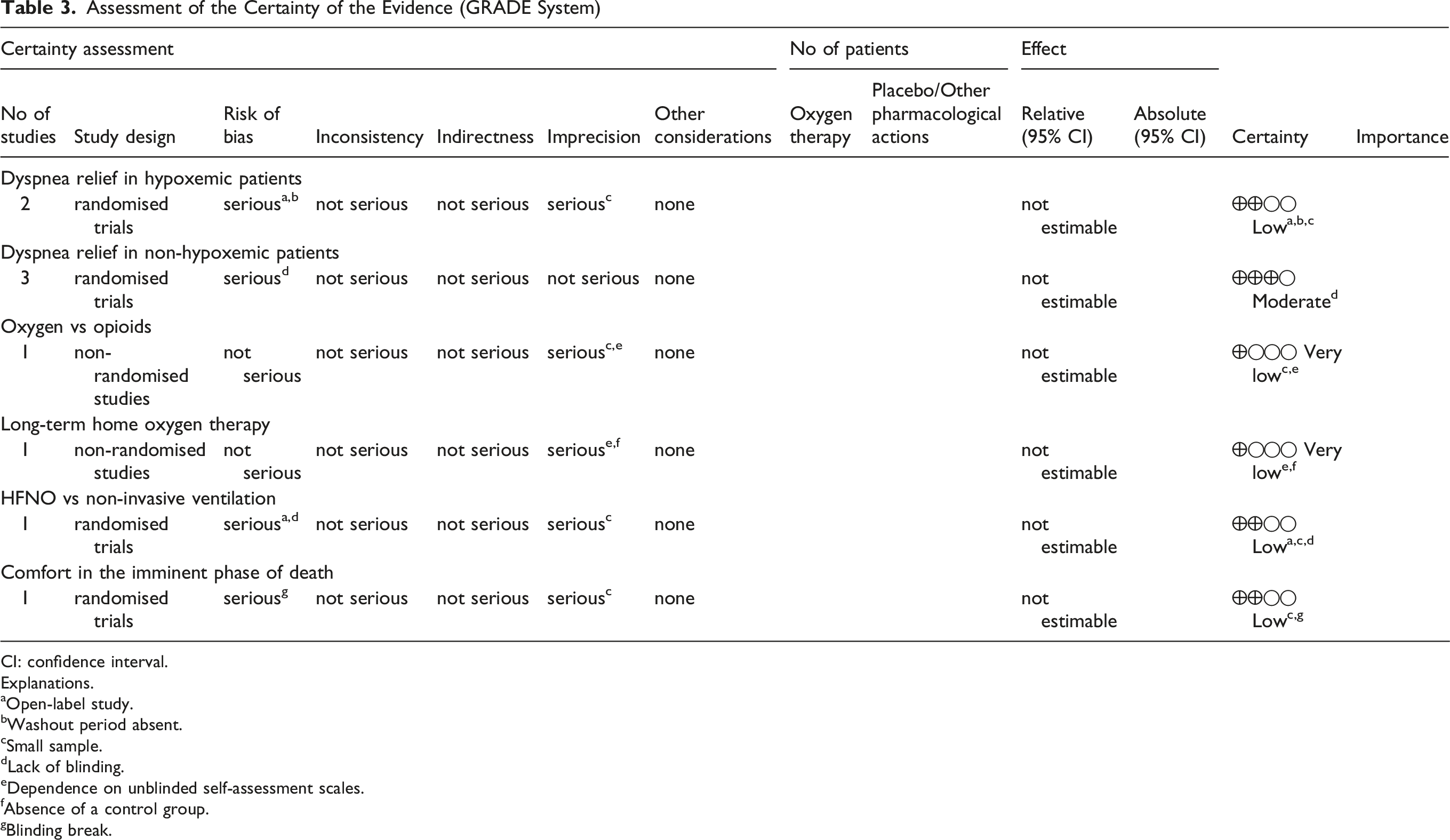
(Table 3) and stratified according to the main clinical subgroups and comparisons: • • • • • • • Assessment of the Certainty of the Evidence (GRADE System) CI: confidence interval. Explanations. aOpen-label study. bWashout period absent. cSmall sample. dLack of blinding. eDependence on unblinded self-assessment scales. fAbsence of a control group. gBlinding break.
Discussion
The primary objective of this systematic review was to evaluate the efficacy of oxygen therapy for relieving dyspnea in patients with advanced, progressive, and incurable diseases. Current evidence reveals that the clinical utility of supplemental oxygen is dichotomous and dependent on the patient’s baseline oxygenation status. While hypoxemic individuals benefit significantly from oxygen therapy,27,28 routine prescription for non-hypoxemic patients remains ineffective for sustained symptom reduction.16,24,30 Despite the robustness of this methodological evidence, a substantial gap persists between science and daily clinical practice. A large percentage of physicians continue to prescribe oxygen to terminal patients without hypoxemia, highlighting the urgent need to demystify its role in end-of-life care. 33
In trials focusing on non-hypoxemic populations, the similar effects observed with oxygen and medical air suggest that dyspnea relief may not depend exclusively on correction of an oxygen deficit. Airflow-related mechanisms, including thermomechanical stimulation of trigeminal receptors and patient expectation, may partly explain symptom improvement when gas is delivered through nasal cannulae. 31 However, in studies using high-flow nasal cannula, additional mechanisms may also contribute, including nasopharyngeal dead-space washout, low-level positive airway pressure, reduced inspiratory resistance, and decreased respiratory effort.18,19 Therefore, the symptomatic benefit observed with high-flow modalities should not be attributed solely to placebo or trigeminal stimulation. Recent evidence on handheld fan therapy further supports the clinical relevance of simple airflow-based interventions, although these should be interpreted as potentially useful adjuncts rather than direct substitutes for all forms of respiratory support. 34
In the spectrum of refractory dyspnea, pharmacological optimization with opioids should play a central role.16,32 However, medical decisions to prescribe or withhold oxygen therapy often face psychosocial and cultural barriers, particularly the fear, shared by families and healthcare professionals, that removing oxygen might precipitate the patient’s death. The cohort study by Igarashi et al 35 attempts to deconstruct this myth. By demonstrating that home oxygen use is not associated with any significant increase in overall survival for non-hypoxemic patients with advanced cancer, the literature does not support the use of oxygen solely with the expectation of prolonging survival in non-hypoxemic patients with advanced cancer, and highlights the need to align oxygen prescription with individualized goals of care.
This lack of long-term clinical benefit 26 is even more pronounced in the imminent phase of death. Discontinuing oxygen therapy during this period does not appear to cause symptomatic worsening. 25 In this phase, masks and nasal cannula often cease to be supportive devices and become physical and emotional barriers between the patient and their family. 13 Current evidence supports the safe removal of this equipment,7,11 promoting a reduction in unnecessary medicalization and prioritizing human touch, non-verbal communication, and dignity, essential elements of the grieving process.
Despite the clinical relevance of these findings, this systematic review has limitations. The search was restricted to PubMed/MEDLINE and Scopus and did not include grey literature or additional databases, so relevant studies may have been missed. The included studies were also heterogeneous in baseline oxygenation status, oxygen flow rates, delivery devices, exposure duration, timing of dyspnea assessment, comparator interventions, and outcome instruments. These differences limited the feasibility of meta-analysis and required a narrative synthesis. Finally, the certainty of evidence was limited by small sample sizes, risk of bias, and the practical difficulty of blinding airflow-based interventions in PC research.
In summary, the results of this review demand a critical reassessment of daily medical practice. Oxygen therapy should not be viewed as a universal treatment for dyspnea in PC. Its prescription must be guided by objective criteria rather than an empirical instinct to treat the sensation of breathlessness. For non-hypoxemic patients, evidence favours a timely transition to non-pharmacological approaches, such as the facial fan, combined with early optimization of systemic opioids (fixed or as needed). Future research should focus on multi-centre clinical trials directly comparing thermomechanical interventions and pharmacological therapy with larger samples. Ultimately, when oxygen provides no measurable symptomatic benefit, its discontinuation should not be interpreted as therapeutic abandonment, but as part of individualized, goal-concordant care focused on comfort, proximity, and dignity at the end of life.
To translate these findings into clinical practice, we propose a simplified algorithm for the palliative management of dyspnea (Figure 3). This algorithm emphasizes baseline oxygenation status, reassessment of symptomatic benefit, monitoring for adverse effects and signs of respiratory distress, and alignment with goals of care. For non-hypoxemic patients, or when oxygen provides no measurable benefit, pharmacological and nonpharmacological strategies should be prioritized. Proposed clinical algorithm for the palliative management of dyspnea according to baseline oxygenation status and symptomatic response. The algorithm emphasizes that supplemental oxygen therapy should be considered primarily in patients with documented hypoxemia and should be reassessed according to symptomatic improvement, side effects, actively dying phase, and observable signs of respiratory distress. In non-hypoxemic patients, or when oxygen provides no symptomatic benefit, pharmacological and nonpharmacological measures such as opioids and handheld fan therapy should be prioritized as part of individualized, goal-concordant care.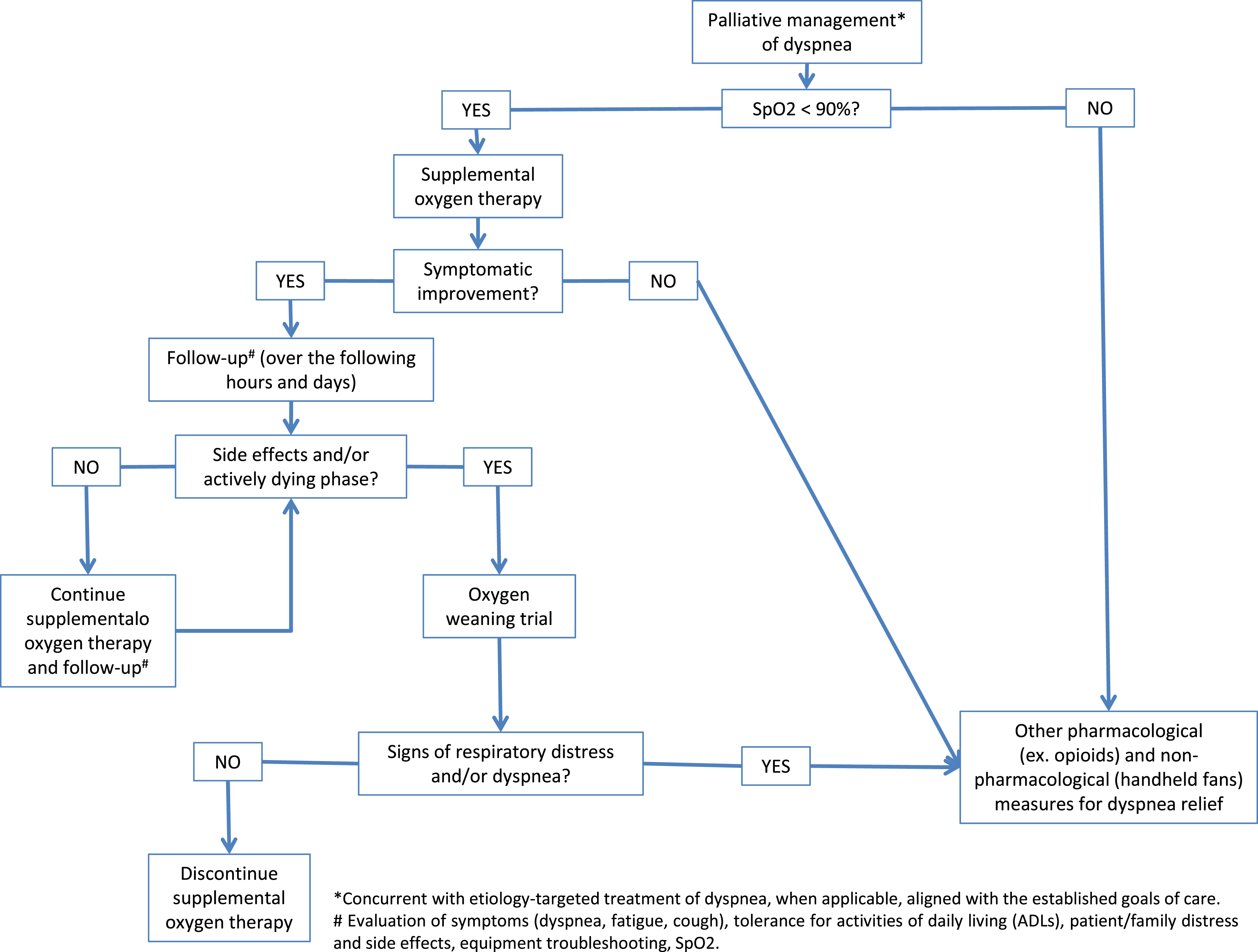
Conclusion
This review suggests that the symptomatic benefit of oxygen therapy in patients with advanced disease depends largely on baseline oxygenation status, delivery modality, and comparator intervention. In non-hypoxemic patients, supplemental oxygen does not appear to provide additional dyspnea relief compared with medical air when delivered under comparable flow conditions. In hypoxemic patients, limited evidence supports the benefit of conventional oxygen therapy compared with room air, while high-flow nasal cannula may provide greater short-term relief than conventional oxygen therapy in selected emergency palliative care settings.
Overall, oxygen therapy in PC should be guided by objective assessment of oxygenation status, expected symptomatic benefit, patient goals, and treatment burden. For non-hypoxemic patients, pharmacological optimization and non-pharmacological airflow-based interventions should be considered as part of individualized, comfort-focused care.
Footnotes
Acknowledgments
During the preparation of this work, the author used the Gemini (Google) language model for grammatical review and to improve text fluency. After using this tool, the author reviewed, edited, and assumes full responsibility for all final content of the manuscript.
Ethical Considerations
Not applicable. As this is a systematic review, no human or animal research was conducted.
Author Contributions
B.S. – conceptualization, literature search, data extraction, and writing of the original manuscript. T.T. – conceptualization, study design, data analysis and interpretation, supervision, critical review, and text editing. C.R. – supervision, critical review, and text editing. All authors approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data used in this systematic review were extracted from previously published studies. The data extraction matrix and risk-of-bias assessments are available from the corresponding author upon reasonable request.