
Abstract
Background:
The association between hypothyroidism and mortality remains inconsistent across studies. We evaluated the associations of overt and subclinical hypothyroidism with all-cause and cardiovascular mortality in a large Chinese cohort.
Methods:
This retrospective cohort study included 70,276 adults aged 25 to 84 years who underwent routine health examinations at a large medical center in northern China between January 1, 2017, and December 31, 2022. Thyroid function was categorized as euthyroidism, overt hypothyroidism, or subclinical hypothyroidism. Mortality data were obtained through linkage with national death registries. Cause-specific Cox proportional hazards models were used to estimate hazard ratios (HRs) for all-cause and cardiovascular mortality. Subgroup analyses were conducted by age and diabetes status.
Results:
Among 70,276 participants, 853 (1.2%) had overt hypothyroidism, and 2436 (3.5%) had subclinical hypothyroidism. During a median follow-up of 5.1 years (interquartile range, 3.6–6.0), 359 deaths occurred. Compared with individuals with euthyroidism, overt hypothyroidism was associated with increased all-cause (HR, 2.01; confidence interval [CI], 1.17–3.45) and cardiovascular mortality (HR, 2.70; CI, 1.18–6.19). Among individuals with diabetes, overt hypothyroidism showed a stronger association with all-cause mortality (HR, 5.45; CI, 2.46–12.07) than among those without diabetes (HR, 1.19; CI, 0.56–2.54) (p for interaction = 0.045). Subclinical hypothyroidism was associated with increased all-cause mortality among participants younger than 50 years (HR, 3.28; CI, 1.31–8.23), including those with thyrotropin (TSH) levels <10 mIU/L (HR, 3.36; CI, 1.34–8.43), but not among those aged 50 to 69 years (HR, 0.32; CI, 0.08–1.31) or 70 years or older (HR, 1.00; CI, 0.51–1.98) (p for interaction = 0.022).
Conclusions:
Overt hypothyroidism was associated with increased mortality, particularly in individuals with diabetes. Subclinical hypothyroidism was associated with increased mortality risk only in younger adults, even at modest TSH elevations.
Background
Hypothyroidism is a common disorder among Chinese adults. The national survey data from 2017 reported prevalence rates of 1.02% for overt hypothyroidism and 12.93% for subclinical hypothyroidism in China.1,2 Subclinical hypothyroidism was more prevalent among older adults, with rates exceeding 16.0% among those aged 60 years or older. 1 Understanding the association between hypothyroidism and mortality, particularly whether this association differs by age, is essential to inform prevention and treatment strategies.
Previous studies have examined the associations between subclinical hypothyroidism and mortality, but the findings remain inconsistent.3–6 A meta-analysis of 55 cohort studies found that subclinical hypothyroidism was associated with increased risks of all-cause and cardiovascular disease (CVD) mortality. 6 However, such an association was not observed in a large individual participant data meta-analysis that included >55,000 participants. 4 Several studies have suggested that the association between subclinical hypothyroidism and mortality may vary by age.7–9 A meta-analysis study reported that subclinical hypothyroidism was associated with the increased risk of mortality in younger (<65 years) populations, but not in older (≥65 years) individuals. 8 Another study found similar results using a 60-year age threshold. 9 Given these inconsistent findings, additional data from diverse populations are needed. Few studies have evaluated these associations in Chinese populations, 5 and age-stratified data remain limited. Furthermore, hypothyroidism and diabetes mellitus frequently co-occur,10,11 but whether diabetes modifies the association between hypothyroidism and mortality has not been well-established.
Therefore, using data from a large retrospective cohort in northern China, we aimed to examine the associations of overt and subclinical hypothyroidism with all-cause and CVD mortality. A secondary aim was to assess whether these associations differed by age group and diabetes status. The findings may provide insights into tailoring prevention and treatment strategies for hypothyroidism.
Methods
Study design and participants
Routine general health examinations are widely implemented in China and are a part of the government’s policy on health literacy. In 2021, approximately 549 million health examinations were performed nationwide, with most participants being employed adults, as many employers provide health checks as employee benefits. 12 In this retrospective cohort study, we identified 116,267 adults aged 25 to 84 years who underwent routine health examinations at China-Japan Friendship Hospital, a tertiary care medical center in Beijing, China, between January 1, 2017, and December 31, 2022. More than 90% of participants were current or retired employees from enterprises, government agencies, or public institutions in Beijing. Participants were followed up from baseline until death or censoring on December 31, 2024, whichever occurred first. Of 116,267 adults identified, 42,051 were excluded for missing thyrotropin (TSH), free triiodothyronine (fT3), or free thyroxine (fT4) measurements. Among 74,216 adults with complete thyroid function testing, 502 with a history of thyroid disease or thyroid medication use and 487 lost to follow-up were excluded. To focus on hypothyroidism, we further excluded 1772 participants with TSH below the reference range (<0.6 mIU/L) and 1179 participants with normal TSH but fT3 below the reference range (<4 pmol/L). The final analysis included 70,276 participants (Supplementary Fig. S1).
The Human Research Ethics Committee of China-Japan Friendship Hospital approved this study and waived the requirement for informed consent given its observational design and the use of fully de-identified data (Approval No. 2025-KY-014-1). The study was conducted in accordance with the Declaration of Helsinki.
Procedures and measures
Routine general health checkups are offered as comprehensive health packages that include routine screenings for multiple diseases during a single visit. 12 Demographic characteristics, medical history, and medication use were recorded during the health checkup. Serum TSH, fT3, and fT4 concentrations were measured once at baseline for each participant using a chemiluminescence analyzer (DXI800; Beckman Coulter, Brea, CA, USA). Systolic and diastolic blood pressure (SBP and DBP, respectively), height, and weight were measured following standardized protocols. Fasting blood glucose (FBG), hemoglobin A1c (HbA1c), total cholesterol (TC), triglycerides (TG), high-density lipoprotein cholesterol (HDL-C), and low-density lipoprotein cholesterol (LDL-C) were measured using standardized laboratory procedures and equipment. More detailed materials and methods of data collection are described in Supplementary Data S1.
Thyroid function status was classified according to the most recent Chinese standard reference ranges for thyroid hormones issued by the National Health Commission of the People's Republic of China (WS/T 404.10—2022): 0.60–4.90 mIU/L for TSH, 8.50–14.50 pmol/L for fT4, and 4.00–6.10 pmol/L for fT3. These reference ranges were established based on a large multicenter study of the Chinese adult population. 13 Euthyroidism was defined as a serum TSH concentration within the reference range.4,5 Overt hypothyroidism was defined as a serum TSH concentration of >4.90 mIU/L with an fT4 concentration of <8.50 pmol/L. Subclinical hypothyroidism was defined as a serum TSH concentration of >4.90 mIU/L with fT4 within the reference range. 14
Body mass index (BMI) was categorized according to the following Chinese BMI cutoffs: underweight (<18.5), normal (18.5–23.9), overweight (24.0–27.9), and obese (≥28.0). 15 Hypertension was defined as SBP ≥ 140 mm Hg, DBP ≥ 90 mm Hg, a self-reported diagnosis of hypertension, or the use of antihypertensive medication. Dyslipidemia was defined as TC ≥ 6.22 mmol/L, TG ≥ 2.26 mmol/L, HDL-C < 1.04 mmol/L, LDL-C ≥ 4.14 mmol/L, or the use of lipid-lowering medications.16,17 Diabetes was defined as FBG ≥ 7.0 mmol/L, HbA1c ≥ 6.5%, a self-reported diagnosis of diabetes, or the use of antidiabetic medication.
Follow-up and outcome assessment
In this study, participants’ vital status and causes of death were collected through passive follow-up by linking the cohort data with the national death registries, which cover the 31 mainland provinces of China. 18 The death records in this system are reported by health care institutions almost in real time, and they are subsequently validated against local residential records and health insurance records on an annual basis. 18 CVD death was defined based on International Classification of Diseases, 10th Revision (ICD-10) (codes I00–I99). 19
Statistical analysis
The baseline characteristics of the study population were summarized overall and by thyroid function status. Continuous variables were presented as means with standard deviations (SDs), and categorical variables were presented as counts with corresponding percentages. Differences across different thyroid function groups were assessed using the Pearson χ2 test for categorical variables and analysis of variance for continuous variables.
Cumulative incidence functions were used to visualize the cumulative incidence of all-cause and CVD mortality from baseline to the end of follow-up across thyroid function status groups. The cumulative incidence of CVD death was estimated using the Fine and Gray method, treating non-CVD deaths as competing events. 20 All-cause mortality was compared across thyroid function groups using the log-rank test, and CVD mortality was compared using Gray’s test. The number of deaths and the rates per 1000 person-years at risk of all-cause and CVD mortality were summarized by thyroid function status. Person-years were calculated from baseline to the date of death or censoring at the end of follow-up, whichever occurred first. Age-standardized mortality rates per 1000 person-years by thyroid function status were computed using the age distribution of the entire cohort as the reference population. Age standardization was performed using the direct standardization method, stratified by 5-year age groups (25–29, 30–34, 35–39, 40–44, 45–49, 50–54, 55–59, 60–64, 65–69, 70–74, 75–79, and 80–84 years).
Cox proportional hazards regression models were used to examine the associations between thyroid function status and all-cause mortality. Cause-specific Cox models were used to assess CVD mortality, treating non-CVD death as competing events. 20 We constructed two models. Model 1 adjusted for age and sex. Model 2 further adjusted for BMI, hypertension, diabetes mellitus, and dyslipidemia on the basis of previous knowledge.5,21 Missing covariate data were addressed using multiple imputation with chained equations. 22 Estimates from each dataset were combined using Rubin’s rules to account for variability across imputations. Details of the imputation procedure, including the variables included in the imputation models and the proportion of missing data for each covariate, are provided in the Supplementary Data S2.
Prior guidelines have used the age of 65 or 70 years as thresholds to recommend for or against the treatment of subclinical hypothyroidism. 23 Studies in Chinese populations have reported significant differences in TSH distributions between individuals younger than 50 years and those aged 50 years or older.24,25 Based on these findings and the available sample sizes for subgroup analyses, we performed stratified analyses by three age groups (<50, 50–69, and ≥70 years) and by diabetes status. Interaction terms between thyroid function status and the age group or diabetes status were included in the models as product terms to evaluate effect modification. We tested for interactions using the likelihood ratio test, which involved comparing models with and without interaction terms. 26 Stratified analyses were limited to all-cause mortality because of the small number of CVD deaths within subgroups. We examined the proportional hazards assumption using the Schoenfeld residual test and the interaction terms between time and covariates.
To verify the robustness of our results, we conducted two sensitivity analyses. First, we repeated Cox proportional hazards analyses using complete case data, excluding participants with missing covariate values. Second, we investigated the potential for reverse causation by excluding participants who died from CVD within the first one or two years of follow-up. We conducted all analyses using R software (version 4.2.3). A two-sided p value of <0.05 was considered statistically significant.
Results
Baseline characteristics
The baseline characteristics of the study population overall and by thyroid function status are shown in Table 1. The mean (SD) age was 42.1 (12.2) years, and 37,017 (52.7%) participants were men. Of 70,276 participants, 66,987 (95.3%) had euthyroidism, 853 (1.2%) had overt hypothyroidism, and 2436 (3.5%) had subclinical hypothyroidism. Compared with participants with euthyroidism, those with overt or subclinical hypothyroidism were older, more likely to be female, and had a higher prevalence of hypertension, diabetes mellitus, and dyslipidemia (all p < 0.001).
Demographic and Clinical Characteristics of the Study Population Overall and by Thyroid Function Status
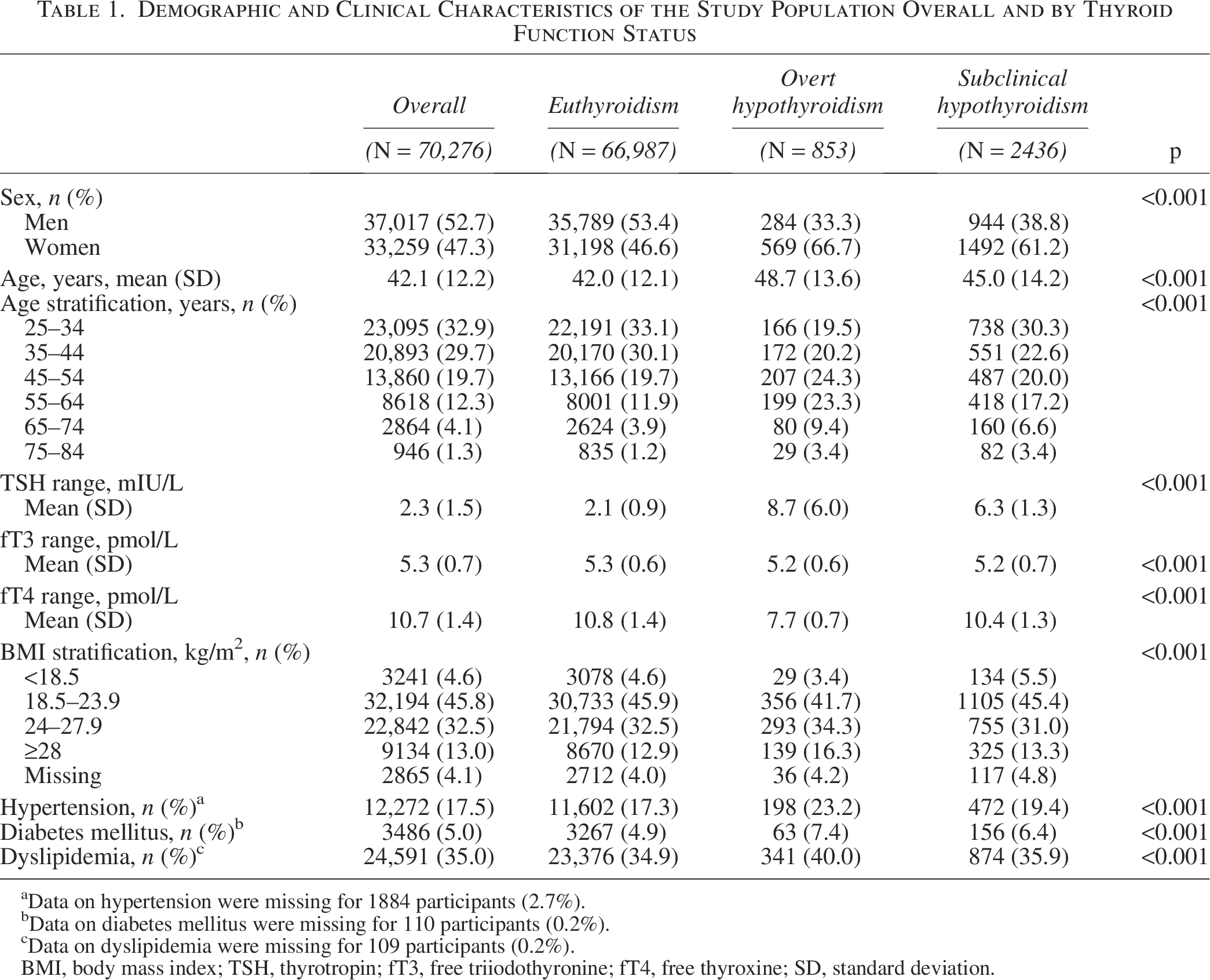
Data on hypertension were missing for 1884 participants (2.7%).
Data on diabetes mellitus were missing for 110 participants (0.2%).
Data on dyslipidemia were missing for 109 participants (0.2%).
BMI, body mass index; TSH, thyrotropin; fT3, free triiodothyronine; fT4, free thyroxine; SD, standard deviation.
All-cause and CVD mortality rates by thyroid function status
During the median follow-up of 5.1 years (interquartile range, 3.6–6.0 years), a total of 359 deaths (0.5%) occurred, including 115 (0.2%) due to CVD. Participants with overt hypothyroidism had significantly higher cumulative all-cause mortality (log-rank p < 0.001) and CVD mortality (Gray’s test p < 0.001) compared with those with euthyroidism (Fig. 1). The age-standardized all-cause mortality rates were 2.1 and 1.0 per 1000 person-years for the overt hypothyroidism and euthyroid groups, respectively. The corresponding age-standardized CVD mortality rates were 0.6 and 0.3 per 1000 person-years, respectively (Table 2).
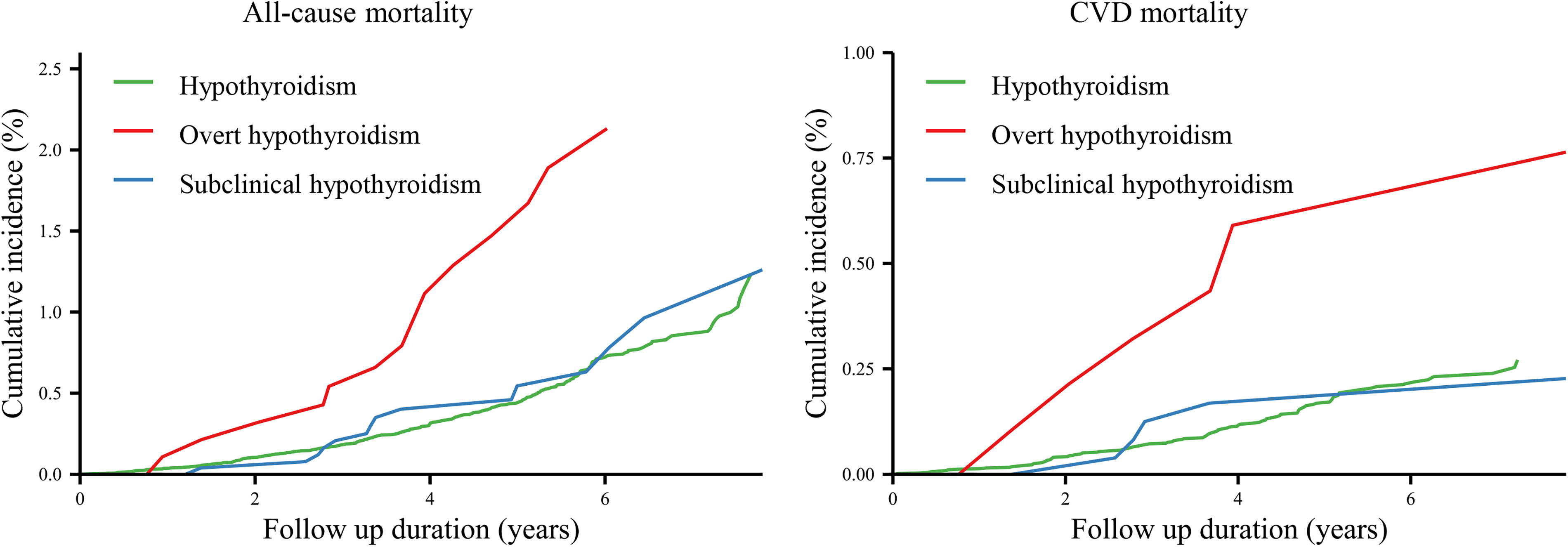
Cumulative incidence of all-cause and CVD mortality according to thyroid function status. CVD, cardiovascular disease.
All-Cause And CVD Mortality during Follow-up Overall and by Thyroid Function Status
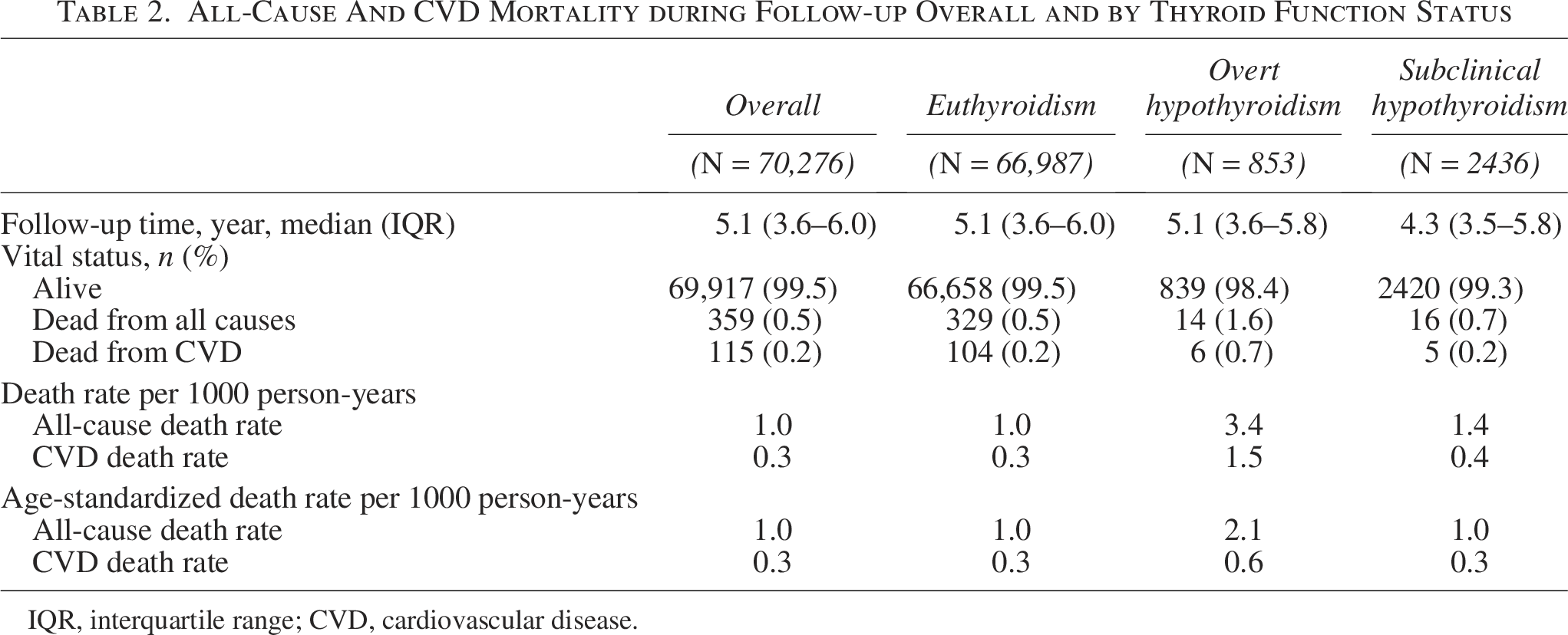
IQR, interquartile range; CVD, cardiovascular disease.
All-cause and CVD mortality risks by thyroid function status
After adjustment for age, sex, and metabolic factors, overt hypothyroidism was associated with a significantly higher risk of all-cause mortality (hazard ratio [HR], 2.01; confidence interval [CI], 1.17–3.45) and CVD mortality (HR, 2.70; CI, 1.18–6.19) compared with euthyroidism. There was no statistically significant association between subclinical hypothyroidism and all-cause mortality (HR, 0.94; CI, 0.57–1.56) or CVD mortality (HR, 0.93; CI, 0.38–2.30) (Table 3).
Hazard Ratios for All-Cause and CVD Mortality Associated with Overt and Subclinical Hypothyroidism Compared with Euthyroidism
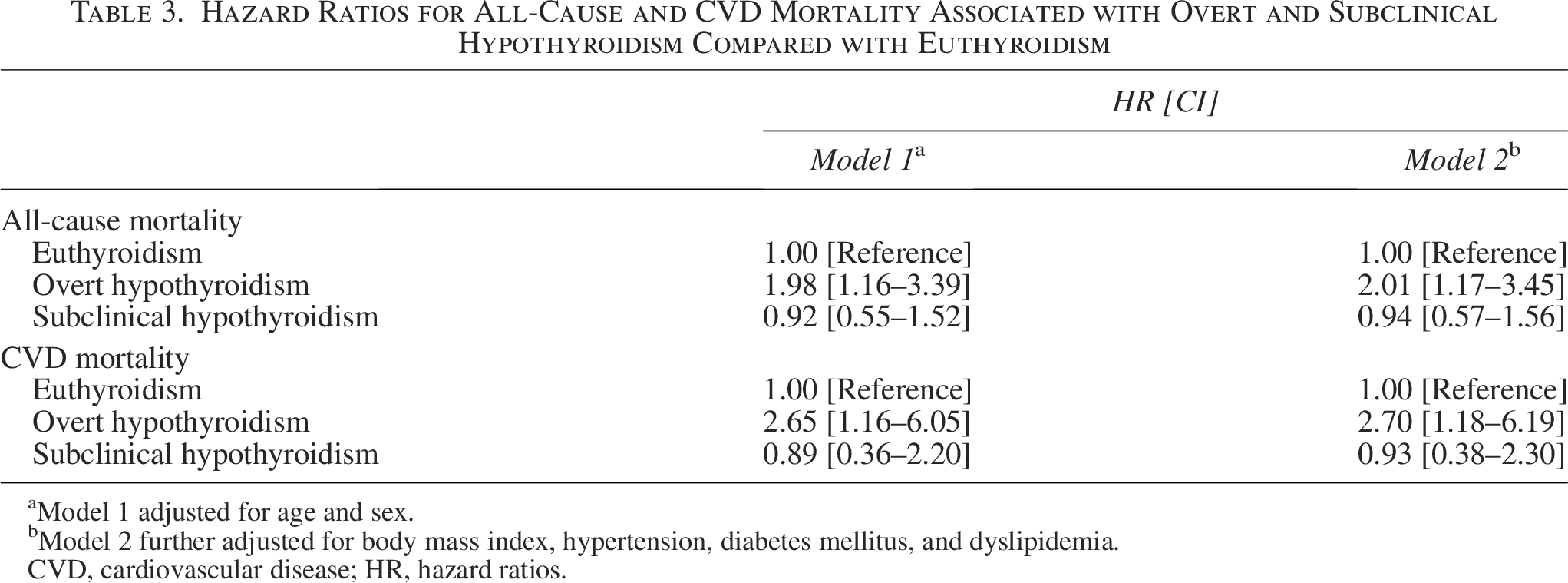
Model 1 adjusted for age and sex.
Model 2 further adjusted for body mass index, hypertension, diabetes mellitus, and dyslipidemia.
CVD, cardiovascular disease; HR, hazard ratios.
In sensitivity analyses restricted to complete case data, the results were consistent with the main findings (Supplementary Table S1). After excluding CVD deaths occurring within the first two years of follow-up, overt hypothyroidism remained significantly associated with higher risks of all-cause mortality (HR, 2.21; CI, 1.24–3.96) and CVD mortality (HR, 3.10; CI, 1.12–8.58) (Supplementary Table S2).
Subgroup analyses according to age and diabetes status
In stratified analyses, overt hypothyroidism was consistently associated with an increased risk of all-cause mortality across age groups (p for interaction = 0.480), although the associations did not reach statistical significance among participants aged 50 to 69 years or 70 years or older. Stratified analyses by diabetes status showed that the association between overt hypothyroidism and all-cause mortality was substantially stronger in participants with diabetes (HR, 5.45; CI, 2.46–12.07) than in those without diabetes (HR, 1.19; CI, 0.56–2.54) (p for interaction = 0.045) (Table 4
Hazard Ratios for All-Cause Mortality Associated with Overt Hypothyroidism Compared with Euthyroidism Stratified by Age Group and Diabetes Status
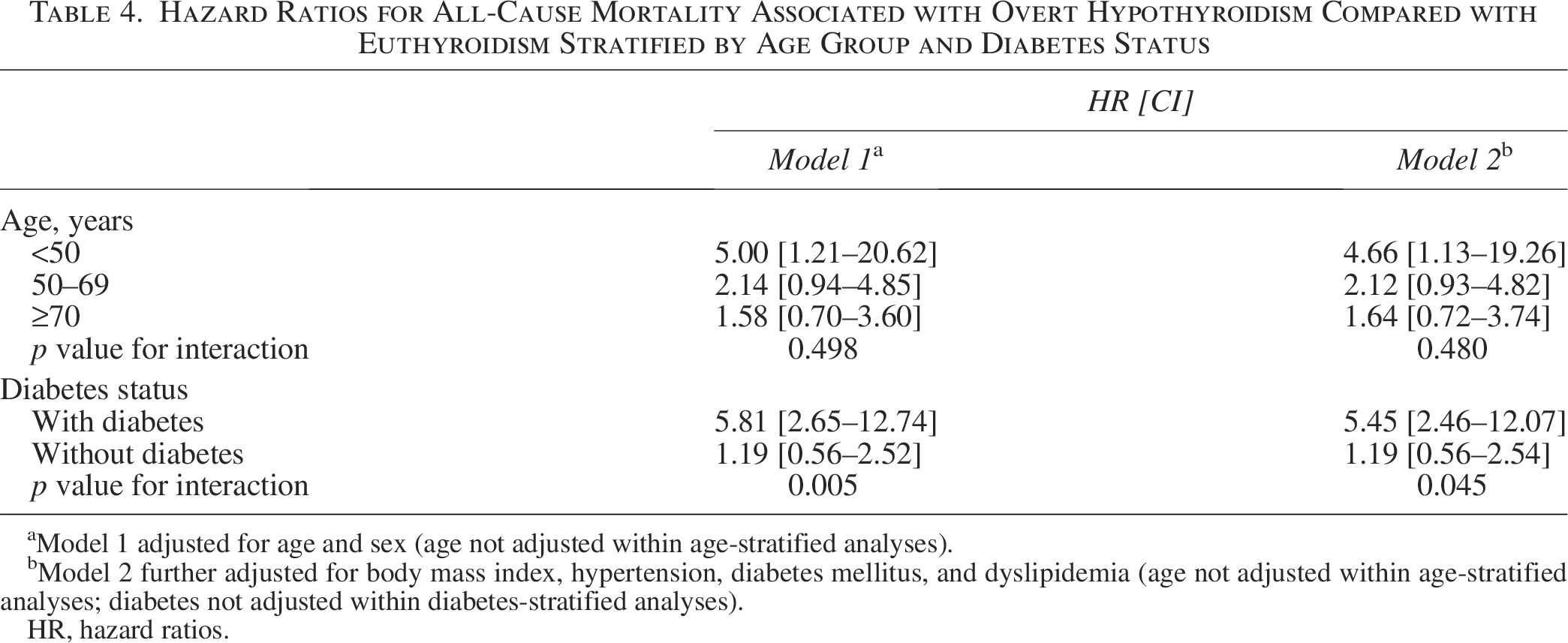
Model 1 adjusted for age and sex (age not adjusted within age-stratified analyses).
Model 2 further adjusted for body mass index, hypertension, diabetes mellitus, and dyslipidemia (age not adjusted within age-stratified analyses; diabetes not adjusted within diabetes-stratified analyses).
HR, hazard ratios.
Subclinical hypothyroidism was associated with a significantly increased risk of all-cause mortality among participants younger than 50 years (HR, 3.28; CI, 1.31–8.23), but not among those aged 50 to 69 years (HR, 0.32; CI, 0.08–1.31) or 70 years or older (HR, 1.00; CI, 0.51–1.98) (p for interaction = 0.022) (Table 5). Among participants younger than 50 years, subclinical hypothyroidism with the TSH concentration of 4.9–10 mIU/L was also significantly associated with elevated all-cause mortality risk (HR, 3.36; CI, 1.34–8.43) (Supplementary Table S3).
Hazard Ratios for All-Cause Mortality Associated with Subclinical Hypothyroidism Compared with Euthyroidism Stratified by Age Group and Diabetes Status
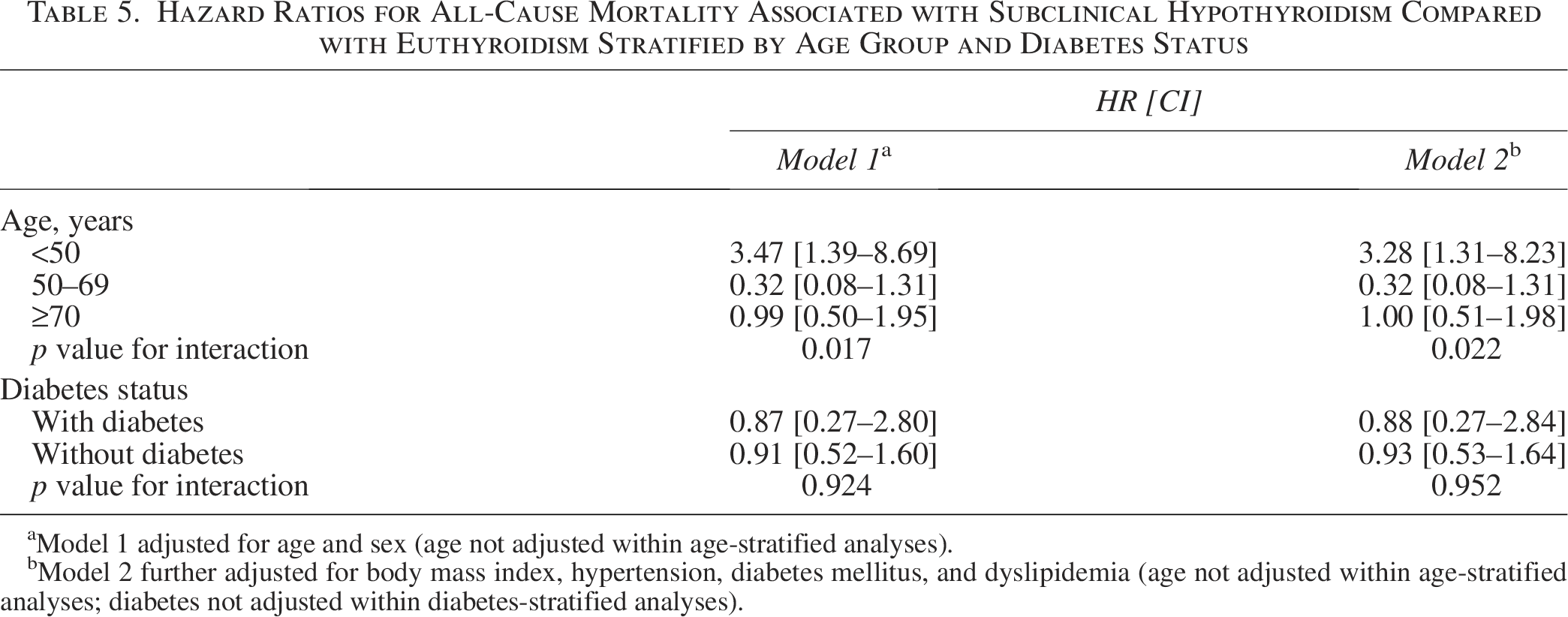
Model 1 adjusted for age and sex (age not adjusted within age-stratified analyses).
Model 2 further adjusted for body mass index, hypertension, diabetes mellitus, and dyslipidemia (age not adjusted within age-stratified analyses; diabetes not adjusted within diabetes-stratified analyses).
We additionally explored potential sex differences in the associations between hypothyroidism and mortality. No significant interaction between sex and overt or subclinical hypothyroidism was observed (all p for interaction >0.05) (Supplementary Table S4).
Discussion
Our results showed that overt hypothyroidism was significantly associated with increased mortality, with stronger associations observed among individuals with diabetes. Subclinical hypothyroidism was associated with increased mortality risk among individuals younger than 50 years, but not among those aged 50 to 69 years or 70 years or older. Notably, among younger adults, subclinical hypothyroidism with TSH levels between 4.9 and 10.0 mIU/L was also associated with increased mortality risk. To the best of our knowledge, this is the most comprehensive and up-to-date cohort study to systematically examine the associations of both overt and subclinical hypothyroidism with mortality in a large Chinese population, including stratified analyses by age and diabetes status. Our findings support the importance of the management of overt hypothyroidism, particularly in individuals with diabetes. For subclinical hypothyroidism, our findings suggest that even modest elevations in TSH may warrant clinical attention among younger adults.
Most long-term consequences of hypothyroidism have been investigated primarily in the context of subclinical hypothyroidism.3,6,8,27 A few studies have reported that overt hypothyroidism was associated with increased mortality in older adults. 9 Similar to the existing findings, 9 we observed that overt hypothyroidism was associated with increased all-cause and CVD mortality risks. Furthermore, stratified analyses showed that the association between overt hypothyroidism and mortality risk was stronger among individuals with diabetes compared with those without diabetes. Hypothyroidism and diabetes mellitus are two closely associated endocrine disorders. 11 Previous studies have consistently reported a higher prevalence of hypothyroidism among individuals with diabetes and, conversely, a higher prevalence of diabetes among those with hypothyroidism.10,28 The current evidence suggests that untreated hypothyroidism may impair glycemic control in patients with diabetes, and that appropriate treatment may improve clinical outcomes. 11 Several endocrine societies, such as the American Thyroid Association and the American Diabetes Association, have recommend routine screening for thyroid dysfunction in individuals with diabetes.29,30 Given the rising prevalence of both hypothyroidism and diabetes in China,2,31 our findings underscore the importance of the integrated management of these coexisting conditions. Further research is warranted to elucidate the relationship between hypothyroidism and diabetes mellitus and to clarify the underlying mechanisms driving their combined adverse effects.
Previous studies have evaluated the associations between subclinical hypothyroidism and mortality, but the findings remain inconsistent.5,7 Several meta-analyses have reported increased risks of all-cause and CVD mortality associated with subclinical hypothyroidism compared with euthyroidism.6,8 Similar associations have also been observed in cohort studies from the United States and Taiwan.3,5 However, this association was not confirmed in a large individual participant-based meta-analysis that included >55,000 participants. 4 In the present study, using the most recent Chinese standard reference ranges for thyroid hormones, we found no significant association between mortality risk and subclinical hypothyroidism. Differences between these studies are probably due to variations in the age distribution and the degree of TSH elevation across study populations.
Consistent with previous findings,7,8,32 we observed that the association between subclinical hypothyroidism and mortality varies by age. A meta-analysis found that subclinical hypothyroidism was associated with increased mortality risk in individuals younger than 65 years, but not in those aged 65 years or older. 8 Similar age-related differences have been reported in studies using a 60-year age cutoff. 9 Notably, studies among individuals aged 80–85 years and older have either reported no association between subclinical hypothyroidism and mortality risk 33 or have shown a survival benefit. 34 Our study also identified age-related differences when stratifying the population using a 50-year age threshold. In China, the most current national reference ranges for TSH concentrations issued by the National Health Commission do not provide age-specific cutoffs. These findings collectively support the growing recommendation to consider age-specific TSH reference ranges in clinical assessment and treatment decisions.
Most current international guidelines account for age in the management of subclinical hypothyroidism; yet, the recommended age thresholds for initiating treatment vary.23,35 The European Thyroid Association distinguishes subclinical hypothyroidism between patients below and above 70 years of age, with more conservative therapy in older patients. 36 The National Institute for Health and Care Excellence Clinical Knowledge Summary suggests observation for adults aged 65 years or older with TSH levels <10 mIU/L.23 In addition, studies examining age-specific reference intervals have suggested a potentially high rate of the overdiagnosis of subclinical hypothyroidism in individuals over the age of 50 or 60 years.37,38 Similarly, significant differences in TSH distributions were observed between Chinese adults younger and older than 50 years.24,25 In the present study, we observed age-related differences in the association between subclinical hypothyroidism and mortality when stratifying the population using a 50-year age threshold. These findings suggest the need for establishing more refined age-specific reference ranges across populations and assay platforms. Moreover, future large-scale cohort studies are warranted to examine the association between subclinical hypothyroidism and long-term adverse health outcomes across narrower age strata, to better inform age-specific clinical guidelines.
Previous studies have reported increased mortality in subclinical hypothyroidism with TSH levels >10 mIU/L, but not in subclinical hypothyroidism with TSH levels below this threshold. 4 The current clinical guidelines generally support thyroid hormone replacement when TSH levels are >10 mIU/L, but there remains no consensus regarding the treatment of subclinical hypothyroidism with TSH levels below this threshold. 35 Our study revealed that subclinical hypothyroidism with TSH levels <10 mIU/L was significantly associated with an increased risk of mortality among adults younger than 50 years, which suggests that even modest elevations in TSH may carry prognostic significance in younger individuals and warrant clinical consideration.
This study has several strengths. First, it used data from a large retrospective cohort with standardized and high-quality measurements of thyroid function obtained during routine health examinations. 12 Second, this study predominantly included young and middle-aged working populations, complementing prior evidence from community-dwelling cohorts composed largely of older adults. 8 Third, mortality outcomes were ascertained through linkage with the national surveillance system, which offers complete, medically verified outcome data using standardized ICD coding and has a low loss-to-follow-up rate (<1%). 18 Fourth, this study evaluated the associations of both overt and subclinical hypothyroidism with mortality, stratified by age and glycemic status, providing a comprehensive assessment of hypothyroidism-related mortality risk.
Our study has several limitations. First, our cohort was drawn from a single medical center in Beijing, which cannot fully represent the general population in China. Second, the follow-up period was relatively short, and the number of mortality events was limited, which may partly explain the wide CIs and precluded some stratified analyses. Longer follow-up in future studies is warranted to provide more precise and comprehensive risk estimates. Third, thyroid function was measured only once, and transient TSH elevations in some participants may have attenuated the observed associations between subclinical hypothyroidism and mortality. 39 Fourth, thyroid function testing was performed only at baseline, and we were unable to assess the potential impact of changes in thyroid function or thyroid hormone replacement therapy during follow-up on mortality risk. This limitation is common in prior studies,3–6 and only a few studies have incorporated such information, 27 highlighting the need for future studies with detailed longitudinal treatment data and repeated thyroid function measurements to clarify these effects. Fifth, baseline data on pre-existing CVD were unavailable, which could confound the observed associations. However, sensitivity analyses excluding CVD deaths within the first one or two years of follow-up yielded consistent results, suggesting that baseline CVD is unlikely to fully explain our findings. Finally, although models were adjusted for age, sex, and multiple metabolic factors, residual confounding from unmeasured factors may remain.
In summary, the study results contribute to the understanding of the mortality risks associated with overt and subclinical hypothyroidism in a Chinese population. The findings underscore the importance of managing overt hypothyroidism, particularly among individuals with diabetes. The age-dependent association between subclinical hypothyroidism and mortality supports the consideration of age-specific reference ranges for TSH, especially given that even modest elevations in TSH among younger adults may carry prognostic significance. Further large-scale studies are needed to evaluate health outcomes across more granular age groups and TSH categories to guide refined and individualized treatment strategies.
Authors’ Contributions
X.R. was involved in data curation (equal), formal analysis (lead), investigation (equal), writing—original draft (lead), and writing—review and editing (equal). N.W. was involved in data curation (equal), formal analysis (supporting), and writing—review and editing (equal). T.Z. was involved in data curation (equal), investigation (equal), writing—original draft (supporting), and writing—review and editing (equal). Z.F. was involved in writing—review and editing (supporting). G.C. was involved in supervision (supporting) and writing—review and editing (equal). X.M. was involved in conceptualization (lead), supervision (lead), and writing—review and editing (equal). All authors approved the final version of the article.
Footnotes
Acknowledgment
The authors want to thank the health workers of the Health Checkup Centre at China-Japan Friendship Hospital for providing detailed health checkup data.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the Noncommunicable Chronic Diseases-National Science and Technology Major Project (2024ZD0522300, 2024ZD0522301), Non-profit Central Research Institute Fund of Chinese Academy of Medical Sciences (2022-ZHCH330-01), Science and Technology Development Project of the Chinese Association of Rehabilitation Medicine (KFKT-2024-KY004), National High Level Hospital Clinical Research Funding, and Elite Medical Professionals Initiative of China-Japan Friendship Hospital (No. ZRJY2025-QMPY20).
Data Availability
Due to Chinese legal restrictions and the current ethical approval for the study, data are not publicly available for sharing, but a data dictionary and descriptive data in the table form are available from the corresponding author upon reasonable request.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.