
Abstract
Background:
The American Thyroid Association (ATA) guideline revisions in 2009 and 2015 encouraged a shift toward less extensive surgery and reduced use of radioactive iodine (RAI) in the management of patients with low-risk papillary thyroid carcinoma (PTC). The aim of this study was to evaluate the real-world impact of these guideline changes on treatment patterns, complications, and oncologic outcomes.
Methods:
In this retrospective cohort study conducted at a high-volume tertiary center in South Korea, we analyzed 31,861 patients treated for PTCs measuring ≤4 cm during 2004–2020. Patients were stratified into three temporal cohorts (triad 0 2004–2009; triad 1: 2010–2015; and triad 2: 2016–2020), and exact matching was performed to balance clinicopathologic characteristics across the groups. Segmented regression analysis was used to identify treatment pattern shifts. Postoperative complications and disease-free survival (DFS) were compared across the matched cohorts by using conditional logistic and stratified Cox regression analyses. Five-year restricted mean survival time (RMST) analysis was performed to adjust for follow-up variation.
Results:
After guideline implementation, total thyroidectomies and RAI use significantly declined. Permanent hypocalcemia decreased from 2.7% to 0.2% (p < 0.001) while transient complications remained stable. Although recurrence rates were lowest in the most recent era (1.3%), DFS analysis revealed higher hazard ratios for recurrence in triad 2 versus earlier cohorts (triad 2 vs. 0 hazard ratio: 1.520, confidence interval: 1.160–1.980). However, 5-year DFS and RMST comparisons revealed no significant differences.
Conclusions:
ATA guideline-driven de-escalation strategies were successfully implemented in real-world practice in this study, reducing overtreatment and surgical morbidity without compromising short-term oncologic outcomes.
Introduction
Thyroid cancer is a common endocrine malignancy with a globally rising incidence.1,2 The vast majority of cases are papillary thyroid carcinoma (PTC), which accounts for over 90% of all cases 3 and exhibits an excellent prognosis. 4 Despite increased detection rates due to advancements in diagnostic techniques over recent decades, 5 this trend is largely attributed to overdiagnosis, 6 as mortality rates have remained stable.4,7,8 Consequently, thyroid cancer management has shifted toward more conservative and personalized approaches to reduce the risk of overtreatment while enhancing patient outcomes.9,10
The American Thyroid Association (ATA) guidelines have significantly influenced the development of these changing treatment strategies. The 2009 ATA guidelines recommended total thyroidectomy (TT) as the standard initial surgery for malignant papillary thyroid tumors >1 cm and suggested lobectomy for very low-risk papillary thyroid microcarcinomas (PTMC; those <1 cm). 11 Subsequent studies demonstrated minimal long-term prognostic differences between lobectomy and TT in low-risk patients with tumors 1–4 cm in size,12–14 supported by evidence that the benefits of radioactive iodine (RAI) therapy are not uniformly applicable across all patients.15,16 Accordingly, the 2015 ATA guidelines introduced active surveillance for very-low-risk PTMC, permitted lobectomy for low-risk patients, and imposed stricter criteria for RAI therapy. 17 Those changes were made to minimize complications from unnecessary surgery and treatment while improving patients’ quality of life, given the stable mortality rates of thyroid cancer.12,18,19
Although numerous studies have been conducted to examine the effects of these guideline revisions, further investigation is warranted to clarify their impact on clinical decision-making and long-term outcomes in specific institutional settings. In this study, we analyzed the management trends of patients with PTC at a high-volume center from 2004 to 2020, focusing on changes in surgical extent and the use of RAI therapy following the 2009 and 2015 ATA guidelines. Additionally, we assessed how these evolving treatment strategies influenced postoperative complications and recurrence rates. By examining a large cohort with long-term follow-up, we aimed to provide meaningful insights into the practical implementation of guideline-based management and its oncologic outcomes.
Materials and Methods
Study design and population
In this retrospective cohort study, we evaluated changes in the management and outcomes of PTC at Severance Hospital, Yonsei University College of Medicine, Seoul, Korea, from January 2004 to December 2020. We included patients diagnosed with PTC with tumor sizes ≤4 cm, confirmed via histopathological examination. The study population was stratified into three cohorts based on the timing of the ATA guideline revisions: triad 0 (2004–2009), triad 1 (2010–2015), and triad 2 (2016–2020). The study protocol was approved by the Institutional Review Board of Severance Hospital, Yonsei University Health System (IRB no.: 4-2023-0462). The need to obtain written informed consent was waived by the Board because of the retrospective nature of the study.
Data collection
Clinical and pathological data were retrospectively collected, including patient demographics (age and sex), tumor characteristics (size, extrathyroidal extension [ETE], multifocality, and pathological subtype), the surgical extent (lobectomy vs. TT), with prophylactic central compartment neck dissection uniformly performed for all patients, the use of RAI therapy, and postoperative outcomes (recurrence and complications such as hematoma, seroma, recurrent laryngeal nerve [RLN] injury, and transient and permanent hypocalcemia). Hematoma was defined as a postoperative neck bleeding event, classified as either requiring surgical reoperation or managed conservatively without reoperation, and seroma was defined as a fluid collection requiring aspiration. RLN injury was determined by postoperative laryngoscopy examination. RLN palsy was classified as transient if vocal cord mobility recovered within 6 months and permanent if vocal cord paralysis persisted beyond 6 months. Transient hypoparathyroidism was defined as symptomatic hypocalcemia or the need for calcium/vitamin D supplementation that resolved within 6 months after surgery. Permanent hypoparathyroidism was defined as persistent hypocalcemia beyond 6 months, requiring ongoing supplementation, with or without low parathyroid hormone levels.
Tumor staging was determined according to the Tumor–Node–Metastasis (TNM) classification system (7th edition of the American Joint Committee on Cancer). In addition, patients were stratified into low-, intermediate-, and high-risk groups according to the 2015 ATA risk stratification system (ATA-RSS). Specifically, the risk categories were defined based on pathological features as follows: low-risk (intrathyroidal disease, N0, no ETE); intermediate-risk (microscopic ETE, N1a, or multifocality); and high-risk (macroscopic ETE, N1b, or distant metastasis [M1]).
Recurrence was defined as cytologically or histologically confirmed locoregional disease during follow-up, or distant disease confirmed either by biopsy or by concordant imaging findings with concomitant thyroglobulin elevation. Pure biochemical recurrence without structural evidence was not considered.
Statistical analysis
All statistical analyses were performed using R software (version 4.4.0, http://www.R-project.org) and the IBM SPSS Statistics for Windows (version 21.0; IBM Corp., Armonk, NY). To account for potential confounding variables and ensure comparability across the three time periods, exact matching was used. We matched patients based on categorical variables (sex, age group [<55 years and ≥55 years], tumor size [≤1 cm, >1 cm to ≤2 cm, and >2 cm to ≤4 cm], ETE [none, microscopic, and macroscopic], and pathological N stage [N0, N1a, and N1b]) to ensure complete agreement between pairs. The matching process was carried out sequentially, first between triads 0 and 1 and thereafter with triad 2, resulting in 7660 matched patients per group. The quality of matching was evaluated using standardized mean differences (SMDs), with an SMD <0.1 defined as an adequate balance. Postmatching SMD values were <0.1 for all covariates.
Segmented regression analysis was performed to evaluate temporal changes in TT and RAI use. Raw annual rates were additionally plotted to directly illustrate observed changes across different guideline periods. To assess risk-specific differences in oncologic outcomes, Kaplan–Meier analyses were conducted across triads stratified by the ATA 2015 risk classification.
Outcomes were separately analyzed via conditional logistic regression for binary outcomes (e.g., complications) and stratified Cox regression for survival endpoints, to account for the matched data structure. Survival endpoints were disease-free survival (DFS) and restricted mean survival time (RMST). DFS was defined as the time from surgery to recurrence, with censoring applied at 5 years for the 5-year DFS analysis to standardize the follow-up duration. The RMST, calculated as the average survival time up to a restricted time point (tau = 5 years), was used to compare survival differences across groups, with beta coefficients representing the mean difference in survival time. Statistical significance was defined as a p value <0.05. All confidence intervals (CIs) were reported at the 95% level. For consistency, all comparisons were presented with the reference category placed after “vs.” (e.g., 1 vs. 0, 2 vs. 1, and 2 vs. 0).
Results
Patient demographics and baseline characteristics
In total, 31,861 patients were included in the analysis: 7841 in triad 0, 12,452 in triad 1, and 11,568 in triad 2. Baseline clinicopathological characteristics are summarized in Table 1. The proportion of female patients decreased from 86.6% in triad 0 to 78.4% in triad 2 (p < 0.001), and the percentage of patients aged ≥55 years slightly declined from 23.0% to 20.5% (p < 0.001). Although the tumor size distribution and minimal ETE remained relatively stable, macroscopic ETE increased from 7.2% to 10.6% (p < 0.001), and multifocality also rose from 11.2% to 13.8% over time (p < 0.001). The median (interquartile range) follow-up durations were 188 (177–205), 131 (114–148), and 70 (66–79) months for triads 0, 1, and 2, respectively.
Baseline Clinicopathological Characteristics of Study Patients
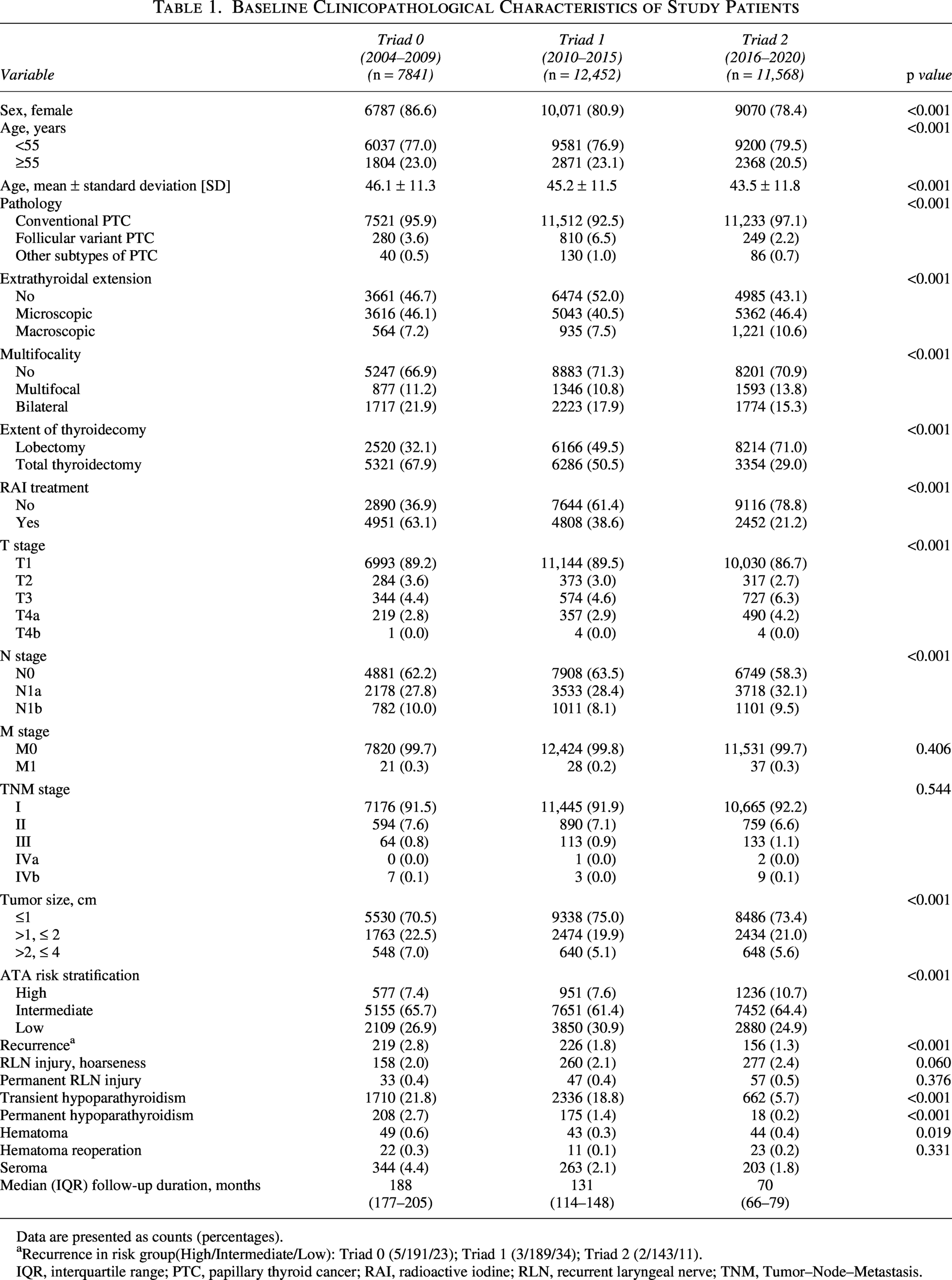
Data are presented as counts (percentages).
Recurrence in risk group(High/Intermediate/Low): Triad 0 (5/191/23); Triad 1 (3/189/34); Triad 2 (2/143/11).
IQR, interquartile range; PTC, papillary thyroid cancer; RAI, radioactive iodine; RLN, recurrent laryngeal nerve; TNM, Tumor–Node–Metastasis.
To reduce selection bias and ensure robust comparisons of outcomes across the three eras, we performed exact matching. Table 2 presents the baseline characteristics after matching, demonstrating excellent balance across key clinicopathological variables (nearly identical among the groups), thereby minimizing potential confounding caused by baseline heterogeneity.
Standardized Mean Difference of the Baseline Characteristics before/after Matching
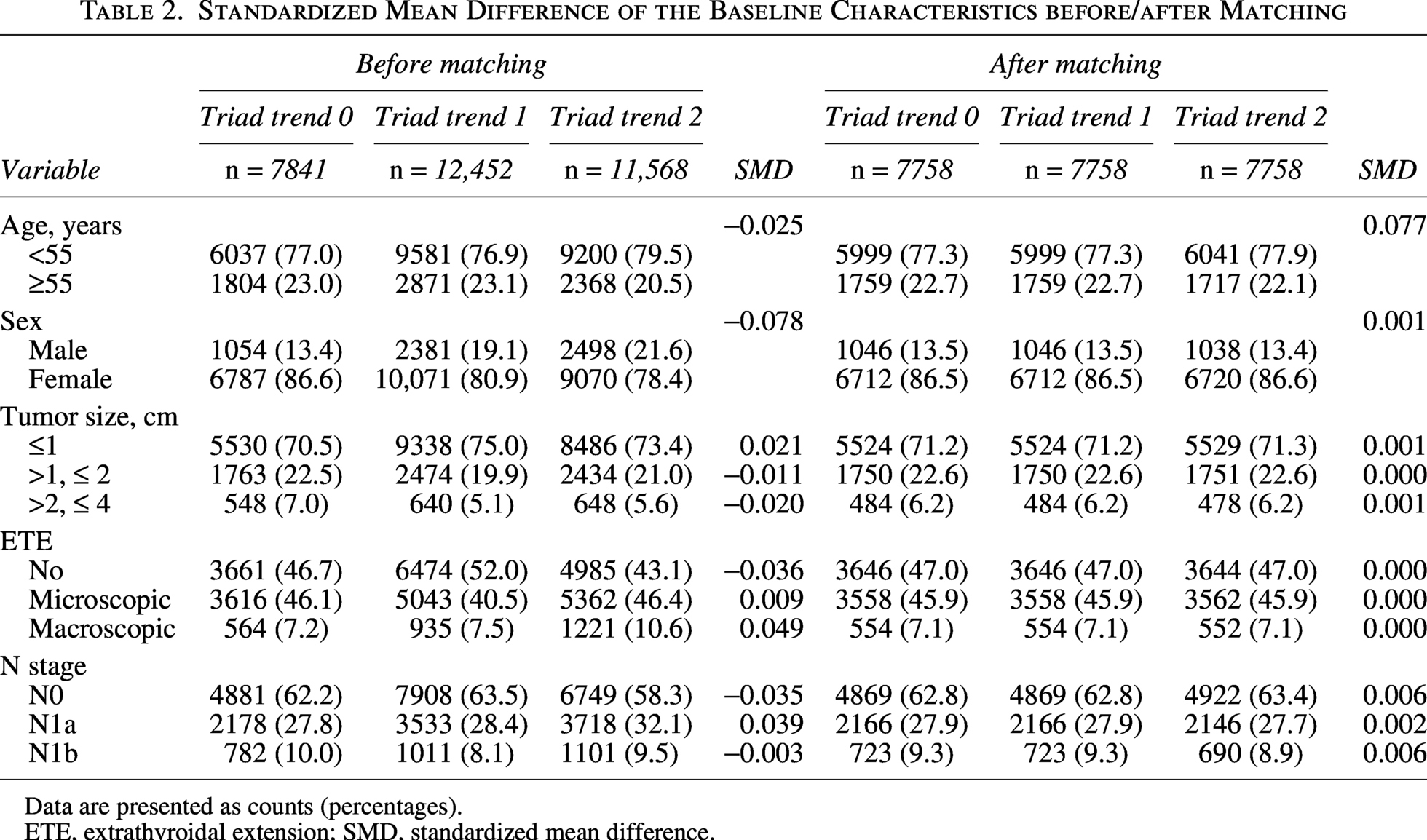
Data are presented as counts (percentages).
ETE, extrathyroidal extension; SMD, standardized mean difference.
Treatment pattern shifts
Substantial shifts in both surgical and adjuvant treatment strategies were observed over the study period, corresponding closely with the release of the 2009 and 2015 ATA guidelines. As shown in Figures 1A–B, annual rates of TT steadily declined across all ATA risk groups, although the absolute proportion of TT differed by baseline risk category. Segmented regression analysis of the overall cohort (Fig. 1C) identified statistically significant inflection points in 2009 and 2017, indicating periods when practice patterns shifted most prominently. Before 2009, TT use decreased slowly and did not reach statistical significance (slope: −1.10%/year, p = 0.124). Between 2009 and 2017, however, the decline accelerated markedly (slope: −4.56%/year, p < 0.001), consistent with the guideline-driven expansion of lobectomy eligibility. After 2017, the trend plateaued (slope: −0.37%/year, p = 0.695), suggesting stabilization of surgical practice in the contemporary era (Table 3).
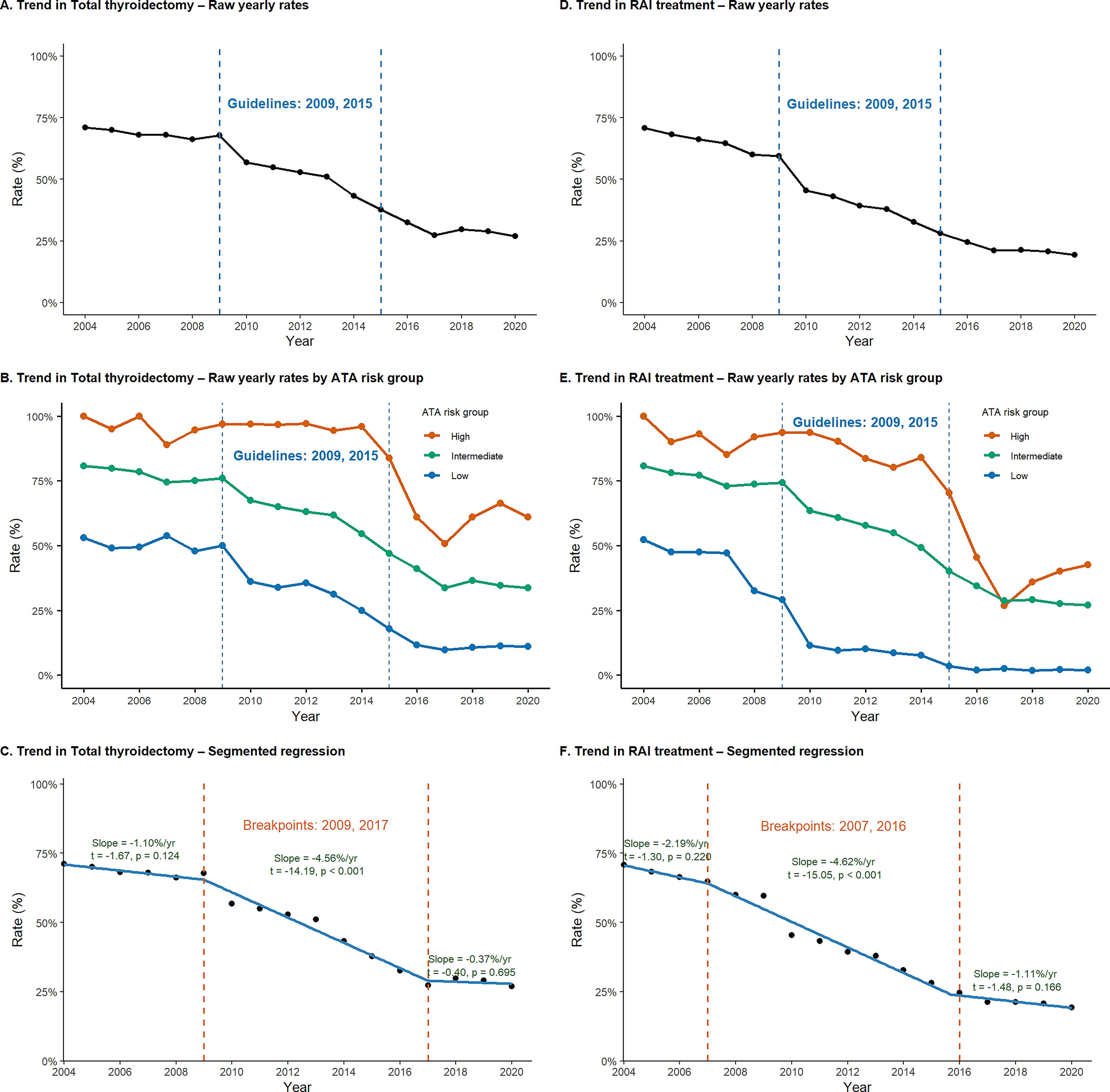
Trends in total thyroidectomy and radioactive iodine (RAI) treatment according to ATA risk stratification and surgical era (Triads 0–2). This multipanel figure depicts temporal changes in the rates of total thyroidectomy and postoperative RAI therapy from 2004 to 2020. The y-axis in all panels represents the proportion of patients (%), and the x-axis represents calendar year. Blue vertical dashed lines indicate the publication years of the ATA guidelines (2009 and 2015). Orange vertical dashed lines in the segmented regression panels represent the estimated breakpoints and corresponding changes in slope.
Segmented Regression Analysis for Treatment Trends
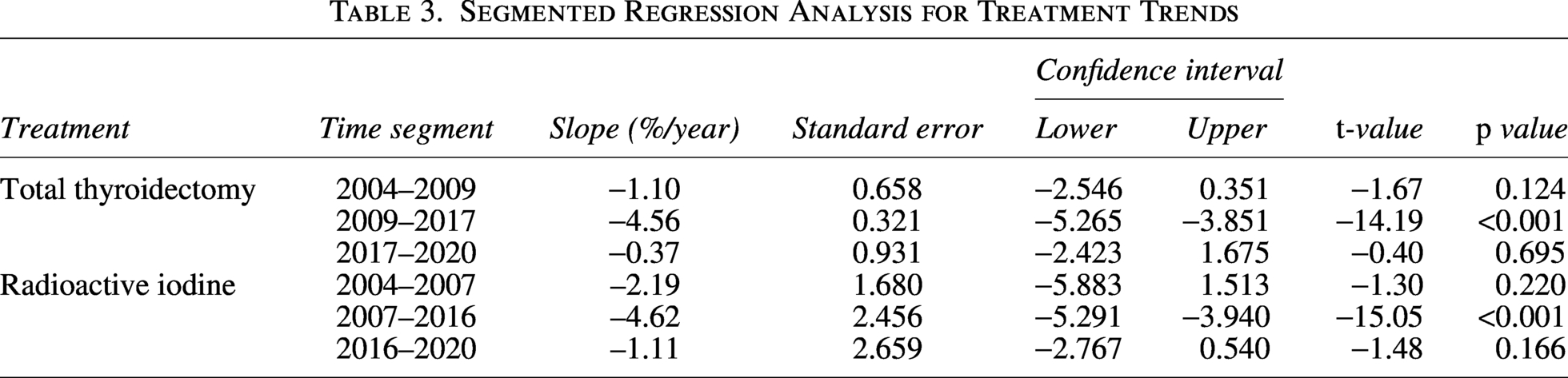
The use of postoperative RAI therapy exhibited a parallel but slightly earlier pattern of reduction (Figs. 1D–E). Segmented regression identified significant breakpoints at 2007 and 2016 (Fig. 1F). Prior to 2007, the decline in RAI administration was modest and not statistically significant (slope: −2.19%/year, p = 0.220). A pronounced decrease was observed from 2007 to 2016 (slope: −4.62%/year, p < 0.001), aligning with the emerging emphasis on selective RAI use. After 2016, the rate of decline slowed (slope: −1.11%/year, p = 0.166), reflecting stabilized adoption of risk-adapted postoperative management (Table 3).
Across all analyses, stratification by ATA 2015 risk categories demonstrated parallel reductions in both TT and RAI use among low-, intermediate-, and high-risk groups (Fig. 1B and E), indicating that temporal de-escalation in treatment was broadly applied across risk strata rather than being confined to any single subgroup.
Postoperative outcomes
In the unmatched cohort, the frequency of postoperative complications declined across the study periods, as detailed in Table 1. Permanent hypoparathyroidism decreased from 2.7% in triad 0 to 0.2% in triad 2 (p < 0.001). Hematoma and seroma rates also significantly decreased, whereas rates of transient hypocalcemia and RLN injury remained stable.
In the matched cohort, outcome analysis (Table 4 and Fig. 2; see Supplementary Table S1 for unmatched data) demonstrated consistent results. Adjusted odds ratios (ORs) for permanent hypoparathyroidism decreased significantly over time (triad 1 vs.0: OR = 0.701, CI = 0.562–0.874, p = 0.002; triad 2 vs.0: OR = 0.078, CI = 0.047–0.130, p < 0.0001). Odds of hematoma and seroma also declined (hematoma, triad 2 vs. 0: OR = 0.408, CI = 0.243–0.687, p = 0.001; seroma, triad 2 vs. 0: OR = 0.392, CI = 0.319–0.482, p < 0.0001), while RLN injury did not differ significantly between triads (See Supplementary Fig. S1 for risk-stratified complication rates).
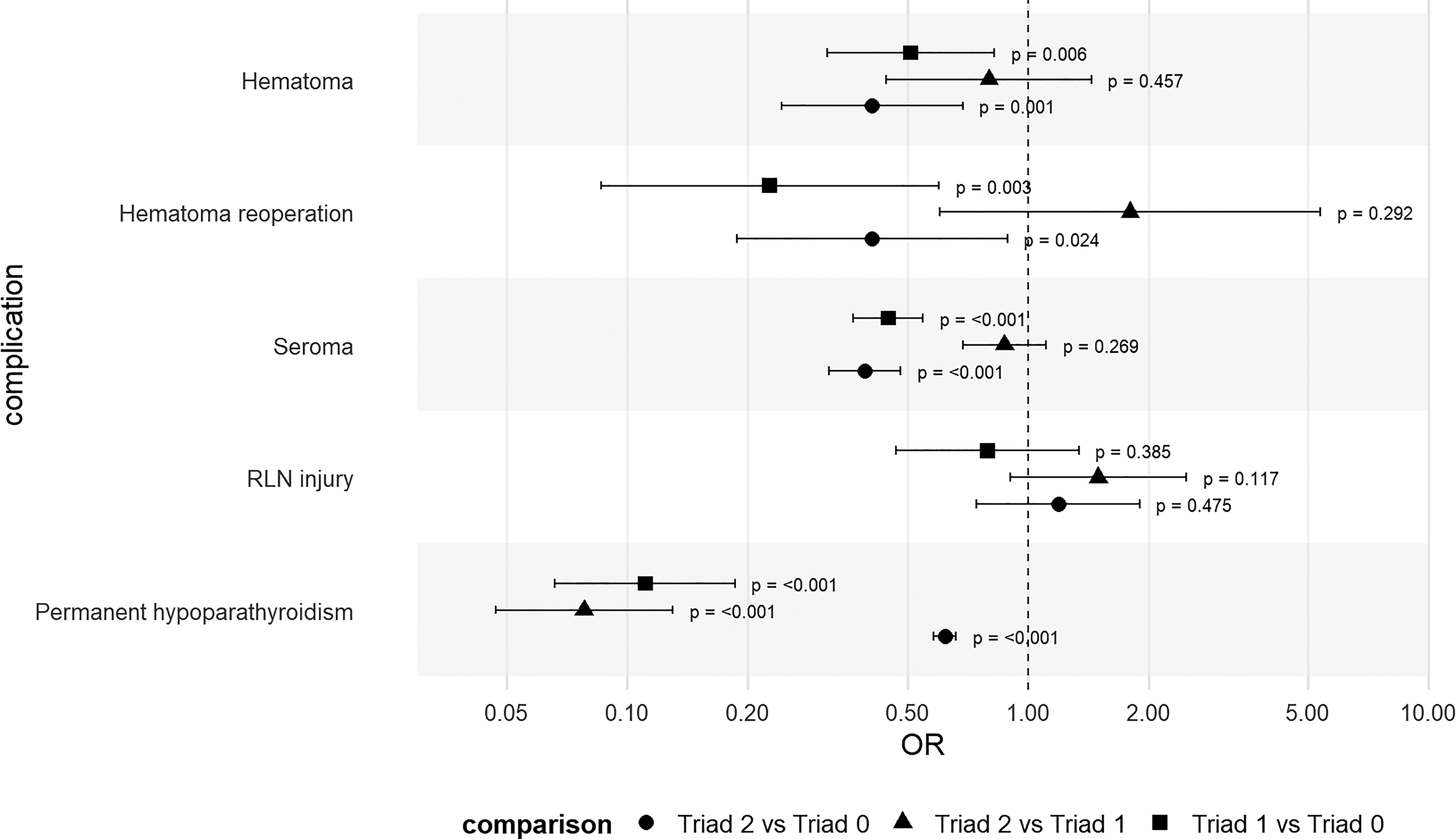
Adjusted postoperative complication outcomes across eras (matched cohort). Forest plot showing adjusted odds ratios (ORs) with confidence intervals (CIs) for major postoperative complications across three time periods. Triad 0 = 2004–2009, Triad 1 = 2010–2015, Triad 2 = 2016–2020. RLN, recurrent laryngeal nerve.
Outcome Analysis of Postoperative Complications after Matching
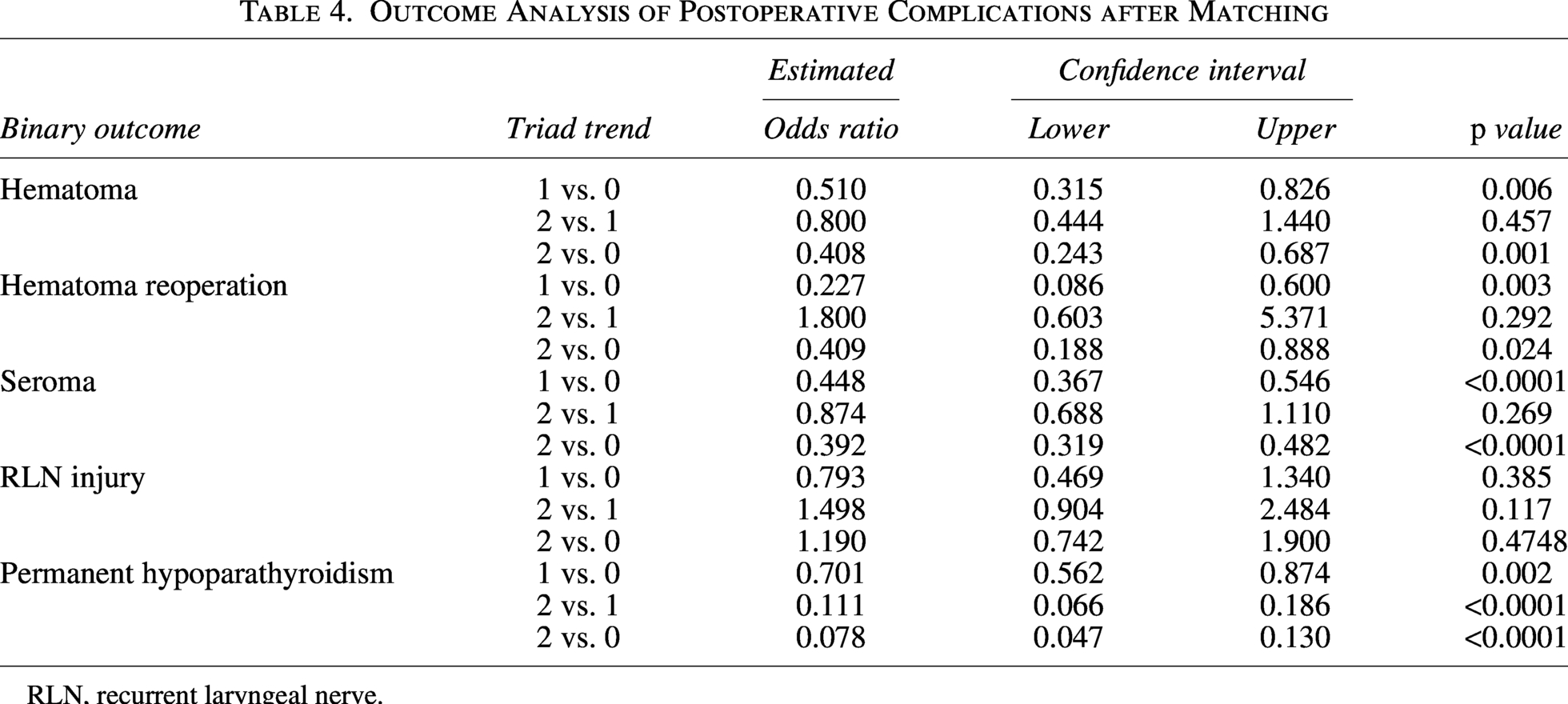
RLN, recurrent laryngeal nerve.
Recurrence and survival outcomes
In the unmatched cohort, the overall recurrence rate decreased from 2.8% in triad 0 to 1.3% in triad 2 (p < 0.001; Table 1; detailed recurrence patterns and treatments are provided in Supplementary Table S2). By the ATA risk classification, the proportion of high-risk patients increased from 7.4% to 10.7%, intermediate-risk patients remained relatively stable (65.7–64.4%), and low-risk patients decreased from 26.9% to 24.9% (p < 0.001).
As shown in Table 5, the patterns differed across risk categories. In the low-risk group, no significant differences in 5-year DFS were observed across triads (see Supplementary Tables S3 and S4 for detailed results of the sensitivity analysis excluding papillary thyroid microcarcinomas) (Supplementary Figs. S2A-C). By contrast, the intermediate-risk group demonstrated a significantly lower recurrence risk in triad 1 compared with triad 0 (hazard ratio [HR] = 0.64, CI = 0.50–0.82, p < 0.001), whereas triad 2 showed a significantly higher risk compared with both triads 0 and 1 (HR = 1.39, CI = 1.01–1.90, p = 0.044; HR = 2.38, CI = 1.70–3.32, p < 0.001). In the high-risk group, triad 2 was also associated with a higher recurrence risk compared with triad 0 (HR = 2.10, CI = 1.28–3.44, p = 0.003).
Hazard Ratios and 5-Year DFS (%) by ATA Risk Group and Triad (before Matching)
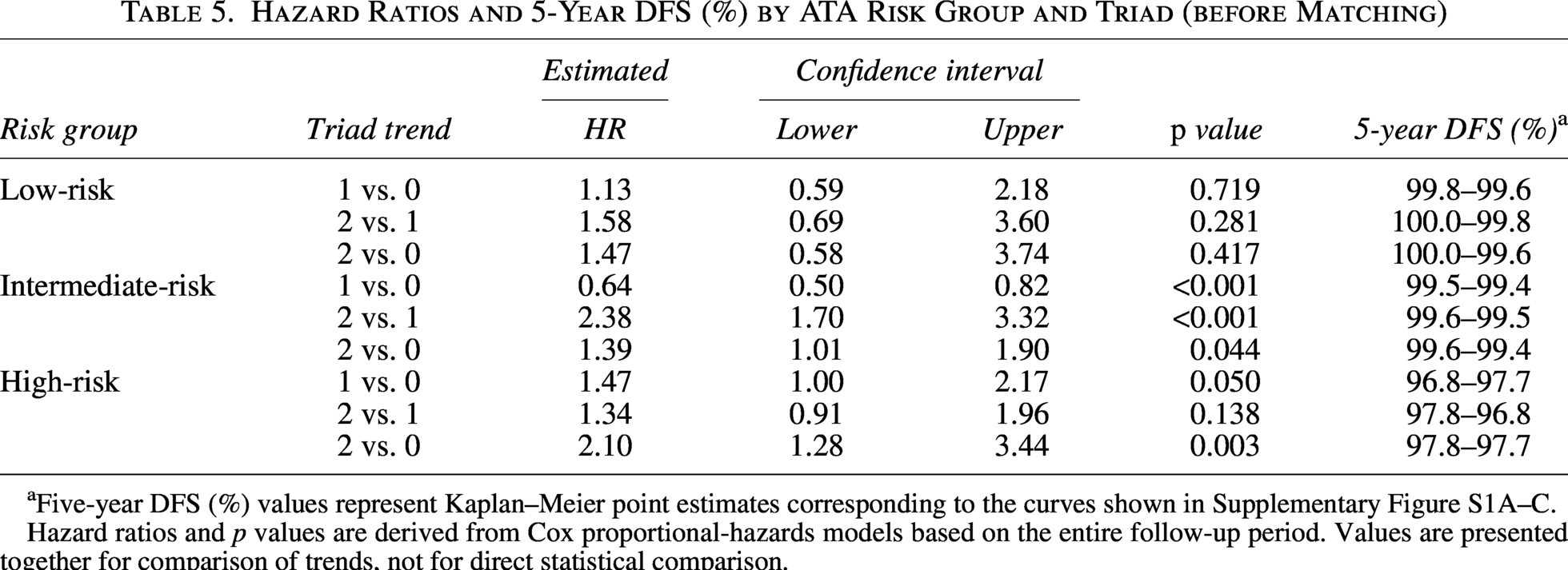
Five-year DFS (%) values represent Kaplan–Meier point estimates corresponding to the curves shown in Supplementary Figure S1A–C.
Hazard ratios and p values are derived from Cox proportional-hazards models based on the entire follow-up period. Values are presented together for comparison of trends, not for direct statistical comparison.
As shown in Table 6 and Figure 3, stratified Cox regression analysis of DFS in the matched cohort revealed no significant difference in the recurrence risk between triads 0 and 1 (HR = 0.973, CI = 0.777–1.220, p = 0.809). However, DFS comparisons involving triad 2 indicated a modest increase in recurrence risk relative to triad 0 (HR = 1.520, CI = 1.160–1.980, p = 0.002) and to triad 1 (HR = 1.560, CI = 1.190–2.040, p = 0.001). To account for differences in follow-up duration, we also performed 5-year-censored DFS and RMST analyses. These revealed no statistically significant differences between groups. For example, the HR for 5-year-censored DFS between triads 0 and 2 was 0.883 (CI = 0.570–1.370, p = 0.575), and the RMST difference was −0.010 months (CI = –0.047 to 0.027, p = 0.586) (Supplementary Table S5 for unmatched survival outcomes).
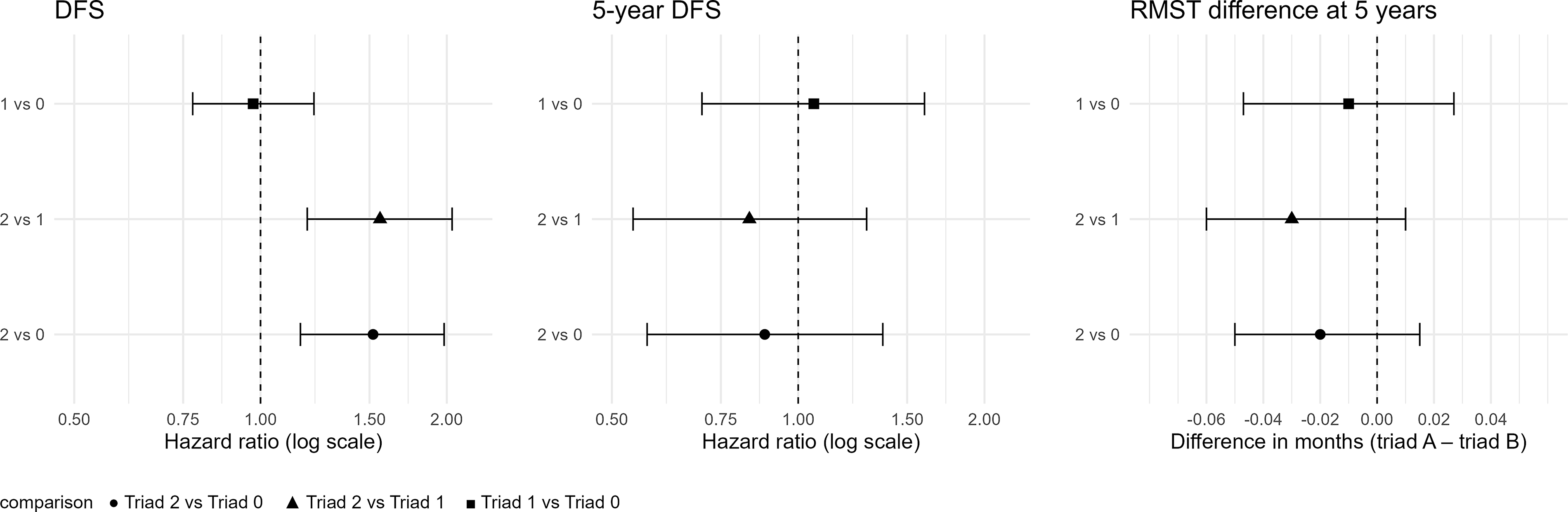
Survival outcomes in the matched cohort. Stratified Cox HRs (left), 5-year–censored DFS (middle), and 5-year RMST (right). Triad 0 = 2004–2009, Triad 1 = 2010–2015, Triad 2 = 2016–2020. DFS, disease-free survival; RMST, restricted mean survival time. (See also Table 6 for the matched estimates).
Outcome Analysis for Matched Data (Progression-Free Survival)
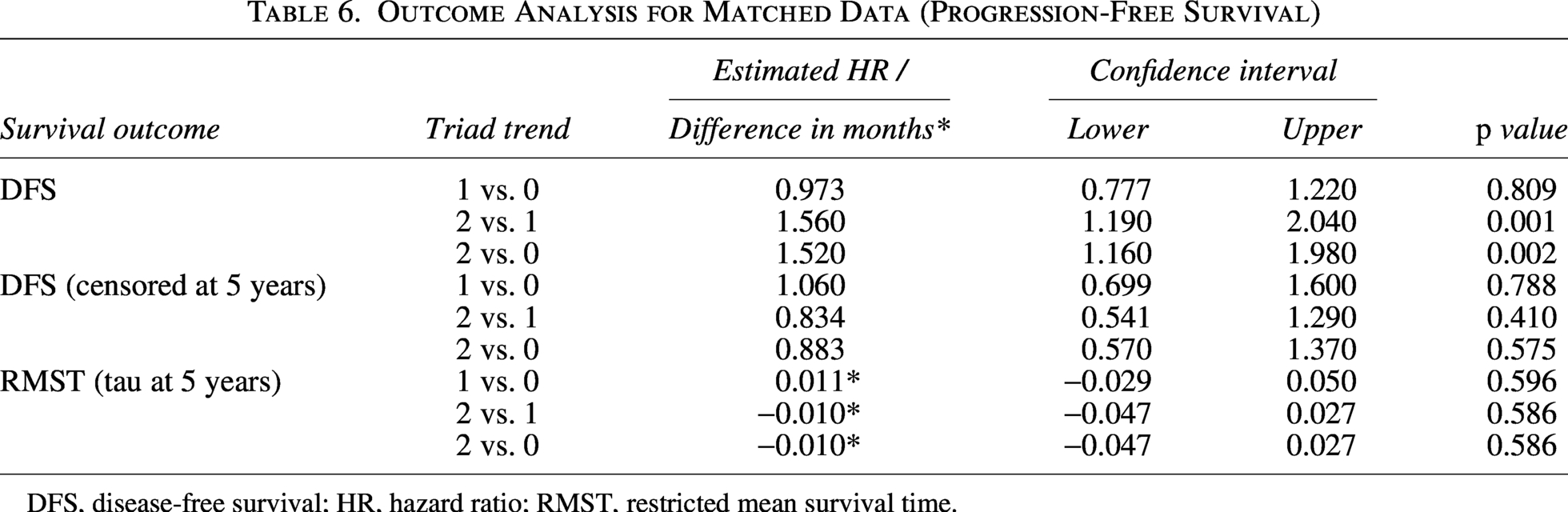
DFS, disease-free survival; HR, hazard ratio; RMST, restricted mean survival time.
Discussion
In this study, we analyzed evolving trends in surgical and adjuvant treatment strategies for PTC at a high-volume tertiary institution from 2004 to 2020, focusing on the real-world impact of the 2009 and 2015 ATA guideline updates. In a cohort of 31,861 patients, we observed significant changes in the extent of thyroid surgery and RAI therapy, accompanied by shifts in complication and recurrence patterns.
At our institution, a significant transition toward more conservative management of patients with PTC was observed over the study period. Segmented regression identified inflection points in TT and RAI rates in 2017 and 2016, respectively. TT declined by 4.56% per year until 2017 and RAI by 4.62% per year until 2016, after which both trends plateaued. Since breakpoints reflect statistical estimation rather than policy dates, we also presented raw annual rates, which visibly declined after the 2009 and 2015 guideline revisions. When stratified by the ATA 2015 risk groups, segmented regression revealed comparable temporal patterns across strata, including the high-risk cohort, with all groups demonstrating parallel reductions in TT and RAI use over time. These findings were consistent with broader national and international trends. Gordon et al. reported a nationwide increase in the use of lobectomy and a concomitant reduction in RAI use following the publication of the revised ATA guidelines in the United States. 20 Similarly, Ullmann et al., using data from the National Surgical Quality Improvement Program, documented a marked rise in lobectomy rates after 2015. 21 Collectively, these external data reinforce the observed national and institutional shifts toward less extensive treatment modalities, particularly the increased use of lobectomy and the reduced reliance on adjuvant RAI therapy, following the publication of the revised ATA guidelines.
The observed declines in TTs and RAI use were accompanied by improved postoperative outcomes, consistent with established evidence that lobectomy—a key component of surgical de-escalation—is associated with a significantly lower complication risk. In a meta-analysis by Hsiao et al., lobectomy was associated with lower rates of transient RLN injury (2.0% vs. 4.2%), transient hypoparathyroidism (2.2% vs. 21.3%), and permanent hypoparathyroidism (0% vs. 1.8%) than TT. 22
Consistent with those results, our institutional data demonstrated a significant reduction in permanent hypoparathyroidism, from 2.7% to 0.2% over time, alongside declines in hematoma and seroma rates. Importantly, in the matched cohort analysis, which accounted for baseline imbalances across eras, adjusted odds ratios confirmed significant reductions in permanent hypoparathyroidism (triad 2 vs. 0: OR = 0.078, CI = 0.047–0.130), hematoma (OR = 0.408, CI = 0.243–0.687), and seroma (OR = 0.392, CI = 0.319–0.482), further supporting the robustness of these trends.
The relative stability of transient complications in this study further suggests that the shift toward less aggressive surgery did not compromise procedural safety. Collectively, these results affirm the clinical feasibility and safety of lobectomy as a contemporary surgical strategy in appropriately selected patients. However, as this was an observational, single-center analysis, these findings should not be interpreted as definitive evidence of noninferiority
Despite the favorable temporal trends in treatment intensity and complication rates in this study, the oncologic consequences of this shift require nuanced interpretation. Since these changes reflected a deliberate effort to minimize overtreatment in patients with low- to intermediate-risk disease, we examined whether disease control varied by underlying risk.
In the unmatched whole cohort, risk-stratified analyses demonstrated that the oncologic impact of treatment de-escalation varied substantially across ATA risk categories. For low-risk patients, outcomes remained uniformly excellent, with 5-year DFS consistently above 99% and no significant temporal differences. This is consistent with maintained disease control under guideline-based de-escalation in this population.
By contrast, intermediate-risk patients displayed subtle but meaningful temporal variation. Although absolute 5-year DFS remained high at 99.4–99.6%, HRs indicated an excess risk in triad 2 compared with earlier eras (triad 2 vs. triad 1: HR 2.38, CI 1.70–3.32, p < 0.001; triad 2 vs. triad 0: HR 1.39, CI 1.00–1.90, p = 0.044). These findings suggest that, even within a group typically considered suitable for conservative management, cautious patient selection is essential. The results highlight the heterogeneity of intermediate-risk disease and suggest that indiscriminate de-escalation may not be appropriate.
High-risk patients showed the lowest 5-year DFS (96.8–97.8%), and the most pronounced decline was observed in triad 2. Survival analyses confirmed significantly inferior outcomes compared with earlier eras (triad 2 vs. triad 0: HR 2.10, CI 1.28–3.44, p = 0.003). Importantly, this decline is unlikely to reflect reduced treatment efficacy.
Collectively, these patterns emphasize that the feasibility of de-escalation is strongly risk-dependent. In low-risk patients, conservative strategies maintain oncologic safety, whereas in intermediate-risk disease, selective de-escalation remains feasible but requires stringent risk stratification. By contrast, the declining DFS signal in high-risk patients underscores the continued need for intensified management. These principles affirm that aligning treatment intensity with ATA risk categories is critical to maintaining oncologic control while minimizing overtreatment.
Notably, the signal of lower DFS in triad 2 observed in the unmatched cohort was also reproduced in the matched cohort, where Cox regression demonstrated significantly lower DFS compared with earlier eras. Rather than representing a true deterioration in survival outcomes, this apparent decline is most plausibly explained by several methodological and clinical factors: (1) shorter follow-up in triad 2, which concentrated early events and depressed DFS estimates; (2) a shift toward a higher-risk patient distribution in triad 2, consistent with the baseline characteristics, partly reflecting broader adoption of active surveillance for small, low-risk tumors, which reduced low-risk operations and increased the relative proportion of higher-risk cases among operated patients; and (3) more sensitive surveillance modalities in the most recent era (e.g., high-resolution ultrasound), increasing detection of subclinical recurrences.
To minimize the influence of these methodological factors, we additionally performed 5-year–censored DFS and RMST analyses on the matched cohort. Importantly, both approaches revealed no statistically significant differences across the eras, suggesting that the timing and clinical impact of recurrences remained comparable. The application of RMST analysis, which accounts for variations in the follow-up duration and censoring, helped to mitigate potential detection bias and reinforces the interpretation that the adoption of ATA guideline–based conservative treatment strategies was associated with maintained oncologic stability in terms of recurrence. These findings complement the apparent decline in DFS observed in triad 2 and support the view that this signal does not reflect a true deterioration in outcomes. Because DFS was defined as time from initial surgery to first confirmed recurrence, any postrecurrence treatments did not affect event ascertainment or the DFS comparisons across eras (Supplementary Table S2).
These observations are concordant with meta-analyses and a large-scale observational study, suggesting that lobectomy may offer comparable oncologic outcomes to TT in patients with low-risk PTC,23–25 and even in selected patients with intermediate-risk PTC.26,27 Reported recurrence rates after lobectomy generally range from 4% to 9%, with long-term disease control achieved in most cases.28–30
Interpretation of our findings should take into account the retrospective and single-center nature of the study, which might have limited their applicability to broader clinical settings. Changes in imaging technology over the study period might have influenced recurrence detection, particularly in more recent cohorts. In addition, the lack of detailed patient data and patient-specific risk factors (e.g., molecular markers such as BRAF mutations, underlying diseases, socioeconomic status, education, and health insurance) may have limited the granularity of our analyses. Data on TSH suppressive therapy, including target TSH levels and actual achieved values, were also unavailable, despite the increasing relevance of TSH suppression as surgical extent decreases and RAI use declines. Furthermore, the 2015 ATA RSS used in this study was applied based on the available clinicopathologic variables, without incorporating more granular parameters such as the number or size of metastatic lymph nodes, vascular invasion, or aggressive histologic subtypes. Although these details are emphasized in the latest ATA (2025) and WHO (5th edition, 2025) classifications, such information was not consistently available in our legacy cohort (2004–2020). These limitations should be considered when interpreting the risk-stratified analyses.
This study demonstrated that the adoption of the ATA guideline-driven management led to a measurable shift toward less aggressive treatment of PTC in our hospital. Surgical and adjuvant treatment became more conservative, resulting in fewer complications with oncologic outcomes remaining comparable across eras. Despite minor variations in recurrence patterns, long-term survival was comparable across eras. Together, these findings suggest that ATA-guided approaches can be implemented in real-world clinical settings to reduce treatment-related morbidity while maintaining comparable oncologic outcomes. However, given the retrospective design and heterogeneity in follow-up and risk stratification, these findings should be interpreted as supportive evidence rather than definitive proof of the oncologic safety of treatment de-escalation. Prospective, multicenter studies with standardized follow-up are warranted to confirm the oncologic safety of de-escalation strategies, especially in intermediate- and high-risk subgroups.
Authors’ Contributions
J.S.R.: Investigation (equal), methodology (equal), visualization (equal), and writing—original draft (equal). E.J.K.: Investigation (equal), methodology (equal), visualization (equal), and writing—original draft (equal). I.A.L.: Investigation (equal), methodology (equal), visualization (equal), and writing—original draft (equal). D.W.K.: Investigation (supporting) and data collection (supporting). J.A.L.: Investigation (supporting) and data collection (equal). D.H.S.: Investigation (supporting) and data collection (supporting). J.A.P.: Investigation (supporting) and data collection (supporting). S.P.: Data collection (supporting). S.K.: Data collection (supporting). S.W.K.: Data collection (supporting). J.J.J.: Data collection (supporting). K.H.N.: Data collection (supporting). W.Y.C.: Data collection (supporting). Y.S.J.: Conceptualization (equal), data collection (equal), funding acquisition (equal), supervision (equal), and writing—review, and editing (equal). J.L.: Conceptualization (equal), data collection (equal), funding acquisition(equal), supervision (equal), and writing—review and editing (equal).
Footnotes
Acknowledgments
The authors would like to thank Ji Young Kim, Hee Chang Yu, and Cheol Jang for their excellent technical support.
Availability of Data and Materials
The datasets generated during and/or analyzed during this study are available from the corresponding author on request.
Author Disclosure Statement
All authors (J.S.R., E.J.K., I.A.L., D.W.K., J.A.L., D.H.S., J.A.P., S.P., S.K., S.W.K., J.J.J., K.H.N., W.Y.C., Y.S.J., and J.L.) declare that they have no competing interests.
Funding Information
This work was supported by the
Supplemental Material
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.