
Abstract
Background:
After progression on selpercatinib, patients with RET-altered medullary thyroid carcinoma (MTC) face a poor prognosis. Tarlatamab—a Delta-like ligand 3-targeted bispecific T-cell engager—is a promising therapeutic option for patients with MTC, but a prior case series raised safety concerns in this population.
Methods:
A patient with RET-altered MTC who progressed on selpercatinib received tarlatamab using a three-step step-up dosing regimen with modified protocols for monitoring and managing cytokine release syndrome (CRS) and immune effector cell-associated neurotoxicity syndrome (ICANS).
Results:
This patient experienced grade 2 CRS and grade 2 ICANS after cycle 1, day 1. He did not experience any grade ≥3 treatment-related adverse events. The patient had rapid improvement of the disease-associated symptoms. After 8 weeks of treatment, the patient experienced a biochemical and radiographic complete response that is ongoing.
Conclusions:
A modified dosing and monitoring protocol may improve the safety of tarlatamab in patients with MTC while maintaining efficacy. Further research is needed to evaluate the role of tarlatamab in MTC.
Introduction
Medullary thyroid carcinoma (MTC) arises from the parafollicular C-cells of the thyroid gland and represents approximately 2% of thyroid malignancies. 1 However, it is associated with higher rates of recurrent/metastatic disease and accounts for approximately 10% of thyroid cancer deaths. 2 More than 50% of MTCs harbor RET alterations, and these tumors have high response rates to the selective RET inhibitor selpercatinib. 3 For most MTC patients without RET alterations who need systemic therapy, the standard of care remains the multikinase inhibitors (MKIs) vandetanib and cabozantinib.4,5 After progression on these standard therapies, tumors demonstrate diverse mechanisms of acquired resistance, and patients experience poor prognoses.6,7 There are no established treatments for MTC after progression on MKIs or selpercatinib.
Delta-like ligand 3 (DLL3), and inhibitory ligand that suppresses Notch signalling, is highly expressed in advanced MTC, and it is a promising therapeutic target.8–10 Tarlatamab, a DLL3-CD3 bispecific T-cell engager (BiTE), was approved by the U.S. Food and Drug Administration (FDA) for treatment of small cell lung cancer (SCLC) based on studies showing efficacy and an acceptable safety profile.11,12 Tarlatamab showed promising clinical activity in a case series of patients with MTC. 13 However, among the 4 patients in this case series, all 4 patients experienced at least one grade 3 or greater treatment-related adverse event (TRAE), and two patients experienced grade 4 TRAEs, including on patient who died from a colonic perforation attributed to immune effector cell enteritis. These data raise concern about whether the dosing of tarlatamab used for SCLC is safe for patients with MTC. 13 Phase 1 data on obtrixtamig, another DLL3 BiTE, showed three-step step-up dosing achieved similar efficacy with lower rates of cytokine release syndrome (CRS) in patients with SCLC. 14 This dosing approach, with additional monitoring and modified management algorithms, could represent a strategy to administer tarlatamab to patients with MTC to improve safety while maintaining efficacy.
This case report describes the clinical course of a patient with MTC who was treated using a modified dosing and monitoring protocol that was developed by a multidisciplinary team to address the unanticipated toxicities seen in the first case series of patients with MTC who were treated with tarlatamab. 13 The protocol used here is detailed in the Supplement. Key differences between this protocol and the FDA-approved dosing for patients with SCLC include use of a three-step step-up dosing approach, increased clinical and lab monitoring early in the treatment course, longer post-treatment monitoring for CRS and immune effector cell-associated neurotoxicity syndrome (ICANS) during the step-up dosing period, and early use of siltuximab, and IL-6 antagonist, to manage ICANS.15–17
Case Presentation
A 54-year-old male initially presented with several months of progressive pain, malaise, and diarrhea. A computed tomography (CT) scan showed lytic bone lesions, and a biopsy showed metastatic MTC. Baseline molecular testing showed a somatic RET E632_I638 deletion. Pre-treatment calcitonin was 184,978 pg/mL (reference range: <5.0 pg/mL), and carcinoembryonic antigen (CEA) was 255 ng/mL (reference range: <3.7 ng/mL). He was started on selpercatinib, and his symptoms improved within several days. Restaging CT scans showed a decrease in the size of his thyroid mass and diffuse sclerosis of osseous lesions consistent with response to treatment. He underwent an uncomplicated total thyroidectomy 6 months after the initial diagnosis. Pathology from the thyroidectomy showed a 2.1-cm low-grade MTC. After his thyroidectomy, his calcitonin and CEA were 9,774 pg/mL and 25.6 ng/mL, respectively. After 8 months on selpercatinib, the calcitonin and CEA began to increase, and a Cu64-Dotatate PET/CT (DOTATATE PET) scan showed progressive osseous disease. ctDNA drawn after progression showed the following new mutations: KRAS G12D, KRAS G12C, KRAS G12V, KRAS G12S, KRAS G12R, BRCA2 loss, and RB1 loss. He was referred for a second opinion.
On presentation at our clinic, he reported significant, diffuse osseous pain that interfered with his daily activities and led to him taking an indefinite leave of absence from work. His Eastern Clinical Oncology Group performance status was 3. He was not a candidate for clinical trials due to his poor performance status and the absence of measurable disease.The molecular alterations detected after progression on selpercatinib indicated that adding targeted therapies or MKIs was unlikely to overcome the mechanisms of acquired resistance. We tested his original tumor specimen for DLL3 expression by immunohistochemistry, which showed strong staining in 30% of cells and weak staining in the remaining 70% of cells. After extensive discussion of the limited treatment options and shared decision-making, we elected to proceed with off-label tarlatamab. The patient provided written informed consent to proceed with tarlatamab using a modified dosing and monitoring regimen. Because this treatment of a single patient was administered off-label through a compassionate use program, this case report was determined to be exempt from review by the Mass General Brigham Institutional Review Board. The patient provided informed consent to share his case details.
Pre-treatment labs showed a calcitonin of 62,509 (reference range <14.3 pg/mL) and a CEA of 37.2 (reference range = 0.0–3.3 ng/mL). His imaging showed diffuse osseous metastases (Fig. 1). The patient was not able to tolerate prolonged selpercatinib dose holds due to the development of diarrhea, fatigue, and worsening pain within 48 hours of stopping selpercatinib, so we were not able to do a 7-day dose hold prior to cycle 1, day 1 (C1D1), as was done with prior patients. Through shared decision making, we decided to hold selpercatinib for 3 days prior to C1D1 of tarlatamab.
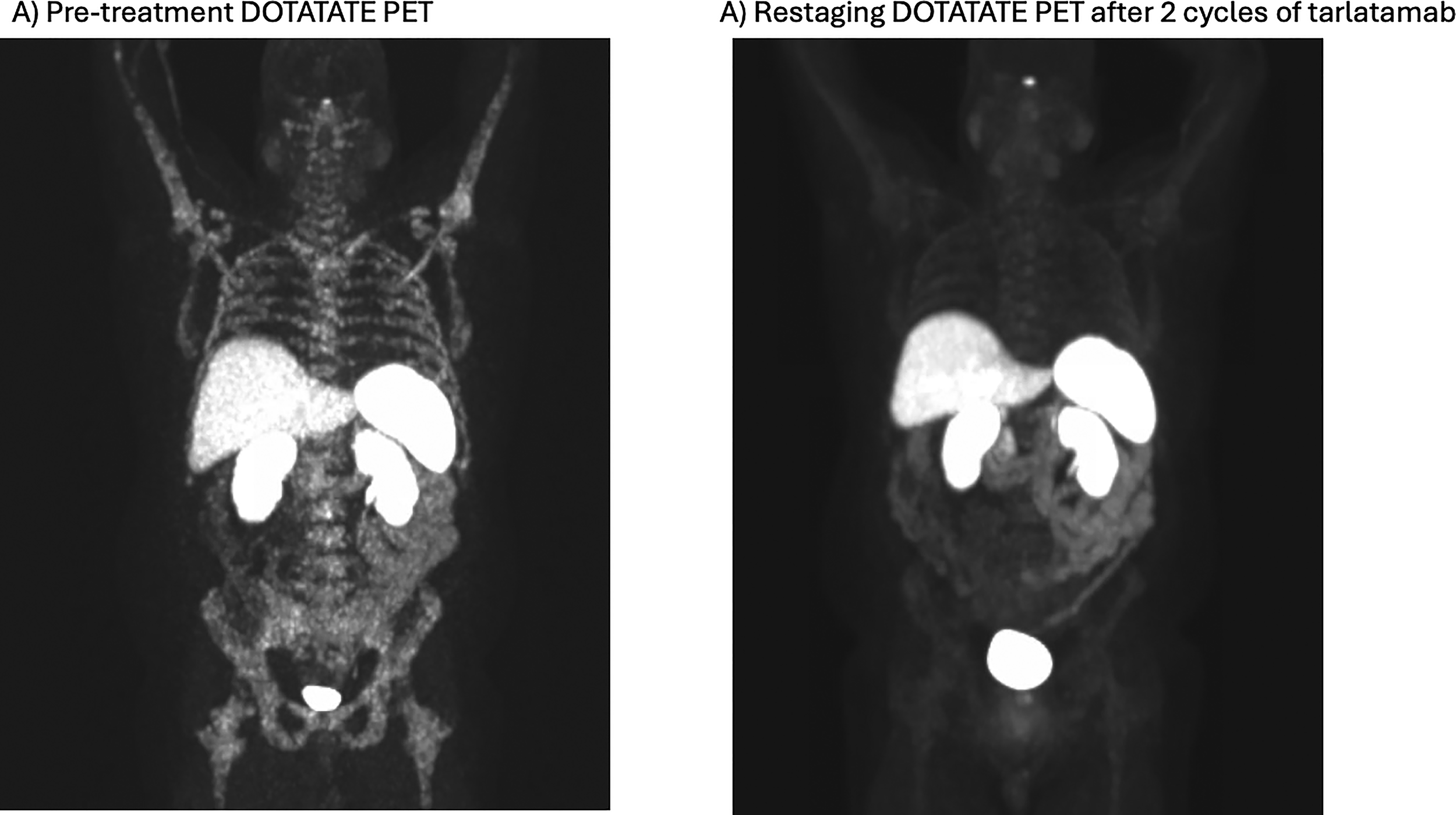
Images from DOTATATE PET prior to treatment initiation and after 2 cycles of treatment. DOTATATE, Cu-64 Dotatate; PET, positron emission tomography.
On C1D1, he received a tarlatamab dose of 0.1 mg with 8 mg of intravenous (IV) dexamethasone as premedication and was admitted to the hospital for 48 hours of monitoring. Lab trends are shown in Figure 2. Baseline labs showed a C-reactive protein (CRP) of 22.1 mg/L (reference range (<8.0 mg/L) and IL-6 of 45.0 pg/mL (reference range <7.1 pg/mL). Seven hours after infusion, he developed a temperature of 38.6 C with a blood pressure (BP) of 84/52 mmHg. His ICE score, a score based on orientation, naming, recall, and attention that is used to assess the severity of ICANS, was 10/10, unchanged from baseline. 15 He received 1 liter of IV normal saline with improvement in his BP. Labs at the time showed a CRP of 51.5 mg/L and an IL-6 of 3,601.0 pg/mL. He received 8 mg IV dexamethasone and 8 mg/kg tocilizumab for grade 2 CRS with no neurotoxicity. On the morning of C1D3, 38 hours after administration of tarlatamab, the patient developed confusion and visual hallucinations. A CT head and electroencephalogram showed no abnormalities. After consultation with neurology, it was felt these hallucinations represented grade 2 ICANS, and he was treated with siltuximab 11 mg/kg. His neurologic symptoms improved over the next 6 hours. He was monitored another 24 hours in the hospital with no recurrence of symptoms. At the time of discharge, the CRP and IL-6 levels were 20.0 mg/L and 5.4 ng/mL, respectively. Due to worsening pain after selpercatinib was held, he resumed selpercatinib, 160 mg twice daily, the day after discharge.
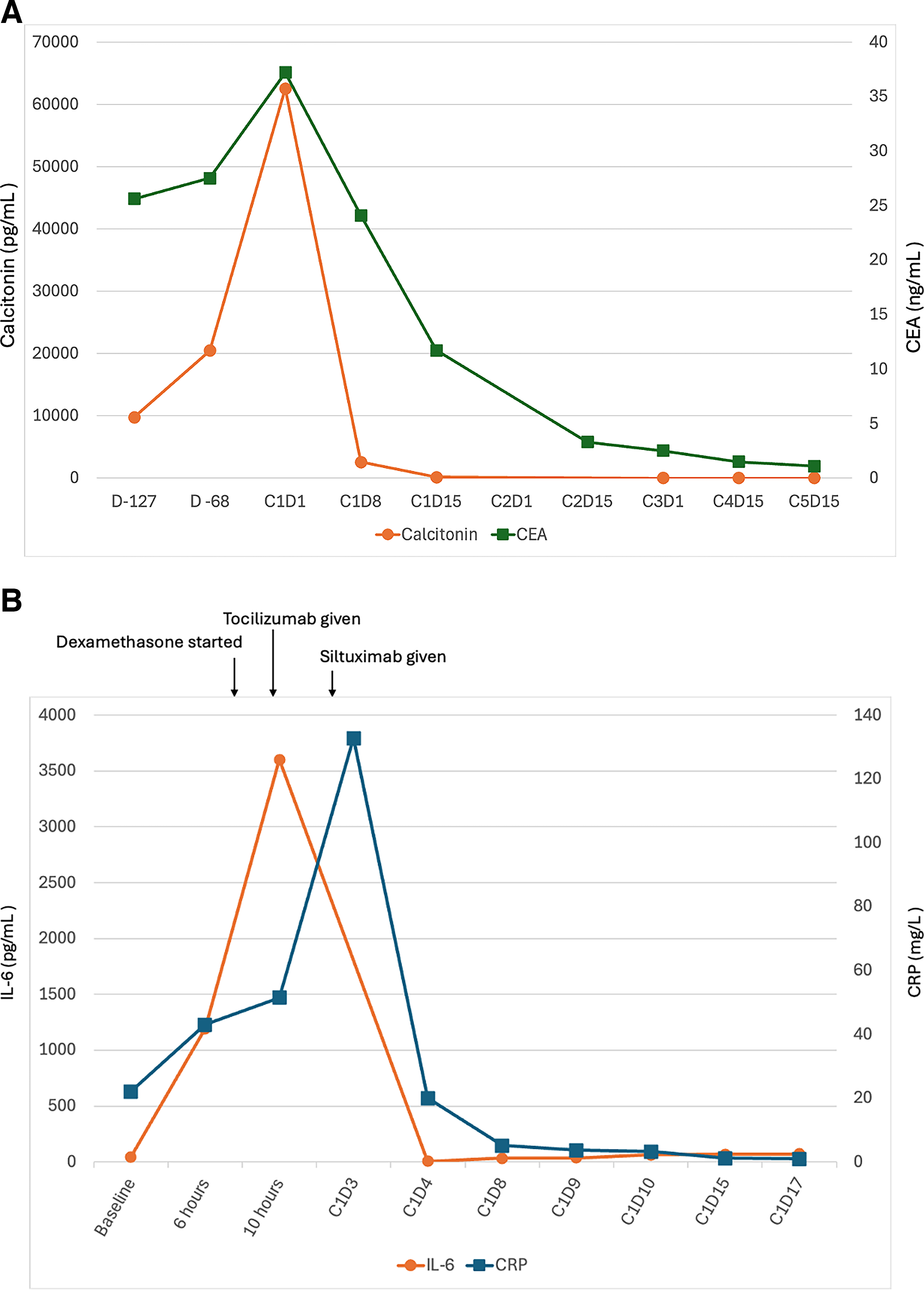
Trends for CEA, calcitonin
On C1D8, he presented to the clinic with a BP of 78/50 mmHg. He reported poor intake over the prior week, and his BP improved with IV fluids. CRP and IL-6 were 5.1 mg/L and 33.3 ng/mL, respectively, prior to administration of the second dose of tarlartamab. He received tarlatamab 1 mg with 8 mg of IV dexamethasone as a premedication and was admitted for 48 hours of monitoring. During this admission, he experienced no CRS or ICANS. CRP peaked at 3.2 mg/L, and IL-6 peaked at 61.9 pg/mL. On C1D15, he received the full 10 mg dose of tarlatamab with 8 mg of IV dexamethasone as a premedication and experienced no clinically significant TRAEs during 36 hours of inpatient monitoring. Beginning on C2D1, he received 10 mg of tarlatamab every 2 weeks with no premedications or admissions for monitoring.
His pain significantly improved within several days of C1D1, and his opioids were discontinued approximately 2 weeks after starting treatment. His fatigue, diarrhea, and appetite loss improved, and he regained 25 pounds between C1D1 and C3D1. His calcitonin and CEA decreased to 132 pg/mL and 11.7 ng/mL on C1D15. On C3D1, calcitonin was less than assay (minimum level of detection = 5.0 pg/mL), and CEA was 2.5 ng/mL. His restaging DOTATATE PET on C3D7 showed minimal uptake in his bones (Fig. 1). At C10D1, the most recent evaluation, his calcitonin remained undetectable, CEA was within normal limits, and imaging showed no evidence of disease.
Discussion
This case describes a patient with RET-altered MTC who had a durable radiographic and biochemical complete response to tarlatamab after progressing on selpercatinib. It is the first case in which a patient with MTC received a three-step step-up dosing tarlatamab regimen with additional monitoring and modified management protocols for CRS and ICANS. While this patient experienced grade 2 CRS and ICANS, the overall safety profile in this patient was improved compared to an earlier cohort of patients with MTC treated with tarlatamab using the SCLC dosing and monitor protocol.11–13 This case report suggests that the dosing and monitoring regimen used here could be a better approach for patients with MTC. However, this single case report does not establish the safety or efficacy or tarlatamab in patients with MTC, and further research, ideally a clinical trial, is required to evaluate the safety and efficacy of this modified tarlatamab regimen in MTC.
Treatment options for patients with MTC after progression on standard therapies, selpercatinib for patients with RET-altered MTC or an MKI for patients with RET wild-type MTC, remain a significant unmet need. Treatment options included in clinical guidelines are based on limited data, and the available data demonstrate limited efficacy with substantial toxicity.18–21 A DLL3 BiTE has the potential to become the standard of care for this patient population if further studies demonstrate safety and efficacy.
The precise mechanisms for the increased toxicity in the initial case series describing the use of tarlatamab in patients with MTC are not certain. However, the incidence of all severe TRAEs in the first 6 weeks of treatment with tarlatamab and good tolerability after the initial two cycles of treatment suggest that the increased toxicity may be due to an exuberant immune response to the initial doses of taralatamab. 13 Potential explanations for stronger immune responses to a DLL3 BiTE in patients with MTC include the lack of prior chemotherapy exposure in most patients with MTC before treatment with tarlatamab, the large volume of metastatic disease seen in the initial cohort of patients with MTC treated with tarlatamab, and the high DLL3 expression in MTC. The data from this case report support these hypotheses by demonstrating an exuberant immune response in a patient who had a large volume of metastatic disease with no prior chemotherapy exposure, and this case report describes how the resulting TRAEs were successfully managed using a modified dosing and management protocol.
This case report, coupled with the prior case series of tarlatamab in MTC, raises the possibility that selpercatinib can be safely combined with tarlatamab, particularly after the first two cycles of tarlatamab, though further investigations are required to assess the safety of this combination. 13 Discontinuation of selpercatinib, even for several days, in patients with RET-altered MTC can be particularly challenging, as many patients experience rapid progression or symptoms with drug holds, so the ability to combine tarlatamab and selpercatinib would expand this treatment option to these patients. Given the timing of severe toxicities and the types of toxicities seen in this case report and the prior case series, it seems unlikely that the increased toxicity seen in patients with MTC is related to the addition of selpercatinib to tarlatamab. 13 Significantly, all severe toxicities in the prior case series occurred before selpercatinib was restarted in patients, and no new toxicities were observed after restarting selpercatinib in this patient.
Conclusions
In a patient with RET-mutant MTC progressing on selpercatinib, tarlatamab administered using a modified dosing and monitoring protocol produced a complete radiographic and biochemical response with an acceptable safety profile. This dosing and monitoring regimen has the potential to become a new option for MTC after progression on selpercatinib, but it requires further research to understand the safety and efficacy in a larger number of patients.
Footnotes
Acknowledgments
The authors thank the patient and his family; the team on Massachusetts General Hospital’s inpatient Ellison 16 ward who cared for this patient during hospital admissions; the finance team who worked with the patient to obtain access to tarlatamab; and Amgen, who provided tarlatamab through their patient assistance program.
Authors’ Contributions
T.J.R.: Conceptualization (lead), data collection, data analysis, writing—original draft (lead); C.B.M.: Conceptualization (supporting), writing—reviewing and editing (equal); A.D.F.: Data collection, writing—reviewing and editing (equal); A.L.: Conceptualization (supporting), writing—reviewing and editing (equal); M.F.: Conceptualization (supporting), writing—reviewing and editing (equal); K.M.H.: Conceptualization (supporting), writing—reviewing and editing (equal); K.R.: Conceptualization (supporting), writing—reviewing and editing (equal); P.M.S.: Data collection, writing—reviewing and editing (equal); L.J.W.: Conceptualization, writing—reviewing and editing (lead).
Author Disclosure Statement
No authors report conflicts of interest directly related to this case report. Outside of this work, the authors report the following disclosures: T.J.R.: Non-executive board director at Biocon Biologics Ltd and receives research funding from Coherus Biosciences. His wife is the CEO of Bicara Therapeutics and a non-executive board director at Relay Therapeutics. They own equity in Bicara Therapeutics, Relay Therapeutics, Biocon Ltd, and Syngene International Ltd. C.B.M.: consulting fees from Genentech, AstraZeneca, and Catalyst Biosciences as well as research funding from Novartis. A.D.F.: No disclosures. Aubrey Lasko: consulting fees from Janssen Pharmaceuticals. M.F.: consulting fees from Sobi Orphan Biovitrum AB, Bristol Myers Squibb, Novartis, Johnson & Johnson, Legend Biotech, Kite Pharma, CytoAgents Inc., Immunofree Inc. K.M.H.: No disclosures. K.R.: Advisory board for SAGA Diagnostics, Regeneron, and Gilead; speaker fees from CME Outfitters, MedScape, Uptodate; research funding from Bristol Myers Squibb. P.M.S.: No disclosures. L.J.W.: Consulting fees Bayer Healthcare, Blueprint Medicines, Eli Lilly, Exelixis, EMD Serono, Illumina, Nested Therapeutics, Ellipses, Novartis, and Merck. She received research support from Eli Lilly, Ellipses, and Novartis.
Funding Information
T.J.R.: Received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. C.B.M.: received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. A.D.F.: received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. A.L.: received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. M.F.: received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. K.R.: received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. P.M.S.: received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. L.J.W.: received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.