
Abstract
Background:
Antiangiogenic and targeted therapies represent the most effective systemic options for advanced thyroid cancers. In this setting, toxicity management is essential to ensure treatment adherence. Among hematological toxicities, erythrocytosis has been rarely investigated, and its clinical pattern and management remain unclear.
Materials and Methods:
We conducted a retrospective cohort study including patients with any advanced thyroid cancer histology treated with antiangiogenic or targeted therapies between 2012 and 2023 at two Italian referral centers. Therapies included RET inhibitors (RETi: selpercatinib, pralsetinib), cabozantinib, the BRAF/MEK inhibitor combination dabrafenib + trametinib, lenvatinib, sorafenib, and vandetanib. Erythrocytosis, defined according to 2022 World Health Organization criteria, was assessed through serial hemoglobin and hematocrit measurements up to 36 months from treatment start. Associations with clinical variables, event-free survival (EFS), overall survival (OS), objective response rate (ORR), disease control rate (DCR), and acute vascular events were assessed using Fisher’s exact and regression models, as appropriate.
Results:
Among 173 screened patients, 135 were included in the final analysis (median follow-up 68.5 months). Erythrocytosis occurred in 24 patients (17.8%), with 16/24 (66.6%) experiencing recurrent events (total: 50). Median time to onset was 1.28 months (Q1–Q3: 0.76–5.14). RETi showed the highest incidence (46.7%), followed by vandetanib (20.7%). Among 14/24 tested patients, no JAK2 V617F or exon 12 alterations were detected. Management involved temporary treatment interruption in 60.0% (30/50) of events, with 53.3% (16/30) resuming at a reduced dose; in selected cases (4/9, 44.4%), hematology-guided phlebotomy was performed without drug discontinuation. Erythrocytosis was not associated with EFS, OS, or ORR, but was associated with higher DCR (p = 0.031). Incidence of acute vascular events was comparable among patients with (8.3%) and without (14.4%) erythrocytosis.
Conclusions:
Erythrocytosis represents an underrecognized, early, recurrent, and indolent adverse event of antiangiogenic and targeted therapies, particularly RETi, in advanced thyroid cancer. Its biological mechanisms and optimal management strategies warrant further investigation.
Introduction
Among the systemic treatment options available for advanced thyroid cancers, antiangiogenic and targeted therapies are the most effective across all histotypes1,2 and have significantly improved patient outcomes over the past decade. 3 Antiangiogenic multikinase inhibitors (primarily vascular endothelial growth factor receptor [VEGFR]-directed) lenvatinib, 4 sorafenib, 5 and cabozantinib 6 are currently approved for radioiodine-refractory (RAI-R) differentiated thyroid carcinoma (DTC), while vandetanib 7 and cabozantinib 8 are approved for medullary thyroid carcinoma (MTC).
Subsequently, more selective inhibitors have emerged. RET inhibitors (RETi, i.e., selpercatinib, pralsetinib) have been studied, with selpercatinib now approved in RET-altered thyroid cancers, including second-line RET fusion-positive DTC 9 and first-line RET-mutant MTC, 10 while pralsetinib has been withdrawn by the European Medicines Agency for commercial reasons, specifically due to a change in the company’s strategy, unrelated to product quality, efficacy, or safety. In BRAFV600E-mutant anaplastic thyroid carcinoma (ATC), the combination of dabrafenib (BRAF inhibitor [BRAFi]) and trametinib (MEK inhibitor [MEKi])11,12 is currently approved by the US Food and Drug Administration, but it remains unavailable in Europe.
Despite these therapeutic advances, the clinical benefit of these agents may be limited by treatment-related adverse events (AEs), which can impair quality of life and compromise treatment adherence.13,14 Among them, hematological AEs are quite uncommon. Clinical trials have provided some data on myelosuppression (e.g., anemia, leukopenia, thrombocytopenia), generally reported at low incidence and grade, especially for agents not approved for advanced thyroid cancer (e.g., sunitinib, pazopanib, vemurafenib). 15 In contrast, information on antiangiogenic and targeted therapy-induced erythrocytosis (or polycythemia) is far more limited and virtually absent in the advanced thyroid cancer setting.16–17 To date, only small case series have described erythrocytosis in other malignancies, including clear cell renal cell carcinoma, melanoma, extra-gastrointestinal stromal tumor, and hepatocellular carcinoma.18–22
Given the increasing use of these therapies in advanced thyroid cancer, there is a need for further investigation of erythrocytosis, to describe its incidence, characteristics, clinical management, and potential impact on acute vascular complications and oncologic outcomes.
Materials and Methods
Study design
We conducted a retrospective cohort study including all advanced thyroid cancer patients (DTC, poorly DTC [PDTC], ATC, MTC) 23 treated with antiangiogenic and targeted therapies between January 2012 and September 2023 at two Italian referral centers: Fondazione IRCCS Istituto Nazionale dei Tumori (INT), Milan, and Istituti Clinici Scientifici Maugeri IRCCS, Pavia.
Patient population
Eligible patients were adults (≥18 years) with advanced thyroid cancer not amenable to loco-regional curative treatments and who received systemic therapy in any treatment line with tyrosine kinase inhibitors (TKIs: cabozantinib, vandetanib, sorafenib, lenvatinib, and/or RETi, i.e., selpercatinib and pralsetinib) or serine-threonine kinase inhibitors (STKIs: BRAFi + MEKi, i.e., dabrafenib + trametinib). All DTC cases were RAI-R. In the event of erythrocytosis, patients were managed according to local clinical practice (i.e., drug discontinuation and/or dose reduction and/or phlebotomy). Patients with a follow-up duration of less than one month were excluded to ensure adequate time to capture the expected peak of drug-induced erythrocytosis. The research was completed in accordance with the Declaration of Helsinki as revised in 2013 and was approved by the Ethical Committee of INT Milan (INT approval no. 151/24). Written informed consent was obtained from all living participants; for deceased patients, the Ethics Committee granted a waiver of consent due to the retrospective nature of the study.
Endpoints
The primary endpoint was erythrocytosis occurrence, defined as the proportion of patients who developed at least one erythrocytosis event.
Erythrocytosis was defined as hemoglobin (Hb) levels >16.5 g/dL in men (and/or hematocrit, Hct >49%) or >16.0 g/dL in women (and/or Hct >48%), according to the World Health Organization (WHO) 2022 guidelines. 24 Multiple erythrocytosis episodes occurring in the same patient during treatment with a single agent were counted as separate events in the analysis. Complete erythrocytosis resolution was defined as Hb and Hct values returning to baseline normal values. For each patient, up to three erythrocytosis events were recorded.
Secondary endpoints included erythrocytosis kinetics (i.e., time to onset), severity (i.e., median Hb and Hct values), dose-dependence, and the association with relevant clinical factors.
Further aims were to describe the clinical management of erythrocytosis and to evaluate the oncologic outcomes assessed by event-free survival (EFS), overall survival (OS), objective response rate (ORR), and disease control rate (DCR). EFS was defined as the time elapsed between the date of treatment start until radiographic disease progression, treatment discontinuation due to unacceptable toxicity, or death by any cause (whichever occurred first). OS was defined as the time elapsed between treatment start and death (by any cause) or last follow-up. Patients without any event and alive at the last follow-up were censored. ORR (i.e., complete response [CR], partial response [PR] vs. stable disease [SD] and progressive disease [PD]) and DCR (i.e., CR, PR, SD vs. PD) were defined according to RECIST 1.1 criteria, 25 based on imaging performed in routine clinical practice.
Statistical methods
Demographic and clinical data were collected from medical records in a centralized anonymized database. Hb and Hct were collected at baseline, at 1 month, at 4 months, and, subsequently, every 4 months up to 36 months from treatment initiation.
Continuous variables were described by median and by first (Q1) and third (Q3) quartile. Categorical variables were described as absolute and relative frequencies. The standardized mean difference (SMD) was used as a measure of between-group differences.26,27
Associations between erythrocytosis events and the most relevant clinical factors (e.g., advanced thyroid cancer histology, sex, age, smoking history, type of antiangiogenic or targeted agent, and chronic obstructive pulmonary disease [COPD]) were assessed using univariable and multivariable logistic models. The multivariable model was designed to estimate pretreatment odds ratio (OR) and included a priori selected covariates: smoking history, COPD, and tumor histotype. Results of logistic models were reported as OR and their confidence interval (CI).
Associations between erythrocytosis and outcomes were assessed using Fisher’s exact tests and univariable and multivariable Cox models. Erythrocytosis was treated as a time-dependent covariate. Multivariable Cox models included the a priori selected covariates: erythrocytosis event (as time-dependent covariate), smoking history, COPD, and tumor histotype. Results of Cox models were reported as hazard ratios (HR) and their CI.
Associations between erythrocytosis and ORR and vascular events were assessed using Fisher’s exact tests.
The difference between time to complete resolution after phlebotomy or medical intervention (i.e., drug discontinuation and/or dose reduction) was assessed by means of a negative binomial generalized linear mixed model with a log link. 28
Dose-event associations were evaluated separately for each drug using a Poisson regression framework with generalized estimating equations29,30 to account for within-patient correlation across repeated observations. The effects were reported as incidence rate ratios (IRRs) with CI.
Median follow-up was calculated using the reverse Kaplan–Meier method. 31 Statistical significance was set at p ≤ 0.05. Analyses were performed using SAS Studio V04.00 (Cary, NC) and R V4.5.1. 32
Further details are reported in the Supplementary Data.
Results
Patient and tumor characteristics
A total of 173 patient records were screened, and 139 met preliminary eligibility and were candidates for analysis. Two records were excluded due to short follow-up (less than 1 month since treatment start) and two for missing data, yielding a final analytic cohort of 135 patients (Supplementary Fig. S1). Median (Q1–Q3) follow-up time was 68.5 months (Q1–Q3: 28.5–97.6). Baseline characteristics are summarized in Table 1, which also reports between-group differences considering patients with versus without erythrocytosis. Half of the patients (51.1%) were female. The median age was 61.0 years (49.2–68.0). Most patients (88.9%) had an Eastern Cooperative Oncology Group (ECOG) performance status of 0–1 and were never-smokers (64.4%). Few patients had a history of COPD (5.2%) or chronic kidney disease (CKD) (1.5%), and a minority were under hormone therapy (3.0%, all in the setting of adjuvant treatment for prior hormone-positive breast cancer), anticoagulants (5.2%), or antiplatelet agents (11.9%). No patients were treated with sodium–glucose cotransporter 2 (SGLT-2) inhibitors. DTC (52.6% in total) was the most prevalent tumor histotype. All patients had stage IV disease and received first-line systemic antiangiogenic or targeted treatment, and all patients were receiving thyroid hormone replacement therapy. Second-line systemic therapies were administered to 37 (27.4%) patients, whereas only 4 (3.0%) received a third-line regimen (Supplementary Table S1).
Demographic, Clinical, and Pathological Characteristics of the Whole Cohort, Overall, and According to Erythrocytosis Event
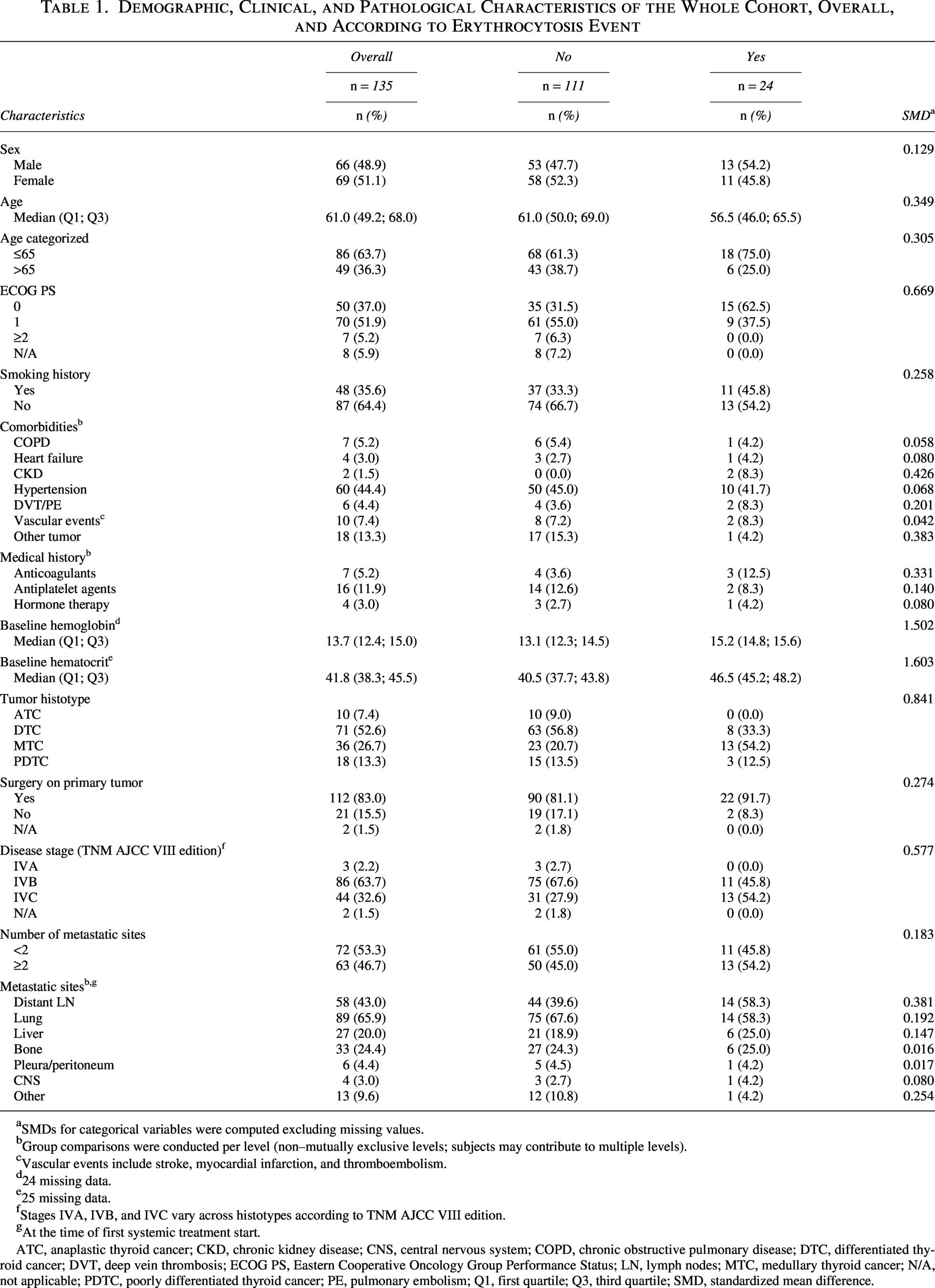
SMDs for categorical variables were computed excluding missing values.
Group comparisons were conducted per level (non–mutually exclusive levels; subjects may contribute to multiple levels).
Vascular events include stroke, myocardial infarction, and thromboembolism.
24 missing data.
25 missing data.
Stages IVA, IVB, and IVC vary across histotypes according to TNM AJCC VIII edition.
At the time of first systemic treatment start.
ATC, anaplastic thyroid cancer; CKD, chronic kidney disease; CNS, central nervous system; COPD, chronic obstructive pulmonary disease; DTC, differentiated thyroid cancer; DVT, deep vein thrombosis; ECOG PS, Eastern Cooperative Oncology Group Performance Status; LN, lymph nodes; MTC, medullary thyroid cancer; N/A, not applicable; PDTC, poorly differentiated thyroid cancer; PE, pulmonary embolism; Q1, first quartile; Q3, third quartile; SMD, standardized mean difference.
Characteristics of erythrocytosis
Twenty-four patients (24/135, 17.8%) developed at least one event, and most of them (16/24, 66.6%) experienced more than one event. Two patients experienced erythrocytosis upon two different drugs: one developed erythrocytosis under cabozantinib and subsequently upon selpercatinib, while the other had a first event on vandetanib and a second event during pralsetinib administration. Overall, 50 erythrocytosis events were recorded.
Out of 15 patients treated with RETi (regardless of treatment line), 7 (46.7%) developed an erythrocytosis episode. Erythrocytosis was also reported in patients receiving treatment with vandetanib (n = 6/29, 20.7%), lenvatinib (n = 11/73, 15.1%), and cabozantinib (n = 2/23, 8.7%). Patients receiving therapy with sorafenib (n = 7) or dabrafenib + trametinib (n = 29) did not develop erythrocytosis (Table 2).
Per-Drug Distribution of Erythrocytosis Events and Affected Patients According to Treatment-Line Exposure
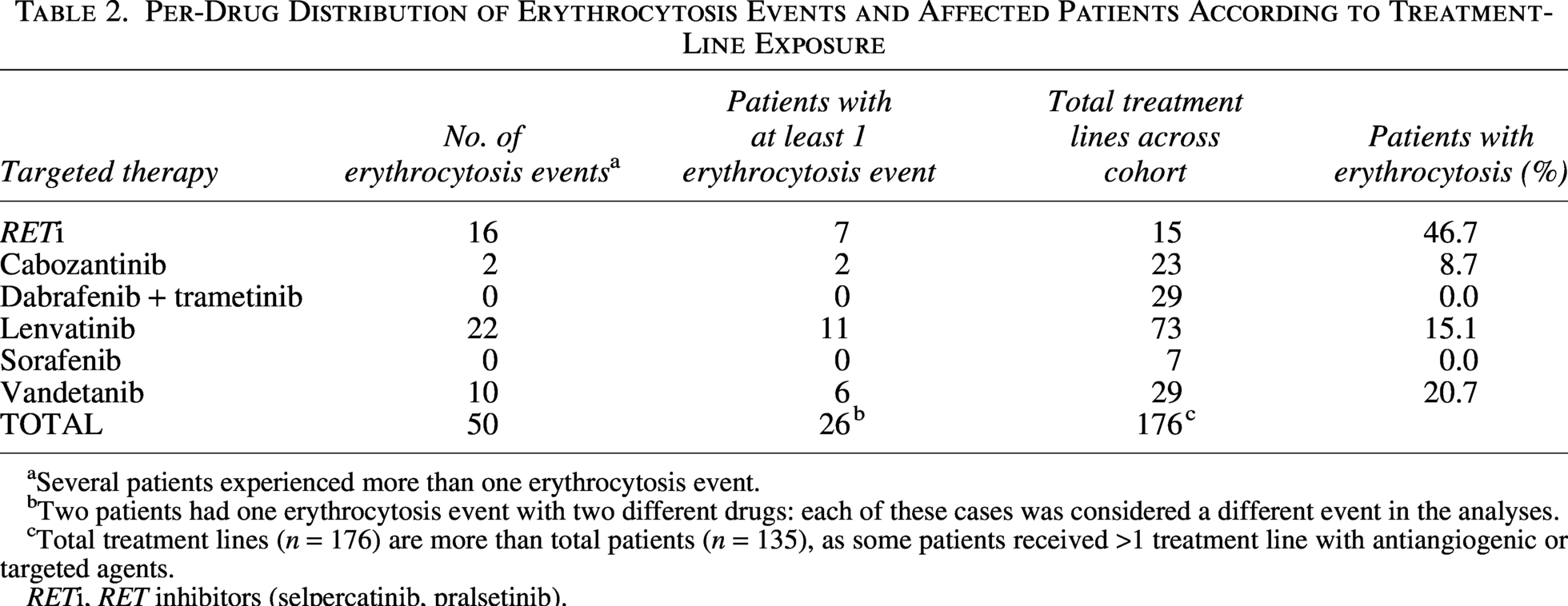
Several patients experienced more than one erythrocytosis event.
Two patients had one erythrocytosis event with two different drugs: each of these cases was considered a different event in the analyses.
Total treatment lines (n = 176) are more than total patients (n = 135), as some patients received >1 treatment line with antiangiogenic or targeted agents.
RETi, RET inhibitors (selpercatinib, pralsetinib).
Among 24 patients who experienced erythrocytosis, 13 had MTC (54.2%), 8 DTC (33.3%), and 3 PDTC (12.5%). No erythrocytosis occurred among the 10 patients with ATC (all treated with dabrafenib + trametinib). Compared with those who did not develop erythrocytosis, patients who did had higher baseline Hb (SMD = 1.5) and Hct (SMD = 1.6) values, although both remained within the normal range, and were more frequently affected by MTC histotype (SMD = 0.8) (Table 1).
The median time (Q1–Q3) to the onset of first erythrocytosis was 1.28 months (0.76–5.14), ranging from 0.76 months with cabozantinib (0.61–0.76) and vandetanib (0.76–0.89) to 2.86 months (1.92–9.70) with lenvatinib. Median time to second and third erythrocytosis episodes was 3.96 months (0.93–11.9) and 6.36 months (5.09–13.7), respectively (Supplementary Table S2).
Hb and Hct distributions at the first, second, and third erythrocytosis episodes are illustrated in Figure 1. No statistically significant dose-event trend was observed for any study drug. RETi showed a borderline-significant inverse trend (IRR: 1.74; CI: 0.95–3.19, p = 0.073), whereas lenvatinib, vandetanib, and cabozantinib showed no evidence of association (Supplementary Table S3A and B).
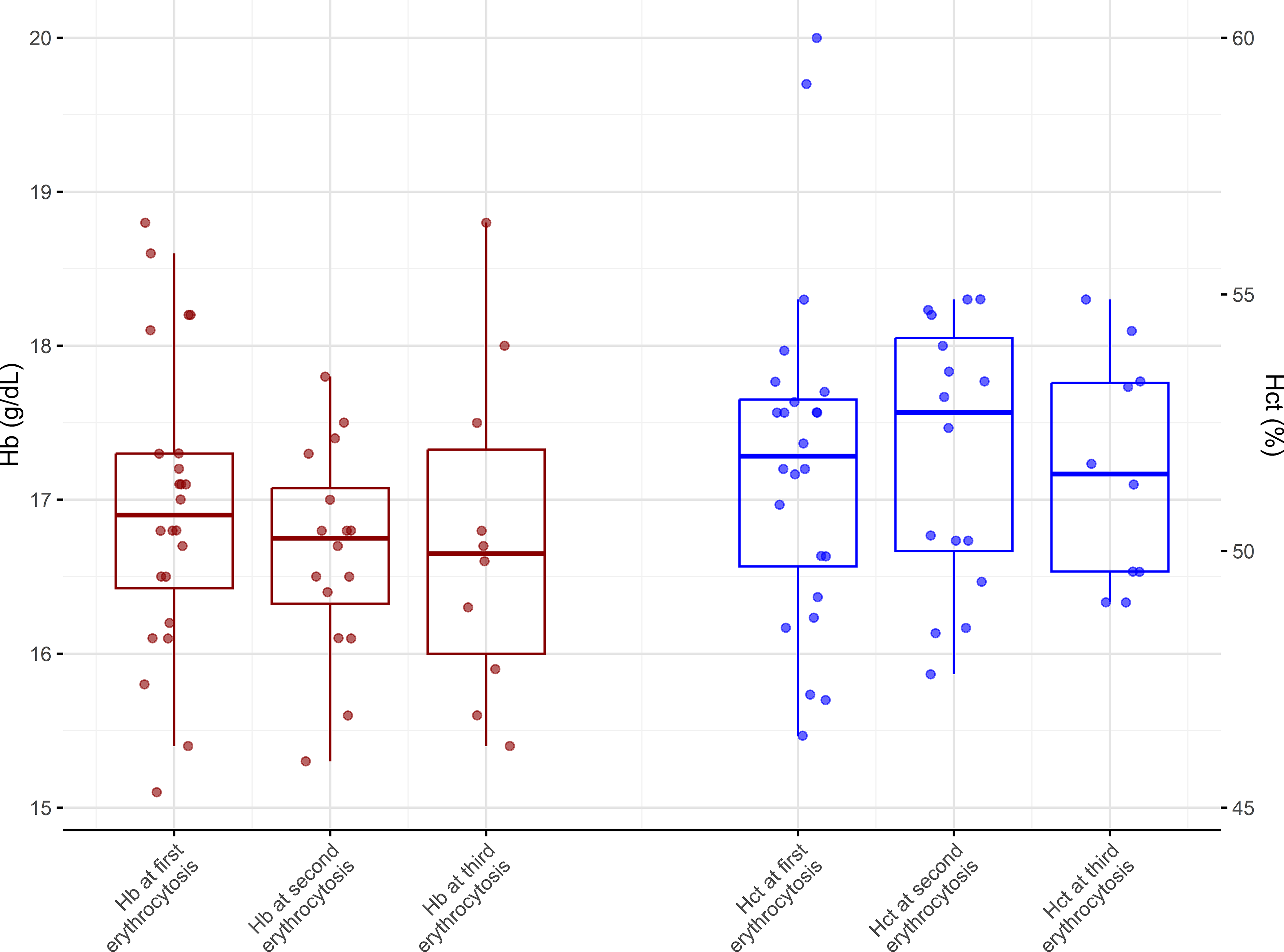
Box plot of Hb and Hct values at erythrocytosis onset in the overall cohort. The figure displays box plots: the central line marks the median, boxes denote the interval between the first (Q1) and third (Q3) quartiles, whiskers extend to 1.5×(Q3–Q1), and points represent individual observations. Hb is plotted in red and Hct in blue. Median Hb and Hct values were comparable across the first, second, and third erythrocytosis episodes, suggesting that the event tends to recur without a gradual increase in severity. Hb, hemoglobin; Hct, hematocrit.
Tumor histology was the only variable significantly associated with erythrocytosis (Table 3): in the multivariable model, patients with MTC had higher odds of erythrocytosis than those with DTC (OR: 4.02; CI: 1.44–11.25; p = 0.028). This association mirrors the close overlap between advanced thyroid cancer histology and the administered treatment (Fisher’s exact test p < 0.001).
Univariable and Multivariable Logistic Models Assessing the Association Between Risk Factors and Erythrocytosis (N = 112) a
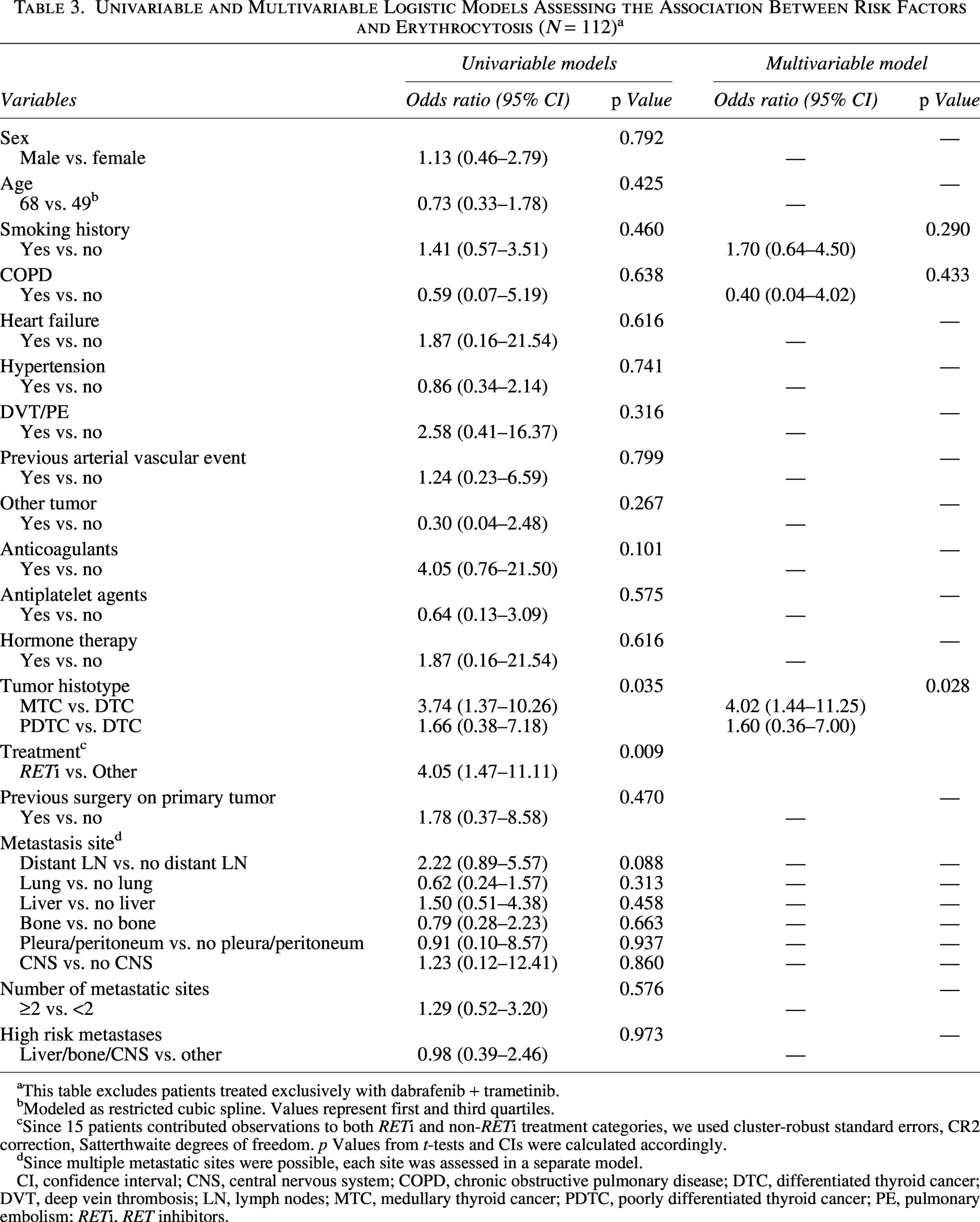
This table excludes patients treated exclusively with dabrafenib + trametinib.
Modeled as restricted cubic spline. Values represent first and third quartiles.
Since 15 patients contributed observations to both RETi and non-RETi treatment categories, we used cluster-robust standard errors, CR2 correction, Satterthwaite degrees of freedom. p Values from t-tests and CIs were calculated accordingly.
Since multiple metastatic sites were possible, each site was assessed in a separate model.
CI, confidence interval; CNS, central nervous system; COPD, chronic obstructive pulmonary disease; DTC, differentiated thyroid cancer; DVT, deep vein thrombosis; LN, lymph nodes; MTC, medullary thyroid cancer; PDTC, poorly differentiated thyroid cancer; PE, pulmonary embolism; RETi, RET inhibitors.
Among the 24 patients who developed erythrocytosis, 14 were evaluated for JAK2 mutations. Among them, no pathological alterations of JAK2 (V617F or exon 12 alterations) were detected.
Patients who did not develop erythrocytosis showed no significant increase in Hb or Hct values over time, regardless of sex and/or treatment line (Supplementary Fig. S2).
Management of TIE events
Treatment was interrupted in 33 of the 50 erythrocytosis events (66%), including 30 temporary and 3 permanent discontinuations. The latter subgroup did not resume therapy due to AEs other than erythrocytosis: G3 hand–foot syndrome, G2 prolonged QTc interval, and G2 proteinuria. In 45% (15/33) of discontinuations, patients were experiencing other concomitant AEs along with erythrocytosis.
At treatment discontinuation, median (Q1–Q3) Hb was 17.1 g/dL (16.4–17.6), while median Hct was 52.3% (49.7–53.9). After interruption, erythrocytosis was completely resolved in 24 out of 33 episodes (72.7%) and remained stable in 3 (9.1%) cases; 6 cases (18.2%) showed an initial improvement without achieving full normalization. The median time to complete erythrocytosis resolution was 14.0 days (7.5–23.5).
Median time (Q1–Q3) to complete resolution was shorter after phlebotomy than after medical intervention (1.0 [1.0–4.0] vs. 16.0 [10.0–27.0] days; n = 4 vs. n = 20), and this difference was supported by the negative binomial mixed model (p = 0.010).
Most patients (30/33) resumed treatment, either with the same (46.7%; n = 14/30) or a reduced dosage (53.3%; n = 16/30). In addition to drug discontinuation, 13 out of 24 patients who experienced erythrocytosis (54.2%) were referred to hematology consultation. After hematologist referral, nine patients were managed by phlebotomy. Among these, treatment was concomitantly discontinued in five cases, whereas four (44.4%) continued without interruption (Supplementary Fig. S3). The median (Q1–Q3) Hb and Hct values at the time of phlebotomy were 17.1 g/dL (16.8–18.5) and 52.3% (51.7–53.2), respectively.
Association of erythrocytosis with disease outcomes
A significantly higher DCR was observed in the presence of erythrocytosis (Fisher’s exact test p = 0.031, Supplementary Table S4A). Responses stratified by specific agents are reported in Supplementary Table S4B.
Erythrocytosis was not significantly associated either with EFS or with OS (Table 4). For EFS, none of the covariates reached statistical significance. For OS, only PDTC histology remained associated with a worse outcome in the multivariable model (PDTC vs. DTC: 2.40, CI: 1.21–4.74; p = 0.037).
Univariable and Multivariable Cox Models for Event-Free Survival and Overall Survival
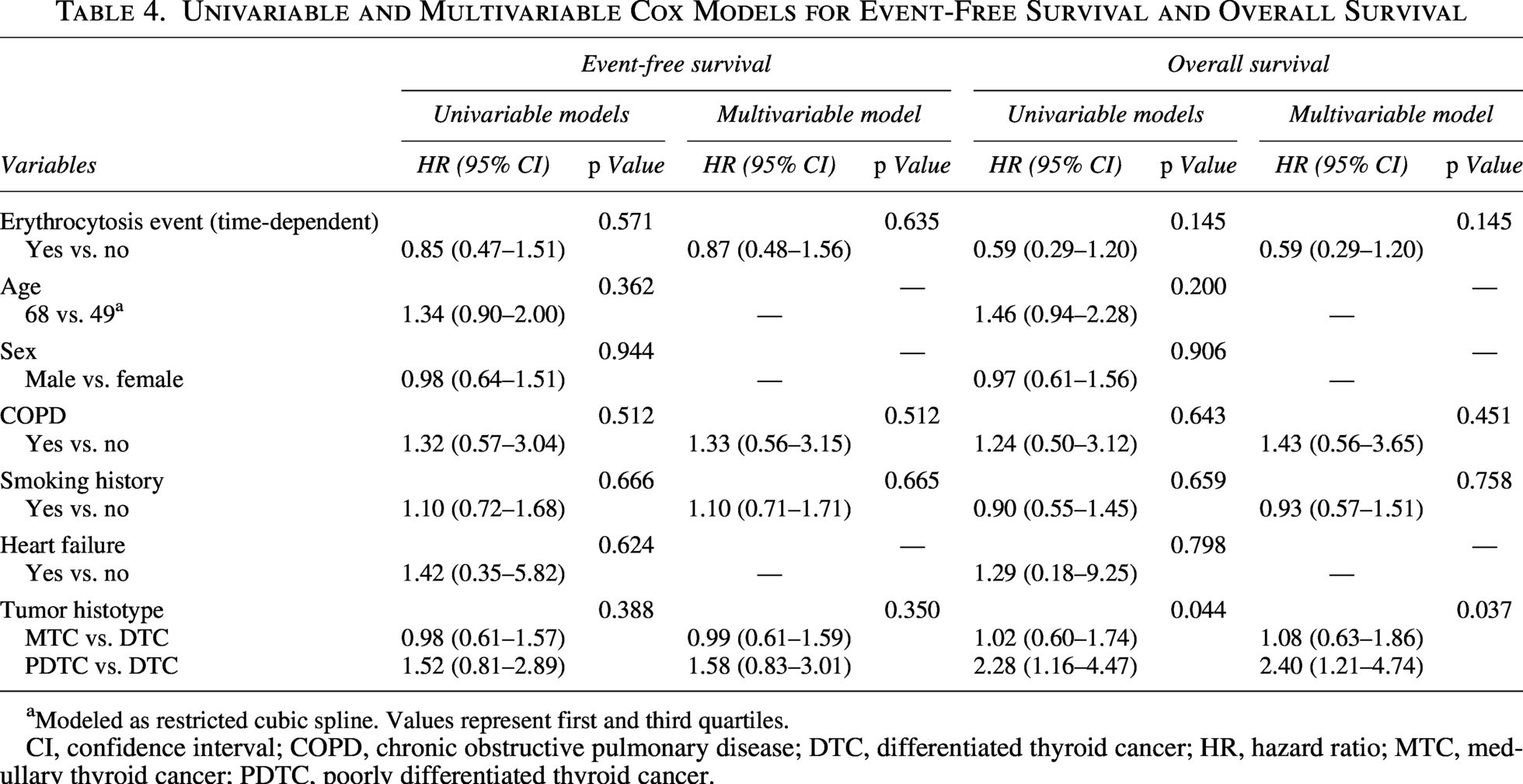
Modeled as restricted cubic spline. Values represent first and third quartiles.
CI, confidence interval; COPD, chronic obstructive pulmonary disease; DTC, differentiated thyroid cancer; HR, hazard ratio; MTC, medullary thyroid cancer; PDTC, poorly differentiated thyroid cancer.
Erythrocytosis was not associated with an increased incidence of acute vascular events, which occurred in 8.3% of patients (2/24, both on lenvatinib) compared with 14.4% (16/111) recorded in patients without erythrocytosis (p = 0.740). Specifically, one patient developed acute deep venous thrombosis during an erythrocytosis episode, while the other experienced an acute myocardial infarction that was not concomitant to erythrocytosis.
Discussion
To the best of our knowledge, this study is the first to comprehensively assess the incidence, clinical pattern, and management of erythrocytosis in advanced thyroid cancer across all histologies and all key available therapeutic agents. A recent systematic review by Liu et al. highlighted drug-induced erythrocytosis, particularly with testosterone, VEGF inhibitors (with antiangiogenic TKIs showing erythrocytosis in up to 43.5% of cancer patients), and SGLT-2 inhibitors. 33 While erythrocytosis has been reported with antiangiogenic agents in other malignancies,18–22 only two case reports have described this AE in thyroid cancer (both in MTC patients treated with vandetanib16,17). Indeed, erythrocytosis remains an underreported side effect in both clinical trials and real-world practice, lacking a specific definition in CTCAE v5.0, 34 which prompted us to adopt the 2022 WHO criteria 24 for its identification and grading.
Our findings showed that erythrocytosis is not rare: approximately one in five patients (17.8%) treated with antiangiogenic or targeted therapies developed it during a median follow-up of 68.5 months. It typically showed an early onset, generally within one to three months, in line with published reports.18–21 More than two-thirds (66.6%) of patients experienced recurrent episodes, without increasing severity (i.e., similar median Hb/Hct values at the first, second, and third event, as shown in Fig. 1). Importantly, erythrocytosis was not associated with an increased risk of acute vascular complications, supporting its indolent behavior. Indeed, permanent discontinuations were uncommon, and, when occurring, they were driven by other, concomitant severe toxicities.
No statistically significant association emerged between dose level and erythrocytosis incidence for any study drug. Unlike other dose-dependent toxicities, such as hypertension or proteinuria, erythrocytosis seems to behave as an on/off phenomenon: patients either develop it or not, regardless of dose intensity, exposure, and clinical features and in the absence of a gradual rise in Hb/Hct in unaffected patients. Notably, in the RETi subgroup, the dose-event analysis showed a borderline-significant inverse pattern, with erythrocytosis appearing numerically more frequent at higher dose-reduction levels (i.e., lower dose intensity). Because this pattern is biologically implausible, it is more likely to reflect treatment dynamics and time-dependent confounding than a true dose effect, as patients managed with dose reductions may represent a more closely monitored, longer-exposed subgroup already enriched for erythrocytosis risk.
Our cohort was predominantly under 65 years, with ECOG performance status of 0–1, non-smokers, and with a low prevalence of COPD or CKD. All baseline Hb and Hct values were within the normal range. JAK2 mutations were absent in the evaluated subset (14/24), excluding an underlying myeloproliferative disorder. In most cases (72.7%), erythrocytosis completely resolved rapidly after treatment interruption (median: 14 days). Taken together, these findings support a genuinely drug-induced origin of erythrocytosis rather than one secondary to other causes.
No erythrocytosis events were observed with dabrafenib + trametinib, consistent with their serine-threonine kinase inhibition on different targets (BRAF, MEK) unrelated to angiogenesis and the VEGF pathway, suggesting that dysregulation of VEGF signaling may represent the central driver of erythrocytosis development. Notably, no cases were observed with sorafenib despite its VEGF-directed activity, most likely due to small sample size, as erythrocytosis with sorafenib has been reported in other malignancies. 18
VEGFR-2 is a key regulator of tumor angiogenesis and is highly expressed in advanced thyroid cancer. 35 Although the precise mechanism of erythrocytosis remains incompletely understood, both erythropoietin (EPO)-dependent and -independent pathways are likely involved. The more established EPO-dependent hypothesis proposes that vascular endothelial growth factor receptor-2 (VEGFR-2) inhibition triggers a rebound upregulation of renal EPO synthesis, resulting in increased erythrocytosis 36 ; however, transient surges may normalize by the time erythrocytosis becomes clinically evident, 37 making the timing of EPO measurement critical.
By contrast, EPO-independent pathways are less well characterized, but several hypotheses can be advanced. First, VEGFR-2 is expressed on hematopoietic progenitors and contributes to erythroid regulation 38 ; moreover, repression of VEGFR-2 by GATA1 has been shown to promote erythroid differentiation. 39 In this context, VEGFR-2 inhibition could lower the threshold for EPO receptor activation, enhancing red cell production via JAK2/STAT5 and PI3K/MAPK signaling even with normal serum EPO concentrations. 40 In addition, VEGF itself has been shown to modulate hepatic EPO synthesis, 41 while VEGFR blockade may induce subtle renal hypoxia or microvascular alterations enhancing local EPO transcription. 42 Moreover, experimental models demonstrated continuous EPO production by renal and tumor cells, 43 suggesting a microenvironment-dependent process.
The higher prevalence of erythrocytosis with selective RETi (46.7% vs. overall 17.8%) may reflect our limited sample size; however, stronger RET inhibition combined with residual VEGFR activity could also produce additive or synergistic disruption of erythropoietic regulation. 10 Moreover, RET blockade may indirectly interact with VEGFR inhibition, further amplifying erythropoietic signaling, 44 while the RET receptor itself has been implicated in renal erythropoietic regulation. 45 Finally, RETi may modulate MAPK/PI3K pathways overlapping with EPO receptor signaling, thereby generating an “EPO-like” proliferative signal even in the absence of elevated circulating EPO. 46
It is possible that the observed higher incidence of erythrocytosis in MTC patients could be entirely attributable to RETi, which was more commonly associated with secondary erythrocytosis, or to additional biological factors intrinsic to MTC.
Erythrocytosis has been described in pheochromocytoma and is thought to be mediated by activation of hypoxia-inducible factor (HIF) pathways, including germline mutations in genes, such as PHD1 and PHD2, leading to increased EPO production and secondary polycythemia.47,48 Similarly, HIF-1α expression has been reported in MTC tumors (55.9% of cases) and has been associated with worse prognosis. 49
In addition, pancreatic neuroendocrine tumors have been reported to rarely secrete EPO, resulting in paraneoplastic erythrocytosis.50–52 A single case report described ectopic EPO production by MTC, leading to secondary polycythemia. 53
As we did not investigate EPO levels, HIF-1 tumor expression, or related signaling pathways in our study, we cannot determine whether the higher incidence of erythrocytosis in MTC patients was exclusively attributable to RETi exposure or whether it also involved tumor-related biological mechanisms.
In line with prior studies linking hypertension to better clinical outcomes, 54 we observed higher disease control in the presence of erythrocytosis. This finding, although speculative in the absence of prospective data, underscores the importance of recognizing and managing erythrocytosis appropriately to avoid unnecessary drug discontinuation. 15
Management practices evolved during the study period. Interventions were generally prompted at Hb ≥17 g/dL and/or Hct ≥52%, including drug continuation, temporary suspension and resumption with or without dose reduction, and/or phlebotomy. These thresholds for intervention are consistent with those reported in case series, although, unlike previous reports,16,17 we did not routinely use antiplatelet agents (i.e., aspirin).
Although definitive conclusions cannot be drawn from our findings, we propose some practical suggestions for erythrocytosis management. First, baseline EPO levels should be measured in patients with advanced thyroid cancer who are initiating antiangiogenic or targeted therapy. Patients with higher baseline Hb and Hct values, even within the normal range, should be monitored more closely. Moreover, patients who develop erythrocytosis should be referred for hematological consultation, and a repeat EPO measurement together with JAK2 mutational analysis should be performed. Finally, clinicians should carefully balance the risks and benefits of drug suspension in cases of isolated erythrocytosis, particularly in light of our data showing no increased risk of vascular complications. In our cohort, treatment discontinuation or phlebotomy was generally undertaken at a threshold of Hb ≥17 g/dL and/or Hct ≥52. This suggests that, while taking interlaboratory variability into account, erythrocytosis below this range can often be safely managed without interrupting therapy, especially if asymptomatic and if not accompanied by other clinically significant AEs. Complete resolution was achieved significantly faster with phlebotomy than with treatment suspension and/or dose reduction alone (median time to complete resolution: 1 vs. 16 days, respectively). However, given that phlebotomy is more invasive and requires dedicated hospital infrastructure and logistical support, the choice of management should remain individualized according to patient preference, local resource availability, and the overall clinical context. We also propose that erythrocytosis be formally included among hematological adverse effects and classified within the CTCAE framework.
Several limitations must be acknowledged. First, the retrospective design with an extended timespan inherently introduces selection bias and heterogeneity, limiting causal inference. Moreover, histotypes were described according to the older WHO 2022 classification, 23 as the 2025 update 1 (which also includes differentiated high-grade thyroid carcinoma) was published after the completion of our analyses. In addition, our study did not include patients treated with antiangiogenic and targeted therapies in combination with immune checkpoint inhibitors, a regimen now approved in selected advanced thyroid cancer histologies (i.e., lenvatinib + pembrolizumab in ATC). This may be relevant as immunotherapy could influence angiogenesis and erythropoiesis through vascular normalization mechanisms 55 and cytokine-mediated cross-talk with erythroid progenitors,56,57 potentially modulating the erythropoietic effects observed with VEGF-pathway inhibition. Also, biological characterization was partial: JAK2 status was available only for a subset, and data on EPO levels were not collected. Furthermore, potential drug–drug interactions were not evaluated systematically; data on concomitant radiotherapy were not collected, with a potential bias in patients with long disease histories and oligo-progression. Bone-directed radiotherapy, in particular, may induce cytopenia followed by marrow stimulation, either dampening or contributing to erythrocytosis. These gaps highlight the need for prospective studies designed with integrated biological assessments to clarify mechanisms, explore pharmacologic interactions, and establish evidence-based management strategies.
In conclusion, erythrocytosis is a common yet often underrecognized adverse effect of targeted agents with antiangiogenic properties. It is important for clinicians to recognize and appropriately manage this AE to prevent unnecessary drug discontinuation, optimizing treatment adherence and patient outcomes.
Authors’ Contributions
S.M.: Conceptualization (lead), investigation (lead), data curation (lead), writing—original draft (lead), and visualization (supporting). A.S.: Conceptualization (supporting), investigation (supporting), and data curation (supporting). R.R.: Writing—original draft (supporting), writing—review and editing (equal), and supervision (supporting). F.B.: Formal analysis (lead), resources (supporting), writing—original draft (supporting), and visualization (supporting). S.B.: Data curation (supporting). M.D.M.: Data curation (supporting). C.S.: Data curation (supporting). S.D.: Data curation (supporting). L.M.: Data curation (supporting). I.N.: Data curation (supporting). C.B.: Data curation (supporting). S.C.: Data curation (supporting). E.C.: Data curation (supporting). A.O.: Data curation (supporting). M.S.: Data curation (supporting). B.P.: Data curation (supporting). A.G.: Data curation (supporting). M.C.: Data curation (supporting). R.M.: Writing—review and editing (supporting) and supervision (supporting). L.L.: Writing—review and editing (supporting) and supervision (supporting). L.D.L.: Writing—review and editing (supporting) and supervision (supporting). S.A.: Conceptualization (lead), methodology (lead), investigation (lead), data curation (lead), writing—original draft (equal), writing—review and editing (equal), and supervision (lead). All authors provided final approval of the article for publication and agreed to be accountable for all aspects of the work.
Author Disclosure Statement
S.C.: Declares occasional fees for participation as a speaker at conferences/congresses from AccMed; support for attending meetings and/or travel from AccMed, MultiMed Engineers srl, and Care Insight sas. L.L.: Reports institutional grants and personal fees from AstraZeneca, Bristol Myers Squibb, Boehringer Ingelheim, Debiopharm International SA, Eisai, Novartis, and Roche; institutional grants from Celgene International, Exelixis, Hoffmann-La Roche, IRX Therapeutics, Medpace, Merck Serono, and Pfizer; and personal fees from Sobi, Ipsen, Incyte Biosciences Italy SRL, Doxa Pharma, Amgen, Nanobiotics SA, GSK, AccMed, Medical Science Foundation G. Lorenzini, Associazione Sinapsi, Think 2 IT, Aiom Servizi, Prime Oncology, WMA Congress Education, Fasi, DueCi Promotion SRL, MI&T, Net Congress & Education, PRMA Consulting, Kura Oncology, Health & Life SRL, and Immuno-Oncology Hub. L.D.L.: Received conference honoraria/advisory board fees from Lilly, MSD, EISAI, Roche, Bayer, Merck Serono, Istituto Gentili Srl, New Bridge. Remaining authors declare no conflicts of interest.
Footnotes
Acknowledgments
We acknowledge Dr. Zyanya Lucia Zatarain-Barrón (
Funding Information
This work was partially funded with Ricerca Corrente funds, Italian Ministry of Health.
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.