
Abstract
Background:
Resistance to thyroid hormone alpha (RTHα) is a rare genetic disorder with symptoms of hypothyroidism, but normal or close-to-normal thyroid function tests. Treatment with levothyroxine (L-T4) may be beneficial. This study investigated the efficacy, safety and biochemical changes of high-dose L-T4 and liothyronine (L-T3) treatment.
Methods:
Four RTHα (Ala263Val) patients were treated with L-T4 (1.75 µg/kg) in a pilot open-label study and monitored for three years. Quality of life (QoL) was assessed using ThyPro. Analysis of auxiological- and biochemical-parameters, bone mineral density (BMD) and exploratory metabolomics was performed. A partial replacement of L-T4 with L-T3 was attempted.
Results:
Treatment with L-T4 increased FT4, FT3, and rT3 to supraphysiological concentrations (relative to reference intervals) and suppressed thyroid-stimulating hormone with no adverse effects. Heart rate, bone markers, and sex hormone-binding globulin transiently increased. Several classes of lipids were reduced. BMD appeared unaltered. Patients reported improved QoL. One patient presented a short non-sustained ventricular tachycardia on L-T3 + L-T4.
Conclusions:
L-T4 treatment of adult RTHα patients was safe and improved QoL in adherent patients.
Introduction
Thyroid hormones (THs) are endocrine hormones that exert effects on almost all tissues, with critical physiological roles during development, including normal cognitive functions, and maintenance of metabolism. 1
THs mediate their effect primarily by binding to TH receptors (TR), encoded by two distinct genes: THRA and THRB that encode the alpha (TRα) and beta (TRβ) receptors, respectively. 2 TRα is the predominant TR in most tissues, including skeletal muscles, the heart, intestines, bone, and most parts of the brain. Loss-of-function variants in THRA cause the disease Resistance to thyroid hormone alpha (RTHα; Orphanet #566231). 3 RTHα patients show symptoms of hypothyroidism that include delayed cognitive development/reduced intellectual abilities, anemia, poor linear growth, a broad face and usually constipation (see reviews4–6). However, the hypothalamic–pituitary–thyroid (HPT) axis is unaffected, making RTHα difficult to diagnose biochemically because patients have normal or close-to-normal thyroid-stimulating hormone (TSH) and free thyroxin (FT4) concentrations. In contrast, RTHβ patients have elevated FT4 and nonsuppressed TSH. 7
RTHα patients generally have heterozygous mutations in THRA; however, a homozygous case was recently reported. 8 RTHα-causing TRα variants result in a receptor with reduced sensitivity to triiodothyronine (T3, active TH): in the presence of normal TH concentrations, TRα fails to recruit co-activators and turn on gene expression, acting instead as a repressor. Several mutations cause partial resistance to T3, in that gene expression is activated by supraphysiological T3 concentrations, at least in vitro.9,10 Treatment with levothyroxine (L-T4) appears to be beneficial for RTHα patients, especially if initiated at a young age. 6 There are few reports on treatment with L-T4 in adulthood and liothyronine (L-T3) therapy has not been tested in this patient group.
We previously reported the first Norwegian RTHα patients, all first-degree relatives with the TRα variant Ala263Val that was reported to cause partial resistance.10,11 This study aimed to investigate efficacy and safety of treatment with high doses of L-T4 and L-T3 in RTHα patients when initiated in adulthood, and secondarily to investigate biochemical and metabolomic changes.
Materials and Methods
A detailed Materials and Methods section is provided in the Supplementary Data.
Study design and patients
This prospective open-label observational cohort study was a pilot study and the result of the clinical treatment of four RTHα (THRA c.788C > T, p.Ala263Val) patients: a father (age 64) and three children (daughters age 19 and 26, son age 25). All had typical symptoms of RTHα and were overweight with main symptoms of tiredness, lack of energy, and constipation. A detailed baseline description of the patients was previously reported and is summarized in Supplementary Table S1. 11
Decisions on treatment doses (Fig. 1A) and monitoring were done by a team of endocrinologists at Oslo University Hospital (OUS), based on previously reported cases by Moran et al. 10 and communication with international experts.
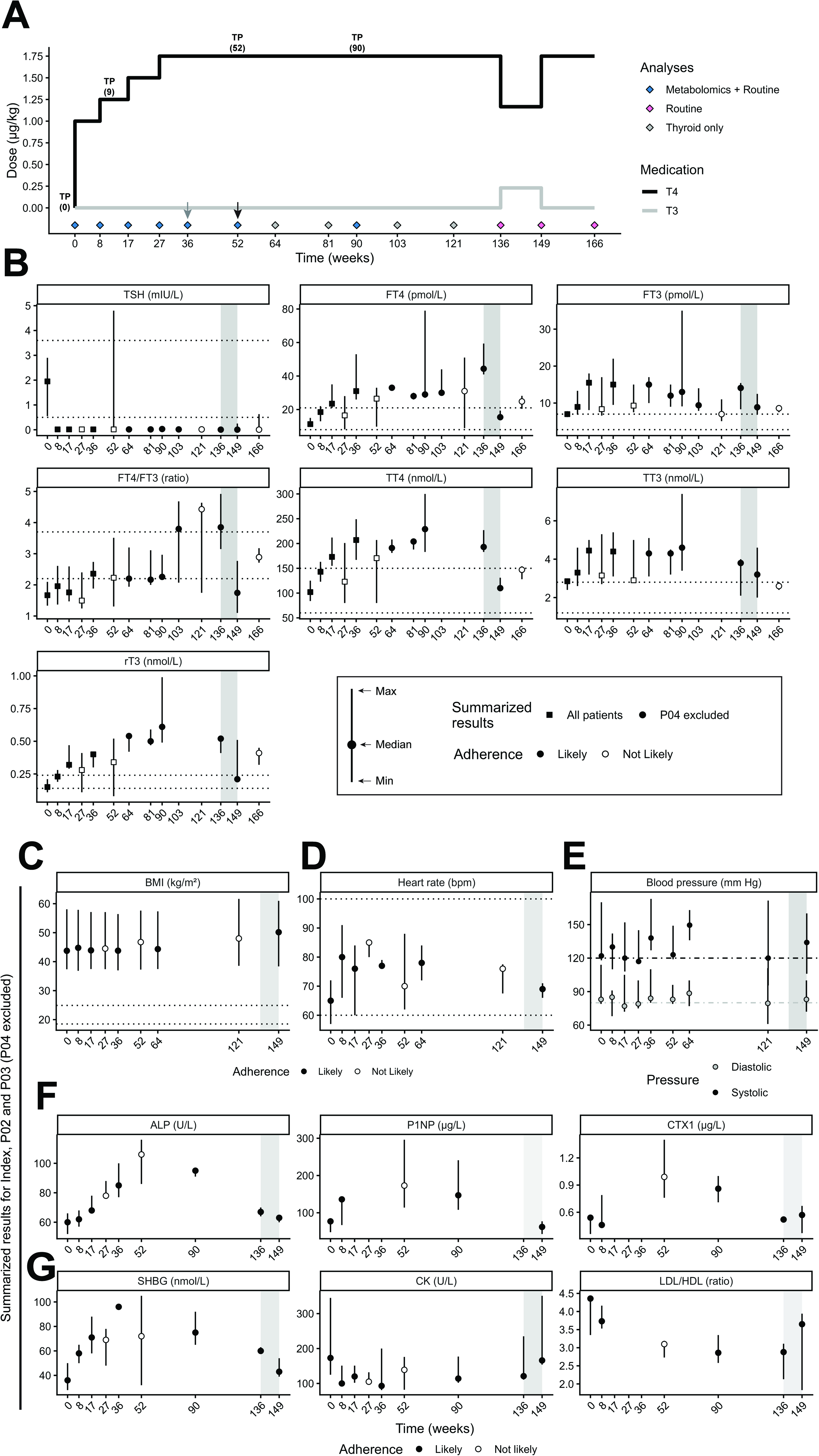
Summary of treatment, thyroid function tests, auxiological and biochemical results.
Ethics and data protection approval
This study was approved by the Regional Committee for Medical and Health Research Ethics South East Norway (ID: 26678). All patients provided written informed consent prior to inclusion.
Statistical methods and interpretation
Data analysis was based on descriptive statistics and interpretations of patterns, that is, assessment of results by the authors. No formal statistical testing was performed, except for the exploratory metabolomic analyses (see SI).
Results
Thyroid-hormone parameter responses
TSH and FT4 were within the reference intervals (RIs), and both FT3 and TT3 were high-normal at baseline (Fig. 1B, week 0). Patients were obese or morbidly obese (Fig. 1C). L-T4 treatment generally suppressed TSH and increased free and total TH concentrations (Fig. 1B and Supplementary Fig. S1). However, adherence-issues (see below) complicated the interpretation of the effect of the treatment. Stepwise increases from 1.0 µg/kg to 1.75 µg/kg L-T4 (Fig. 1A) gradually increased FT4 and FT3, TT4, TT3, and rT3 (Figs. 1B and Supplementary Fig. S1). The FT4/FT3-ratio, low at baseline compared with controls, 11 increased following treatment (Fig. 1B and Supplementary Fig. S1). FT4 remained relatively stable for the subsequent year (week 36–90) while on 1.75 µg/kg for the two “fully adherent” patients P02 and P03 (Fig. 1B and Supplementary Fig. S1). In contrast, rT3 gradually increased and FT3 gently decreased during this period (Fig. 1B and Supplementary Fig. S1).
Medication adherence issues
Two patients (Index and P04) self-reported issues with treatment adherence, partly due to forgetting to take the prescribed medication and the fasting requirement. This was confirmed by test results at several timepoints (e.g., week 27; Fig. 1B and Supplementary Fig. S1). P04 stopped taking medication completely after week 52 for reasons not related to the drug treatment (reason not disclosed). FT4 normalized to pre-treatment levels by week 64, while TSH fluctuated in the following months (Supplementary Fig. S1). P04 was therefore not included in the summarized results (Figs. 1C–1G and 2B).
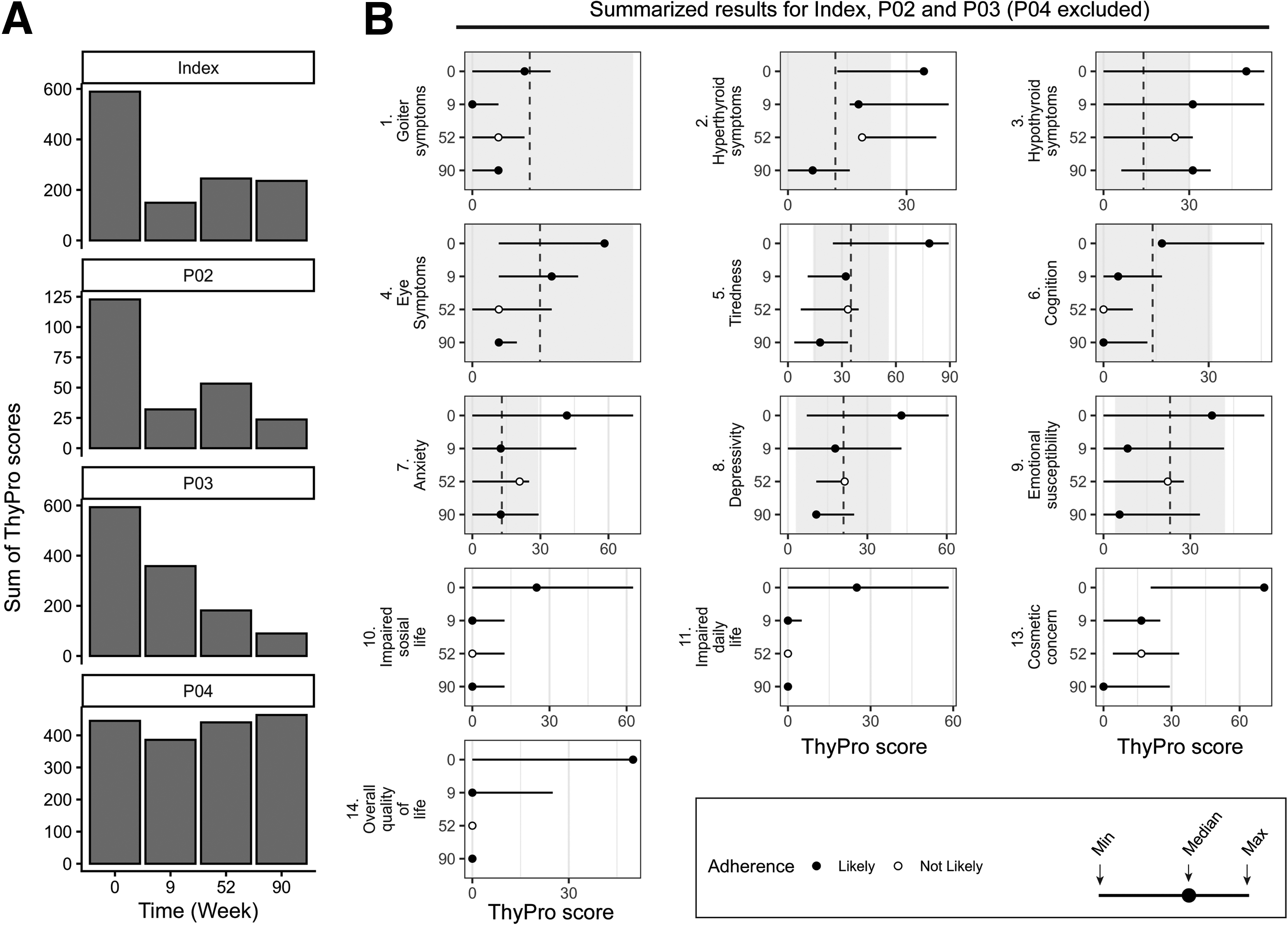
ThyPro quality of life questionnaire results. Scores for the self-reported quality of life (QoL) questionnaire ThyPro.
The Index patient’s TH concentrations fluctuated markedly, likely due to adherence issues (Supplementary Fig. S1).
Transiently changed heart rate and bone markers
There was minimal change in body mass index (BMI) during the entire treatment (Fig. 1C and Supplementary Fig. S3A). Heart rate increased transiently following L-T4 initiation for all patients but remained within normal limits (Fig. 1D and Supplementary Fig. S3A). Blood pressure was generally high-normal or elevated without a consistent temporal pattern (Fig. 1E and Supplementary Fig. S3A).
Markers of bone formation (Procollagen type 1 N; P1NP) and resorption (C-terminal telopeptide of Type I Collagen; CTX1) and alkaline phosphatase transiently increased after L-T4 initiation, peaking around week 52 and subsequently declining (Fig. 1F, Supplementary Fig. S4A); however, bone mineral density scans indicated no major change (Supplementary Fig. S3B).
The known TH-responsive markers sex hormone-binding globulin (SHBG) and creatine kinase (CK) were also transiently changed (Fig. 1G, Supplementary Fig. S4B and S4C). Cholesterol levels improved following treatment: the ratio of low-density lipoprotein cholesterol (LDL) to high-density lipoprotein cholesterol (HDL) decreased to below 3.5:1 and stayed low until at least week 136 (Fig. 1G and Supplementary Fig. S4E). Additional biochemical markers are shown in Supplementary Fig S4.
Exploratory metabolomics indicated that many circulatory lipids were altered following the L-T4 treatment
Effects on plasma metabolomes were investigated using exploratory analysis. Principal component analysis (PCA) did not show any clear clustering by time, treatment, or adherence (Supplementary Fig. S5A). Thirty-nine metabolites (all lipids) correlated negatively with FT4 concentration (Supplementary Table S2). A machine learning model (partial least squares, PLS) trained on weeks 0–36 predicted the general trend in FT4 concentration (e.g., low or high FT4) for the “unseen” timepoints 52 and 90, most notable for the Index patient (Supplementary Fig. S5B). However, the errors in the predictions were very large (Supplementary Fig. S5C). The important metabolites for the PLS model were mainly lipids, including hexosyl-ceramides and triglycerides (Supplementary Fig. S5C).
L-T3 + L-T4 combination therapy was stopped following ventricular tachycardia
Our group has clinical experience with L-T4 and L-T3 combination therapy and L-T3 monotherapy for patients with residual hypothyroid symptoms on L-T4 monotherapy. 12 We hypothesized that combination therapy would further improve symptoms and included L-T3 from week 136 (0.23 µg/kg; Fig. 1A). Combination therapy was discontinued week 149 because the index-patient presented with heart palpitation and Holter registration showed a short episode of nonsustained ventricular tachycardia (data not available). All patients were then restored to L-T4 monotherapy.
While on combination treatment, FT4 and TT4 fell to within the RIs for the three adherent patients and rT3 was reduced to within the RI for two of the three patients (week 149, Fig. 1B). SHBG decreased while CK increased (Fig. 1G, Supplementary Fig. S2B and S2C).
QoL improvements
ThyPro was used to monitor patient-reported outcomes at four timepoints (Fig. 1A). At baseline, P02 (father) scored on average markedly better than the other patients and within or below the expected reference population (mean score ± standard deviation [SD]) (Fig. 2A, B and Supplementary Fig. S6). The three (partially) adherent patients reported overall subjective improvement following treatment (Fig. 2A) and several ThyPro-scales appeared improved, including Tiredness, Cognition, Impaired social-, Impaired daily- and Overall QoL (Fig. 2B and Supplementary Fig. S6). P03 also reported improvements in anxiety and depression (Supplementary Fig. S6).
In contrast, the non-adherent P04 reported overall no marked change in the sum of symptoms (Supplementary Fig S2A), but increased symptoms of both hyper- and hypothyroidism at later timepoints (Supplementary Fig. S6).
Discussion
Four adult first-degree related RTHα patients were treated with THs at doses resulting in elevated FT4, FT3, and rT3, and suppressed TSH and monitored closely for up to 166 weeks (∼3 years; Fig. 1A and B). To the best of our knowledge, this is the first study to report systematic and detailed long-term monitoring, QoL and metabolomic changes of adult RTHα patients treated with L-T4 (and L-T3). In contrast, the three RTHα patients (mother and her two sons; Ala263Val) reported by Moran et al. (2014) received TH treatment from a young age (2–3 years old). 10 Another patient, a boy (Ala263Val) with mild pubertal delay initiated L-T4 treatment at age 17 years. 13 Patients with other TRα-variants have also been reported to receive L-T4.9,13–20
No adverse effects, in particular an increase in heart rate or blood pressure, were observed while on L-T4 treatment. However, during treatment with L-T3 (0.23 µg/kg) in combination with L-T4, one episode of nonsustained ventricular tachycardia was observed. Combination treatment was promptly stopped and the patients returned to L-T4 monotherapy. No other instances of arrhythmia occurred during the follow-up period. Heart rates, which were low prior to treatment, were transiently increased by L-T4 while blood pressure was not affected (Fig. 1D and E). The absence of tachycardia while on L-T4 monotherapy, despite high levels of FT4 and FT3 (Fig. 1B,D, Supplementary Fig.S1 and S3A), is consistent with reports that RTHα, at least the Ala263Val-variant, appears to protect or offer a resistance to TH-induced tachycardia.10,13,21
QoL was improved by L-T4 for the three (fully or partially) adherent patients Index, P02, and P03, especially symptoms related to hypothyroidism, tiredness, anxiety, and social relations (Fig. 2A and B). Improvements following treatment have also been reported for patients with the Ala263Ser variant. 16
The LDL/HDL cholesterol ratio was improved (reduced) following treatment (Fig. 1G), an effect likely mediated by the liver and TRβ. 22 Furthermore, exploratory metabolomics indicated that many circulating lipid classes were reduced by L-T4 (Supplementary Table S2), consistent with the known lipid-lowering effects of THs. 23
TRα is the predominant receptor in bone. RTHα patients (including ours 11 ) often have mild to moderate skeletal alterations and L-T4 treatment of young RTHα patients improved bone development.6,24 Bone-turnover markers transiently changed, but no marked changes in bone density were observed following treatment of our patients (Fig. 1F and Supplementary Fig. S3B).
Treatment did not affect BMI (Fig. 1C). This may indicate that while the dose resulted in supraphysiological FT4 and FT3 concentrations relative to normal reference ranges, it may not have resulted in sufficiently supraphysiological levels in the end organs of the RTHα patients to fully activate TRα and facilitate increased metabolism and weight loss, despite the positive effects on QoL (Fig. 2) and effects on SHBG, CK, and LDL/HDL (Fig. 1G). It is possible that a higher dose of L-T4 is needed to restore normal TRα-activity in tissues. We note that rT3 continued to increase and FT3 decreased slightly while on a constant L-T4 dose (Fig. 1B and Supplementary Fig. S1), possibly indicating reduced conversion of T4 to T3 over time despite constant FT4.
Our study has several limitations: this was a pilot, observational study of only four RTHα patients, all first-degree relatives. Two of the patients had reduced adherence to the medication. The interpretations of biochemical and QoL results are exploratory in nature and based on our interpretations of differences and trends, not a priori hypotheses or formal statistical testing. Because many markers were monitored and interpreted, this may have led to “Type I” errors (false positives). The exploratory metabolomics results should be considered hypothesis-generating rather than firm conclusions. This warrants caution when generalizing our findings to other RTHα patients and thyroid hormone-related metabolism as a whole.
RTHα patients appear to benefit from treatment. Future research should focus on both early diagnostics and improved treatment strategies. Increased awareness of RTHα among primary care physicians and interdisciplinary follow-up is important to improve adherence to treatment. The ideal treatment of RTHα most likely involves a compound that selectively activates TRα, but to the best of our knowledge, none is currently available. 25 In contrast, there are several compounds selective for TRβ including the recently FDA-approved TRβ agonist resmetirom. 26
To summarize, RTHα is a rare genetic disorder, but likely underdiagnosed, and patients generally have several symptoms that retrospectively can be associated to hypothyroidism. If suspected, genetic testing should be offered to patients with characteristic features of RTHα with normal TSH and FT4. Phenotype-severity is associated with the specific variant, but clinical presentation is highly variable, even for patients with the same variant. Our study showed that L-T4 treatment at high doses initiated at adulthood was safe, improved QoL and improved the lipid-profile. L-T3 should be used with caution.
Authors’ Contributions
A.W.: Data curation (lead); Software (lead); Formal analysis (lead); Visualization (lead); Writing—Original Draft (lead); Writing—Review and editing (equal). L.D.: Conceptualization (lead); Methodology (lead); Investigation (lead); Project administration (equal). M.B.: Conceptualization (supporting); Resources (equal); Writing—Review and editing (equal). P.T.: Resources (equal); Supervision (supporting); Conceptualization (supporting). S.H.: Supervision (lead); Project administration (equal); Resources (equal); Writing—Review and editing (equal).
Data Availability
The data that support the findings of this study are not openly available due to reasons of sensitivity but can be made available from the corresponding author upon reasonable request. The data is located in controlled-access data storage at OUS.
Author Disclosure Statements
A.W., L.D., and M.B.: Declare no competing interest. P.T.: Has received grants from Sanofi and Ferring Pharmaceuticals not related to this study. S.H.: Is a member of an advisory board for Amgen, not being related to this study.
Footnotes
Acknowledgments
The authors would like to thank the patients who participated in the study and consented to the publication of results. They also thank Nina Gjerlaugsen and Ranveig Østrem for help with biobanking and Betty Ann Bjerkreim for assistance with the LIMS.
Funding Information
A.W., L.D., M.B., and P.T.: No funding to declare. S.H.: Supported this study with a grant from the Norwegian patient organization for thyroid disease (“
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.