
Abstract
Background:
Thyroid dysfunction has been associated with adverse postoperative outcomes, but little is known about its effects on patients undergoing coronary artery bypass grafting (CABG). Here, our goals were (1) to evaluate the incidence of CABG in patients with hypothyroidism receiving thyroid hormone replacement therapy, and (2) to assess short-term and long-term outcomes in patients with hypothyroidism undergoing CABG compared with controls without thyroid disease, and (3) to determine whether abnormal preoperative thyroid-stimulating hormone (TSH) levels modify postoperative surgical risk in this patient population.
Methods:
Retrospective longitudinal study using the TriNetX Global Collaborative Network database. The incidence of CABG was evaluated in about 1.23 million patients with hypothyroidism during a 20-year observation period (median of 4.4 ± 5.9). Post-CABG outcomes, including mortality, cardiovascular events, and postsurgical complications, were evaluated in 6557 patients with hypothyroidism over 10 years after 1:1 propensity score-matching.
Results:
Over 20 years, patients with a diagnosis of hypothyroidism had a higher incidence of CABG compared with controls (0.27% vs. 0.22%; hazard ratio [HR] 1.08; confidence interval [CI]: 1.03–1.14). Among patients who underwent CABG, the diagnosis of hypothyroidism was associated with mild increased risk of short-term postsurgical infections (HR:1.10, CI:1.01–1.20), CABG-specific complications (HR: 1.24, CI: 1.08–1.42), and critical care utilization (HR:1.14, CI:1.07–1.21). During long-term follow-up, these patients were at increased risk of incident heart failure (HR:1.15, CI:1.04–1.28), stroke (HR:1.18, CI:1.01–1.39), and major adverse cardiovascular events (MACE) (HR:1.15, CI:1.01–1.29). Sensitivity analysis, including only patients with hypothyroidism diagnosis, showed that abnormal preoperative TSH levels, particularly those with elevated TSH, had a higher risk of short-term mortality and long-term embolic events.
Conclusions:
Hypothyroidism is associated with a higher incidence of coronary disease requiring CABG and increased risks of postoperative complications, heart failure, stroke, and MACE. These findings support the potential value of preoperative thyroid function assessment and optimization to mitigate postoperative complications and improve surgical outcomes in this high-risk group.
Introduction
Hypothyroidism is a chronic endocrine disorder characterized by decreased levels of circulating thyroid hormones, which reduces thyroid hormone signaling throughout the body. 1 Early diagnosis is generally made through the compensatory elevation in thyroid-stimulating hormone (TSH) and reduction in free thyroxine (FT4) levels. In the United States, the prevalence of hypothyroidism is about 5%, while globally it ranges between 0.2% and 11.0% in the general population, 2 with higher rates in iodine-deficient regions and in older female adults. 3 Although levothyroxine (LT4) hormone replacement therapy is effective, hypothyroidism is associated with various comorbidities, in particular cardiovascular disease.4,5 Patients with hypothyroidism often experience elevated low-density lipoprotein cholesterol despite higher utilization of statins,6,7 diastolic hypertension, arterial stiffness, endothelial dysfunction, and altered myocardial contractility.4,5,8,9
Recent studies suggest that patients with hypothyroidism undergoing surgery are at higher risk of postoperative complications such as infections, cardiovascular adverse events, and hospital readmissions.10,11 Moreover, in various settings, abnormal TSH levels before hospitalization have been linked to worse hospital outcomes, including prolonged hospital stays and readmission, 12 as well as increased postoperative mortality.13,14 Nonetheless, in some settings, abnormal TSH levels have not been deemed sufficient to delay a cardiac surgery, 15 while others recommend preemptive adjustment of the LT4 dose. 16
Coronary artery bypass grafting (CABG) is a high-risk surgical procedure that restores adequate blood flow to the myocardium in select patients with severe coronary artery disease (CAD).17,18 Although thyroid hormones play a critical role in cardiovascular function, influencing myocardial contractility and systemic vascular resistance, limited research has examined the impact of hypothyroidism on outcomes following CABG.19–23 This question is particularly relevant given that patients with hypothyroidism exhibit an increased risk of cardio-renal-metabolic dysfunctions.9,24,25
Existing studies suggest that patients with hypothyroidism undergoing CABG may have increased rates of postoperative complications, require inotropic support, and prolonged mechanical ventilation,20,22 as well as an elevated risk of postoperative atrial fibrillation 19 and higher 30-day mortality among women. 23 However, these findings have not been consistently observed,20,21 and most available studies have been limited by small sample sizes, single-center designs, and short follow-up durations, restricting the generalizability and robustness of their conclusions.19,21–23 Moreover, long-term risk assessment has been explored in only a single study to date. 20
The present study used a large, multicenter, real-world dataset from the TriNetX network to (1) investigate the incidence of CABG among patients with hypothyroidism, (2) evaluate the short-term and long-term risks of adverse outcomes in patients with hypothyroidism undergoing CABG, and (3) determine whether abnormal preoperative TSH levels modify postoperative surgical risk in this patient population.
Material and Methods
Study I—Incidence of CABG in patients with hypothyroidism
This was a secondary analysis of a previously described cohort. 26 Briefly, we compared the incidence of new CABG procedures among patients with hypothyroidism on replacement therapy compared with controls without thyroid disorders over a 20-year follow-up period (Supplementary Table S1 for International Classification of Diseases, Tenth Revision [ICD-10] and Current Procedural Terminology [CPT] codes). The cohort of patients with hypothyroidism included patients diagnosed with hypothyroidism (ICD-10: E03.9, E03.8; ICD-9: 244.8, 244) at least two times in their record who had been undergoing hormone replacement therapy (LT4, liothyronine [LT3], or desiccated thyroid extract [DTE]) after the diagnosis. Given that hypothyroidism is a chronic condition requiring lifelong management, thyroid hormone replacement therapy was assumed to be ongoing throughout the follow-up period. Exclusion criteria: diagnosis of iodine-deficiency related thyroid disorders (ICD-10 E01), hyperthyroidism (ICD-10 E05), thyroid malignancies (ICD-10 C73), or prescription of methimazole or propylthiouracil. A subsample restricted to patients with a documented TSH level ≥7.00 mU/L within 6 months on or before the first hypothyroidism diagnosis was designed to conduct a subgroup analysis. The control cohort consisted of patients presenting for general examinations without new complaints, suspected, or reported diagnoses (ICD-10 Z00), reflecting routine primary care visits. Patients were excluded if they presented with a diagnosis of hypothyroidism (ICD-10 E03.9 or E03.8), hyperthyroidism, or iodine-deficiency related thyroid disorders. Other exclusion criteria were prescription of methimazole, propylthiouracil, or thyroid hormone therapy, as well as TSH levels out of the normal range (≤0.45 or ≥ 4.50 mIU/L). Cohort assignment was hierarchical: patients who met criteria for the hypothyroidism cohort at any point in their medical record were assigned exclusively to that cohort. Eligibility for the control cohort required that no hypothyroidism cohort criteria were met at any time, with no temporal restriction applied. No patient appeared in both cohorts. This approach ensured that controls remained free of any thyroid disorder or TSH abnormality throughout the entire study period. The index events were the first recorded diagnosis of hypothyroidism for cohort with hypothyroidism and the first qualifying primary care visit for controls, occurring between January 1, 2004, and January 1, 2024, among patients aged 18 years or older at that time. We then applied 1:1 propensity score matching (PSM) based on age, sex, race, hypertension, diabetes, dyslipidemia, obesity, and hospitalization history to ensure comparability between cohorts. The outcome was the incidence of CABG, assessed from 1 to 20 years after their first hypothyroidism diagnosis or primary care visit.
Study II—Adverse outcomes following CABG in patients with hypothyroidism
Study design
This retrospective cohort study leveraged a live dataset from TriNetX (Cambridge, MA, USA), a global federated research network with real-time access to de-identified electronic health records. Patient deidentification is conducted at the network level and certified by a qualified expert in accordance with the Health Insurance Portability and Accountability Act (HIPAA) Privacy Rule. Patient counts fewer than 10 are obfuscated to protect anonymity. Reporting followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for cohort studies. All studies were exempt from informed consent (University of Texas Medical Branch Institutional Review Board #20-0085) and were completed in accordance with the Declaration of Helsinki as revised in 2013.
Participants
A real-time search and analysis of the Global Collaborative Network database [167,337,420 patients and 148 health care organizations (HCO)] was conducted in June 2025. The sample consisted of patients aged 18 years or older who underwent CABG between June 1, 2005, and June 1, 2024. Patients were excluded if they had a history of organ transplantation, cancer, prior aortocoronary bypass grafting, severe or end-stage chronic kidney disease (CKD), previous heart or pericardial surgery, or thyroid disorders related to iodine deficiency diagnosed at least 1 day before CABG. Use of antithyroid medications (methimazole or propylthiouracil) at any time before or on the day of surgery was also an exclusion criterion. The eligible patients with a hypothyroidism diagnosis (ICD-10: E03.8, E03.9, E06.3), undergoing hormone replacement therapy (LT4, LT3, and/or DTE) any time before the CABG, were included in the cohort with hypothyroidism). In control cohort, patients with any disorder of the thyroid (ICD-10: E00-E07, E89) or those who were taking LT4 and/or LT3, or DTE at any time before or after the CABG procedure were excluded (Fig. 1). The index event for these cohorts was the first occurrence of CABG.
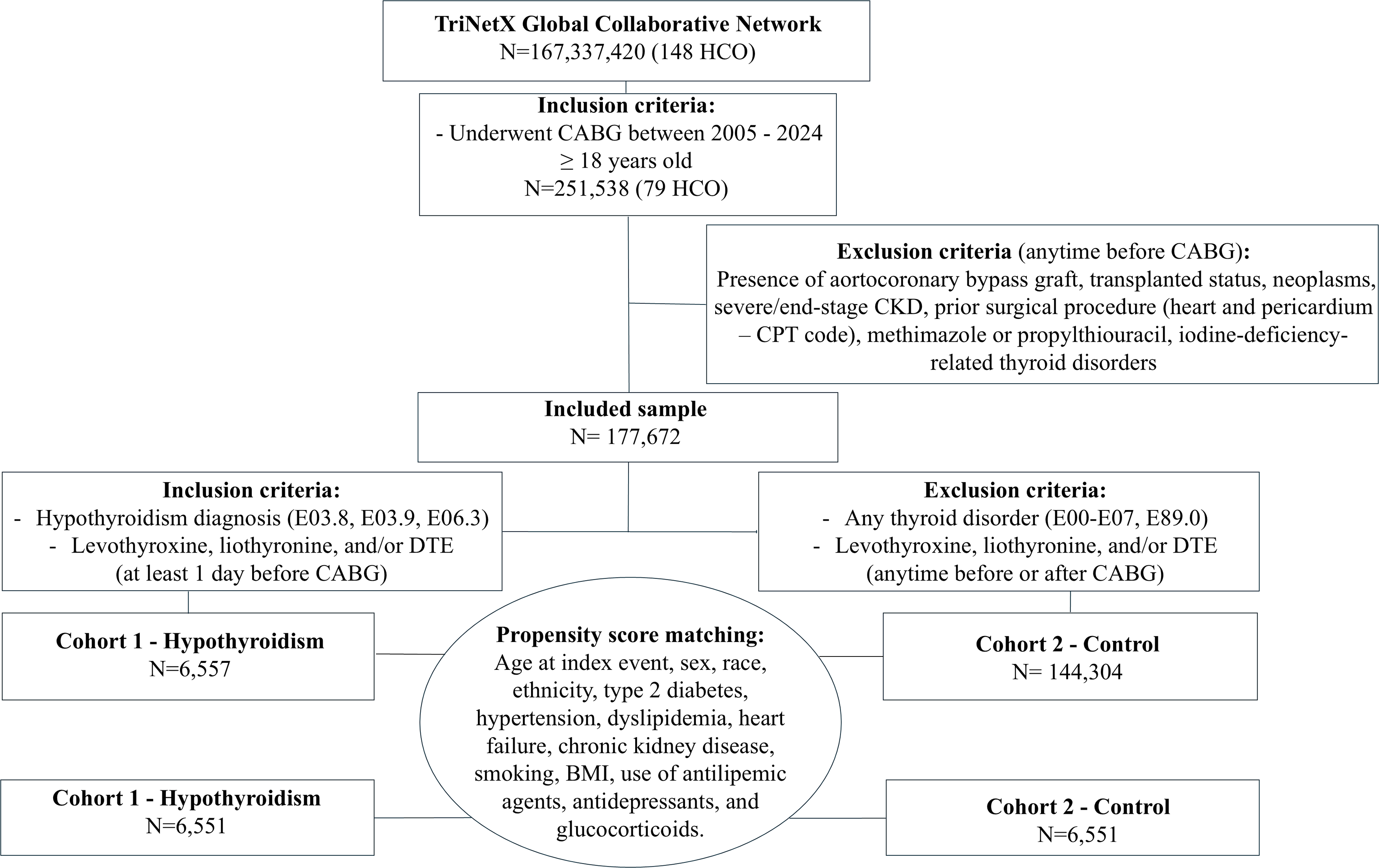
Flowchart of the study sample for Study 2 (adverse outcomes following CABG in patients with hypothyroidism). CABG, coronary artery bypass grafting.
Propensity score matching
The cohorts were propensity score-matched (1:1) to minimize confounding and selection bias, based on age at index, sex, race (White), ethnicity (Not Hispanic or Latino), type 2 diabetes, hypertension, dyslipidemia, heart failure (HF), CKD, nicotine dependence, body mass index, use of antilipemic agents, antidepressants, and glucocorticoids. We used the standardized mean difference (SMD) to assess the balance between cohorts (SMD ≥ 0.1 indicated a residual imbalance).
Outcomes
The outcomes were identified based on the ICD-10, CPT, and Veterans Affairs drug classification system (VA), among other codes (Supplementary Table S1). Short-term adverse outcomes were defined as mortality, cardiovascular outcomes, postsurgical infections, specific CABG complications, or intensive care unit (ICU) admission within 90 days following CABG. Cardiovascular outcomes included myocardial infarction (MI), HF, stroke, atrial fibrillation, embolism, thrombosis, and major adverse cardiovascular events (MACE, a composite of MI, stroke, and HF). Postsurgical infections were defined as the composite of surgical wound infections, device-related infections, respiratory and urinary tract infections, sepsis, and other postprocedural infectious complications. Specific surgical complications included aneurysm, myocarditis, pericarditis, rupture of the cardiac wall, and endocarditis. Long-term outcomes assessed mortality, cardiovascular outcomes, and another revascularization procedure (redo CABG or a percutaneous coronary intervention [PCI]) from 3 months to 10 years after the index event. For all outcomes, except for ICU admission and another revascularization procedure, we evaluated the risk of new cases, excluding patients with outcomes prior to the time window.
Baseline characteristics
A comprehensive set of baseline characteristics was evaluated within 1 year prior to the CABG procedure and included sociodemographic factors, clinical diagnoses, medication use, and laboratory measurements.
Statistical analysis
All statistical analyses were performed using the analytical tools embedded in the TriNetX platform in June 2025. Continuous variables are reported as mean and standard deviation (standard deviation [SD]) and compared using independent sample t-tests. Categorical variables are expressed as absolute (n) and relative (%) frequencies. For each outcome and cohort, percentual risk was calculated as the number of patients with the outcome divided by the total number of patients multiplied by 100. Hazard ratios (HR) with confidence intervals (CI) were estimated using Cox proportional hazards models. Patients who experienced the outcome prior to the defined time window were excluded from the respective analyses, except for ICU admissions and another revascularization procedure, to minimize the influence of pre-existing diagnoses and conditions. Regarding subgroup and sensitivity analysis, we conducted an analysis restricted to ICU admissions occurring between the day of the surgery and postoperative day 2, as well as from day 3 to day 90, to better assess when postoperative ICU care was most used by the patients. Then, we compared outcomes between CABG patients with hypothyroidism with abnormal TSH levels and those with normal-range TSH levels within 6 months on or before surgery. Patients with at least one TSH measure <0.4 or >7.0 mIU/L were considered in the abnormal TSH cohort. Patients with only TSH between 0.4 and 7.0 mIU/L were included in the normal-range TSH cohort. This subgroup analysis was performed to verify potential bias from preoperative thyroid dysfunction [16]. Then, we performed an additional analysis comparing controls with a subsample of patients with hypothyroidism who did not have TSH levels <0.4 or ≥7.00 mU/L during: (i) the first 3 months after surgery (short-term outcomes), (ii) the first 12 months after surgery, and (iii) the first 10 years after surgery (long-term outcomes). These analyses addressed the potential influence of ongoing thyroid dysfunction on early and late outcomes after CABG. We conducted a sub-analysis including in the hypothyroid cohort only patients with a diagnosis of hypothyroidism for at least 6, 12, or 24 months before CABG to assess the impact of hypothyroidism duration. In addition, sex-stratified analyses were performed. Analyses were conducted using data from the TriNetX platform, with no external imputation. Missing data were minimal (<5%) and showed no systematic patterns, so patients with incomplete follow-up or missing key variables were excluded. A p value <0.05 was considered significant throughout the study.
Results
Study I—Incidence of CABG in patients with hypothyroidism
About 1.23 million patients with hypothyroidism were compared with 1.23 million propensity score-matched controls. During a 20-year follow-up (median of 4.4 ± 5.9 years in the hypothyroidism cohort and 4.0 ± 4.7 years in controls), the incidence of CABG procedures was 0.27% (3266 cases) in the cohort with hypothyroidism and 0.22% (2651 cases) in the control cohort. Thus, patients with hypothyroidism exhibited an increased relative risk of undergoing CABG (risk ratio [RR]: 1.23; CI: 1.17–1.30; HR: 1.08; CI: 1.03–1.14).
To ensure accuracy in the diagnosis of hypothyroidism, we performed a subgroup analysis restricted to patients with a documented TSH ≥ 7.00 mU/L at 6 months before or at the diagnosis (n = 116,894). Subsequently, the propensity score was used to match a control cohort. The association between hypothyroidism and risk of CABG remained consistent with the primary analysis (incidence: 0.34% vs. 0.25%; RR: 1.26; CI: 1.09–1.47; HR: 1.19; CI: 1.02, 1.38).
Study II—Adverse outcomes following CABG in patients with hypothyroidism
Patient characteristics
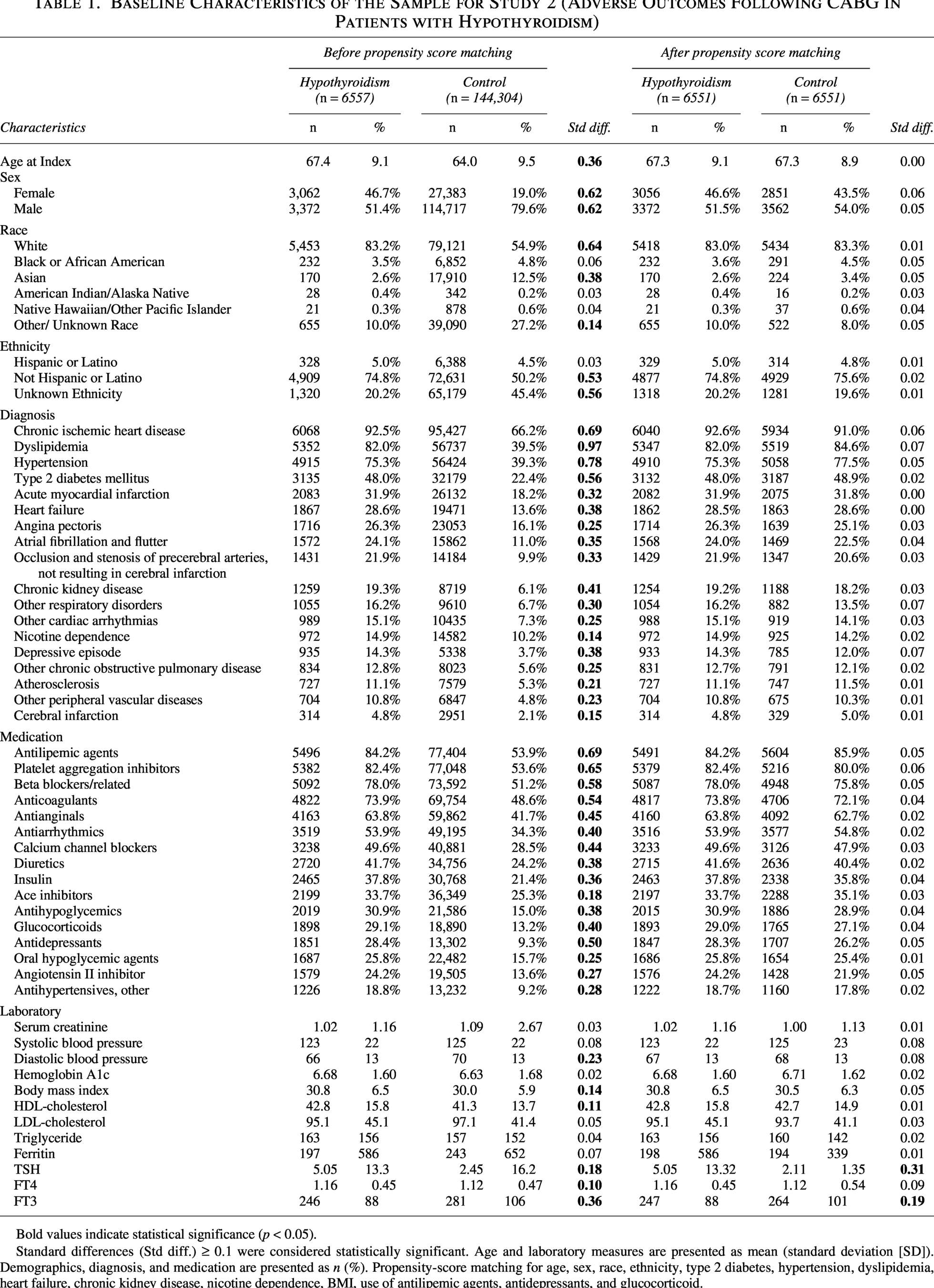
We identified 251,538 patients who underwent CABG between 2005 and 2024. After applying exclusion criteria, 177,672 patients remained in the study. Among them, 6557 patients (3.7%) presented a prior diagnosis of hypothyroidism and had been prescribed thyroid hormone replacement therapy before surgery. The control group included 144,304 patients without any documented thyroid disorder before or after CABG. Following PSM, 6551 patients remained in each cohort (Fig. 1). The matched groups were comparable in age (mean 67 ± 9 years) and sex distribution (47% vs. 44% females). Baseline characteristics were well-balanced across demographics, comorbidities, medication use, and laboratory results (all SMDs < 0.1), except for thyroid function tests. Patients with hypothyroidism had higher mean TSH levels (5.05 ± 13.32 mIU/L vs. 2.11 ± 1.35 mIU/L; SMD = 0.31) and slightly lower FT3 levels (247 ± 88 pg/dL vs. 264 ± 101 pg/dL; SMD = 0.19) compared with controls (Table 1).
Baseline Characteristics of the Sample for Study 2 (Adverse Outcomes Following CABG in Patients with Hypothyroidism)
Bold values indicate statistical significance (p < 0.05).
Standard differences (Std diff.) ≥ 0.1 were considered statistically significant. Age and laboratory measures are presented as mean (standard deviation [SD]). Demographics, diagnosis, and medication are presented as n (%). Propensity-score matching for age, sex, race, ethnicity, type 2 diabetes, hypertension, dyslipidemia, heart failure, chronic kidney disease, nicotine dependence, BMI, use of antilipemic agents, antidepressants, and glucocorticoid.
Adverse outcomes
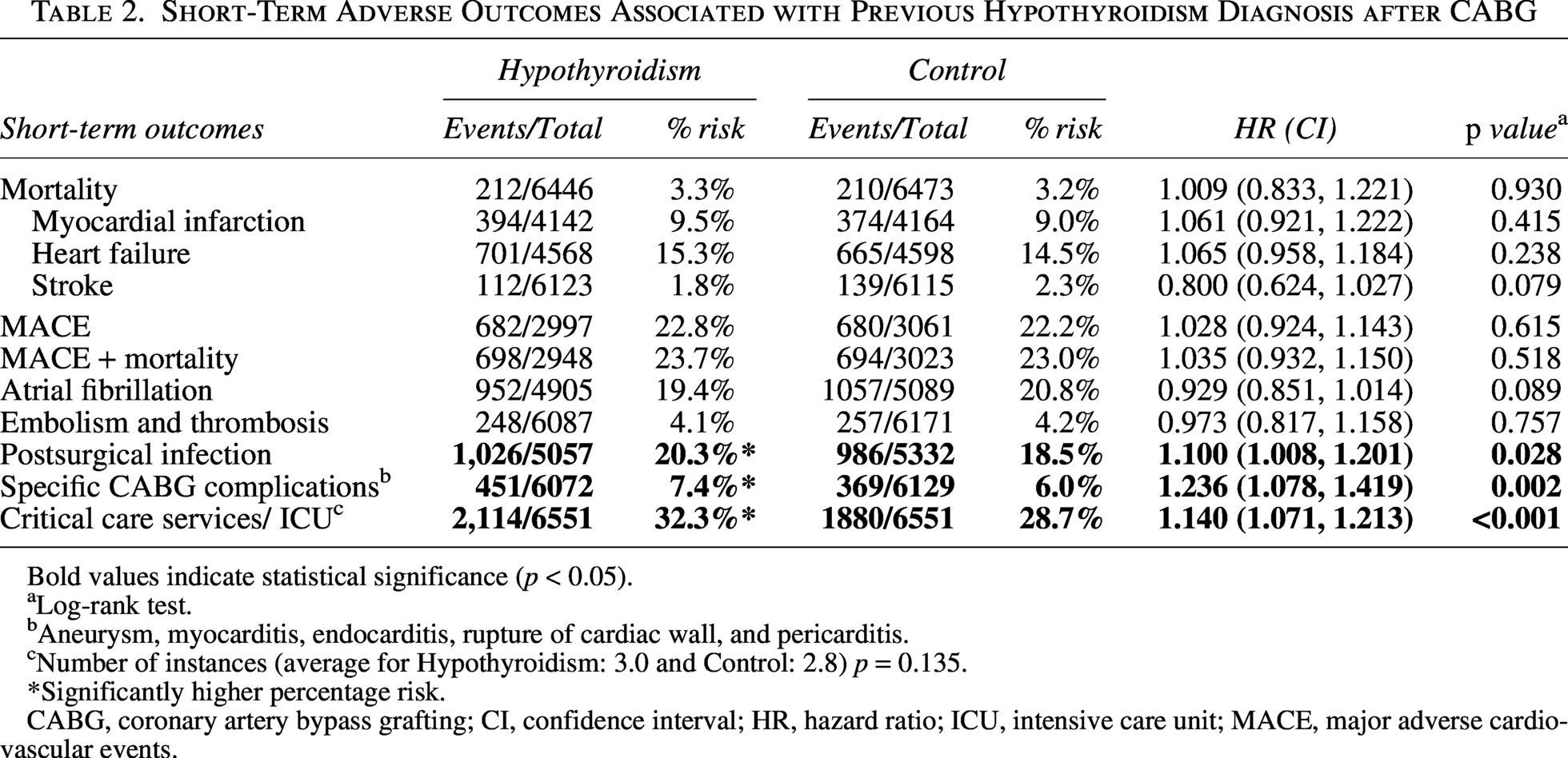
Patients with a prior diagnosis of hypothyroidism were at significantly higher risk of short-term and long-term adverse outcomes following CABG when compared with matched controls. During the first 90 days following CABG, patients with hypothyroidism were associated with increased risk of postsurgical infections (HR:1.10, CI: 1.01–1.20), surgical complications (HR: 1.24, CI: 1.08–1.42), and ICU admissions (HR: 1.14, CI: 1.07–1.21). No significant differences were observed between groups for all-cause mortality, MACE, atrial fibrillation, or thromboembolic events (p > 0.05) (Table 2).
Short-Term Adverse Outcomes Associated with Previous Hypothyroidism Diagnosis after CABG
Bold values indicate statistical significance (p < 0.05).
Log-rank test.
Aneurysm, myocarditis, endocarditis, rupture of cardiac wall, and pericarditis.
Number of instances (average for Hypothyroidism: 3.0 and Control: 2.8) p = 0.135.
*Significantly higher percentage risk.
CABG, coronary artery bypass grafting; CI, confidence interval; HR, hazard ratio; ICU, intensive care unit; MACE, major adverse cardiovascular events.
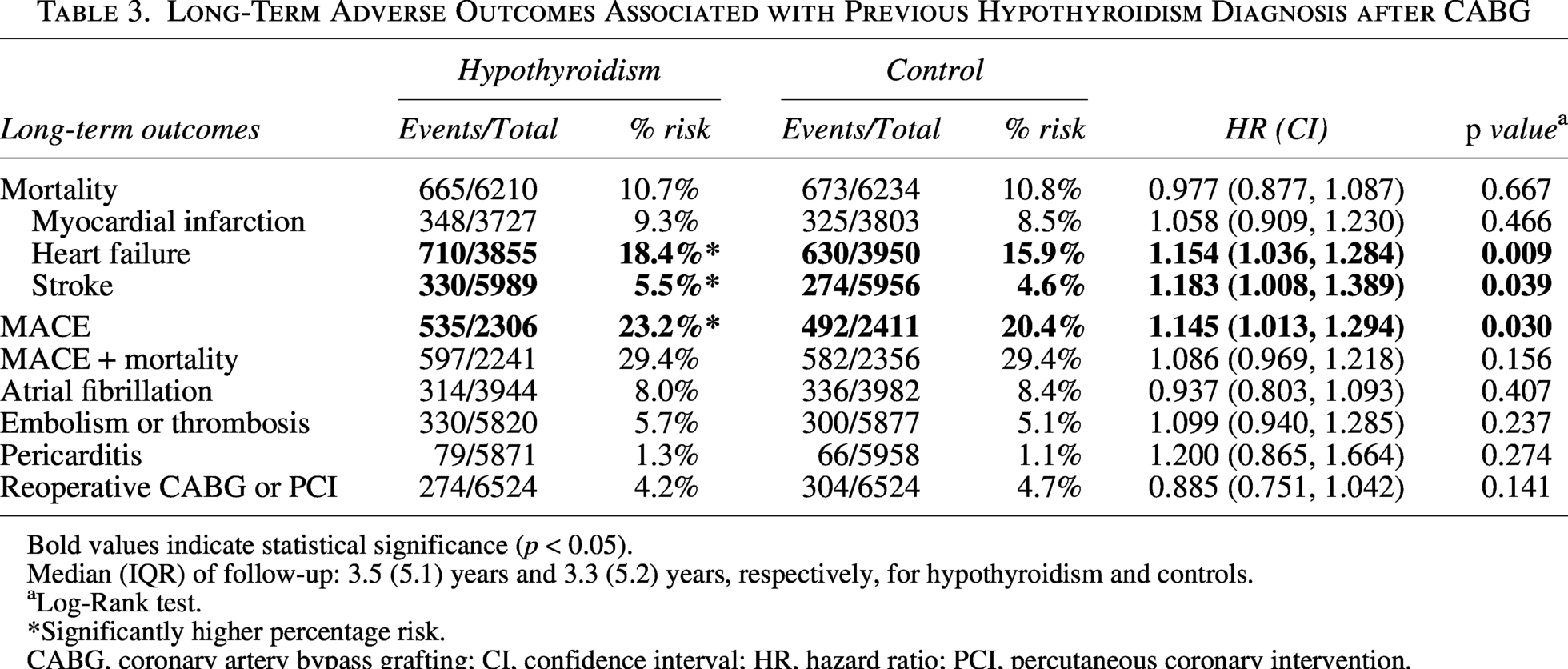
Over a median follow-up of 3.5 years in hypothyroid group and 3.3 years in controls, patients with preoperative hypothyroidism were associated with higher risk of heart failure (HR: 1.15, CI: 1.04–1.28), stroke (HR: 1.18, CI: 1.01–1.39), and MACE (HR: 1.15, CI: 1.01–1.29). No significant differences were observed in long-term mortality, myocardial infarction, atrial fibrillation, thromboembolic events, pericarditis, or redo CABG or PCI (p > 0.05) (Table 3).
Long-Term Adverse Outcomes Associated with Previous Hypothyroidism Diagnosis after CABG
Bold values indicate statistical significance (p < 0.05).
Median (IQR) of follow-up: 3.5 (5.1) years and 3.3 (5.2) years, respectively, for hypothyroidism and controls.
Log-Rank test.
*Significantly higher percentage risk.
CABG, coronary artery bypass grafting; CI, confidence interval; HR, hazard ratio; PCI, percutaneous coronary intervention.
Subgroup and sensitivity analyses
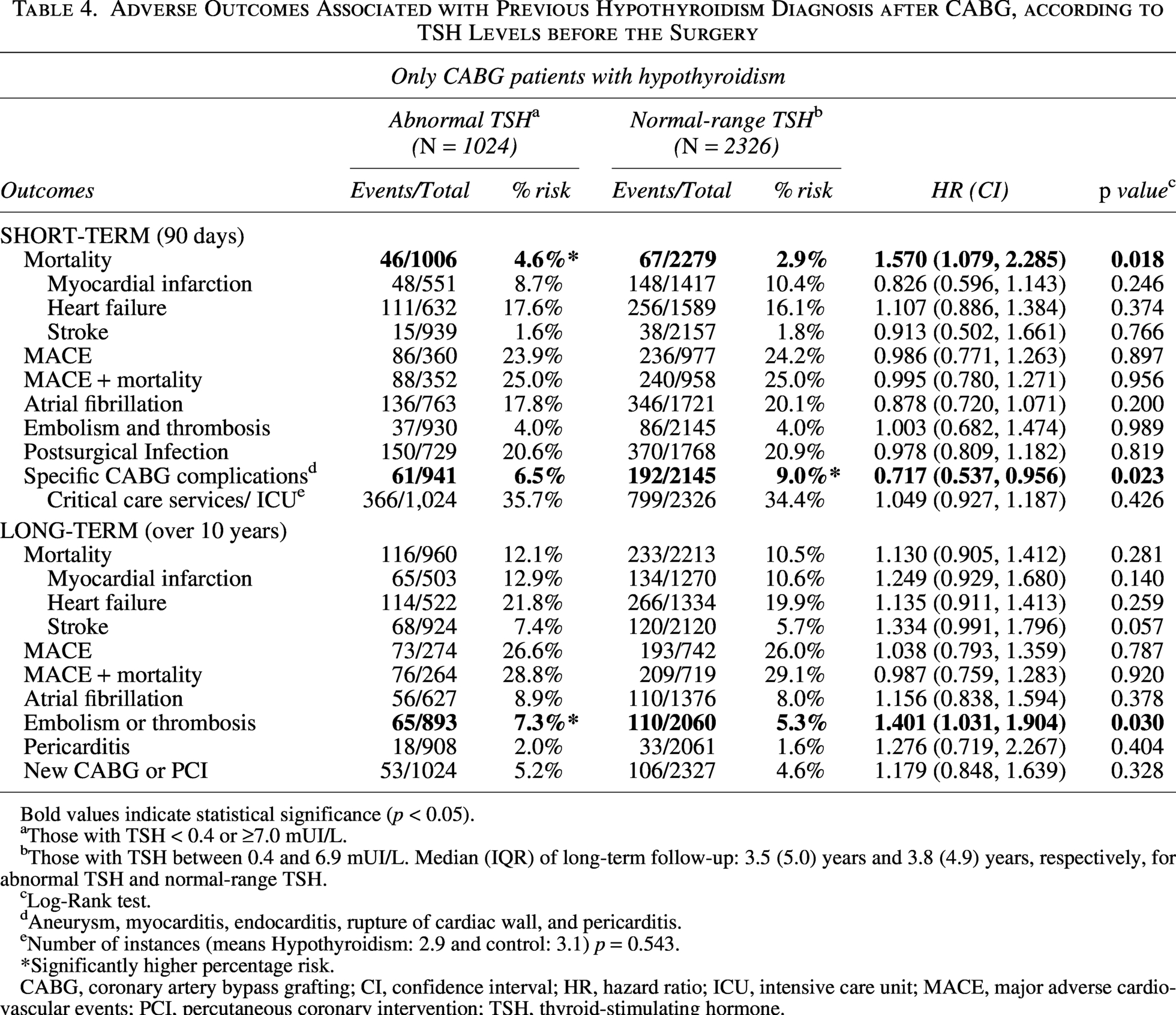
All subgroup and sensitivity analyses compared the hypothyroidism cohort to controls, with the exception of the preoperative TSH subgroup analysis (Table 4, Supplementary Tables S3 and S4), which was performed exclusively within the cohort with hypothyroidism.
Adverse Outcomes Associated with Previous Hypothyroidism Diagnosis after CABG, according to TSH Levels before the Surgery
Bold values indicate statistical significance (p < 0.05).
Those with TSH < 0.4 or ≥7.0 mUI/L.
Those with TSH between 0.4 and 6.9 mUI/L. Median (IQR) of long-term follow-up: 3.5 (5.0) years and 3.8 (4.9) years, respectively, for abnormal TSH and normal-range TSH.
Log-Rank test.
Aneurysm, myocarditis, endocarditis, rupture of cardiac wall, and pericarditis.
Number of instances (means Hypothyroidism: 2.9 and control: 3.1) p = 0.543.
*Significantly higher percentage risk.
CABG, coronary artery bypass grafting; CI, confidence interval; HR, hazard ratio; ICU, intensive care unit; MACE, major adverse cardiovascular events; PCI, percutaneous coronary intervention; TSH, thyroid-stimulating hormone.
In analyses comparing hypothyroid patients to controls, when restricting ICU utilization to admissions occurring between the day of surgery and postoperative day 2, patients with hypothyroidism had a higher risk of ICU admission compared with controls (22.2% vs. 20.5%; HR: 1.09, CI: 1.01–1.19). In contrast, when ICU admissions occurring between postoperative day 3 and day 90 were analyzed, the association was attenuated and did not reach statistical significance (9.5% vs. 8.5%; HR: 1.12, CI: 0.98–1.28).
To assess the potential impact of preoperative thyroid hormone status, we examined only CABG patients with hypothyroidism who had TSH measurements recorded within 6 months before surgery (n = 3,350). Of these, 30.6% (1024 patients) had abnormal TSH levels (<0.4 or >7.0 mIU/L. Compared with patients with normal-range TSH, those with abnormal levels had a significantly higher risk of short-term mortality (HR: 1.57; CI: 1.08–2.29) and a lower risk of CABG-specific complications (HR: 0.72; CI: 0.54–0.96) (Table 4). During long-term follow-up, abnormal TSH was associated with increased risk of embolism or thrombosis (HR: 1.40; CI: 1.03–1.90) (Table 4). Stratified analyses suggested that the increased risk of short-term mortality and long-term embolic events was primarily driven by patients with elevated TSH (≥7.0 mIU/L), whereas suppressed TSH levels were independently associated with an increased long-term risk of stroke (Supplementary Tables S3 and S4).
When comparing controls to hypothyroid patients stratified by disease duration, analyses restricted to patients with a diagnosis of hypothyroidism ≥6 or ≥12 months before CABG showed that both short- and long-term associations remained consistent with the primary analysis. However, among patients with hypothyroidism diagnosed ≥24 months before surgery, short-term risks remained elevated, whereas long-term associations with heart failure, stroke, and MACE were attenuated and no longer statistically significant (Supplementary Table S5).
In an analysis comparing controls to a subsample of patients with hypothyroidism who maintained normal TSH levels, short-term associations with ICU utilization and CABG-specific complications remained significant, whereas postsurgical infections were attenuated to borderline significance. Long-term associations with heart failure, stroke, and MACE persisted when euthyroidism was maintained during the first postoperative year. However, these associations were no longer statistically significant among patients who maintained sustained TSH normalization for up to 10 years (Supplementary Table S6).
In sex-stratified analyses comparing hypothyroid patients to controls, statistically significant associations were observed primarily among females. For them, hypothyroidism was associated with increased short-term ICU utilization (HR 1.18, CI 1.07–1.30) and long-term heart failure (HR 1.19, CI 1.02–1.39) (Supplementary Table S7). In males, no statistically significant associations were identified for short- or long-term outcomes, although a borderline association was observed for long-term heart failure (HR 1.17, CI 0.99–1.37) (Supplementary Table S8).
Discussion
This study revealed that patients with a diagnosis of hypothyroidism have an increased likelihood of undergoing CABG compared with matched individuals without thyroid disorders. Furthermore, among patients undergoing CABG, the diagnosis of hypothyroidism was associated with a modest but significantly increased risk of postoperative infections, CABG-specific complications, and ICU utilization, as well as a higher long-term risk of heart failure, stroke, and MACE. The increased ICU utilization was primarily driven by admissions occurring within the first two postoperative days, suggesting that early perioperative vulnerability may account for much of this signal. Restricting the cohort to patients with documented TSH levels revealed that preoperative off-target TSH levels were associated with a risk of short-term mortality and long-term embolic events. Stratified analyses indicated that these increased events were primarily associated with elevated preoperative TSH, but factors such as acute illness or treatment adherence could also influence these findings. In addition, when postoperative euthyroidism was maintained, long-term cardiovascular associations were no longer statistically significant, suggesting that maintaining adequate thyroid hormone replacement can positively affect the outcome of CABG surgery.
Collectively, these findings indicate that both the diagnosis of hypothyroidism and whether it is adequately treated are associated with adverse outcomes following CABG. The higher risk of adverse outcomes may translate into prolonged recovery, a higher risk of long-term morbidity, reduced quality of life,27,28, and may lead to greater healthcare utilization. 29 The results highlight the importance of preoperative assessment and optimization of thyroid hormone homeostasis to not only reduce complications but also healthcare costs in this population.
The increased incidence of CABG observed among patients with a diagnosis of hypothyroidism may reflect persistent cardiometabolic risk despite thyroid hormone replacement therapy. Accumulating evidence suggests that patients treated with levothyroxine frequently exhibit residual metabolic abnormalities, including higher total cholesterol and low-density lipoprotein (LDL) cholesterol levels, even when TSH concentrations are within the reference range. 30 Observational studies have further demonstrated increased statin utilization among levothyroxine-treated individuals, supporting the presence of ongoing dyslipidemia and residual cardiovascular risk. 6 More recently, lower serum triiodothyronine (T3) levels have been identified as an independent determinant of dyslipidemia in patients receiving levothyroxine, suggesting that tissue-level thyroid hormone signaling may remain suboptimal despite normalized TSH. 31 While causality cannot be established in the present study, the convergence of persistent dyslipidemia, increased statin exposure, and higher CABG incidence supports the hypothesis that thyroid hormone imbalance may contribute to accelerated cardiometabolic risk over time.
Beyond their influence on metabolic pathways, thyroid hormones also play a critical role in cardiovascular regulation, including myocardial contractility, heart rate, systemic vascular resistance, and endothelial function. 32 While it is well established that these mechanisms are disrupted in patients with overt hypothyroidism, it is often assumed that in LT4-treated patients with normal TSH levels, they are fully restored. However, a growing body of evidence indicates that this is not the case in all bodily systems. For example, in LT4-treated rodents, it has been observed that normalization of TSH coexists with residual hypothyroidism in the brain 33 and in other organs. 34 Similar findings were observed in the clinical setting. Despite the elevated cholesterol and LDL levels,6,7 LT4-treated patients with normal TSH levels also weigh about 10 pounds more and may exhibit reduced metabolic rate.30,35–38 Therefore, incomplete normalization of thyroid hormone signaling in LT4-treated patients undergoing CABG, either caused by suboptimal thyroid hormone replacement or inherent limitations of the LT4-therapy, could lead to endothelial dysfunction, 32 impaired immune function, 39 and reduced respiratory drive. 40 This scenario could not only contribute to the increased incidence of CABG in patients with hypothyroidism but also to their increased susceptibility to postoperative infections and prolonged ventilation, aligning with the higher infection rates and ICU utilization observed in our cohort. Further studies are needed to evaluate treatment adequacy and the comparative effectiveness of specific thyroid hormone replacement strategies to clarify these hypotheses.
The strength of the present study is the use of a large, multicenter, real-world dataset with PSM, enabling robust comparisons, independent of confounders such as diabetes and dyslipidemia. In addition, the associations of adverse outcomes and the diagnosis of hypothyroidism were further strengthened in the subgroup and sensitivity analyses. Nonetheless, several limitations exist, which are inherent to the observational design and limited granularity of patient data. The present study assessed multiple outcomes following CABG. Multiple comparisons warrant careful interpretation. While we feel our results show consistency, we cannot rule out type 1 error as an explanation of our results. Potential residual confounding factors include reliance on administrative codes, the absence of detailed T3/T4 measurements or thyroid hormone replacement data, as well as factors that may influence both access to surgery and postoperative outcomes, such as socioeconomic status, insurance type, or regional healthcare system characteristics. Although controls were not selected based on the absence of comorbidities, and a robust PSM was performed, the control cohort may still be affected by selection or surveillance bias. Detailed information regarding the underlying etiology of hypothyroidism (e.g., autoimmune vs. iatrogenic) was not available, but we know that among the patients who had antithyroperoxidase antibody results, positivity was observed in about 50% of the cases, which is similar to what was observed in a large population of patients with hypothyroidism. 41
In this large, multicenter cohort study, we found that patients with a diagnosis of hypothyroidism had a higher incidence of CABG, which was associated with an increased risk of early postoperative infections, CABG-specific complications, and ICU utilization, as well as a higher long-term risk of heart failure, stroke, and MACE. These findings highlight hypothyroidism as a potential risk factor for CABG and for postsurgical adverse outcomes. Prospective studies are needed to evaluate whether targeted thyroid hormone management can improve surgical outcomes in patients with hypothyroidism undergoing CABG.
Authors’ Contributions
V.M.: Conceptualization (equal), formal analysis (lead), methodology (equal), visualization (lead), writing—original draft (lead). F.E.d.L.B.: Conceptualization (equal), data curation (supporting), formal analysis (equal), visualization (supporting), writing—review and editing (equal). A.I.: Conceptualization (equal), data curation (supporting), formal analysis (equal), visualization (supporting), writing—review and editing (equal). S.H.: Conceptualization (equal), methodology (equal), writing—review and editing (equal). G.G.: Data curation (supporting), formal analysis (supporting), software (supporting), writing—review and editing (equal). K.K.: Data curation (supporting), formal analysis (supporting), software (supporting), writing—review & editing (equal). M.D.E.: Methodology (equal), writing—review and editing (equal). I.M.B.: Methodology (equal), writing—review and editing (equal). A.C.B.: Conceptualization (equal), methodology (equal), supervision (lead), writing—review and editing (lead).
Data Sharing Statement
Data were obtained from the TriNetX Research Network and are not publicly available due to licensing restrictions. The corresponding author will provide details about the restrictions and any conditions for accessing some data upon request.
Footnotes
Author Disclosure Statement
V.M., F.E.d.L.B., A.I., S.H., G.G., K.K., M.D.E., and I.M.B.: no conflicts to disclose. Antonio Bianco: consultant for AbbVie, Acella, Aligos, Synthonics, and Xeris.
Funding Information
V.M.: funded by the Fundação de Amparo a Pesquisa de São Paulo (FAPESP), Brazil. #
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.