
Abstract
Background:
Over recent decades, variations have been observed in the incidence of pediatric hyperthyroidism (HT) and Graves’ disease (GD), preferred treatment modalities, and long-term outcomes. This study aimed to evaluate trends and long-term outcomes of pediatric HT across a 20-year period in a large cohort.
Methods:
We conducted a retrospective study using the electronic database of a large health maintenance organization. Children aged 2–18 years who were diagnosed with HT between 2000 and 2019, received antithyroid drugs (ATDs) for at least 6 months, and were followed up through 2024 were included in the analysis.
Results:
Of 5,111,304 insured children, 518 (75% females) met the inclusion criteria. The median age at diagnosis was 15.1 (13.0–16.5) years, and the median follow-up was 10.4 (6.5–15.1) years. The median ATD treatment duration was 3.8 (1.8–6.6) years. The mean initial methimazole dose decreased from 15.8 (8.5–23.4) mg/day in 2000–2009 to 12.9 (7.3–19.4) mg/day in 2010–2019 (p = 0.030). The overall remission rate was 31.1%. Compared with children diagnosed in 2000–2009, those diagnosed in 2010–2019 were less likely to undergo definitive treatment (27.5% vs. 59.6%, p < 0.001) and had higher nonremission (19.0% vs. 3.8%, p < 0.001) and relapse rates (15.9% vs. 4.6%, p < 0.001). Among the 161 children achieving remission, the median time to remission was 2.36 years. Younger age and antithyroid peroxidase positivity were associated with later remission (p = 0.010 and p = 0.018, respectively). Higher baseline free thyroxine levels at diagnosis were found in children with late remission than in those with early remission (42.4 [26.7–61.5] vs. 32.6 [24.4–42.5] pmol/L, p = 0.014).
Conclusions:
Over the past two decades, the management of pediatric HT has evolved toward more prolonged medical therapy and decreased reliance on definitive treatments. This change in practice appears to coincide with an increased relapse rate, underscoring the clinical implications of these changes. Future studies should focus on evaluating the influence of these treatment strategies on the long-term prognosis of children with pediatric HT.
Keywords
Introduction
Hyperthyroidism (HT) in children and adolescents is an uncommon but clinically significant endocrine disorder characterized by excessive thyroid hormone production, leading to multisystem effects, including cardiovascular, metabolic, and neurocognitive disturbances. The etiologies of HT in childhood are diverse and include autoimmune, inflammatory, and nodular thyroid diseases, as well as transient causes such as thyroiditis. 1 Among these, Graves’ disease (GD) is by far the most common cause of HT in the pediatric population, accounting for the vast majority of cases requiring prolonged antithyroid treatment.2–4 As in adults, the three treatment modalities in pediatric GD are antithyroid drugs (ATDs), thyroid ablation by radioactive iodine (RAI), and thyroidectomy; however, the risks and benefits of each modality differ. The first-line treatment for pediatric GD is medical therapy with ATDs. When remission is not achieved or severe ATD-related adverse events occur, definitive treatment (DT) with RAI or surgery is indicated. Current management guidelines recommend carbimazole or its active metabolite, methimazole (MMI; also known as thiamazole), as first-line therapy, whereas propylthiouracil (PTU) should generally be avoided because of its association with hepatic failure. 1 ATD therapy should be continued for at least 3 years and may be extended to 5 years or longer. 1 Total thyroidectomy or RAI should be considered in individuals who experience significant side effects from ATDs, such as severe neutropenia, agranulocytosis, or hepatic dysfunction, as well as in those who remain thyrotoxic despite high-dose ATD therapy or who fail to achieve remission after a prolonged treatment course. These options are also appropriate for patients who prefer not to continue ATD therapy.
Disease remission in pediatric GD is defined as 12 months of normal thyroid function after ATD cessation. 2 Reported remission rates range from 20–30% after 2 years of ATD therapy to 24–46% after treatment durations of up to 6 years and are consistently lower than those reported in adults GD.2,3 One small study with a treatment duration of 9 years reported a remission rate of 75%, 4 suggesting that remission rates may increase with longer treatment duration. However, there is not enough data to support this observation. Once in remission, the relapse rate in children ranges from 6% 5 to 42% 6 across cohorts, and it is most likely to occur within 1 year of treatment cessation. 2
Over the past few decades, the management of pediatric GD has evolved considerably. The earlier, more permissive use of RAI and thyroidectomy, either at presentation or following 2 years of medical therapy, has shifted toward an initial, long-term medical approach with MMI as first-line therapy.1,7 Moreover, lower initial MMI doses are now commonly used to minimize adverse effects. 8 It remains unclear, however, whether this shift in therapeutic strategy has influenced the course of disease or long-term outcomes.
This study examined temporal changes in the management of persistent pediatric HT and their effects on long-term outcomes by comparing cohorts diagnosed during 2000–2009 and 2010–2019. The cohort was restricted to children requiring prolonged ATD treatment, consistent with Graves’ disease.
Methods
A retrospective study analyzing medical records from the electronic database of Clalit Health Services (CHS), the largest health maintenance organization (HMO) in Israel, serving about 54% of the population. The database is compiled from continuous, real-time input from physicians and health service providers. It includes coded diagnoses, demographic, socioeconomic, and clinical data, as well as hospital discharge summaries, outpatient clinic diagnoses, laboratory results, medical treatments, and medication dispensation records.
Study population
The electronic database of CHS was searched for all children and adolescents aged 2–18 years, diagnosed with “hyperthyroidism,” “Graves’ disease,” or “thyrotoxicosis” between 2000 and 2019. Case identification was based on the presence of biochemical HT (suppressed thyrotropin (TSH) with elevated fT4 and/or fT3), a diagnostic code for GD or HT (ICD-10 E05.0, E05.8, E05.9), and treatment with ATDs for at least 6 months to exclude cases of transient HT as part of Hashimoto’s disease and cases of toxic thyroid nodules. This approach was applied as TSH receptor antibody (TRAb) measurements and imaging findings were not consistently available in the database, particularly in earlier years. Given that GD accounts for the vast majority of pediatric HT requiring prolonged antithyroid therapy, this approach was considered highly suggestive of GD, although antibody confirmation was not available for all cases. Follow-up data were collected through the end of 2024. Children with type 1 diabetes were excluded from the analyses as the disease in this population has distinct features. 9
The study was approved by the local institutional ethics committee in accordance with the principles of the Declaration of Helsinki (approval number 0649-23-RMC). In accordance with Ministry of Health regulations, the institutional ethics committee did not require written informed consent, as data were collected anonymously from computerized medical files, without active patient participation.
Data collected
Data collected from the electronic database included sex, age, ethnic origin, socioeconomic status, blood test results, ATD dispensations, and relevant medical procedures. As data on pubertal status were not available in the registry, an age-based stratification was performed, using 10 years as a surrogate threshold for prepubertal versus pubertal status. Ethnic origin was defined as Jewish or Arab. The socioeconomic status was determined according to the socioeconomic position (SEP) index of the Israel Central Bureau of Statistics. 10 This is an adjusted calculation of 14 variables that measure social and economic levels in the domains of demographics, education, standard of living, and employment. SEP clusters are ranked on a scale of 1–10, with 1 representing the lowest SEP, and were categorized in our analysis into three levels: low (clusters 1–4), medium (clusters 5–6), and high SEP (clusters 7–10).
Laboratory data included TSH, fT3, fT4, antithyroid peroxidase (TPO) antibodies, anti-thyroglobulin (TG) antibodies, and TRAbs. Blood tests were retrieved at 6 months before the diagnosis date, at diagnosis, and throughout follow-up. Antibody positivity was defined as a value exceeding the upper limit of the normal range for the specific assay used. Information on dispensed ATDs (MMI, carbimazole, and PTU) included the drug name, dose per pill, quantity, and date of dispensation. Data on levothyroxine dispensations included the dispensation date. Reported ATD-related adverse effects, including leukopenia, neutropenia, agranulocytosis, hepatic abnormalities, rash, and arthritis (both coded diagnoses and biochemical disturbances), were also collected. Data on DT procedures included total or partial thyroidectomy (available in the database from 2005) and RAI ablation (available from 2015).
Outcome measures
Outcomes were defined as follows: No remission—continuous ATD dispensations throughout the entire follow-up period. Temporary interruptions of <12 months were considered a continuation of the initial treatment course; remission—discontinuation of ATD therapy at least 6 months before the end of follow-up, accompanied by normal TSH levels for at least 3 months after the last dispensation, with no further ATD or levothyroxine prescriptions thereafter; relapse—discontinuation of ATD therapy for at least 12 months followed by reinitiation of treatment. This group also included children with persistently suppressed TSH levels after ATD cessation, without subsequent reinitiation of therapy; Definitive therapy—since direct records of thyroidectomy and RAI therapy were incomplete, DT was inferred in children who discontinued ATD therapy before the end of follow-up and subsequently received levothyroxine prescriptions initiated at least 1 year after the diagnosis of HT. Lost to follow-up—cessation of ATD dispensations before the end of follow-up, with no available TSH results thereafter. Disease severity was defined according to the levels of fT4 at presentation (higher levels represent greater severity).
Treatment duration was calculated as the interval between the first and last ATD dispensation. The mean daily ATD dose during the first 6 months was calculated for MMI only using the formula: number of tablets dispensed × tablet dose / 180 days. Mean follow-up duration was determined by subtracting the age at diagnosis from the age at the last available TSH measurement.
Statistical analysis
Statistical analyses were performed using SPSS software, version 28 (SPSS Inc., Chicago, IL). Data are presented as n (%) for categorical variables and as median (interquartile range) for skewed numerical distributions. Comparisons between two groups (sex, year, diagnosis categories, or early vs. late remission) were conducted using Pearson’s chi-square test for categorical variables and the Mann–Whitney U test for numerical variables. Comparisons among three outcome categories were conducted using Pearson’s chi-square test for categorical variables and the Kruskal–Wallis test for numerical variables. Post hoc multiple comparisons were performed using the Bonferroni method to compare each pair of groups. Comparisons of adverse events between medication types were conducted using Fisher’s exact test. Predictive models for remission and time to remission were developed using multivariate forward logistic regression. Variables with p < 0.3 in the univariate analysis were included in the models.
Results
Cohort characteristics
During the study period, 5,111,304 children aged 2–18 years were insured by CHS. Of these, 637 met the inclusion criteria for pediatric HT consistent with probable GD. After excluding 119 children diagnosed between 2020 and 2024 who had insufficient follow-up, the final analytic cohort comprised 518 patients, of whom 75% were females (Fig. 1). The median age at diagnosis was 15.1 (interquartile range 13.0–16.5) years, and the median follow-up duration was 10.4 (6.5–15.1) years. The median duration of ATD therapy was 3.8 (1.8–6.6) years, with a mean initial MMI dose of 13.4 mg/day (7.8–20.3). Overall, 161 patients (31.1%) achieved remission with no subsequent relapse, 59 (11.4%) had persistent HT, 53 (10.2%) relapsed after remission, and 226 (43.6%) underwent definitive therapy (Table 1).
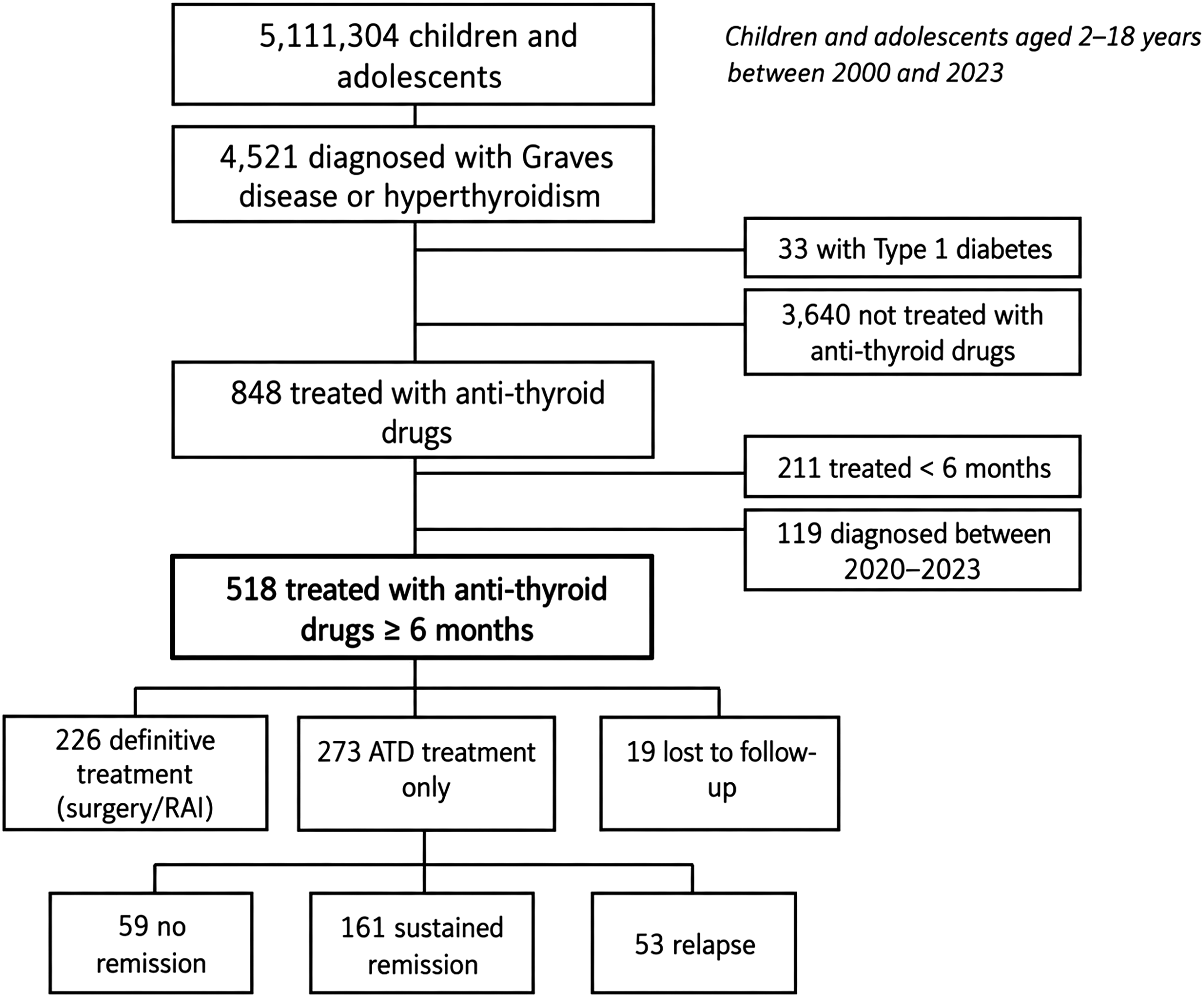
Study flowchart.
Patient Characteristics According To Year Of Diagnosis
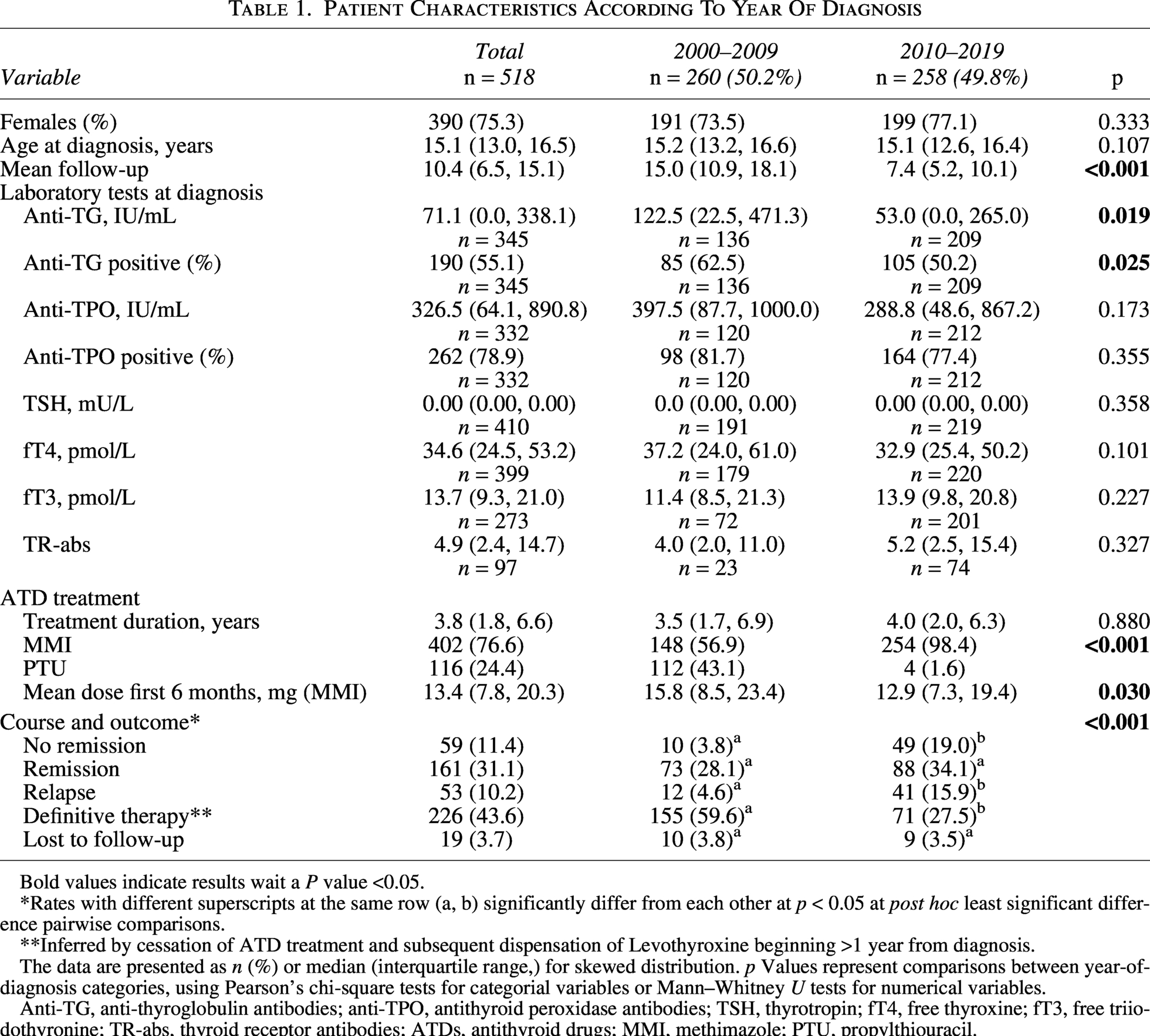
Bold values indicate results wait a P value <0.05.
*Rates with different superscripts at the same row (a, b) significantly differ from each other at p < 0.05 at post hoc least significant difference pairwise comparisons.
**Inferred by cessation of ATD treatment and subsequent dispensation of Levothyroxine beginning >1 year from diagnosis.
The data are presented as n (%) or median (interquartile range,) for skewed distribution. p Values represent comparisons between year-of-diagnosis categories, using Pearson’s chi-square tests for categorial variables or Mann–Whitney U tests for numerical variables.
Anti-TG, anti-thyroglobulin antibodies; anti-TPO, antithyroid peroxidase antibodies; TSH, thyrotropin; fT4, free thyroxine; fT3, free triiodothyronine; TR-abs, thyroid receptor antibodies; ATDs, antithyroid drugs; MMI, methimazole; PTU, propylthiouracil.
Children diagnosed before 10 years of age (n = 53) were compared with those diagnosed at ≥10 years of age (n = 465) (Supplementary Table S1). Remission rates were lower among younger children than among older children (23% vs. 32%, respectively; p < 0.001).
Temporal trends in management and outcomes
Demographic features, including sex distribution, age at diagnosis, and ethnic composition, were similar between the two decades (2000–2009 and 2010–2019) (Table 1). The biochemical profile at presentation was comparable, except for higher anti-TG antibody levels (122.5 [22.5–471.3] IU/mL vs. 53.0 [0.0–265.0] IU/mL; p = 0.019) and TG-antibody positivity (62.5% vs. 50.2%; p = 0.025) in the earlier decade. A marked shift in therapeutic practice was observed. The use of PTU as the initial ATD declined sharply from 43.1% in 2000–2009 to 1.6% in 2010–2019 (p < 0.001). Among patients starting MMI therapy, the mean initial dose decreased from 15.8 (8.5–23.4) mg/day in 2000–2009 to 12.9 (7.3–19.4) mg/day in 2010–2019 (p = 0.030). The proportion of patients undergoing definitive therapy (RAI or thyroidectomy) decreased from 59.6% to 27.5% (p < 0.001). Despite these therapeutic changes, remission rates remained stable (28.1% vs. 34.1%; p = 0.138). Conversely, relapse rates (15.9% vs. 4.6%; p < 0.001) and rates of nonremission (19.0% vs. 3.8%; p < 0.001) were more frequent among patients diagnosed during 2010–2019 (Fig. 2).
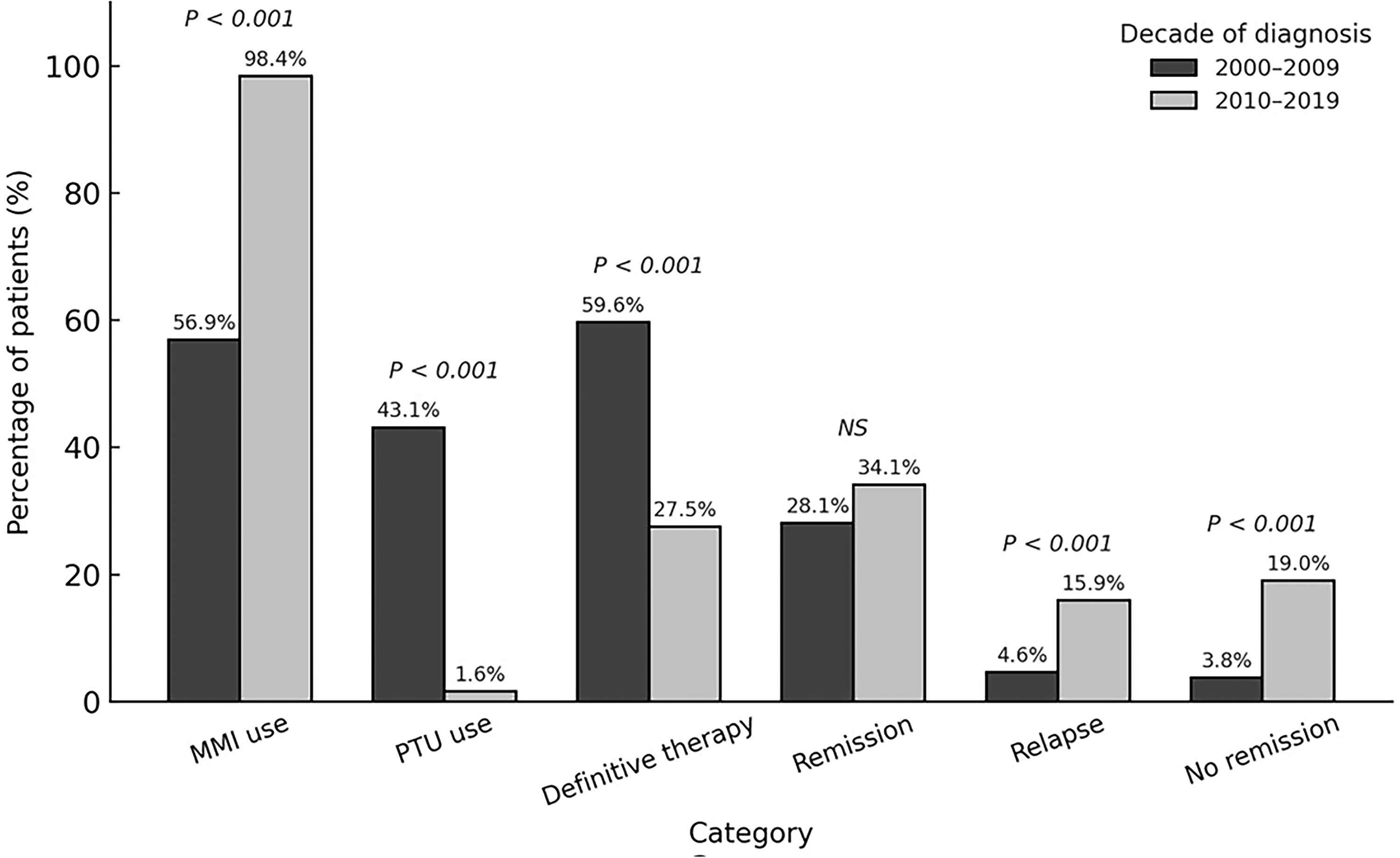
Temporal trends in management, treatment, and outcomes by decade of diagnosis. Decade-wise differences in methimazole (MMI) and propylthiouracil (PTU) use, as well as outcome distribution (definitive therapy, remission, relapse, no remission), among children diagnosed with Graves’ disease. p Values are shown above each comparison. The outcomes remission, relapse, and no remission refer only to patients treated with antithyroid drugs. NS, nonsignificant.
Clinical and biochemical correlates of treatment outcome
Among children who did not undergo definitive therapy (n = 273), three outcome groups were defined: no remission (59 [21.6%]), remission without relapse (161 [59.0%]), and relapse after remission (53 [19.4%]) (Fig. 1, Table 2). Children with no remission were younger at diagnosis, with a median age of 14.1 (10.8–16.0) years, compared with those achieving remission (15.2 [13.1–16.6]) or relapse (15.3 [13.5–16.8]; p = 0.012). They also presented with higher fT4 (38.2 [29.2–55.8] pmol/L) and fT3 (17.1 [11.3–24.8] pmol/L) levels than the relapse group (fT4 28.7 [20.6–38.6] pmol/L, p = 0.009; fT3 11.8 [8.8–16.5] pmol/L, p = 0.022). Treatment duration, socioeconomic status, and ethnic distribution were comparable among the three groups.
Characteristics Of Patients Receiving Antithyroid Treatment According To Outcome
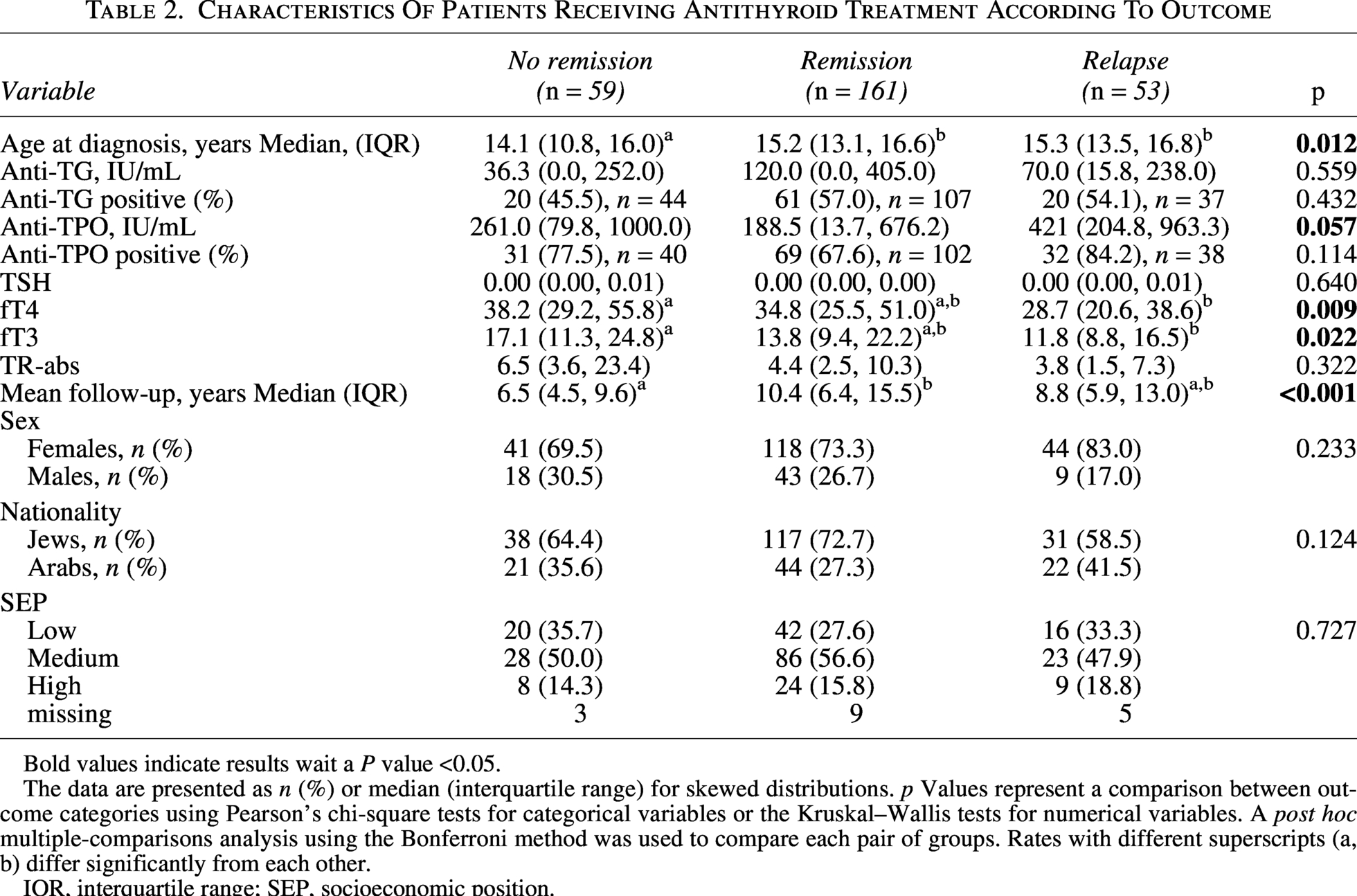
Bold values indicate results wait a P value <0.05.
The data are presented as n (%) or median (interquartile range) for skewed distributions. p Values represent a comparison between outcome categories using Pearson’s chi-square tests for categorical variables or the Kruskal–Wallis tests for numerical variables. A post hoc multiple-comparisons analysis using the Bonferroni method was used to compare each pair of groups. Rates with different superscripts (a, b) differ significantly from each other.
IQR, interquartile range; SEP, socioeconomic position.
Socioeconomic status did not influence rates of referral for DT (p = 0.739). However, a larger proportion of Arab children underwent DT compared with Jewish children (51.4% vs. 41.9% respectively, p = 0.041).
To determine which variables were associated with remission, we performed a multivariable logistic regression. Variables included in the model were: age at diagnosis, anti-TPO level, anti-TPO positivity, fT4 level, fT3 level, mean MMI dose during the first 6 months of treatment, mean follow-up duration, sex, nationality, and SEP. In the final model, the only variables that were associated with higher rates of remission were older age at HT diagnosis (odds ratio [OR] = 1.13 CI [0.998–1.286], p = 0.054), lower fT4 levels at diagnosis (OR = 0.96, CI [0.929–1.000], p = 0.048), and longer follow-up duration (OR = 1.20, CI [1.015–1.417], p = 0.033).
Among patients who achieved remission, the median time to remission was 2.36 years (Table 3, Fig. 3). Those with late remission (≥2.36 years) had higher baseline fT4 concentrations than those with early remission (<2.36 years) (42.4 [26.7–61.5] vs. 32.6 [24.4–42.5] pmol/L; p = 0.014) and tended toward a higher anti-TPO positivity (76.0% vs. 59.6%; p = 0.077).
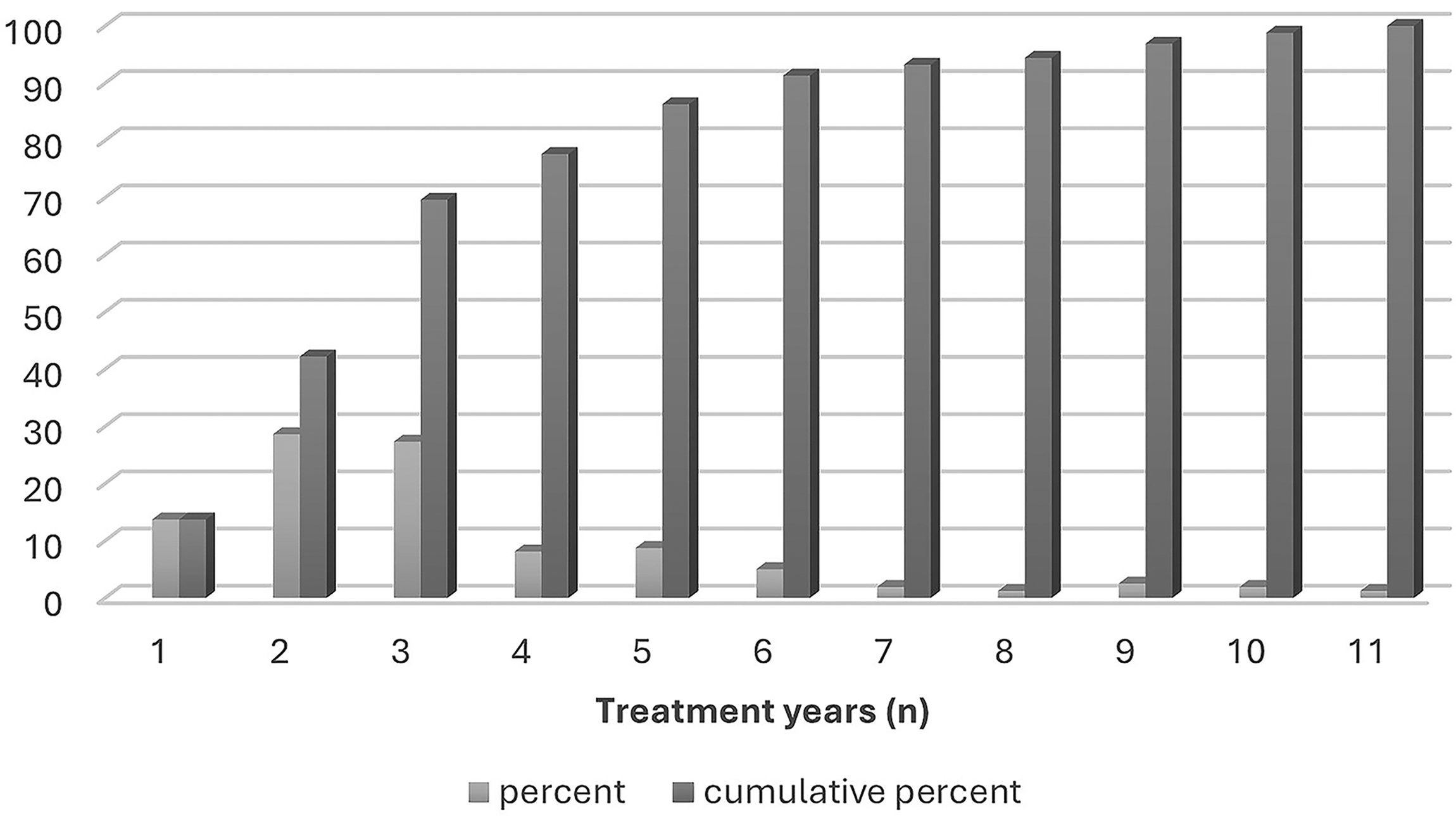
Annual and cumulative remission rates (%). Annual rate of remission (light gray) and cumulative rate of remission (dark gray) during the first 11 years of follow-up, in patients who were treated with antithyroid drugs only and achieved remission during follow-up.
Characteristics Of The Remission Group Patients According To Early And Late Remission (Before/After Median Survival Of 2.36 Years)
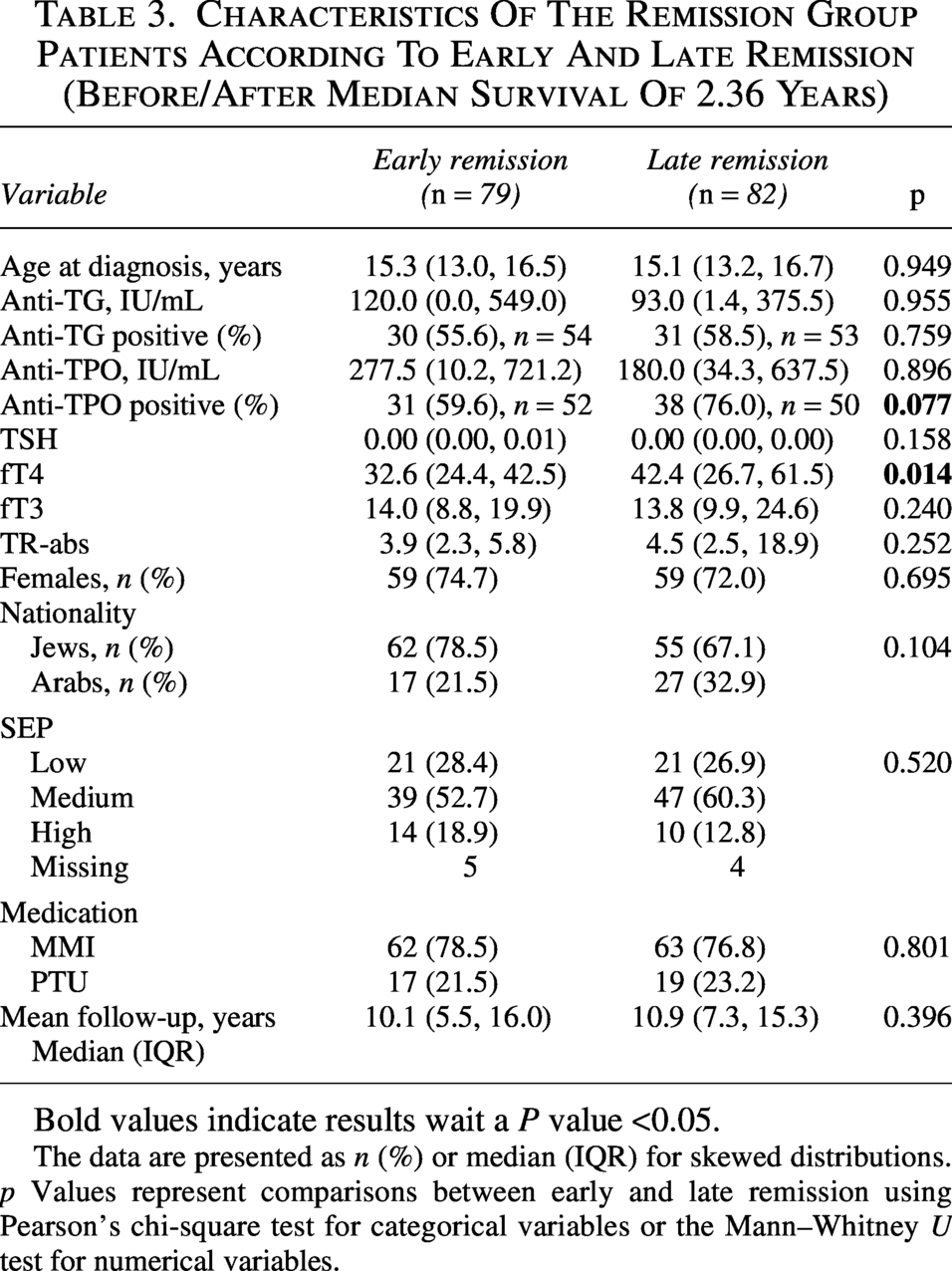
Bold values indicate results wait a P value <0.05.
The data are presented as n (%) or median (IQR) for skewed distributions. p Values represent comparisons between early and late remission using Pearson’s chi-square test for categorical variables or the Mann–Whitney U test for numerical variables.
A multivariable logistic regression was performed as a post hoc secondary analysis to identify factors associated with late (≥2.36 years) versus early (<2.36 years) remission (Supplementary Table S3). Variables included in the model were: anti-TPO positivity, TSH level, fT4 level, fT3 level, mean follow-up duration, and nationality. The variables that entered the final model were age at diagnosis and anti TPO positivity. Younger age at diagnosis (OR = 0.87 [CI 0.784–0.967], p = 0.010) and positive anti-TPO antibodies (OR = 2.282 [CI 1.154–4.514], p = 0.018) were associated with increased odds of being in the late (≥2.36 years) remission group.
Sex-related differences in presentation and outcome
Of the 518 patients, 390 (75.3%) were female and 128 (24.7%) were male (Supplementary Table S2). Age at diagnosis, socioeconomic level, ethnic background, and treatment duration were comparable between the sexes. However, males presented with higher fT3 levels (15.7 [10.8–25.0] vs. 13.4 [8.8–20.3] pmol/L; p = 0.023) and a higher rate of anti-TPO antibody positivity (87.2% vs. 76.4%; p = 0.041). Despite these differences at presentation, treatment response and long-term outcomes were similar between the sexes, with remission rates of 33.6% in males and 30.3% in females (p = 0.413).
Discussion
This study aimed to evaluate trends and long-term outcomes of pediatric GD over a 20-year period in a large cohort by comparing individuals diagnosed with persistent pediatric HT during 2000–2009 and 2010–2019. The use of DT declined markedly between the two decades, accompanied by a decrease in the use of PTU and the use of lower absolute MMI doses. The remission rate remained stable throughout the decades studied, whereas the rates of relapse and nonremission increased during the second decade. Younger age and higher fT4 and fT3 levels at diagnosis were associated with a lower likelihood of remission.
The severity of disease at presentation, as reflected by the initial biochemical profile, did not differ between the decades. Our findings differ from those of adult cohorts, in which declining disease severity, reflected by smaller goiters and less intense eye involvement,11,12 has been described over recent years. While initial fT4 and fT3 levels were comparable between the decades in our cohort, anti-TG antibody positivity and absolute levels were lower in the second decade compared with the first. Such a trend in recent years has not been previously described, and its clinical significance is unclear. In adults, anti-TG antibody positivity has been linked to reduced responsiveness to antithyroid therapy, 13 but in children, in whom anti-TPO Ab and anti-TG Ab are often positive at diagnosis, neither their presence nor their titer predict long-term outcomes. 14
Over the past 20 years, the management of pediatric GD has undergone a substantial shift toward prolonged medical therapy with MMI and away from the use of PTU and definitive treatment. This shift is reflected in our findings by a marked decline in the use of definitive therapy and PTU. This evolution likely reflects the implementation of updated pediatric and adult guidelines that emphasize MMI as the preferred ATD, and caution against PTU because of hepatotoxicity risk. 15 Although the European Thyroid Association guideline formally endorsed prolonged ATD therapy in children in 2022, accumulating pediatric evidence supporting extended treatment durations and dose-titration strategies had already been published during the preceding decade.3,4,16 These publications likely contributed to gradual changes in clinical practice prior to formal guideline updates.
Lower initial MMI doses are now recommended to reduce the rate of adverse events. 2 Consistent with this trend, we observed a reduction in initial absolute MMI doses over time. Because dosing was assessed using absolute rather than weight-based measures, this finding should be interpreted with caution. However, the similar age distributions between the cohorts suggest that it likely reflects a true shift in prescribing patterns. Despite this change, remission rates remained stable across decades, suggesting that prolonged lower-dose therapy may achieve outcomes comparable to those of earlier, more intensive regimens. However, both relapse and nonremission rates increased during the second decade, possibly reflecting greater reliance on prolonged medical therapy before definitive intervention. Therefore, definitive therapy remains warranted in selected cases.
Consistent with prior pediatric reports demonstrating higher remission rates with prolonged treatment,12–14 our analysis of remission rates per year showed almost 10% remission between the 7th and the 11th years of treatment. These findings support recommendations for extending ATD therapy beyond 3 years in children with persistent disease and good tolerance. 1 Although we were not able to consistently record adverse events of MMI treatment from the electronic records, previous studies showed a favorable profile of adverse events in children, explaining the decrease in RAI and thyroidectomy over the years. 7
The paradigm shift toward prolonged ATD treatment is also described in a recent adult GD management survey that included 1400 health care providers from 85 countries. 17 The survey found that almost 90% of the providers chose ATDs as their primary treatment modality in 2023, compared with 59.7% in 2012 and 31% in 1990. This trend conveys increasing awareness of the long-term consequences of thyroid ablation, lifelong hypothyroidism, and the potential effects of RAI exposure, balanced against the possibility of eventual remission with prolonged medical therapy. Meta-analyses in adults have shown no differences in mortality or morbidity between patients treated with ATDs and those treated with definitive treatment, 18 whereas other studies have argued that early ablation prevents recurrent HT. 19
Younger age and higher fT4 and fT3 levels at diagnosis were associated with nonremission, aligning with prior studies identifying symptom severity, laboratory markers, and age as key determinants of treatment response. 16 Higher baseline fT4 levels were also characteristic of individuals who achieved remission after a longer duration of therapy, although this factor did not enter our prediction model of early versus late remission under ATD treatment. In children who eventually achieved remission, younger age and anti-TPO positivity were associated with higher odds of achieving late rather than early remission. In adults, anti-TPO positivity has sometimes correlated with improved remission, 20 possibly reflecting coexisting destructive autoimmunity; however, in children, this association remains inconsistent. 14
To contextualize our findings, we summarized the largest pediatric GD cohorts published over the past 15 years (Table 4).3,5,6,21–25 Reported remission rates vary widely across studies, ranging from as low as 6% to more than 50%, with similarly broad variation in relapse rates and the use of definitive therapy. These differences likely reflect heterogeneity in follow-up duration, definitions of remission and relapse, duration of ATD therapy, and patient age distribution. The variability across studies underscores the importance of standardized outcome definitions and prolonged follow-up when interpreting long-term disease trajectories in pediatric GD.
Main Findings Of Previous Large Cohorts of Pediatric Graves’ Disease Published In 2010–2025
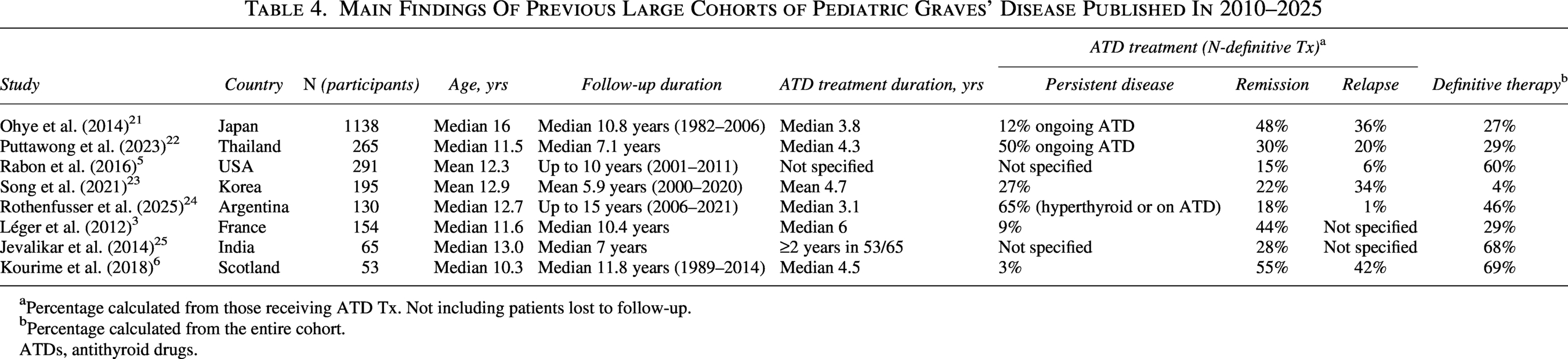
Percentage calculated from those receiving ATD Tx. Not including patients lost to follow-up.
Percentage calculated from the entire cohort.
ATDs, antithyroid drugs.
This study has several important strengths. It is one of the largest population-based cohorts of pediatric HT reported to date, encompassing more than five million insured children over a 20-year period within a single national health system. The centralized electronic database allowed the inclusion of virtually all children treated for HT within the HMO, thereby minimizing referral bias and enhancing representativeness. Although the dataset is subject to inherent limitations, the cohort likely represents children with GD and is therefore well suited to capturing temporal changes in disease management. The prolonged follow-up duration, extending up to two decades and through 2024, enabled robust assessment of long-term outcomes.
Our study is subject to several limitations. Because the study is based on a registry, some clinical details are missing. Systematic TRAb measurements and imaging findings were not available for the entire cohort, particularly during the earlier years of the registry. Consequently, the diagnosis of GD was presumed based on biochemical thyrotoxicosis, diagnostic coding, and prolonged ATD therapy. Although this approach may allow for some degree of misclassification, GD accounts for the vast majority of pediatric HT requiring long-term antithyroid treatment, and the likelihood of substantial diagnostic misclassification is low.
Another limitation stems from incomplete procedural data on thyroidectomy and RAI therapy in the first years of the study; therefore, the use of DT was inferred from ATD cessation along with initiation of long-term levothyroxine ≥1 year after diagnosis. While spontaneous permanent hypothyroidism may occur, it is uncommon in children, and levothyroxine initiation likely represents a reasonable proxy, though limited misclassification cannot be excluded. To validate our findings on procedural rates, we compared our results with the true rates of surgery and RAI performed in a subgroup of children who were treated in our tertiary center (n = 87, unpublished data). During the same follow-up period, 7% (6/87) of these children underwent thyroidectomy and 37% (32/87) underwent RAI, with a total of 44% (38/87) undergoing DT. These numbers suggest our finding of DT in 36.3% of the children is a reasonable result, and do not imply an overestimation due to misclassification of children with spontaneous conversion to hypothyroidism as children who underwent DT.
MMI dosing was assessed using absolute values rather than weight-based measures because body weight data were not consistently available in the registry. Given the similar age distribution between cohorts, this finding likely reflects a true change in prescribing patterns; however, it should be interpreted with caution. Outcome definitions relied on biochemical and prescription data rather than direct clinical assessment. The registry lacked data on goiter size, ophthalmopathy, pubertal stage, symptom severity, physician decision-making, and consistent body weight, precluding weight-based MMI dosing analysis. Although adverse events were identified using coded diagnoses and laboratory abnormalities, these data were not sufficiently robust for detailed evaluation. Future studies should also focus on long-term complications that we could not assess, such as permanent hypoparathyroidism after thyroidectomy. As with all observational studies, residual confounding and unmeasured variables cannot be excluded, and external validation would strengthen the generalizability.
In summary, this extensive cohort study demonstrates a clear shift in the management of pediatric HT toward prolonged MMI therapy, with a marked reduction in the use of definitive treatments and a lower absolute initial dose, yet without compromising remission rates. The observed increase in relapse rates highlights the need for individualized long-term follow-up. Future studies should confirm these findings and focus on defining the optimal therapy duration, as well as assessing the long-term impact of these evolving practices, to guide more personalized management strategies for children and adolescents with HT and GD.
Authors’ Contributions
T.O.: Conceptualization (equal) and writing—review and editing (equal). M.Y.-G.: Methodology (lead); formal analysis (equal); and writing—review and editing (equal). L.L.: Methodology (supporting) and writing—review and editing (supporting). N.F.-S.: Conceptualization (equal); writing—original draft (lead); and formal analysis (equal).
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding information to declare.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.