
Abstract
Background
The COVID-19 pandemic led to significant changes in daily routines and lifestyles, potentially affecting eating behavior and psychological well-being.
Objectives
This study aims to determine the level of fear caused by the COVID-19 pandemic in healthcare professionals and to investigate the effect of fear of coronavirus on individuals’ eating habits.
Methods
108 male and 388 female healthcare professionals working in any healthcare facility in Turkey during the COVID-19 pandemic filled out an online survey that included socio-demographic characteristics, nutrition and food purchasing habits, Fear of COVID-19 Scale, and Emotional Appetite Questionnaire (EAQ).
Results
We found that fear of COVID-19 is higher in female healthcare professionals than in males. Higher COVID-19 fear predicted a greater risk of positive emotional appetite (OR:2.2; 95%CI:1.4–3.2). In addition, the Fear of COVID-19 Scale total score positively correlated with negative EAQ scores in females (p < 0.05). Fear of COVID-19 Scale scores of healthcare professionals who reported that they experienced a decrease in appetite levels and meal frequency during the COVID-19 pandemic were higher than those who declared that their appetite level and meal frequency did not change (p < 0.05). Finally, we found that the odds of positive emotional eating were 2.3 times higher in overweight and obese people compared to underweight and normal weight people.
Conclusions
These findings highlight the significant impact of COVID-19-related fear on the emotional eating behaviors and overall dietary habits of healthcare professionals, emphasizing the need for targeted interventions to address psychological and nutritional challenges in this vulnerable population during and after pandemics.
Introduction
In December 2019, a new disease (COVID-19) appeared in Hubei Province, China. Global problems began in business, economy, and health during this period. 1 The epidemic quickly reached the size of a pandemic. To reduce the adverse effects of the epidemic, some measures, especially social isolation, and hygienic rules, were taken in many countries. These restrictive practices changed many people's behaviors and food choices due to increasing stress levels. 2
Fear of contracting the disease was one of the substantial reasons that increased stress during the COVID-19 pandemic. As COVID-19 fear increases the perception of risk, it can be increased attention to the measures taken against the disease. However, it can cause harm to mental and physical health. 3 Changes in daily routine during the pandemic, fear of COVID-19, and negative mood caused by being away from social environments such as work, school, etc., triggered emotional and binge eating behaviors. 4
Healthcare professionals are among the groups most affected by the pandemic.5,6 Most of the time, healthcare professionals, who had met with patients diagnosed with COVID-19 without adequate medical supplies and personal protective equipment, had to stay away from their social environment due to the high risk of infection.7,8 The intense working conditions in this period, sleep disorders caused by extended and changing working hours, and decreased social interaction caused an increase in the stress level of healthcare professionals.9,10,11 Difficulties in accessing food, disturbance in mealtimes, and increased stress have increased the consumption of unhealthy foods (fast food, added sugar, energy-dense foods, beverages, etc.) among healthcare professionals. 12
Eating behaviour can be influenced by changes in an individual's emotional state. 13 Emotional eating is defined as ‘the tendency to overeat in response to negative emotions such as anxiety, depression and irritability’. According to psychosomatic theory, the typical response to stress is a loss of appetite; however, some people have been observed to increase their food intake during stress. 14 As in the rest of the world, healthcare professionals in Turkey had to continue to work with more intense hours during the COVID-19 pandemic and were exposed to significant stress. This situation can lead to changes in emotional appetite and put healthcare workers at risk of eating disorders due to increased fear, anxiety and stress. It is essential to determine the mental and physical negativities that may occur because of the COVID-19 pandemic and to plan improvement activities such as dietary strategies, legal regulations, and rehabilitation works for this group. We did not find any studies in the literature that investigated the relationship between COVID-19 anxiety and emotional appetite in healthcare workers in our country during the pandemic. Therefore, we aimed to determine the coronavirus-related fear levels of healthcare professionals who had to continue their working life under intense stress during the pandemic, to compare the fear of coronavirus between genders, and to investigate the effect of coronavirus fear on individuals’ emotional appetite levels and eating habits in this study.
Materials and methods
Study design and subjects
The population of the research comprised healthcare professionals. Healthcare professionals working in different cities in Turkey filled out the online survey through social media channels between July and September 2020. All participants declared that they read the written consent form before participating. With G power analysis, the total sample size was 484 people with an effect size of 0.3, a margin of error of 0.05, and a reliability of 95%. The inclusion criteria are to be a healthcare worker for at least 6 months before the pandemic and to continue working during the pandemic period, 18–64 years of age, not to have any diagnosed psychological illness, not to use a drug that affects appetite and mood.
Research instruments
The first part of the questionnaire included questions about the characteristics of the participants, anthropometric measurements (height, body weight), and changes in dietary habits, food shopping, and dietary supplement use during the pandemic. The following sections included the Fear of COVID-19 Scale and the Emotional Appetite Questionnaire.
The fear of COVID-19 scale
Ahorsu et al. 15 developed the Fear of COVID-19 Scale in 2020. The total score on the scale is between 7 and 35. High scores on the scale indicate that the participant's level of fear about COVID-19 increased. The Cronbach's Alpha internal consistency coefficient of the original scale was 0.82,, 15 and it was 0.87 in our study.
Although there are various validity and reliability studies of the Fear of COVID-19 Scale, we used the scale adopted by Bakioğlu et al. in this study. 16 The result of the evaluation made with the receiver operating characteristics (ROC) analysis showed that the cut-off point of the Fear of COVID-19 Scale is 17.5.17,18
Emotional appetite questionnaire (EAQ)
In 2010, Nolan et al. 19 developed The Emotional Appetite Questionnaire. The questionnaire consists of 14 items that determine the effect of the participants’ emotions and thoughts on their appetite. Participants rate the level of affecting their appetite statements in each item as less, the same, and more. We calculated the EAQ negative total score by adding the negative emotions and states scores and the EAQ positive total score by adding the positive emotions and states scores. The scale has no cut-off score. In 2014, Demirel et al. 20 performed the Turkish validity and reliability of EAQ and found Cronbach's alpha coefficient was 0.73, and we found 0.86 in the current study.
Statistical analysis
We analysed data through SPSS 23.0 package program. Categorical variables such as demographic data of individuals, smoking, and using dietary supplements were expressed as numbers (n) and percentages (%). Continuous variables such as age, anthropometric measurements, and scale scores are given as mean and standard deviation (x ± sd). The Shapiro-Wilk test was used to determine whether the variables had a normal distribution. Pearson Correlation Coefficient was calculated to evaluate the relationship between continuous variables. Pearson Chi-square test was used to evaluate the relationship between categorical variables. Independent Student t-test was used to compare continuous variables between two groups, the one-way ANOVA test was used for parametric data, and the Kruskal-Wallis test was used for non-parametric data to compare continuous variables between three or more groups. After the one-way ANOVA, post hoc testing was performed using Tukey's test to identify which groups differed, with p-values adjusted using Bonferroni correction for multiple tests. Multivariable logistic regression was performed to examine the relation between positive emotional appetite and BMI, gender, and COVID-19 fear. Age (continuous) was controlled in multivariable adjusted model. The p < 0.05 value was taken as significant. 21 The cut-off point of the Fear of COVID-19 Scale was analyzed using ROC curve analysis. In the presence of significant threshold values, sensitivity, specificity, positive predictive value, and negative predictive value were calculated. While evaluating the area under the curve, a 5% type-I error level was used to accept a statistically significant predictive value of the test variables.17,18,21
Results
This study had a sample size of 496 healthcare professionals, 108 of whom are male and 388 are female. It's also important that participants from 63 different cities across Turkey took part, covering all health professions. 39.1% of the participants have children under the age of 18, and 12.1% have individuals over the age of 65 in their households. 12.9% of the participants have a chronic disease. 44.5% of the participants reported that they did not take any dietary supplements, 20.6% that they took before the COVID-19 pandemic, and 34.6% that they started to take them during the coronavirus epidemic. 25.4% of the participants reported that they smoke. The mean age of the participants is 32.4 ± 9.2 years. With regards to the distribution of Fear of COVID-19 Scale score averages of healthcare professionals as per their profession, the highest score average is observed in dieticians by 16.9 ± 5.1, followed by nurses by 16.8 ± 6.2, while the lowest average was in EMT/paramedic healthcare professionals by 13.0 ± 5.3 (p < 0.05) (Table 1).
General characteristics and a comparison of fear of coronavirus scale total score averages with the general characteristics of individuals.
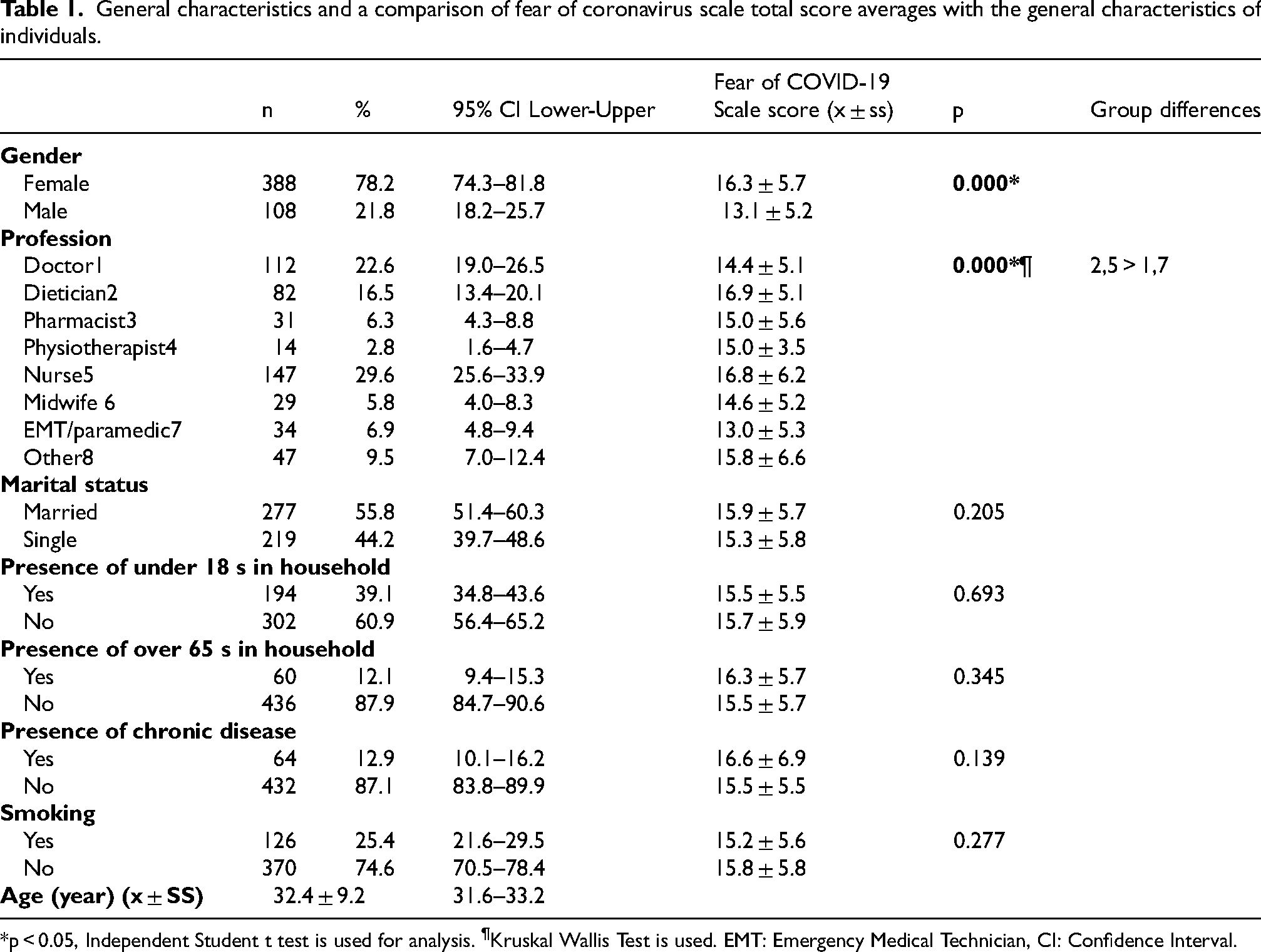
*p < 0.05, Independent Student t test is used for analysis. ¶Kruskal Wallis Test is used. EMT: Emergency Medical Technician, CI: Confidence Interval.
There was a significant difference between male and female healthcare professionals in the change in the frequency of eating out (p < 0.05). During the COVID-19 pandemic, 16.1% of healthcare professionals reported that their packaged food consumption increased, 37.3% of them that a decrease, and 46.6% that no change. 10.1% of healthcare professionals reported that their consumption of sugar increased, 25.0% decreased, and 64.9% did not change during the COVID-19 pandemic. In the COVID-19 pandemic, the changes in water consumption, the amount of food stocked, and the status of being a food tried for the first time were different according to gender (p < 0.05). The EAQ positive total score was significantly higher in male participants (6.2 ± 1.5) than in female participants (5.5 ± 1.5). Female healthcare professionals had significantly higher Fear of COVID-19 Scale scores than males (p < 0.05) (Table 2).
Distribution of some characteristics of healthcare professionals as per gender.
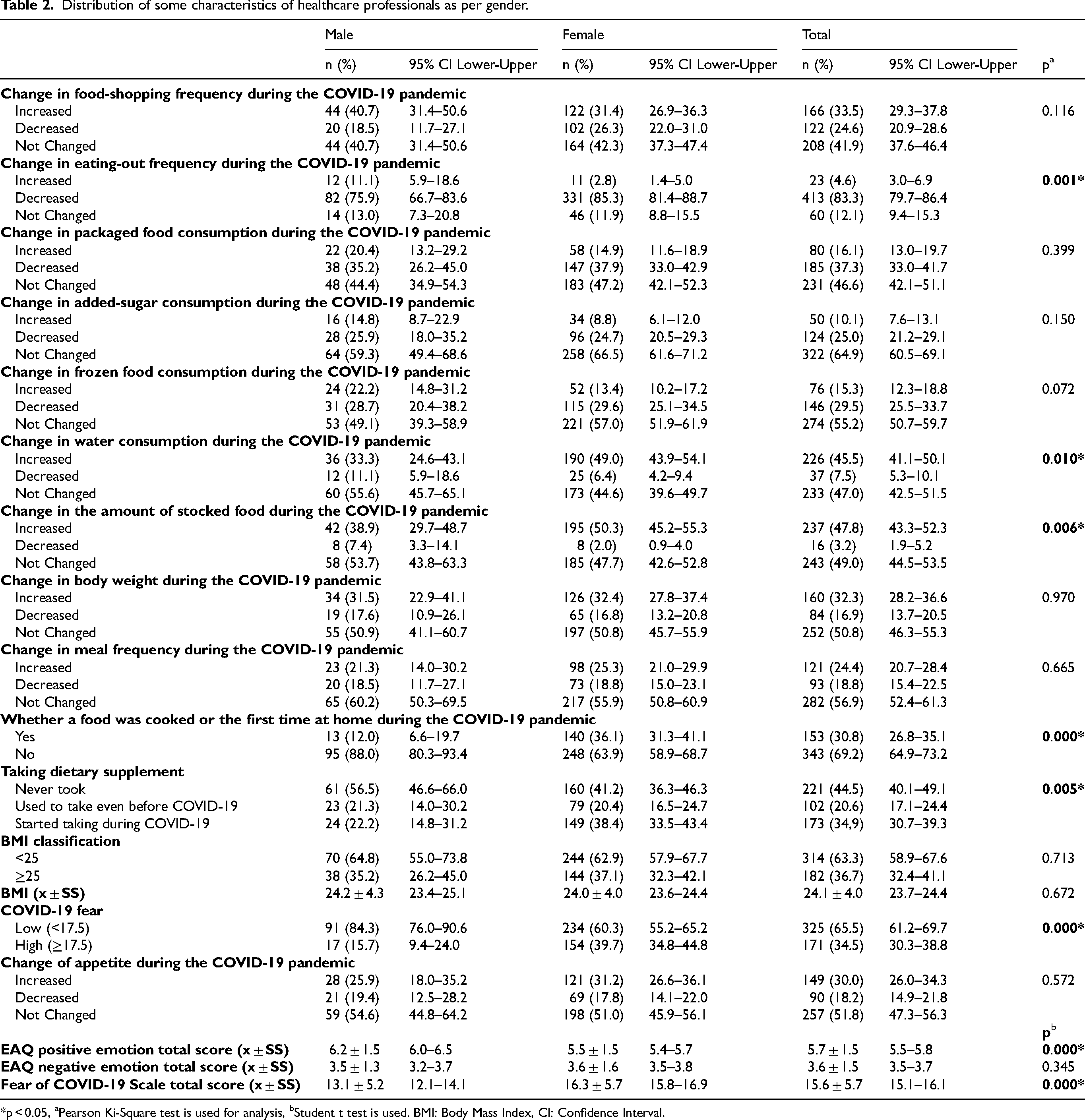
*p < 0.05, aPearson Ki-Square test is used for analysis, bStudent t test is used. BMI: Body Mass Index, CI: Confidence Interval.
The place of shopping for vegetables and fruits among healthcare professionals was significantly different before and after COVID-19 (p < 0.05) (Figure 1).
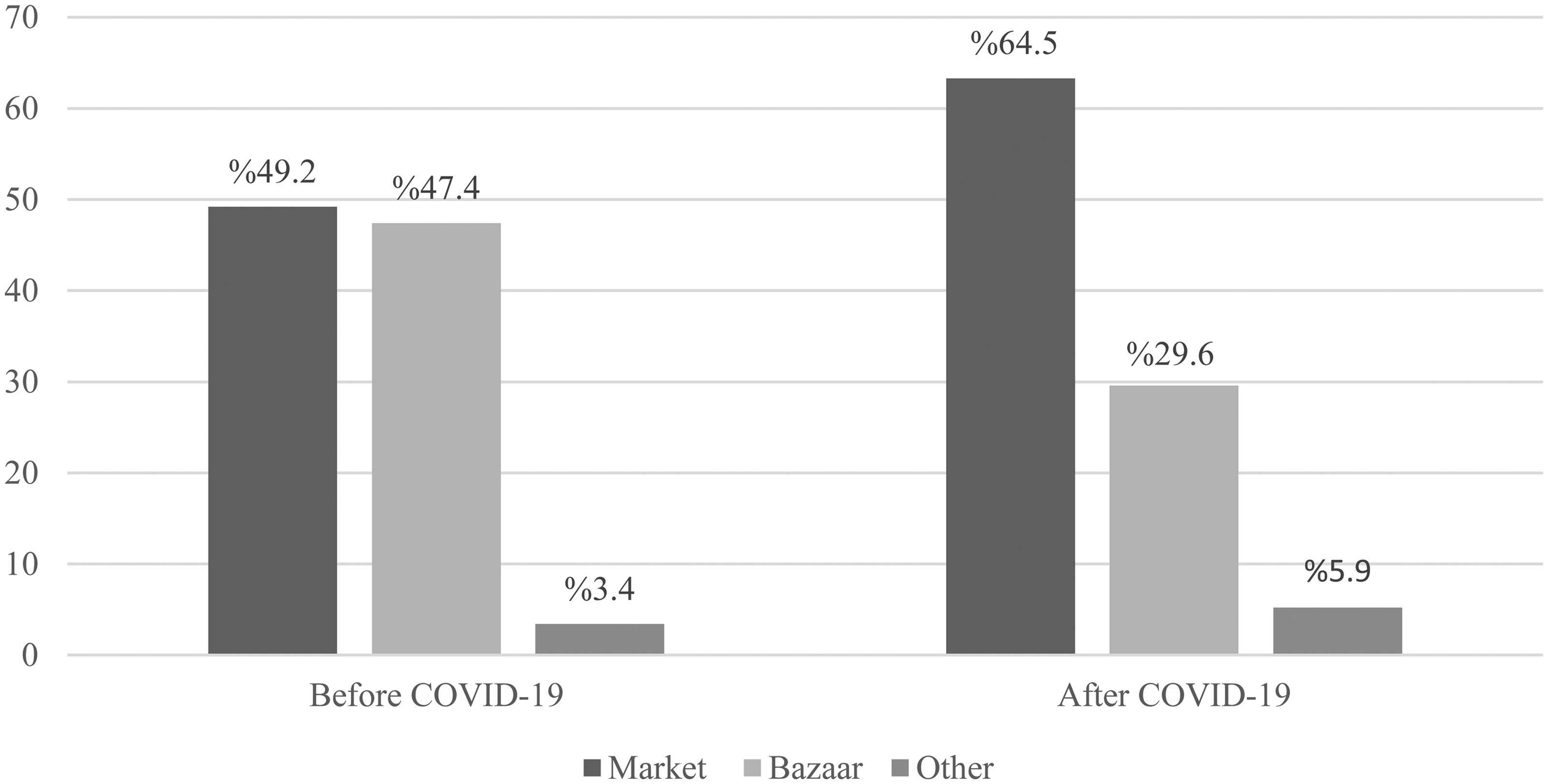
The change in fruit and vegetable shopping area before and during the COVID-19 pandemic.
The Fear of COVID-19 Scale score was the highest in individuals who reported a decrease in packaged food consumption, appetite, meal frequency, and frequency in food shopping and eating out during the COVID-19 pandemic (p < 0.05). The fear of COVID-19 Scale score of individuals who believe that the coronavirus can transmit through food packaging is higher than those who don't think (p < 0.05). Individuals who reported increased consumption of added sugar and frozen food during the COVID-19 pandemic had a higher Fear of COVID-19 Scale score (p < 0.05). The mean score of the Fear of COVID-19 Scale was higher for those who took supplements before the COVID-19 pandemic than those who never took supplements (p < 0.05). During the COVID-19 pandemic, individuals who reported an increase in appetite and meal frequency had significantly higher negative EAQ scores. It was observed that those who reported no change in added sugar consumption had higher negative EAQ scores compared to those who reported a decrease. We found that those who reported an increase in added sugar consumption and food shopping frequency had significantly higher positive Emotional Appetite Questionnaire (EAQ) scores compared to those who reported no change (Table 3).
The means of scores of the scales to the dietary habits of healthcare professionals.
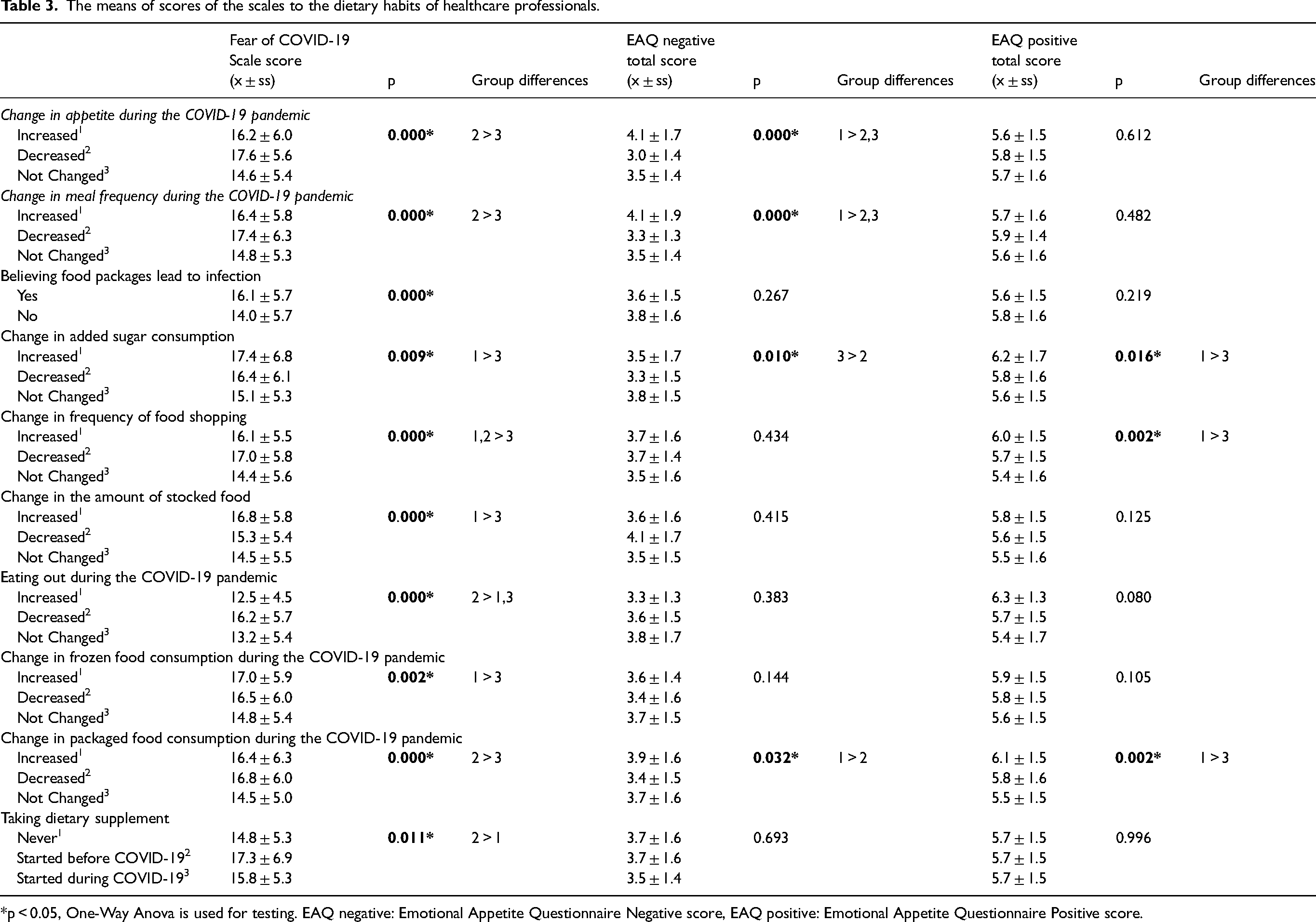
*p < 0.05, One-Way Anova is used for testing. EAQ negative: Emotional Appetite Questionnaire Negative score, EAQ positive: Emotional Appetite Questionnaire Positive score.
There was a positively significant correlation between the Fear of COVID-19 Scale score and EAQ positive-negative emotional total scores of participating female individuals (p < 0.05). Furthermore, there was a positive correlation between BMI and positive emotional appetite scores of male participants (p < 0.05) (Table 4).
The relation between the emotional appetite scale score and BMI and the fear of COVID-19 scale score.
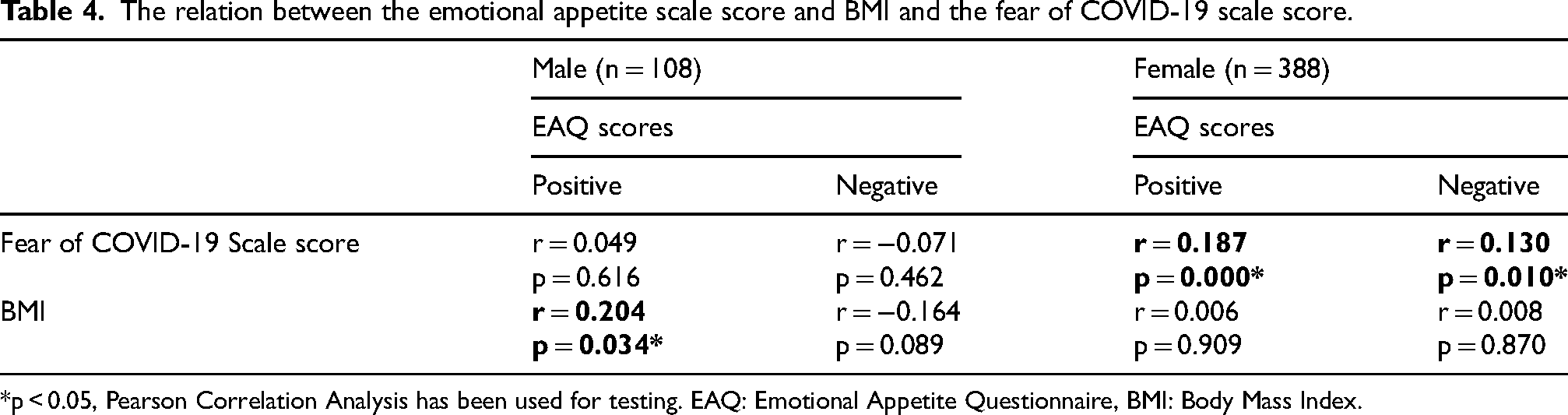
*p < 0.05, Pearson Correlation Analysis has been used for testing. EAQ: Emotional Appetite Questionnaire, BMI: Body Mass Index.
The result of logistic regression analyses suggested that men had a 2.3-fold higher risk of positive emotional appetite than women [95% confidence interval (CI): 1.4–3.7]. Participants having high COVID-19 fear had a 2.2-fold higher risk of positive emotional appetite than others. These results remained significant after adjusting for age. Regarding the relationship between BMI and emotional appetite, no significant association was observed in the unadjusted model. However, when age was included as a confounding factor in model 1, the relationship between BMI and positive emotional appetite became significant (OR: 1.4; 95% CI:1.0–2.1) (Table 5).
Multivariable logistic regression models using score of positive emotional appetite.
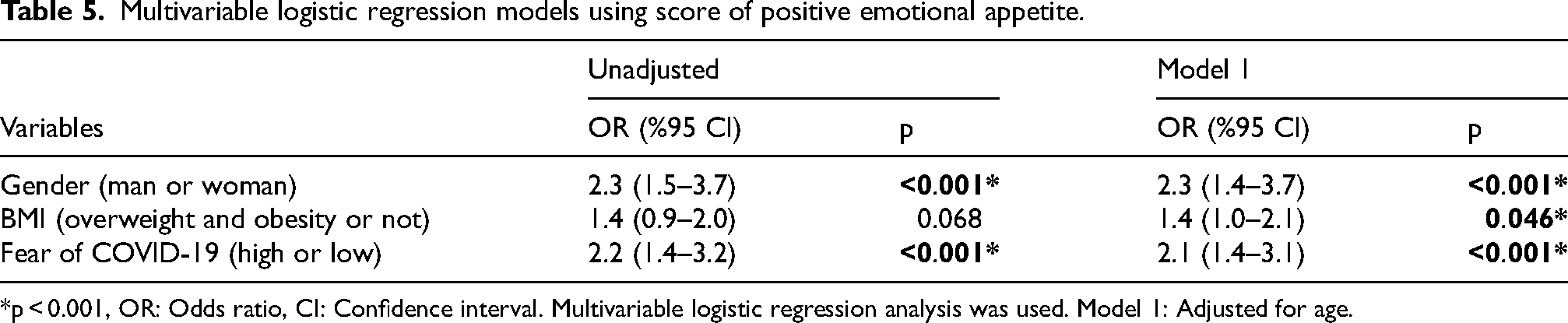
*p < 0.001, OR: Odds ratio, CI: Confidence interval. Multivariable logistic regression analysis was used. Model 1: Adjusted for age.
Discussion
This study aims to determine the coronavirus-related fear levels of healthcare professionals, compare the fear of coronavirus between genders, and investigate the effect of coronavirus fear on individuals’ emotional appetite levels and dietary habits. To the best of our knowledge, this is the first study to investigate the relationship between fear of COVID-19 and emotional appetite among healthcare professionals working in any healthcare facility in Turkey during the COVID-19 pandemic.
Fear has been one of the most common psychological reactions in the general population during the COVID-19 pandemic. 3 In addition to their fears about COVID-19, healthcare professionals have intensely experienced the concern of transmitting the disease to their family members. 22 Moreover, the main risk groups for the COVID-19 outbreak are the elder and individuals with chronic diseases. 23 Hence, at the beginning of this study, we predicted that the fear of COVID-19 is higher among healthcare professionals having children and elderly individuals in their homes. However, contrary to expectations, it has been determined that the fear of coronavirus is not significantly different from the status of healthcare professionals having children under age 18 and individuals over age 65 in their residences. It may be because many healthcare professionals isolate themselves from their families during the COVID-19 pandemic. Additionally, we found that fear of coronavirus was higher in female healthcare professionals than in males (p < 0.05). In other similar studies, the fear of COVID-19 varies according to gender and is higher in women than in men.24,25 In a study conducted with nurses, during the COVID-19 pandemic, it was reported that women had a significantly lower level of resilience than men. 26 In addition, in the current study, the fear of COVID-19 is significantly diverse according to occupation. Dietitians and nurses have higher COVID-19 fear than other healthcare professionals (doctor and EMT/paramedic) (p < 0.05). It seems to be because most of these occupational groups are female. Supporting this prediction, it was reported that the level of COVID-19 anxiety was higher in healthcare workers and women in Turkey. 27 In addition, the necessity of nurses to have more intensive contact with patients diagnosed with COVID-19 within the scope of occupational practices may be one of the important factors that increase the level of fear in this group. 6
Another purpose of this article was to examine the impact of the fear experienced during the COVID-19 pandemic on the dietary habits of healthcare professionals. During the COVID-19 pandemic, 83.3% of healthcare professionals decreased frequency of eating outside, and 24.4% increased the meal frequency in a day. Similarly, some studies reported the relationship between fear, anxiety, stress due to the COVID-19 epidemic, and the frequency of meals.28,29 The current study found that 33.5% of healthcare professionals reported an increase in the frequency of grocery shopping, while 24.6% reported a decrease. The shopping frequency decreased during the COVID-19 quarantine period in Poland, Austria, and the United Kingdom. 2 It may be because the countries and groups examined are different, and data is not about food shopping frequency during the quarantine period in the current study. The food shopping frequency may have decreased due to the thought that markets will be risky in terms of contamination, warnings for social distance, and the decrease in individual purchasing power due to economic losses during the COVID-19 pandemic. 30 In addition, one of the changes in the shopping routines of individuals was the panic-stocking of food products such as bread and pasta during the pandemic. 31 In this study, 47.8% of healthcare professionals reported that they increased the amount of food stocked during the COVID-19 pandemic. Such a result may have arisen due to disruptions in food supply and difficulties in reaching food during the quarantine. 30 COVID-19 epidemic may affect individuals not only in terms of the epidemic but also by changing their lifestyles.
The fact that there is no definite cure for coronavirus has made individuals perform actions that would enhance their immune systems. 32 20.6% of healthcare professionals reported that they started taking dietary supplements before the coronavirus period, and 34.9% started during the COVID-19 pandemic. Similarly, in a study examining the change in dietary habits after the coronavirus epidemic in adults, 36.1% of individuals began to take dietary supplements after COVID-19. 33 In addition, Ural et al. 32 also reported that 26.7% of young adults began to take dietary supplements during the COVID-19 pandemic. Healthcare professionals often had to come into contact with patients without adequate personal protective equipment during the onset of the COVID-19 pandemic. Vukovic et al. 34 reported that participants using more dietary supplements also had higher levels of coronavirus fear. Hence, we thought that fear of coronavirus might encourage the use of dietary supplements. Good nutrition is too substantial during and after infection, and the organism needs extra energy and nutrients. That's why it's so substantially to maintain a healthy diet during the COVID-19 pandemic. However, any food or dietary supplement alone cannot prevent COVID-19 infection. In addition to a healthy diet, other healthy lifestyles as not smoking, exercising regularly, getting enough sleep, and minimizing stress, should be kept in mind for a robust immune system. 35
Negative emotions such as depression, stress, and anxiety can increase food intake, but also, they may have a contrary effect and decrease it in some cases. 36 Macit 33 conducted a study on 341 adults aged 18–65 and reported that individuals experienced an average of 1.0 ± 1.5 kg body weight gain during the COVID-19 pandemic. In the current study, during the COVID-19 pandemic, 32.3% of healthcare professionals reported that their body weight increased, and 16.9% reported a decrease. In addition, the risk of positive emotional appetite was 2.2 times higher in participants with high COVID-19 fear than in others (OR: 2.2; 95% CI:1.4–3.2). Moreover, the total COVID-19 anxiety score was positively correlated with the negative EAQ scores among women. The Fear of Accordingly, negative emotions such as stress, anxiety, and fear experienced during the pandemic may affect the appetite levels of individuals and cause a change in body weight. This finding may be substantial for optimizing health and healthy body weight in unusual situations.
In the current study, nearly half of the healthcare professionals reported that their appetites changed during the coronavirus pandemic (18.2% reported a decrease, and 30% reported an increase). Similarly, Owen et al. 37 found that 53.6% of Australian adults were disturbed by anorexia or overeating during the coronavirus pandemic. Experiencing positive and negative emotions can affect the appetite level of individuals. 38 Appetite changes are responses to the biological process of the organism to cope with stress. 39 The coronavirus fear of healthcare professionals who reported a decreased appetite during the COVID-19 pandemic was significantly higher than healthcare professionals who did not experience any appetite changes (p < 0.05). In addition, the negative emotional appetite score, who reported that their appetite increased during the COVID-19 pandemic, is significantly higher than the others. In a study examining the relationship between negative emotions and food consumption, people in a negative emotion consumed more food than people in a positive emotion. 40
As a result of logistic regression analysis, we found that overweight and obese individuals had a 2.3 times higher risk of positive emotional appetite than others. Studies on this subject have shown a similar relationship between emotional appetite and BMI.38,41 This relationship between BMI and emotional appetite is not confusing, as emotional eaters tend to front energy-dense, high-fat foods to cope with their emotions.38,42 A significant number of individuals have reported an increase in body weight during the pandemic. In addition, emotion management should be considered in obesity prevention and treatment strategies since obese individuals have a higher risk of contracting COVID-19, hospitalization, morbidity, and mortality risk. 43
Strengths and limitations
Most of the participants are doctors and nurses working in the emergency room, who are the first and most intense contact with patients with COVID-19 or at risk was the strongest aspect of this study. Another strength is that healthcare professionals from 63 cities in Turkey were included in this study, whereas similar studies are generally single-centered. In addition, since this study was carried out at the end of the complete closure period (March-June 2020) implemented in Turkey, it includes up-to-date and realistic data.
The emotional states, body weight, and height based on personal statements are the most crucial limitation of this study. The low number of male professionals can also be considered as a limitation.
Conclusions
In conclusion, the restrictions during the pandemic, fear, worry, and panic induced by the disease may impact dietary habits. Nutrition is a basic physiological need for this group to maintain health care, which must be maintained even under limited conditions, and to protect their own health. Unlike the rest of society, health professionals work for longer hours during the pandemic, natural disasters, and other similar extraordinary events. Special attention should be paid to the nutritional needs and mood of health care professionals, especially under unusual conditions. It is crucial for the physical and mental health of this group to ensure positive measures in organizing mealtimes, facilitating access to food, maintaining food hygiene, and providing healthy food during emergencies. In addition, considering that unhealthy foods are generally preferred in negative emotional states, special recommendations and practices should be developed for health professionals in unusual conditions such as pandemics in terms of body weight control. Preventive and remedial measures should be implemented to prevent, mitigate, and address negative emotional states caused by extraordinary situations. Psychotherapy support should be offered to individuals who are intensely affected by negative emotional states.
Footnotes
Acknowledgments
The authors want to thank the health care workers that participated in this study and for their work during the COVID-19 pandemic.
Ethical approval
This study protocol was approved by the Çankırı Karatekin University Ethics Committee (Meeting no:16).
Informed consent
Informed consent was obtained from all participants prior to their participation in the study.
Author contributions
FT was responsible for designing the research protocol, writing the protocol and report, conducting the search, extracting and analysing data, interpreting results, updating reference lists and creating ‘Summary of findings’ tables. SB was responsible for designing the research protocol and screening potentially eligible studies. She contributed to writing the report, extracting and analysing data, interpreting results and creating ‘Summary of findings’ tables.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.