
Abstract
Background
Musculoskeletal disorders (MSD) are work-related injuries that can impact the movement or function of the human body's musculoskeletal system.
Objective
This study aims to assess musculoskeletal disorders and ergonomic risk factors (awkward posture and repetitive motions) among laboratory workers.
Methods
49 laboratory workers were assessed in this cross-sectional study. MSD prevalence was evaluated using the Cornell Musculoskeletal Discomfort Questionnaire (CMDQ). Awkward posture was assessed with the Rapid Upper Limb Assessment (RULA) approach, and repetitive motion was evaluated using the Assessment of Repetitive Tasks (ART) Tools. The data was analysed using SPSS Version 26.0.
Results
MSDs were most prevalent in the neck (91.8%), followed by the left shoulder (87.5%), right shoulder (85.7%), and lower back (85.7%) in the past week. The level of ergonomic risk for awkward posture is high risk (RULA score = 7), although most repetitive motion tasks indicate low risk (ART score <11). There is a significant correlation between the frequency of MSD and risk factors such age, gender, and shift employment.
Conclusions
It is recommended to implement ergonomic approaches, such as modifying workstations to promote good body postures during jobs, to decrease the likelihood of musculoskeletal problems among laboratory workers.
Introduction
Musculoskeletal disorders (MSD) are injuries that can impact the movement of the human body or the musculoskeletal system, which includes muscles, tendons, ligaments, nerve cells, spinal discs, and blood vessels.1,2 1.71 billion people worldwide suffer from musculoskeletal disorders (MSDs), mainly characterised by chronic pain that restricts movement, flexibility, and skeletal muscle performance, thus impacting their work capacity. 3 In 2022, the Department of Occupational Safety and Health (DOSH) reported 678 incidents of industrial accidents and musculoskeletal ailments, which is higher than the 201 cases recorded in 2021. 4
Laboratory workers who conduct tests and analyses on patient fluids and tissues to provide diagnostic information to physicians are a crucial part of the medical workforce. 5 The workers spend the most of their work hours seated at a microscope, utilising pipettes, and examining clinical samples. Despite their critical role, the risk factors for MSDs among laboratory workers have been relatively underexplored compared to other healthcare professionals such as nurses, surgeons, and dentists.6–8 Most existing studies on laboratory workers have concentrated on chemical and biological hazards, with ergonomic risks and musculoskeletal diseases receiving less attention. 9 The immediate and observable impacts of chemical and biological dangers often overshadow the insidious nature of ergonomic hazards, which may take years to manifest as symptoms.
MSDs in laboratory workers are commonly associated with conditions affecting the neck, wrists, shoulders, arms, lower back, and legs.8,10–12 Laboratory tasks like pipetting require repetitive hand movements, which could lead to cumulative trauma disorders if not properly managed. 13 The risk of musculoskeletal discomfort and injury may be increased by the lengthy periods of awkward posture that are frequently associated with microscope use, including static hand positions and neck flexion. 14 Studies indicate a high prevalence of MSDs among laboratory workers, with rates of 84.5% in Spain, 82% in Saudi Arabia, 77.1% in Oman, and up to 90% in parts of Pakistan.8,10,11
The demands of laboratory work, including prolonged sitting or standing and repetitive motions such as pipetting and microscope use, place significant strain on the musculoskeletal system. For instance, the necessity to maintain a forward-leaning posture while performing pipetting tasks can result in pressure on the neck, shoulders, and lower back.13,15 In addition, everyday use of microscopes sometimes involves adopting uncomfortable neck and wrist positions in order to get the best viewing angles. This can lead to musculoskeletal discomfort and strain over time. 16 The repetitive nature of thumb movements during pipetting tasks may increase the likelihood of hand and wrist injuries, such as repetitive strain injuries (RSIs), especially if ergonomic guidelines are not adhered to.14,15 Furthermore, the repetitive manipulation of microscope settings necessitates precise hand and finger motions, which may result in hand-arm disorders (HADs) if appropriate ergonomic practices are not followed. 17 A survey revealed that 97% of medical laboratory workers are dissatisfied with the use of manual pipettes for more than four hours a day, 2 highlighting the increased risk of developing conditions like Carpal Tunnel Syndrome due to sustained pressure on the fingers. 11 Additionally, prolonged microscope use can exacerbate ergonomic issues by forcing workers into uncomfortable postures that lack proper support, leading to pain in the head, neck, shoulders, waist, and back.5,7,18
There is a significant research gap in the comprehensive investigation of ergonomic risks associated with laboratory tasks such as pipetting, microscope use, and equipment handling, and their direct correlation with MSDs among laboratory workers. This study aims to address this gap by examining the relationship between the prevalence of MSDs and the level of ergonomic risk factors specifically awkward postures and repetitive motion among laboratory workers. By conducting an investigation on MSDs and ergonomics risk factors among laboratory workers can provide insights into how ergonomic variables contribute to MSDs. This, in turn, allows organisations to take proactive actions to lower injury rates among laboratory workers. This encompasses the creation of equipment and processes that reduce physical and mental stress and exhaustion. 16 Moreover, creating comfortable and safe work environments can enhance employee satisfaction and productivity while reducing absenteeism due to work-related injuries.14,19,20
Methodology
Participant
The research design was a cross sectional study conducted in a medical laboratory in Kuala Lumpur. There are 49 laboratory workers were selected based on the inclusion criteria that responders must have a minimum of three months of working experience in the laboratory. Respondents in this study will be disqualified if they have been diagnosed with musculoskeletal problems. The medical laboratory consists of six (6) sections which are Integrated Diagnostic Laboratory (IDL), microbiology, histopathology, cytopathology, Research Business Center, and Molecular Diagnostic Laboratory (MDL). IDL involves laboratory workers conducting tests on blood, urine, triglycerides, and other body substances to detect diseases or mutations. This is crucial for diagnosing the presence of diseases such as hepatitis and tuberculosis.
Various tests are conducted on specimens to observe their response to different treatments. Microbiology laboratories are facilities dedicated to the cultivation, analysis, and identification of microorganisms, such as yeast, fungi, and bacteria. 21 Histopathology laboratories examine diseased tissues and cells to perform prognostic or diagnostic tests for various diseases, including cancer and various organ diseases. Cytopathology laboratories use microscopic analysis to diagnose malignant or pre-malignant diseases. RBC laboratory serves as a central location for gathering samples from the hospital, which are then divided and dispatched to the appropriate laboratories for analysis. MDL laboratory specialises in developing, optimising, validating, implementing, and troubleshooting novel nucleic acid-based diagnostic assays for infectious diseases.
Several tasks involving awkward posture and repetitive motion were observed, including using the microscope, transferring data into the computer, taking photos, grossing, and pipetting. Observing microscopes demand individuals to examine various samples and cases based on specific tasks, often necessitating longer periods of sitting. Transferring data from agar plates to this computer requires observers to analyse the bacteria's response to antibiotics by measuring the inhibition zones on agar plates. During the photo component, the workers must use a camera to snap pictures of samples while standing for an extended period. Grossing requires the worker to cut, measure, and collect specific tissue samples. Five workers were observed engaging in repetitive motion by often using single-channel micropipettes throughout the workday.
Sample size
To calculate the sample size needed to collect for the questionnaire, reliable sample size formula from known population is being used.
22

The calculated estimation of sample size is as follow:



Data collection and procedure
A questionnaire in a printed form was distributed to the laboratory workers. A questionnaire consisting of three sections was distributed physically to the 49 respondents. Section A was about socio-demographic data, lifestyle, and health conditions. Meanwhile, section B consists of working information. Section C contains questions to determine the prevalence of musculoskeletal disorders by using the Cornell Musculoskeletal Discomfort Questionnaire (CMDQ) that consists of three sections which are the frequency of pain and discomfort, level of discomfort, and the interference with the ability to work.1,23,24 The body map is used to indicate 11 body regions that experienced pain or discomfort in the past week, namely in the areas of the neck, shoulders, upper back, arms, lower back, forearms, wrists, hips/lower back, thighs, knees, and calves. The frequency of pain and discomfort was divided into five scales which are 0 (never), 1.5 (1–2 times last week), 3.5 (3–4 times last week), 5 (once every day), and 10 (several times every day). Next, the level of discomfort was divided into three scales which are 1 (slightly uncomfortable), 2 (moderately uncomfortable), and 3 (very uncomfortable). The interference was divided into three scales which are 1 (not at all), 2 (slightly interfered), and 3 (substantially interfered). The Cornell Musculoskeletal Questionnaire (CMDQ) was used for this study because it has a demonstrated record of being reliable and valid in assessing musculoskeletal disorders (MSDs) in different work environments.1,23,25 The CMDQ is specifically intended to systematically collect comprehensive data on the prevalence, severity, and impact of musculoskeletal problems among laboratory workers.6,25,26
The selection of Rapid Upper Limb Assessment (RULA) and Assessment of Repetitive Tasks (ART) over alternative ergonomic assessment approaches in this study focusses on practical principles. While tools like the Occupational Repetitive Actions (OCRA) method or the Strain Index offer detailed assessments but they demand additional time, training and resources which may not be feasible in an intensely busy laboratory environment. Despite their comprehensive nature, these alternatives lack the simplicity and quick applicability of RULA and ART, particularly when rapid evaluations are required. RULA and ART assessment tools are particularly tailored to evaluate upper limb activities and repetitive motions that making them highly suitable for addressing the primary ergonomic issues in laboratory settings. Its application guarantees a concentrated and efficient evaluation and enables specific actions to tackle the most important hazards in this setting.
Rapid Upper Limb Assessment (RULA) was decided to use due to its established advantages in terms of simplicity and effectiveness in evaluating ergonomic risks related to upper limb tasks. The reliability of RULA in assessing ergonomic risks across various industries and labour tasks27–29 has been extensively researched and validated, as demonstrated by previous studies.30,31 The RULA worksheet was utilised to assess posture, force exertion, and repetition of actions. The ultimate RULA score was categorised into four levels of musculoskeletal disorder risk. Score 1–2 indicates insignificant danger and appropriate posture. A score of 3–4 suggests low risk, requiring more investigation and maybe a change in posture. A score of 5–6 indicates medium risk, necessitating further examination and a prompt change in posture. A score of 7 indicates very high risk, requiring quick additional assessment and a change in posture.
The Assessment of Repetitive Tasks (ART) was utilised to assess the ergonomic risk level associated with repetitive movements in laboratory personnel. This specificity enables an intensive evaluation of tasks that are recognised to contribute to musculoskeletal diseases (MSDs) in laboratory environments and may precisely identify high-risk activities and prioritise interventions to successfully mitigate these risks.2,32,33 The ART approach ensures consistency in risk assessment across various laboratory settings. This method is validated and reliable in identifying ergonomic hazards.31,34,35 It assists organisations in implementing targeted interventions to enhance workplace ergonomics and decrease the occurrence of musculoskeletal disorders (MSDs). The assessment comprises four stages: frequency and repetition, force, awkward posture, and extra considerations. The ART score was categorised into three exposure levels: 0–11 (low), 12–21 (mid), and 22 or higher (high), necessitating immediate additional scrutiny.
The data was analysed using SPSS version 26. Descriptive statistics were utilised to assess the frequency of musculoskeletal diseases and the extent of ergonomic risk factors (awkward posture and repetitive motion) in laboratory personnel. Spearman's rho was utilised to establish the correlation between the occurrence of musculoskeletal illnesses and several characteristics evaluated among laboratory workers. Authorization was requested and granted for data collection at the laboratory. The researchers were allowed to gather data for a duration of around seven days, specifically during their designated working hours. Furthermore, this work has obtained approval from the Research Ethics Committee.
Results and discussions
In this study, the sample population consisted of 49 respondents with 87.8% (n = 43) being female and 12.2% (n = 6) male. The age range of respondents was between 23 and 40 years with a mean age of 28.6 years (±4.01). A majority (69.4%, n = 34) were aged between 21 and 30 years. A significant portion of respondents (77.6%, n = 38) worked in shifts. The socio-demographic data are presented in Table 1.
Distribution of socio-demographic (n = 49).
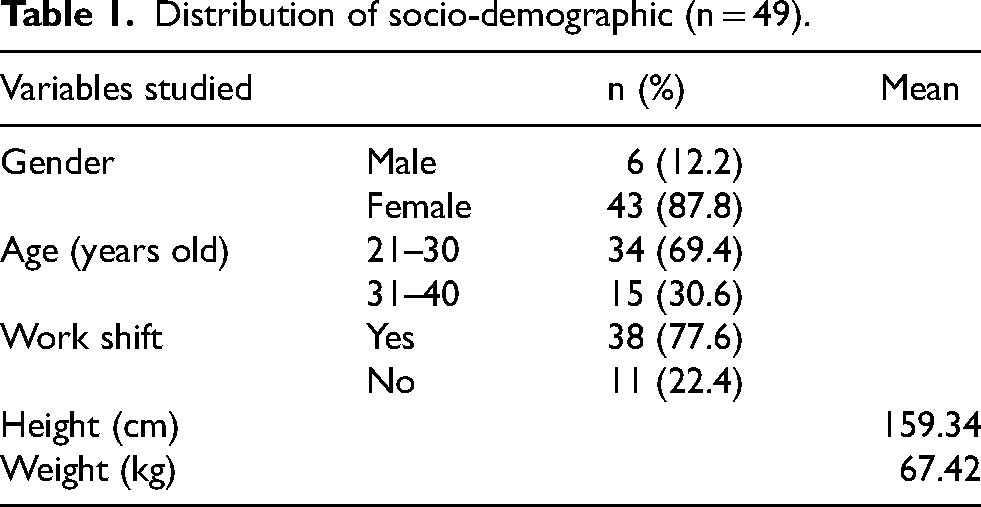
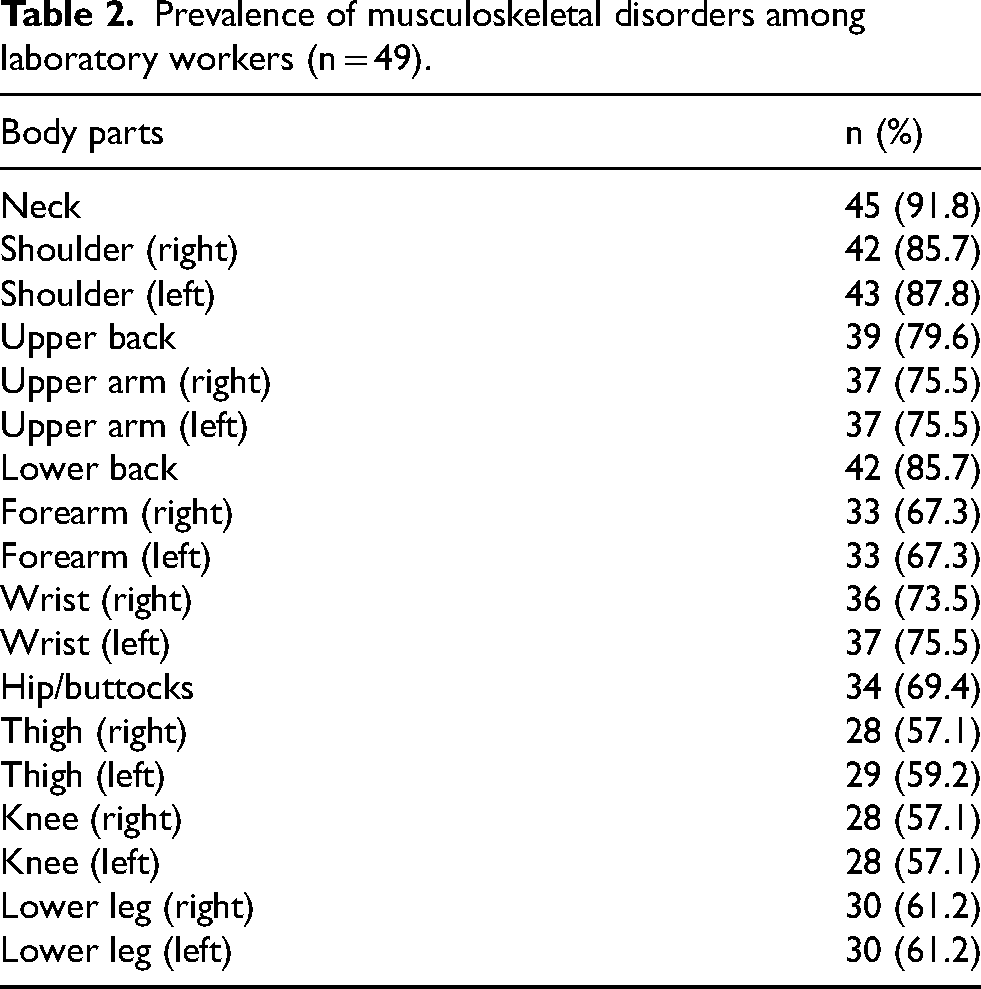
Table 2 shows the prevalence of musculoskeletal disorders among laboratory workers. The results of the Cornell Musculoskeletal Discomfort Questionnaire (CMDQ) revealed that the neck region had the highest prevalence (91.8%), followed by the left shoulder (87.8%), right shoulder (85.7%), and lower back (85.7%). Additionally, 79.6% of respondents reported discomfort in the upper back, with similar percentages observed for both arms and wrists, ranging between 73.5% and 75.5%. Other areas, such as the calves, thighs, and knees, also showed significant levels of discomfort, with a prevalence rate above 57%.
Prevalence of musculoskeletal disorders among laboratory workers (n = 49).
The high prevalence of neck discomfort could be attributed to prolonged non-neutral neck positions, such as forward bending or looking upward. These postures overactivated neck and upper back muscles leading to fatigue and discomfort. Prolonged tension in these muscles restricts blood flow, reducing oxygen supply and contributing to muscle stiffness and pain.36,37 These findings align with previous research on laboratory workers in Indonesia and Germany, which found similar patterns of neck, shoulder, and back discomfort.11,38 The study further supports evidence that laboratory tasks, including microscope use, often require workers to maintain awkward postures for extended periods, leading to MSDs. 9
Shoulder discomfort was also prevalent among respondents, with 87.8% reporting left shoulder pain and 85.7% reporting right shoulder pain. 6 This work task creates a risk because it involves prolonged and continuous holding of the arms and shoulders in static positions. This can produce strain on the shoulder joints, resulting in higher pressure on the joint surfaces and surrounding structures. Consequently, it cause the joint pain and discomfort, particularly in individuals who do not have adequate rest periods to allow for joint recovery. 36 The repetitive nature of laboratory tasks without sufficient breaks increases the risk of overuse injuries to the muscles, tendons, and ligaments surrounding the shoulder.
Lower back discomfort was reported by 85.7% of respondents that reflecting the strain on muscles such as the erector spinae and quadratus lumborum, which support prolonged poor postures. This can also be exacerbated by workers slouching or sitting with an excessively bent lower back (lordosis), which causes strain on the spinal discs and vertebrae. This pressure can cause compression of the spinal nerves, resulting in pain and discomfort.37,39 These findings are consistent with research indicating that static postures and repetitive upper limb movements contribute to significant fatigue and discomfort in laboratory workers.2,9
Table 3 summarizes the ergonomic risk levels for awkward postures, with microscope use and photo section activities showing the highest Rapid Upper Limb Assessment (RULA) scores of 7, indicating a need for intervention. Poor workstation design particularly the lack of anthropometric adjustments for microscope use, forces laboratory workers into “pathological stooping” postures that further exacerbating MSD risks. Similarly, photo section tasks require prolonged static postures, such as standing and bending, which lead to elevated shoulder strain and discomfort.
Level of ergonomics risk for awkward posture among laboratory workers.
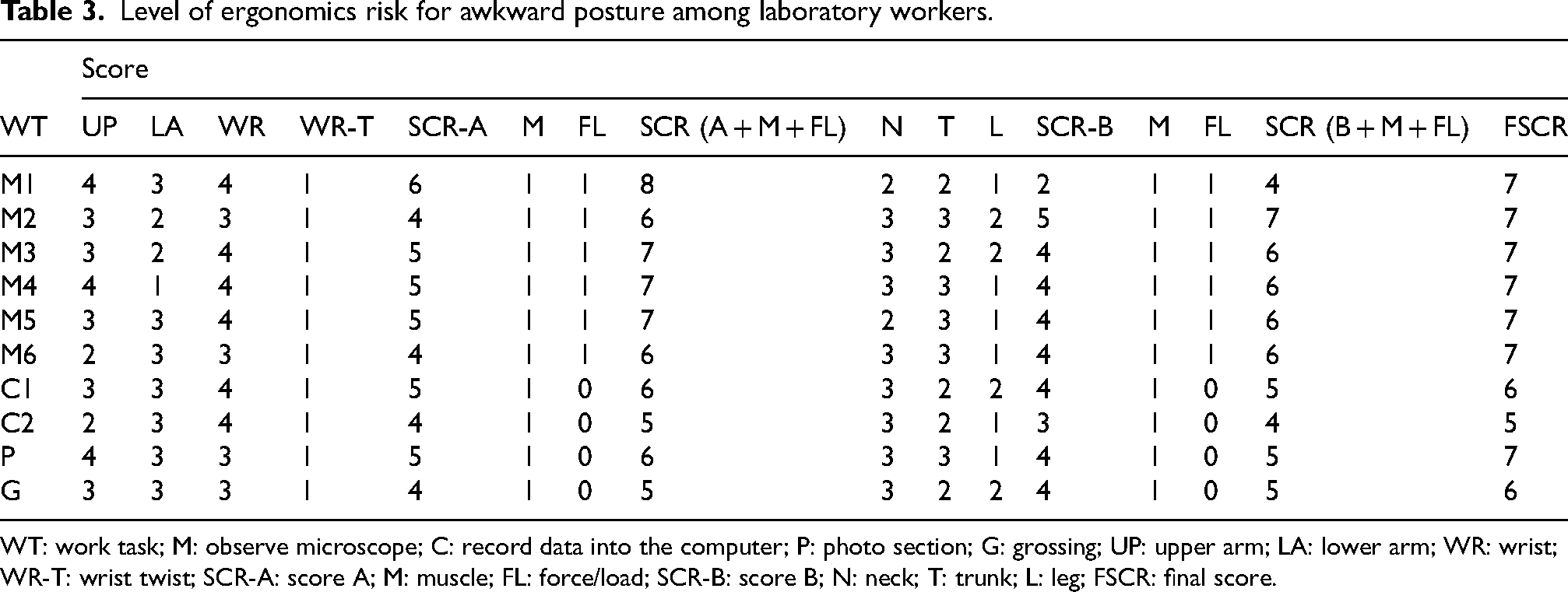
WT: work task; M: observe microscope; C: record data into the computer; P: photo section; G: grossing; UP: upper arm; LA: lower arm; WR: wrist; WR-T: wrist twist; SCR-A: score A; M: muscle; FL: force/load; SCR-B: score B; N: neck; T: trunk; L: leg; FSCR: final score.
Overall, the study results for the risk factors of awkward postures indicate a high level of risk when observing the microscope and grossing. This indicates that the body positions while observing the microscope for six respondents are approximately the same. Some studies suggest that commonly used microscopes in laboratories are not optimized and do not provide a neutral sitting position, requiring pathologists to bend forward, resulting in a posture referred to as ‘pathological stooping’. 32 The use of microscopes also requires respondents to repeat thousands of wrist and hand movements throughout the day, typically involving back and extended neck flexion, elevated shoulders, elbow abduction, and awkward wrist and hand postures. 2 To prevent this, clinical microscopes should be adjustable to meet user needs, allowing them to adjust the microscope's height, choose eyepieces and viewing angles, place their hands and arms on the workbench, and strive for a symmetrical position with aligned shoulders.
The photo section recorded a high RULA score of 7. This activity requires respondents to stand statically for a prolonged period to capture sample pictures. Through observation, the posture of respondents is seen bending at the neck and lower back, with elevated shoulders. The high RULA score results from the workstation not being designed with the user's anthropometric measurements, which could lead the worker into awkward postures. For example, a desk that is too high or too low can cause excessive upper-limb reaching or bending, resulting in muscle tension and exhaustion. 40 Meanwhile, grossing activity scored 6, indicating the need for further investigation and changes. Besides improper body posture, the placement of areas and workstations can also contribute to musculoskeletal disorders. For example, laboratory workers may be forced to work in awkward positions due to the height of the workstation used to handle samples, including raising their hands or excessively bending their wrists, which can cause discomfort and eventually contribute to musculoskeletal problems. 33
In terms of repetitive motion, Table 4 shows that pipetting on the right arm yielded the highest score (9.5), indicating moderate ergonomic risk. Performing a pipetting activity requires accurate and repetitive movements of the fingers and muscles in the hand. Due to the relatively small and delicate nature of finger muscles compared to bigger muscle groups, there is a significant risk of muscle fatigue. According to prior research, nine muscles are involved in generating force during pipetting, with the abductor pollicis brevis (APB) exhibiting the highest level of force. Inexperienced users of pipettes may exert excessive lateral force on the push button and experience relative sliding of the pipette in their hand while pipetting. These factors also contribute to the variability in muscle forces. 41
Level of ergonomics risk for repetitive motion among laboratory workers.
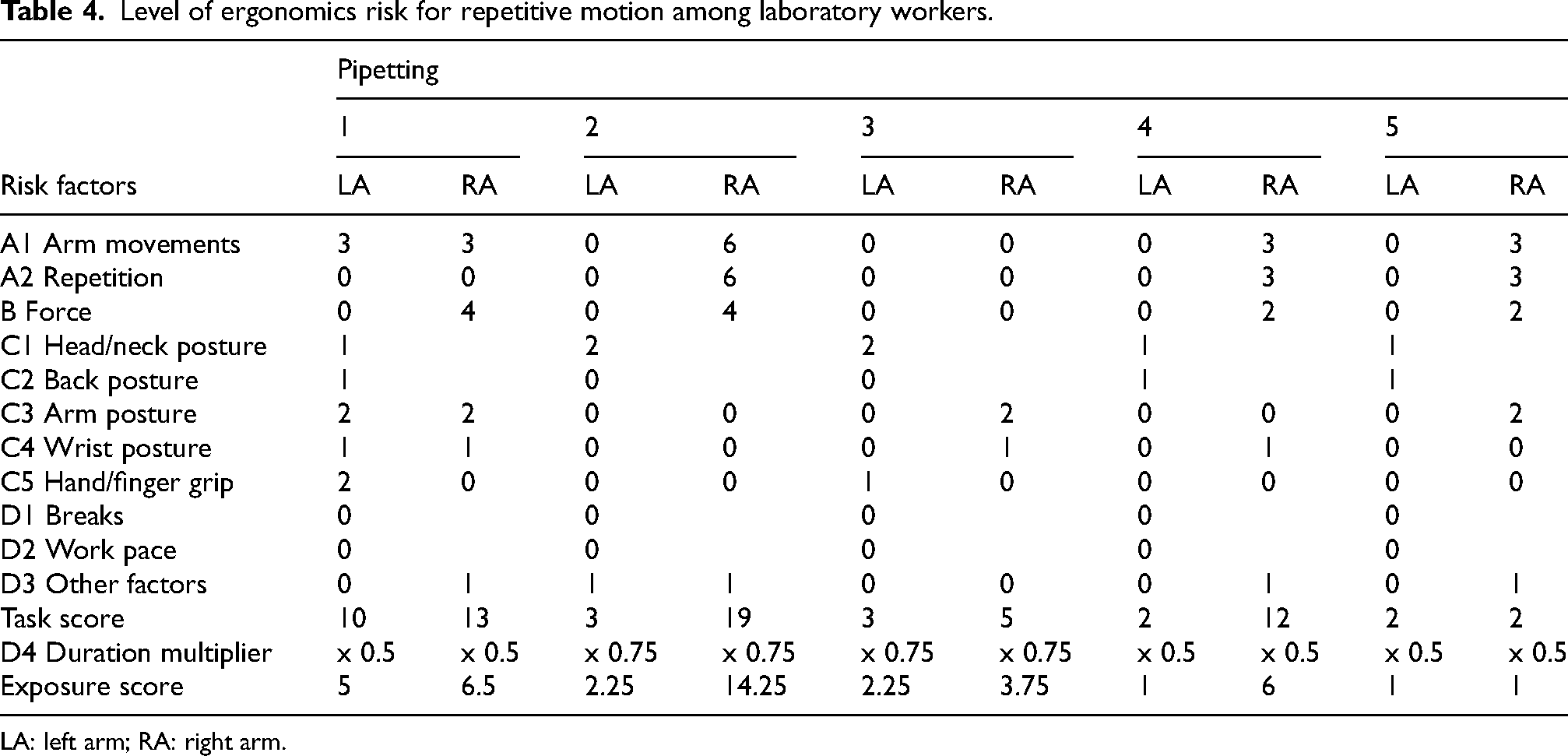
LA: left arm; RA: right arm.
The observations made for repetitive motion factors recorded a final Assessment of Repetitive Tasks (ART) score of less than 11 overall. This indicates a low level of exposure risk. However, individual circumstances should be taken into account. Nevertheless, the study results for the use of pipet 2 found that the exposure risk level for the right arm was high with a score of 14.25 compared to the use of other pipets. The significant difference in scores is in the repetition score, where the same movement pattern is repeated more than 20 times per minute compared to the use of other pipets. Pipetting activities involve various ergonomic pressure points, including the shoulders, arms, and wrists. This pressure is mostly due to excessive thumb force, repetition, and awkward postures. Moreover, it was found that individuals have a higher chance of developing MSD, especially when their work requires significant manual effort and involves long working hours. 1 Several practices can be adopted to reduce ergonomic hazards in pipetting. Among them is ensuring a comfortable pipet grip, and using an electronic pipette with mixing features for operations like mixing or dispensing. This can reduce the need for repetitive movements and excessive force on the thumb. Additionally, ergonomic solutions, such as adjustable pipettes or multi-channel pipettes, could mitigate these risks by reducing repetitive strain on hand and thumb muscles.
A significant finding, as shown in Table 5, is the negative correlation between total RULA scores and height, r(49)=−0.385, (p < 0.01). This suggests that taller individuals may adopt more extended postures, leading to lower ergonomic risk scores. The influence of anthropometric characteristics, such as height, on ergonomic risk levels is critical in designing workplace interventions tailored to individual worker needs. 42 Individuals with greater height may encounter difficulties or advantages in completing tasks due to ergonomic design factors.
Relationship between level of ergonomics risk for awkward posture and variables studied among laboratory workers.

N = 49.
*p-value is significant at p ≤ 0.05.
**p-value is highly significant at p < 0.01.
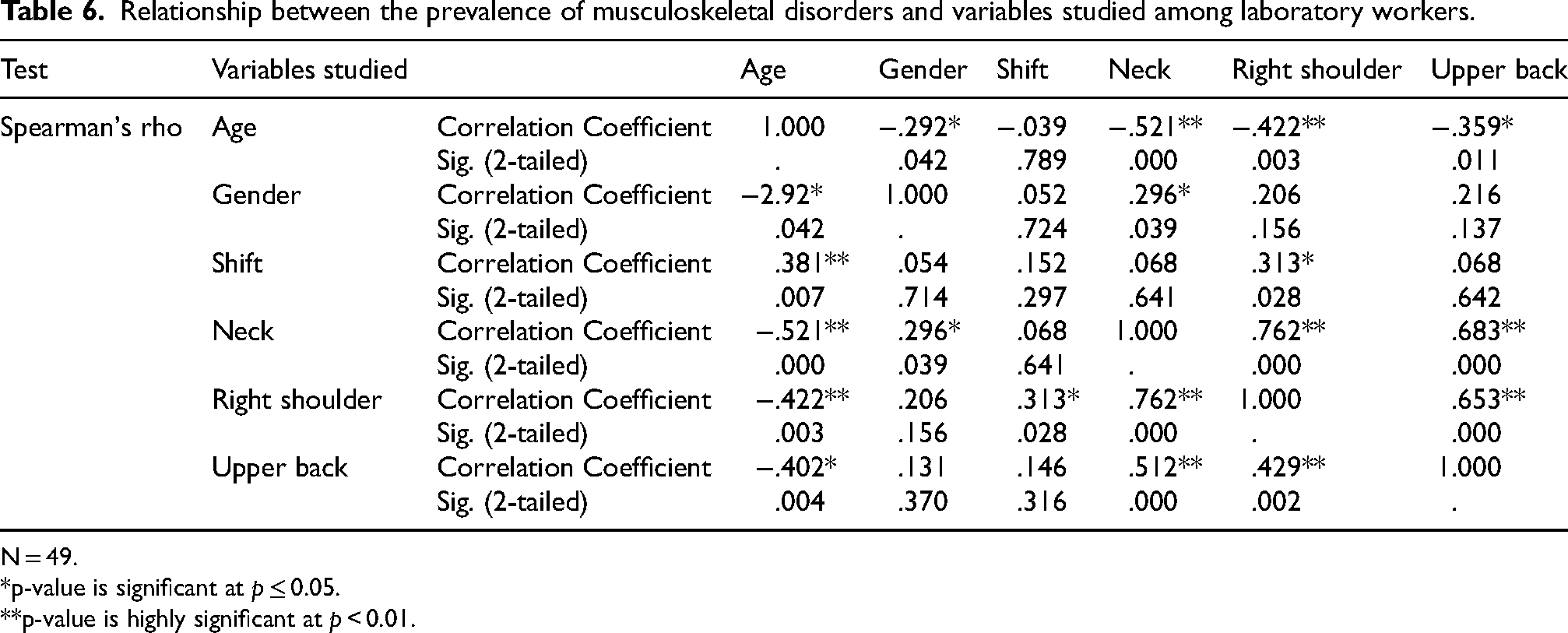
Table 6 further revealed significant correlations between age and musculoskeletal discomfort in specific body regions, including the neck(r (49) = 0.521, (p < 0.01), right shoulder (r(49) = 0.422, p < 0.01) and lower back (r(49) = 0.402, p < 0.05). Additionally, a weak positive correlation was observed between shift work and right shoulder discomfort (r(49) = 0.313, p < 0.05). Gender was also significantly correlated with neck discomfort (r(49) = 0.296, p < 0.05), suggesting that anatomical and physiological differences between men and women influence the development of MSDs. The study found that gender factors show a significant relationship with the prevalence of musculoskeletal disorders (MSD) in the neck. This finding is consistent with previous study that showed a significant relationship between gender and MSD. 43 The development of MSDs might be influenced by the anatomical and physiological differences between men and women. Women typically have smaller and more narrow shoulders in comparison to men, which can potentially impact their ability to bear the weight of their heads and sustain proper posture. 44 Furthermore, hormonal variations, including those associated with reproductive cycles in females, might impact muscular tension and susceptibility to pain. The hormonal changes can potentially lead to a higher vulnerability to musculoskeletal discomfort, such as neck pain. 45 Women are more likely to experience MSD symptoms more frequently, 46 with the prevalence of neck issues being twice as high as that of men. One possible explanation for the higher prevalence of musculoskeletal disorders (MSD) among female laboratory workers is the biological differences between men and womenThe prevalence of MSD can be influenced by gender, as women usually have smaller bodies, less muscle strength compared to men, and face physical work demands. 43
Relationship between the prevalence of musculoskeletal disorders and variables studied among laboratory workers.
N = 49.
*p-value is significant at p ≤ 0.05.
**p-value is highly significant at p < 0.01.
Age is significantly associated with the prevalence of musculoskeletal issues, particularly in the right shoulder, neck, and lower back. This association is attributed to intrinsic changes in musculoskeletal structures that occur with aging, including reductions in muscle mass, increased joint stiffness, and decreased flexibility of tendons and ligaments. These alterations can diminish an individual's ability to adapt and heighten the risk of strains and sprains in these areas. 47 The study highlights that younger workers specifically those aged 21 to 30 are at an elevated risk for musculoskeletal disorders likely due to their increased engagement in manual tasks compared to older colleagues who are often in managerial roles. 9 Conversely, older individuals may experience exacerbated musculoskeletal issues due to age-related health conditions such as arthritis or osteoporosis, which can aggravate injuries in the shoulder, neck, and lower back.11,47 Thus, ergonomic solutions should consider these age-related changes by including designs that allow the physical constraints related with ageing. For older workers, these kinds of adjustments are absolutely essential for lowering their risk of accident and raising their general ergonomic efficiency.
Shift work also shows a significant relationship with the prevalence of issues in the right shoulder. The disruption of the body's natural circadian rhythms caused by shift work leads to irregular sleep patterns and reduced sleep quality.This circadian misalignment often results in fatigue, diminished alertness, and impaired motor coordination, all of which significantly increase the risk of musculoskeletal injuries, including shoulder-related issues. 48 Additionally, specific shift work patterns, such as night shifts or rotating shifts, require workers to perform physically demanding tasks during periods when their bodies are less physiologically prepared. This mismatch between work demands and the body's natural rhythms can result in excessive physical exertion and stress, particularly in the shoulder region. 49 The present study corroborates these findings by demonstrating that respondents engaged in shift work are at a greater risk of developing MSDs compared to those working regular office hours. This is consistent with recent research highlighting a higher prevalence of musculoskeletal disorders among nurses with irregular work schedules, frequent night shifts, or a tendency to stay awake late. 50 Furthermore, recent studies have shown that nurses working in three-shift systems are more likely to suffer from MSDs compared to those on a single-shift schedule, with an incidence rate of 61.4%.51–53
Conclusion
This study highlights the significant prevalence and impact of musculoskeletal disorders (MSDs) among laboratory workers, with a particular focus on gender, age, and shift work. The high prevalence of MSDs in the neck (91.8%), left shoulder (87.8%), and lower back (85.7%.) underscores the ergonomic challenges faced by this workforce. Notably, the results indicate that female respondents are disproportionately affected by neck pain and other MSDs, potentially due to anatomical and physiological differences such as smaller shoulder widths and hormonal fluctuations. This finding is consistent with previous research linking gender differences to MSD prevalence.
However, this study is limited by the use of a small sample size, which may lead to findings that are not directly applicable to the general population due to its low representativeness. Moreover, the study's reliance on self-reported measures introduces several potential sources of bias beyond just response bias. Recall bias is particularly pertinent as participants may struggle to accurately remember or quantify the frequency and intensity of ergonomic stressors and symptoms of MSD. This can lead to both over- and under-reporting, skewing the data and potentially leading to inaccurate conclusions. The homogeneity of the study sample also presents a limitation particularly if the participants were drawn from a single institution or geographic area. It can reduce the ability to generalize findings across different laboratory environments. In this context, the influence of unexamined variables such as the specific type of laboratory work, the availability of ergonomic interventions, or institutional policies may play a significant role in shaping the results. In light of these limitations, future research should consider adopting longitudinal designs, expanding sample diversity, and incorporating both objective measures and additional variables that may influence the development of MSD. This would enhance the robustness of the findings and provide a more comprehensive understanding of the ergonomic challenges faced by laboratory workers.
In conclusion, the study revealed that laboratory workers are at a high risk to acquire awkward postures due to their posture and workstation design. Developing preventive strategies that include individualized ergonomic assessments and interventions will be essential for minimizing the risk of MSDs in laboratory settings. Further research should evaluate the effectiveness of these strategies and devise customized solutions that cater to the diverse needs of laboratory workers, considering factors such as gender, age, and anthropometric differences. It is crucial to implement appropriate interventions through comprehensive ergonomic training. This training should cover topics such as posture awareness and the significance of taking breaks to minimise prolonged exposure to ergonomic risk factors. Furthermore, to mitigate risks over time, it is essential for the company to incorporate ergonomic principles into the design of laboratory workstations. This can be achieved by including adjustable seats, workbenches, and monitors that promote neutral body positions when performing operations such as pipetting and using microscopes. The risk of repetitive movement, which was also high in this study, can be reduced by encouraging laboratory workers to use correct pipetting techniques, taking regular breaks to rest muscles and joints, as well as encouraging task rotation, which allows different muscle groups to be used and gives workers opportunities to rest and recover between tasks. Therefore, by focusing these techniques to target specific affected body regions, completing comprehensive ergonomic assessments, and taking into account individual risk factors, organisations can successfully minimise the occurrence of musculoskeletal disorders (MSDs) among laboratory workers. This strategy not only improves the health and safety of workers, but also leads to increased productivity and job satisfaction in laboratory settings.
Footnotes
Acknowledgements
With gratitude, the author would like to thank all of the study participants for their time and cooperation that enabled this study feasible.
Ethical considerations
This study was granted ethical approval by the UKM Research Ethics Committee (Approval No. JEP-2023-595). All procedures involving human participants were conducted in line with the ethical standards set by the institutional and/or national research committees.
Informed consent
Informed consent was obtained from all individual participants included in the study. Participants were fully informed about the purpose, procedures, potential risks, and benefits of the study, and they were assured that their participation was voluntary and that they could withdraw at any time without any consequences.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors acknowledge funding for Dana Mutiara from the Faculty of Health Sciences at Universiti Kebangsaan Malaysia.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.