
Abstract
Background
Percussion massage therapy (PMT) integrates traditional massage with vibration therapy.
Objective
This study compared the effects of percussion massage therapy (PMT), kinesiology tape (KT), and dynamic stretching (DS) on shoulder strength, proprioception, and functionality.
Methods
The KT group had kinesiology tape applied to the deltoid muscles. The DS group performed dynamic stretching in flexion and abduction. The PMT group received percussion massage on the deltoid muscles. Assessments included the Becure system for joint position sense (JPS), the Timed Functional Arm and Shoulder Test (TFAST), and a hand-held dynamometer for muscle strength.
Results
Significant improvements were observed in almost all JPS parameters for all groups (p < 0.05). Total TFAST scores improved in all groups. Muscle strength significantly improved in the DS group (p < 0.05), while PMT and KT groups showed no significant change (p > 0.05). Statistically significant differences were found between the groups (p < 0.05). JPS 30°, 60°, and 90° flexion parameters had effect sizes of 0.51, 0.64, and 0.49, respectively; JPS 30°, 60°, and 90° abduction parameters had effect sizes of 0.38, 0.46, and 0.45, respectively. The effect size for Total TFAST was 0.55, flexion muscle strength 0.59, and abduction muscle strength 0.68. DS was more effective for muscle strength, DS and PMT for functionality, and KT and PMT for proprioception (p < 0.017).
Conclusions
PMT and KT were more effective for proprioception, PMT and DS were more effective for functionality, and DS was most efficient in enhancing muscle strength.
Introduction
Percussion massage therapy (PMT) integrates traditional massage with vibration therapy principles and has gained popularity in clinical settings, especially among athletes. Portable, affordable PMT devices, which allow frequency, amplitude, and force adjustments, have made self-application possible and reduced therapists’ workload. PMT primarily improves the range of motion during warm-ups and aids recovery post-exercise. Despite its growing use, there is limited research on the therapy's underlying mechanisms, post-treatment effects, and impact on athletic performance. PMT uses mechanical devices powered by electricity or batteries to apply rapid compression forces to myofascial structures through various attachments. However, PMT has been extensively studied, particularly in its effects on the lower extremities.1–4 Research on its application to the upper extremities remains limited. Studies on the lower extremities have shown that PMT can acutely increase the range of motion in muscles like the gastrocnemius and hamstrings.5–7 However, the literature is inconclusive, and further research is needed to clarify its effectiveness, especially for the upper extremities.
The length of the muscle can be increased using a variety of stretching techniques. Dynamic stretching (DS) is used primarily to increase range of motion (ROM) temporarily and is conducted to improve athletic performance. It is recommended that athletes performing DS consider their ROM as the first warm-up exercise to increase countermovement jump height and agility. 8 Numerous recent studies have investigated the impact of pre-activity stretching on performance measures, particularly explosive movements, using various stretching techniques.9–11 Another study suggests that the dynamic stretching technique has a good impact on performance and flexibility parameters when conducted before an activity or sports. Consequently, many medical professionals advise performing dynamic stretches before sports. 12 Kinesiology taping, or neuro-proprioceptive taping, is widely used to improve proprioception, joint stability, and range of motion while reducing pain. Despite its common clinical use, evidence supporting its effectiveness, especially for shoulder proprioception, remains limited and inconclusive. 13 Some studies, such as those involving swimmers, show improvements in shoulder functionality. 14 While systematic reviews report mixed results and insufficient evidence for enhancing physical performance.13,15 Overall, research on kinesiology taping's effects on shoulder proprioception, muscle strength, and functionality remains controversial and of low evidence quality.
Given the lack of consensus in the literature regarding the effectiveness of kinesiology taping (KT) and percussion massage therapy (PMT), particularly for the upper extremities, our study focuses on the shoulder. We aim to compare the effects of PMT, KT, and dynamic stretching (DS) on shoulder proprioception, muscle strength, and functionality. By identifying which method is most effective for each parameter, our study seeks to fill gaps in the literature and provide new insights. While individual studies have assessed these techniques, no research has directly compared all three interventions. Additionally, to our knowledge, no study has examined PMT's effect on shoulder proprioception and functionality. We hypothesize that PMT's local vibration effect may be more effective than KT and DS in improving shoulder proprioception, muscle strength, and functionality.
Methods
Study design
This study utilized a single-blind, randomized design, with participants evenly allocated (1:1:1) into one of three groups. Participants were recruited from students at Istanbul Medipol University through a random selection process. A total of 45 healthy individuals who met the inclusion criteria were included in the research. The study adhered to the ethical standards outlined in the Declaration of Helsinki for research involving human participants. Ethical approval was obtained from the non-interventional ethics committee of Istanbul Medipol University (Approval Number: E-10840098-772.02-1948), and all participants provided written informed consent.
Participants were randomly assigned to one of three groups in this randomized controlled trial: the Percussion Massage Therapy (PMT) group, the Kinesiology Taping (KT) group, and the Dynamic Stretching (DS) group. Each participant was assigned a number according to their order of enrollment, and these numbers were used for randomization. The randomization process was carried out using the “randomizer.org” website, where the 45 participant numbers were randomly distributed among the three groups. Based on the random numbers generated, the 45 participants were equally divided into the following groups: PMT (n = 15), KT (n = 15), and DS (n = 15).
Participants
The study included participants aged 20 to 25 years with no history of professional sports and no limitations in their range of motion. Exclusion criteria were as follows: individuals with orthopedic issues in the dominant shoulder, those experiencing shoulder pain for the past four weeks, inability to follow intervention instructions, and those with neurological, vascular, or cardiac conditions that could limit function. Additionally, participants with allergic reactions to kinesiology tape or wounds in the shoulder area were also excluded. Initially, 49 volunteer students who met the inclusion criteria were selected for the study; however, two were excluded for not meeting the criteria, and two others withdrew after initially agreeing to participate.
A detailed flowchart of the study process was provided in the CONSORT flow diagram, following the consolidated standards of reporting trials (Figure 1).
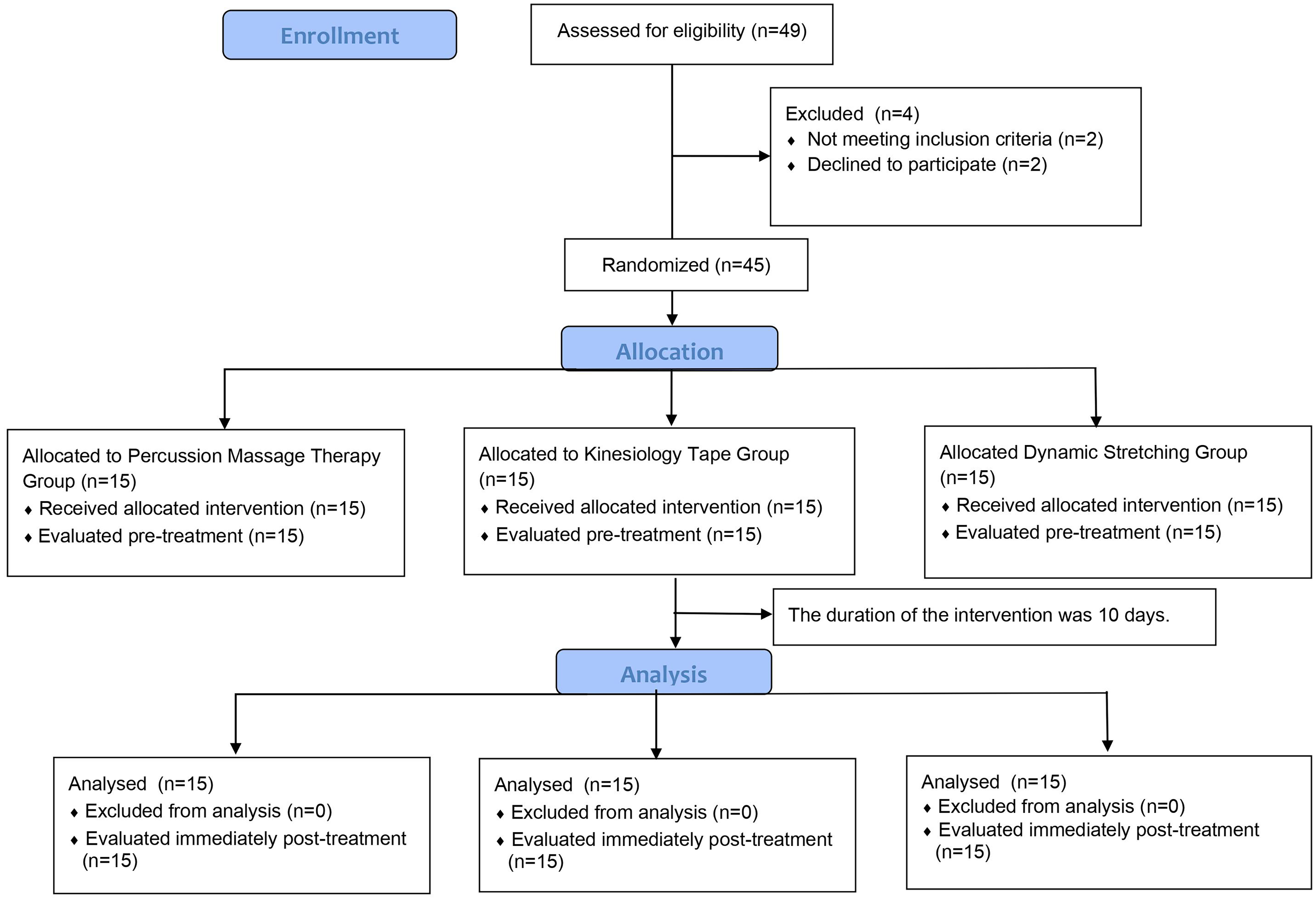
Design and flow of participants through the trial.
Intervention
Percussion massage therapy group
Percussion massage therapy was performed on the deltoid muscle group for a duration of 5 min. The treatment was consistently administered by the same physiotherapist using a Hypervolt device (Hyperice, CA, USA), which operates at a frequency of 40 Hz. A flat head attachment was used for the massage. The physiotherapist applied the device along the targeted area, moving it in a straight line from proximal to distal and then back to proximal, with each stroke lasting 5 s. Percussion massage therapy was administered every other day, with a total of five sessions over a span of 10 days. The application was made to the dominant shoulder of the individuals. (Figure 2) The dominant side of the participants was determined by asking which side they use for writing and which they prefer for activities requiring strength in their daily lives.

Percussion massage therapy.
Kinesiology tape group
Kinesiology taping was performed with 25% tension by applying Y tape to the Deltoid muscle group in the KT group. (Figure 3) The Kinesio Taping (KT) application was conducted in accordance with the guidelines of the Kinesio Taping Association International (KTAI) and performed by the physiotherapist, who is a certified KT practitioner by KTAI. After cleansing the skin with isopropyl alcohol, a Y-shaped Kinesio Tex Classic tape (Kinesio Holding Corp., Albuquerque, New Mexico) was applied to the dominant shoulder. 16 After taping, the Kinesiology tape remained on the participant for two days and was removed on the 3rd day. Kinesiology taping was applied to the body for 48 h, and the application was repeated after the tape had been removed. Kinesiology taping was applied to the dominant extremity of the participants for ten days. 17

Kinesiology tape.
Dynamic stretching group
Dynamic stretching exercises with 15 repetitions in shoulder flexion and abduction directions were applied to the individuals in the DS group under the supervision of a physiotherapist every other day. Each repetition lasted approximately 2 s, with one set taking around 30 s to complete. A total of three sets were performed, with a 10-s rest interval between each set. 18
Participants repeated stretching exercises for ten days. Dynamic stretching exercises are applied in the directions of abduction and flexion.
Outcome measures
Muscle strength, joint position sense, Timed Functional Arm and Shoulder Test (TFAST), and demographic data were assessed at the beginning and end of the study by the same physiotherapist. All assessment methods applied to the participants were repeated before the treatment and again ten days after the interventions were completed.
Muscle strength
The shoulder flexion and abduction muscle strength of the participants were measured. This study measured the deltoid muscle strength using a myometer device (JTECH Medical - Commander Powertrack, USA), whose validity and reliability have been established. 19 After providing information on how the test would be conducted, a trial test was performed. Subsequently, the muscle test was started. The maximum force recorded by the gadget was measured, and the force application stopped when the patient could not continue moving. Muscle strength measurement was repeated three times, and the test average was recorded. 20
After providing information on how the test would be conducted, a trial test was performed. Subsequently, the muscle test was started.
Functionality
The TFAST is a functional assessment tool designed to evaluate joint range of motion, muscle strength, and endurance, particularly in non-athletic individuals. This test consists of three functional tasks: hand-to-head & back, wall wash, and gallon lift. For each task, the total number of repetitions was recorded, and a cumulative TFAST score was computed. The equipment utilized in the test included small towels to minimize wall friction, a plastic gallon jug filled with water, and a shelf. Developing a practical and valid test for arm function would improve clinical assessments and the measurement of outcomes. 21
The duration of this test was 30 s. It started with the participant's arm positioned at their side, followed by a movement where they reached up to touch the back of their head. Any part of the hand making contact, preferably the full palm, was considered acceptable. After touching the back of the head, the participant lowered their arm to place the back of their hand against the lower back. This motion was repeated throughout the test period. Each successful touch of the back of the head was counted as one repetition, and the total number of repetitions completed during the test was recorded. 21
This test was conducted for 60 s in each direction. Participants were instructed to perform circular movements with their hands and arms at shoulder level. To reduce friction with the wall, a towel was placed under the hand. The movement began from the top of the circle, continuing for 60 s. The participant performed inward and outward circles while maintaining the arm at shoulder level, with each complete circle being recorded. 21
The test had a 30-s time limit. The shelf was positioned 20 inches above a 36-inch high counter, reflecting typical home and workplace dimensions. The jug used in the test weighed 3.78 kg. Participants lifted the jug to the height of the counter, touched the shelf, and then lowered it back to counter height, repeating the process as many times as possible within the 30-s timeframe without placing the jug on the shelf. Each touch of the shelf was counted as one repetition, and the total number of repetitions was recorded. Data were collected using the following formula: “Hand to Head & Back + ((Wall wash inward + outward)/4) + gallon jug lift. 21
Joint position sense
The joint position sense of the study's participants was evaluated using Becure Extremity ROM. (Figure 4) Participants’ joint position sense was evaluated by a physiotherapist experienced with the Becure Extremity ROM system. This Kinect-based system, developed by computer engineers and physiotherapists, quantitatively assesses joint range of motion and position sense using a Kinect camera. It is a valid and reliable tool for evaluating shoulder movements. 22 Becure Extremity ROM uses cameras and sensors to detect reference points during extremity movement, enabling objective joint ROM assessment. Patients perform shoulder flexion and abduction movements in front of the camera. For joint position sense measurement, participants first raised their shoulders to a specific angle and then repeated the movement with closed eyes. The difference between the angles with eyes open and closed was recorded. 23
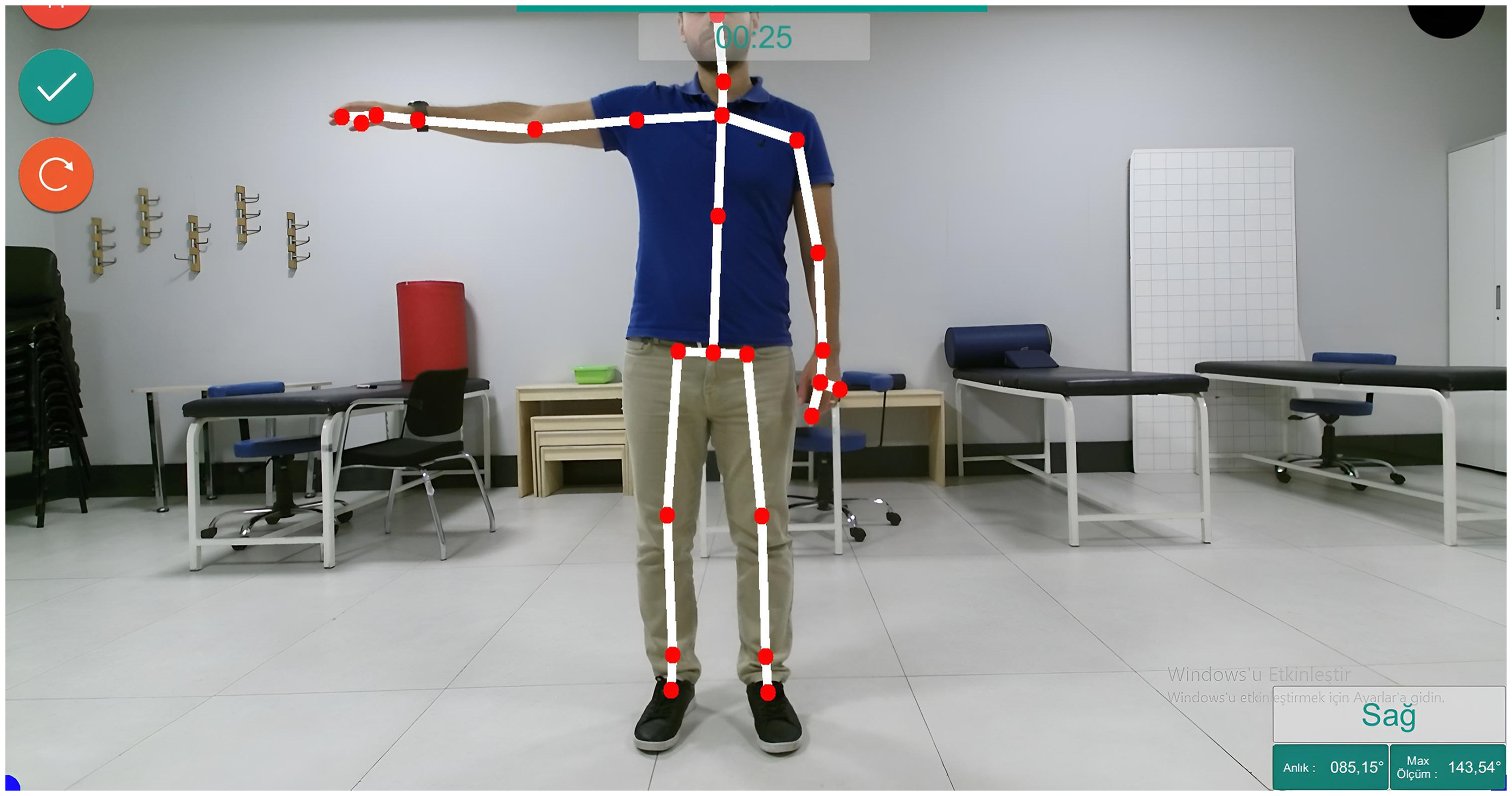
Becure extremity Rom.
Statistical analyses
The sample size was calculated using the G*Power software (version 3.0.10). A total of 42 participants were required to achieve 80% statistical power (α = 0.05, β = 0.20) with a medium effect size (f = 0.5). 24 Data analysis for the study was conducted using SPSS (Statistical Package for Social Sciences) version 20 (SPSS, Inc., Chicago, IL). For both intragroup and intergroup analyses with normally distributed data, a one-way analysis of variance (ANOVA) was applied. To compare the pre-and post-treatment results within the groups, the Paired Samples t-test was used. Post-hoc comparisons between groups were performed using Tukey's HSD test. Effect sizes were calculated using Cohen's d and interpreted based on Cohen's thresholds: small (< 0.2), moderate (0.5), and large (> 0.8). 25 A significance level of p < 0.05 was considered for the one-way ANOVA, while the significance threshold for the post-hoc test was set at p < 0.017. ANOVA results included the df, F-value and p-value. Associated 95% confidence intervals (CI) estimated reliability.
Results
As presented in Table 1, the demographic variables, including gender, height, age, and weight, were similarly distributed across the groups. When comparing the intra-group pre and post-differences, no statistical difference was found in pre and post-muscle strength values in the PMT and KT groups (p > 0.05). However, a statistically significant difference was found in the pre and post-proprioception and functionality parameters in both groups (p < 0.05). DS positively influenced some parameters of muscle strength, functionality, and proprioception (JPS-30° flex, JPS-60° flex, JPS 60° abd) (p < 0.05). (Table 2) When comparing the evaluation measurements of the groups, a statistically significant difference was found between the groups (p < 0.05). JPS 30°,60°,90° flexion parameters were 0.51, 0.64, and 0.49, respectively, while the effect sizes for the JPS 30°-60°-90° abd parameters were 0.38, 0.46, and 0.45, respectively. The effect size for Total TFAST was found to be 0.55; for flexion muscle strength, it was 0.59; and for abduction muscle strength, it was 0.68. (Table 3) While PMT and DS did not show superiority to each other in functionality parameters (p > 0.017, F: 26.66), both groups were found to be more effective than the KT group (p < 0.017). PMT and KT applications were found to be more effective than DS in the proprioception parameter (p < 0.017). When difference values of PMT and KT were compared, improvements were observed in JPS flexion and abduction at 30°, 60° and 90° difference values. However, no superiority was found between them (p > 0.017). When the three groups were compared in terms of muscle strength, there was a statistically significant difference between them (p < 0.05). However, when comparing the post hoc values of muscle strength between PMT and KT, no significant difference was found between the two groups (p > 0.017). Also, there was an increase in muscle strength in the DS group by comparing the other groups (p < 0.017) (Table 3).
Characteristics of the participants.
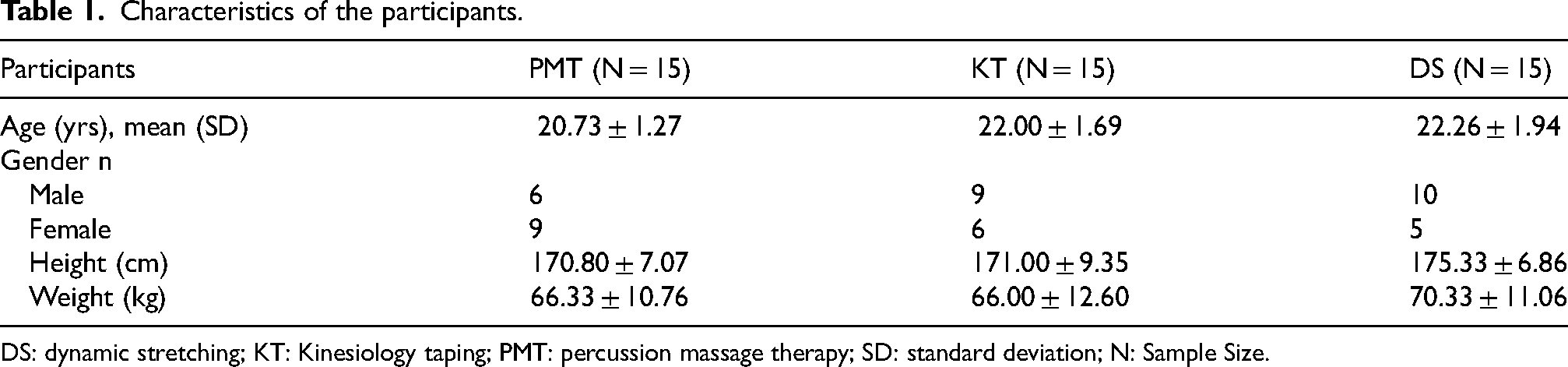
DS: dynamic stretching; KT: Kinesiology taping; PMT: percussion massage therapy; SD: standard deviation; N: Sample Size.
Comparison of the values pre-treatment and post-treatment within the group.
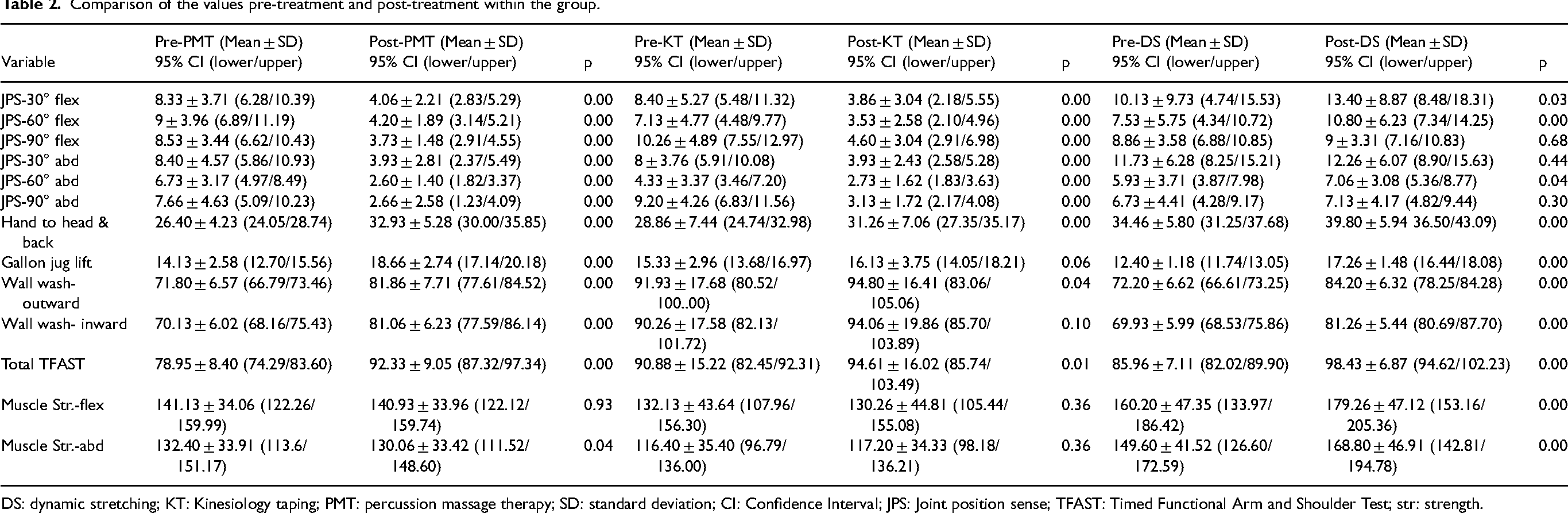
DS: dynamic stretching; KT: Kinesiology taping; PMT: percussion massage therapy; SD: standard deviation; CI: Confidence Interval; JPS: Joint position sense; TFAST: Timed Functional Arm and Shoulder Test; str: strength.
Intra-Group differences of values pre-treatment and post-treatment and comparison of differences between groups.
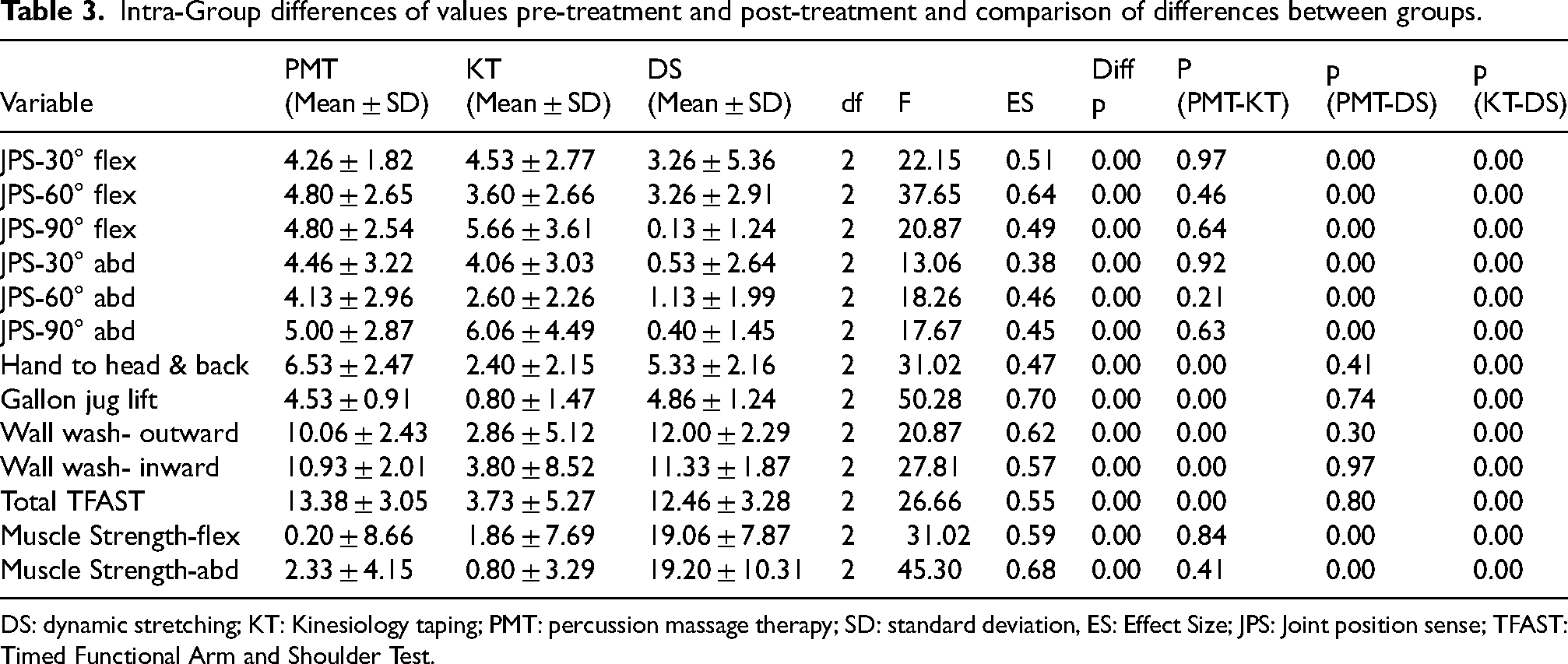
DS: dynamic stretching; KT: Kinesiology taping; PMT: percussion massage therapy; SD: standard deviation, ES: Effect Size; JPS: Joint position sense; TFAST: Timed Functional Arm and Shoulder Test.
Discussion
Our study observed significant improvements in almost all proprioception parameters across all three groups. While the PMT and KT groups were found to be superior in proprioception parameters compared to the DS group, no significant differences were observed between these two groups. Improvements were seen in the total TFAST scores for all groups. No significant difference in the total TFAST score was observed between the PMT and DS groups; however, both groups were found to be more effective than the KT group. In terms of muscular strength, the DS group was determined to be more effective than the other groups.
Proprioception
Foam rolling with local vibration has been shown to enhance proprioception more effectively than foam rolling without vibration or static stretching. 26 Similarly, whole-body vibration therapy has enhanced knee proprioception in ACL reconstruction patients and joint position sense in healthy individuals.27,28 In our study, local vibration was more effective than dynamic stretching in improving proprioception, likely due to its stimulation of the proprioceptive system. Previous studies suggest external stimuli like neoprene shorts, insoles, and taping can influence proprioception.29–31 Kinesiology taping (KT) has shown mixed results, with some studies reporting improvements in knee and shoulder proprioception,32–34 while others found no significant effect.35–38 Our findings align with those showing KT's positive impact on shoulder proprioception, especially after longer application durations. While many studies measure only immediate effects, our study observed improvements with a 10-day KT application. Stretching exercises, however, did not show significant effects on joint position sense, consistent with previous research.39,40
Functionality
Research on the effects of local vibration therapy on shoulder functionality is limited, and its efficacy remains debated. Some studies have found that while vibration therapy increases muscle strength in osteoarthritis patients, it has no effect on functionality. 41 Similarly, local vibration therapy applied to the forearm showed no functional improvement. 42 However, PMT has been reported to enhance joint range of motion and flexibility in the short term.43,44 Our study aligns with this, showing that percussion massage therapy improves functionality with a moderate effect size. Studies on the impact of kinesiology taping (KT) on functionality in healthy individuals are also limited. One study reported no functional improvements with KT. 45 In contrast, our study found that applying KT for ten days enhanced functionality. Additionally, vibration and stretching exercises proved more effective than KT, likely due to their more active stimuli.
Muscle strength
Studies have shown that vibration therapy, both local and whole body, can increase muscle strength in the short and long term, particularly when combined with strengthening exercises.46–48 Localized percussive massage therapy has also been reported to improve physical performance and balance. 49 Szymczyk et al. suggested that mechanical percussion before explosive athletic activities could enhance performance. 2 However, our study did not include a strengthening program, which may explain the lack of observed muscle strength improvement. The impact of kinesiology taping (KT) on muscle strength is debated. Some studies report increased quadriceps strength with KT, 50 while others found no effect. 51 In our study, KT did not lead to changes in muscle strength, indicating that incorporating strengthening exercises alongside KT may be necessary for optimal results. High-intensity stretching has been shown to instantly increase muscle strength in some cases, 52 though other studies suggest it may not have an immediate effect. 53 In our study, dynamic stretching resulted in a statistically significant increase in muscle strength. Percussion massage therapy (PMT) proved beneficial due to its effectiveness and ease of use in clinical settings, while kinesiology taping (KT) improved shoulder proprioception. However, dynamic stretching showed the most significant improvement in shoulder muscle strength. A key limitation of this study is the lack of long-term outcome evaluation. Additionally, the limited research on massage guns leaves uncertainties about the optimal vibration speed, amplitude, and timing of use (before or after exercise). Although clinical studies remain limited, PMT has recently gained popularity in therapeutic settings and sports medicine. In this study comparing PMT, KT, and DS, PMT was most effective for proprioception and functionality, DS for functionality and muscle strength, and KT for proprioception. These findings can guide practitioners in choosing the appropriate intervention. However, given the varying results across proprioception, muscle strength, and functionality, further clinical studies are necessary to draw more definitive conclusions.
Footnotes
Ethical approval
The research followed the ethical guidelines of the Declaration of Helsinki for studies involving human participants. The study protocol was approved by the Non-Interventional Ethics Committee of Istanbul Medipol University (Approval Number: E-10840098-772.02-1948).
Informed consent
All participants provided written informed consent prior to their involvement in the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.