
Abstract
Background:
The scope of practice for physiotherapists encompasses a range of specialized areas, including orthopedics, neurology, pediatrics, general practice, and public health.
Objective:
This study aims to elucidate the influence of occupational preferences among physiotherapists in diverse practice fields on the prevalence of professional satisfaction, burnout, and musculoskeletal pain.
Methods:
The study was designed as an observational study conducted between September 2023 and January 2024. A total of 255 physiotherapists were included and divided into five groups based on their primary areas of practice: general, neurology, orthopedics, pediatrics, and public health. All participants were evaluated with the Expanded Nordic Musculoskeletal Questionnaire (NMQ), the Pain Coping Inventory (PCI), the Maslach Burnout Inventory (MBI), and the Job Satisfaction Scale (JSS).
Results:
Physiotherapists in general and orthopedics had a higher prevalence of low back pain than those in pediatrics and public health. General, neurology, and pediatrics physiotherapists experience a higher prevalence of burnout than those in public health and orthopedics. Neurology and pediatrics physiotherapists have higher emotional exhaustion prevalence than public health physiotherapists, while neurology physiotherapists demonstrate higher depersonalization prevalence than pediatrics and public health physiotherapists. Orthopedics physiotherapists exhibit higher personal achievement prevalence than other physiotherapists. Orthopedic physiotherapists have a higher JSS prevalence compared to other specialties. In PCI, the majority of them utilize active strategies and distancing compared to pediatric physiotherapists.
Conclusions:
Prevalence of job satisfaction, burnout risk, musculoskeletal pain, and coping strategies differ in physiotherapists in diverse fields of practice.
Introduction
Physiotherapy aims to optimize an individual's mobility and functionality to their maximum potential, thereby ensuring the maintenance of existing abilities and the restoration of lost functions. 1 A physiotherapist is a health professional who facilitates improvements in an individual's functional ability by applying their professional experience, knowledge, and skills to achieve the most appropriate level of functionality. 2 The scope of practice for physiotherapists encompasses a range of settings, including private and public hospitals, branch centers, private workplaces and clinics, special education, and rehabilitation centers, clinics working with athletes, as well as specializations in orthopedics, neurology, pediatrics, general practice, and public health. 3
Musculoskeletal disorders are highly prevalent among healthcare professionals, with a prevalence exceeding 80% among physiotherapists. Due to the nature of their work, the primary cause of work-related musculoskeletal disorders among physiotherapists is the performance of repetitive movements or intense physical demands, including lifting heavy patients, manual handling, patient handling, awkward positioning, and prolonged constrained postures.4,5 The most frequently affected areas are the lower back, the neck and upper back, and the thumb. 6 This situation has a dual impact on the individual, affecting both their physical and psychological well-being. Furthermore, discontent with the conditions of the working environment can give rise to psychological effects, including occupational dissatisfaction. 7 It is established that the most significant determinants of occupational satisfaction are factors such as working hours, the working environment and conditions, the quality of cooperation and communication with colleagues and management, and performance evaluation such as salary and promotion. 8 The high level of occupational satisfaction among physiotherapists is closely associated with a range of factors, including their working conditions, remuneration, workload, opportunities for advancement within their profession, professional experience, and emotional state within the workplace. Therefore, the long-term nature of physiotherapists’ treatment processes may contribute to a decline in professional satisfaction and an increase in burnout. 9
In Turkey, the majority of physiotherapists are employed in the public and private sectors. 7 In a study investigating the prevalence of musculoskeletal pain among physiotherapists based on their employment status in public or private institutions, it was found that musculoskeletal pain was lower among those employed in public institutions. 10 A further study demonstrated that physiotherapists in private healthcare facilities reported greater satisfaction with their working environment and conditions than those in public institutions and organizations. 7 The prevalence of burnout among physiotherapists has been documented in various studies, with rates ranging from 15.7% among Italian physiotherapists, 11 over 22.5% among Polish physiotherapists, 12 to 42% among Portuguese physiotherapists. 13 However, there is a lack of available data concerning the impact of occupational preferences of physiotherapists engaged in different professional domains on physical complaints and satisfaction in Turkey.
Therefore, this study aims to elucidate the influence of the occupational preferences of physiotherapists engaged in diverse fields of practice on the prevalence of professional satisfaction, burnout, and musculoskeletal pain.
Methods
Study design
This study was conducted between September 2023 and January 2024 after obtaining ethical approval from the Uskudar University Non-Interventional Research Ethics Committee with the reference number 61351342/January 2023-09. The protocol is registered with http://clinicaltrials.gov/ (17/August/2023, NCT06006481).
Determination of sample size
The G*Power Version 3.1.9.7 program was employed to ascertain the requisite sample size for the study. Following the power analysis, 255 individuals were surveyed to achieve a statistical significance value of 0.05, an effect size (Cohen's d) of 0.25, and a power of 0.95.14,15 The population under investigation comprised physiotherapists practicing in Turkey. The study was conducted among individuals who had graduated from the Physiotherapy and Rehabilitation Departments or Physical Therapy and Rehabilitation Schools of the Faculties of Health Sciences, which provide four-year education in universities in Turkey and have the title of “physiotherapist”.
The following criteria were employed to determine eligibility for participation in the study: (1) volunteering to participate in the study, (2) being a physiotherapist, (3) having completed at least one year in the profession and continuing active working life, and (4) being between 21 and 60 years of age. The exclusion criteria were defined as being currently unemployed and holding a position other than that of a physiotherapist.
The study was designed as a descriptive, cross-sectional, and analytical online survey. The questionnaires were uploaded to the Google Forms database. Thereafter, the participants were contacted via online channels, including e-mail, mobile phone applications, and social media, and invited to participate in the study.
Procedure
Before commencing the study, participants were requested to complete a voluntary consent form. Subsequently, they were required to complete a personal information form, the Expanded Nordic Musculoskeletal Questionnaire, the Pain Coping Inventory, the Maslach Burnout Scale, and the Occupational Satisfaction Scale. According to the results obtained, 5 different groups were evaluated among themselves by the parameters determined. The physiotherapists were divided into five groups according to their areas of practice: general (n = 82), orthopedics (n = 64), neurology (n = 38), pediatrics (n = 45), and public health (n = 26).
Outcome measurements
Personal information form is a questionnaire consisting of 20 questions about demographic characteristics such as age, gender, educational status, monthly earnings, and whether they have sports habits and sleep patterns.
The Expanded Nordic Musculoskeletal System Questionnaire (NMQ) is used to determine the prevalence of pain in the musculoskeletal system. 16 The questionnaire aims to determine the pain and complaints in parts of the body and to make comparisons. There is a visual showing nine parts of the body in the questionnaire. These body parts are the neck, shoulders, back, elbows, hands, waist, hips, knees, and feet. The questionnaire is designed to ascertain whether individuals have experienced pain and discomfort in specific body parts over the past 12 months, the past four weeks, and on the day of assessment. The questionnaire includes a series of questions on the duration of pain, whether individuals have changed jobs due to pain, whether they have taken leave from their workplaces due to pain, and the use of medication due to pain. The questionnaire provides reliable information regarding the duration of the discomfort and its impact on daily activities.
Maslach Burnout Inventory (MBI) scale comprises a total of 22 questions. 17 The responses to the questions are provided on a 5-point Likert-type scale comprising a series of options, including 0 (Never), 1 (Very Rarely), 2 (Sometimes), 3 (Most of the Time), and 4 (Always). It is requested that volunteers indicate their responses by selecting the most appropriate option for each question. The scale is divided into three subcategories. The scale comprises nine items about emotional exhaustion, five items about depersonalizationtion, and eight items about personal achievement. Individuals exhibiting a high level of exhaustion are anticipated to exhibit elevated emotional exhaustion and depersonalization scores, accompanied by diminished personal achievement scores. The scores that can be obtained from the subscales vary between 0 and 36 for emotional exhaustion, 0 and 20 for depersonalization, and 0 and 32 for personal accomplishment.
Job Satisfaction Survey (JSS) scale was developed to determine whether employees enjoy their jobs and to what extent they are happy and satisfied. 18 The scale comprises 20 five-digit Likert-type questions. The scoring for items 1, 2, 3, 5, 6, 7, 8, 12, 13, 15, 16, 17, 18, 20 is as follows: “5: Always, 4: Frequently, 3: Occasionally, 2: Rarely, 1: Never”. Items 4, 9, 10, 11, 14, and 19, which constitute the negative items, are scored in reverse.
Pain Coping Inventory (PCI) scale was developed to identify the behavioral and cognitive strategies employed by individuals with chronic pain to cope with this condition. The original form of the scale comprises sub-dimensions, including pain transformation, distancing, and demand reduction, and six passive sub-dimensions, including withdrawal, worrying, and rest. 19 The scale comprises 22 items and is scored according to a 4-point Likert scale. The lowest possible score is 1 (indicating that the behavior in question is rarely observed), while the highest score is 4 (indicating that the behavior in question is observed very often).
Data analysis
The SPSS 25.0 program was employed in the analysis of the data. The total and sub-dimensional scores for the scales were obtained by summing the scores for the questions in the sub-dimensions. The conformity to the normal distribution was examined with the Shapiro-Wilk test. Given that a substantial number of scores according to the groups exhibited a lack of conformity to the normal distribution, the non-parametric Mann-Whitney U Test and Kruskal-Wallis H Test were employed to examine any potential differences between the groups. Following the Kruskal-Wallis H Test, the Dunn-Bonferroni test was employed as a post hoc test.
The effect size is a value that describes the effect of the test. For the Kruskal-Wallis H test, the following effect size (eta-squared) was used; η2 = (H − k + 1) (n − k). 0.01–0.06 is considered a small effect, 0.06–0.14 is considered a medium effect, and >0.14 is considered a large effect. Cramer's V value was analyzed for the magnitude of the chi-squared test result. To evaluate the Cramer's V value, one was subtracted from the row and column values of the cross table, and the test was evaluated as 0.01 weak, 0.30 medium, 0.50 strong if it has 1 category, 0.07 weak, 0.21 medium, 0.35 strong if it has 2 categories, 0.06 weak, 0.17 medium, 0.29 strong if it has 3 categories.
Results
A total of 255 physiotherapists were included in the study and were divided into five distinct groups based on their primary area of practice: general (n = 82), neurology (n = 38), orthopedics (n = 64), pediatrics (n = 45), and public health (n = 26).
Table 1 demonstrates the distribution of categorical demographic characteristics of participants. The analysis revealed no statistically significant difference between the area of work and gender, marital status, educational status, and length of experience in the current workplace (p > 0.05). However, there was a statistically significant difference in terms of years of professional experience (p < 0.01), income status (p < 0.001), and workplace (p < 0.001).
The distribution of categorical demographic characteristics of participants according to field of study.
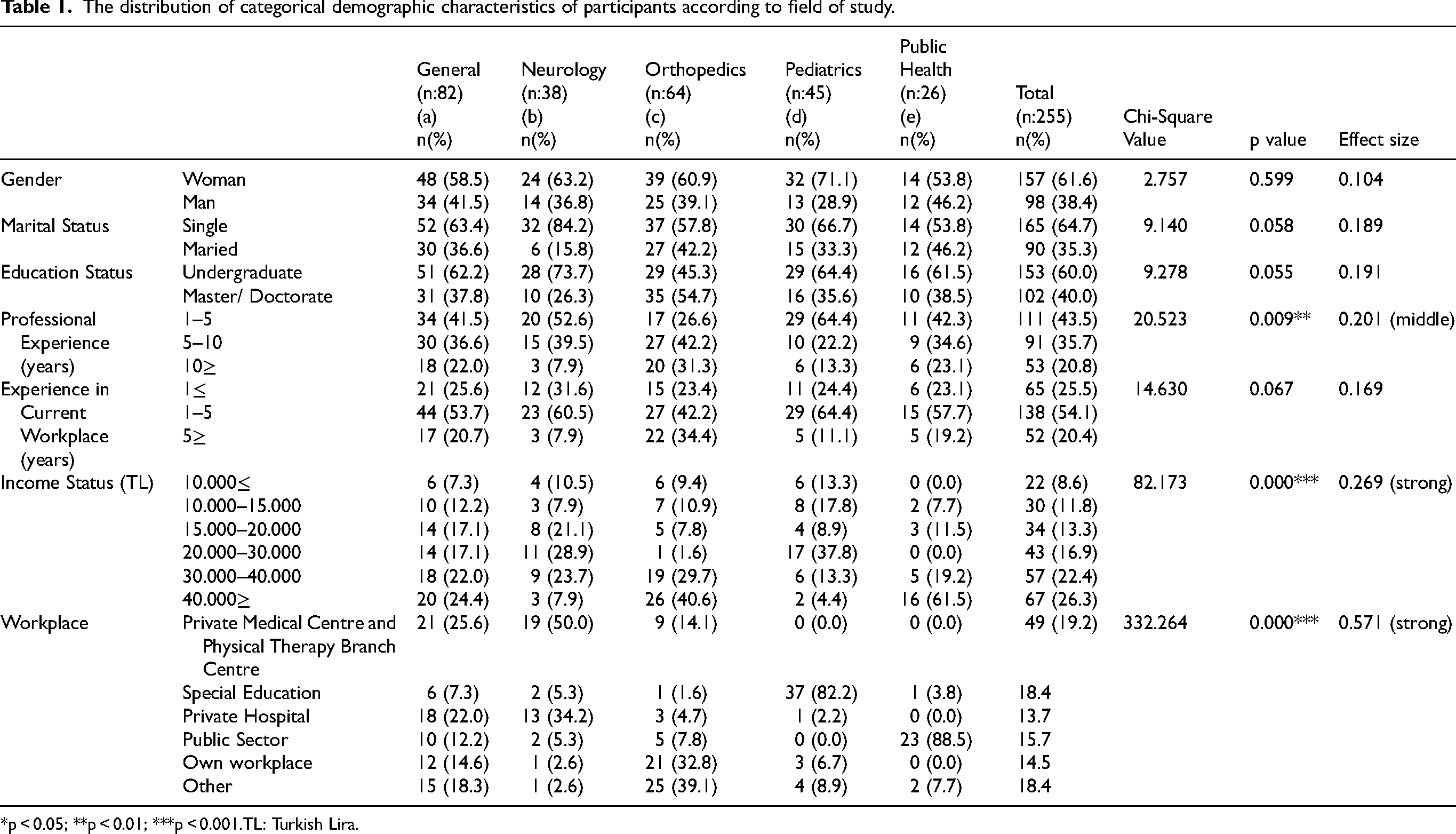
*p < 0.05; **p < 0.01; ***p < 0.001.TL: Turkish Lira.
Table 2 demonstrates the distribution of numerical demographic characteristics of the participants according to the field of study. The mean age of physiotherapists engaged in orthopedics was significantly higher than that of their neurology and pediatrics counterparts (p < 0.001). The mean age of public health physiotherapists is less than that of general, neurology, and orthopedics physiotherapists. Pediatric physiotherapists ‘ mean age is higher than general and neurology physiotherapists (p < 0.001). A comparison of the daily sleep duration scores revealed that orthopedic physiotherapists exhibited a higher mean score than neurology physiotherapists (p < 0.05). No statistically significant difference was observed in the daily working time on weekends according to the field of specialization (p > 0.05).
Distribution of numerical demographic characteristics of the participants according to the field of study.
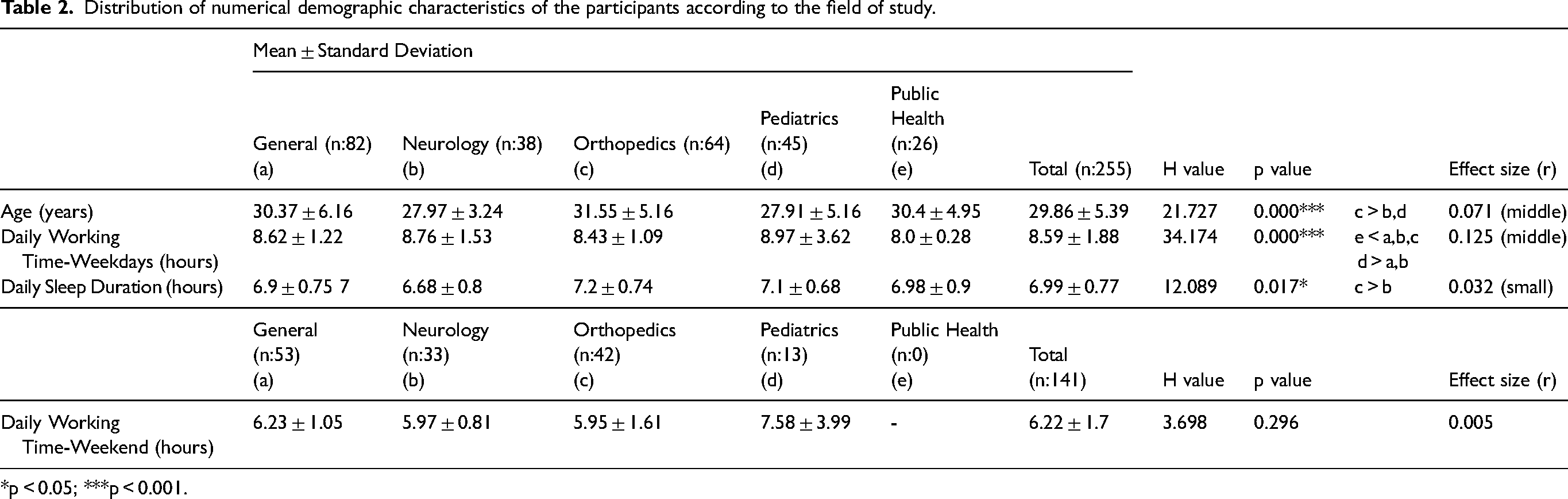
*p < 0.05; ***p < 0.001.
Table 3 shows the distribution of NMQ scores among physiotherapists There is a significant variation with rates of 20% for pediatricians, 43.9% for general practitioners, 40.8% for orthopedic surgeons, and 50% for public health professionals (p < 0.05) in the prevalence of low back pain based on field of study. The prevalence of low back pain was significantly higher among physiotherapists engaged in general and orthopedic practice compared to those working in pediatrics and public health (p < 0.05). No statistically significant differences were observed in the prevalence of neck, shoulder, upper back, elbow, wrist/hands, hip/thigh, knee, and ankle/foot pain according to the field of study (p > 0.05).
Distribution of expanded NMQ according to field of study.
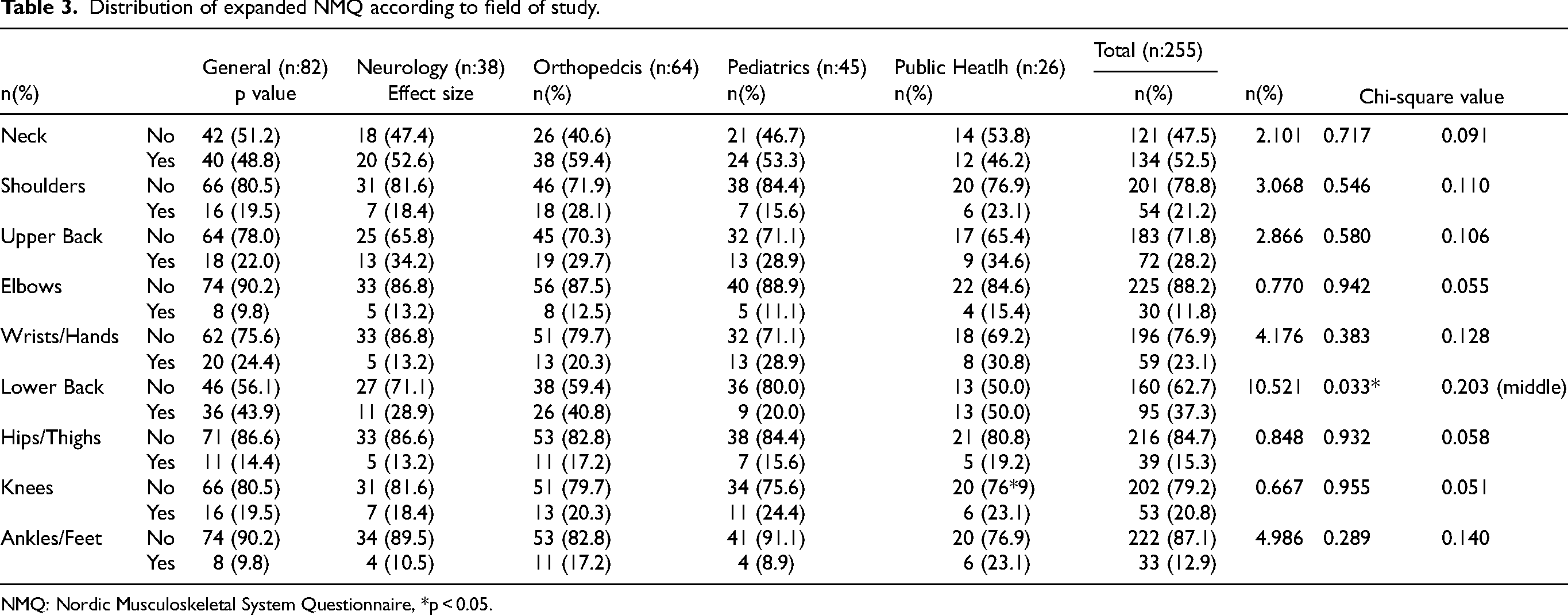
NMQ: Nordic Musculoskeletal System Questionnaire, *p < 0.05.
Table 4 demonstrates the distribution of MBI, JSS, and PCI scores among physiotherapists. There are statistically significant differences in terms of the prevalence of the total MBI score, as well as the sub-dimensions of emotional exhaustion, depersonalization, and personal achievement, according to the field of study (p < 0.001, p < 0.01). General, neurology, and pediatrics physiotherapists exhibit a significantly higher prevalence of burnout than their counterparts in public health and orthopedics (p < 0.001). In the sub-dimension of emotional exhaustion, the mean scores of neurology and pediatrics physiotherapists significantly demonstrated a higher prevalence of emotional exhaustion than those of public health physiotherapists (p < 0.001). Furthermore, general, neurology, and pediatrics physiotherapists depicted a higher prevalence of emotional exhaustion than those of orthopedics physiotherapists (p < 0.001). Neurology physiotherapists are found to demonstrate a higher prevalence of depersonalization than that of pediatrics and public health physiotherapists (p < 0.01). Also, orthopedics physiotherapists demonstrated a higher prevalence of personal achievement than that of general, neurology, pediatrics, and public health physiotherapists (p < 0.001).
MBI, JSS, and PCI scores according to the field of study.
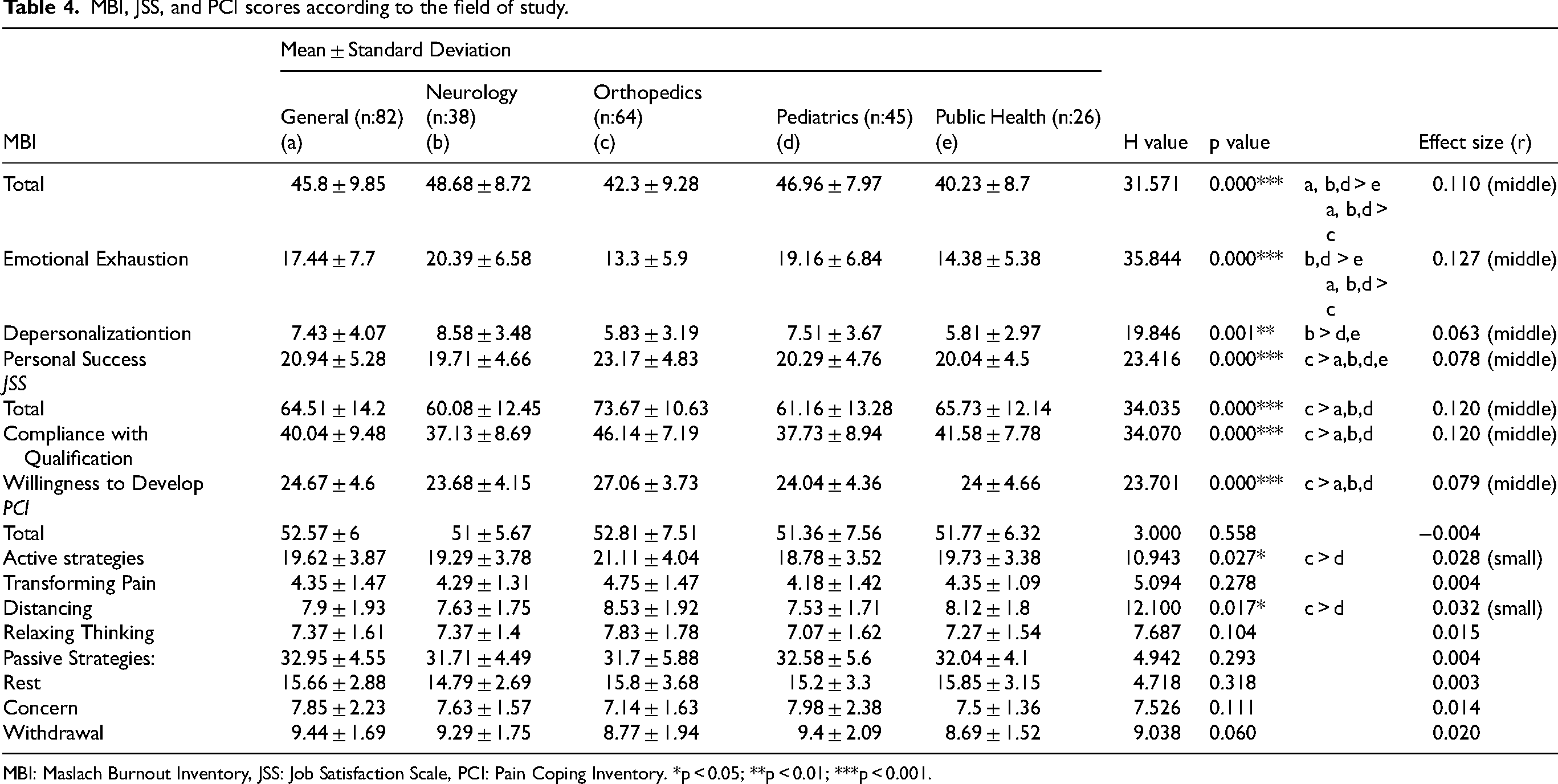
MBI: Maslach Burnout Inventory, JSS: Job Satisfaction Scale, PCI: Pain Coping Inventory. *p < 0.05; **p < 0.01; ***p < 0.001.
The total score and all sub-dimensions of the JSS indicated that the vast majority of orthopedics physiotherapists exhibited markedly elevated scores compared to those working in other specialties, including general medicine, neurology, and pediatrics (p < 0.001). In PCI, the mean scores of orthopedic physiotherapists demonstrate a significantly higher prevalence of active strategies and distancing than pediatric physiotherapists (p < 0.05).
Table 5 demonstrates a univariate analysis of low back pain in physiotherapists working in different fields. Univariate analysis showed that among the single factors, gender (man), educational status (undergraduate), age (31–48), professional experience (5≥), experience in the current workplace (1≥), workplace (except public sector), and field of study (except pediatrics) were all related to the occurrence of lower back pain (p < 0.05). The prevalence of lower back pain is higher in males, and an inverse relationship has been observed between education level and lower back pain, indicating that as education level rises, the likelihood of experiencing lower back pain decreases. Furthermore, an increase in the duration of employment has been associated with a rise in the risk of lower back pain. The highest prevalence of lower back pain has been observed among private hospital employees and physiotherapists working in private educational institutions. When considering the field of study, the prevalence of lower back pain was highest among physiotherapists specializing in public health (p < 0.05).
Univariate analyisis of low back pain as dependent variable.
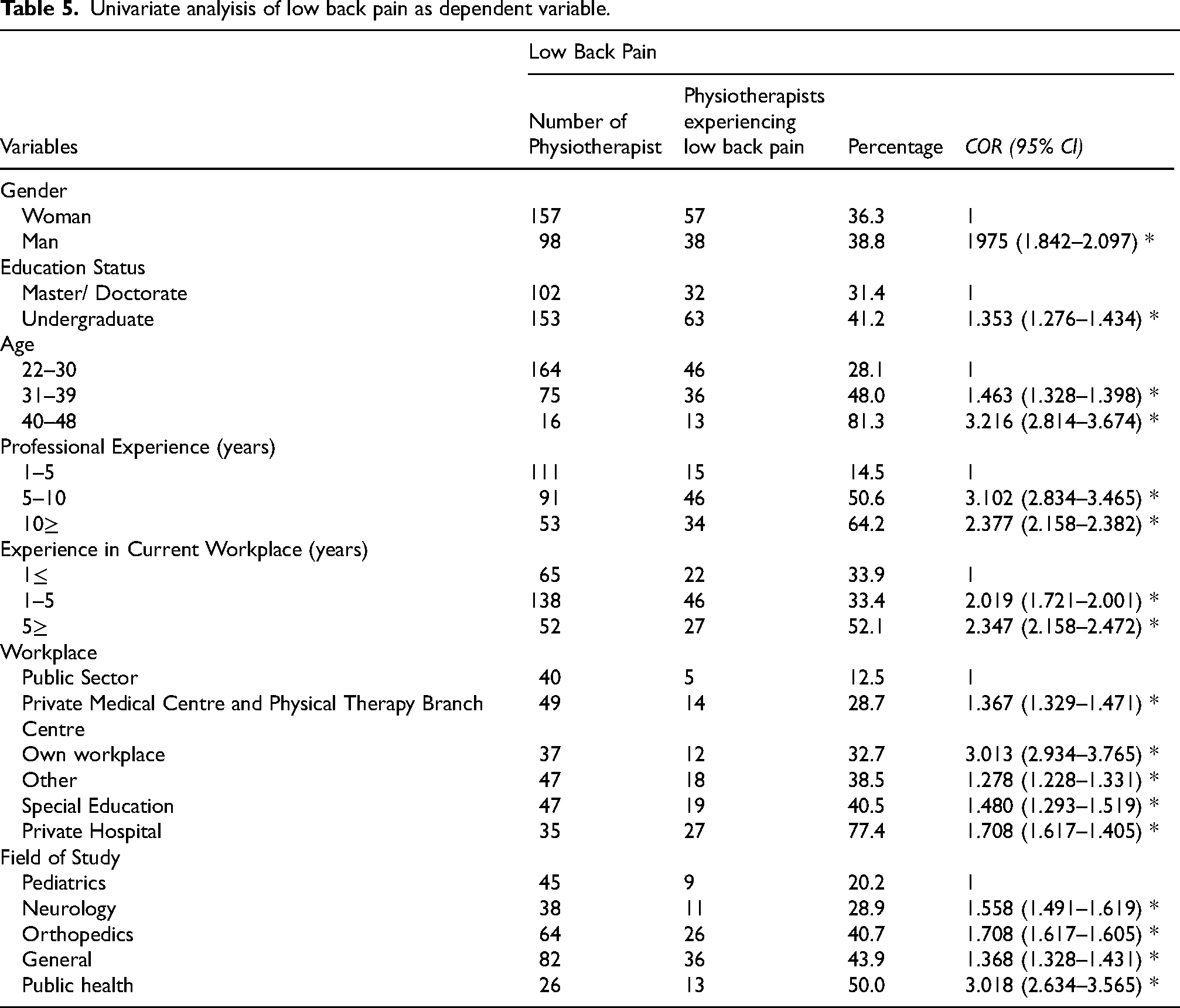
Table 6 demonstrates multivariate logistic regression analysis to estimate the probability of lower back pain among physiotherapists working in different fields. The application of multivariate logistic regression analysis revealed the following factors to be influential in the occurrence of low back pain: education status, professional experience, experience in the current workplace, workplace, field of study, and age.
Multivariate logistic regression análisis of low back pain.
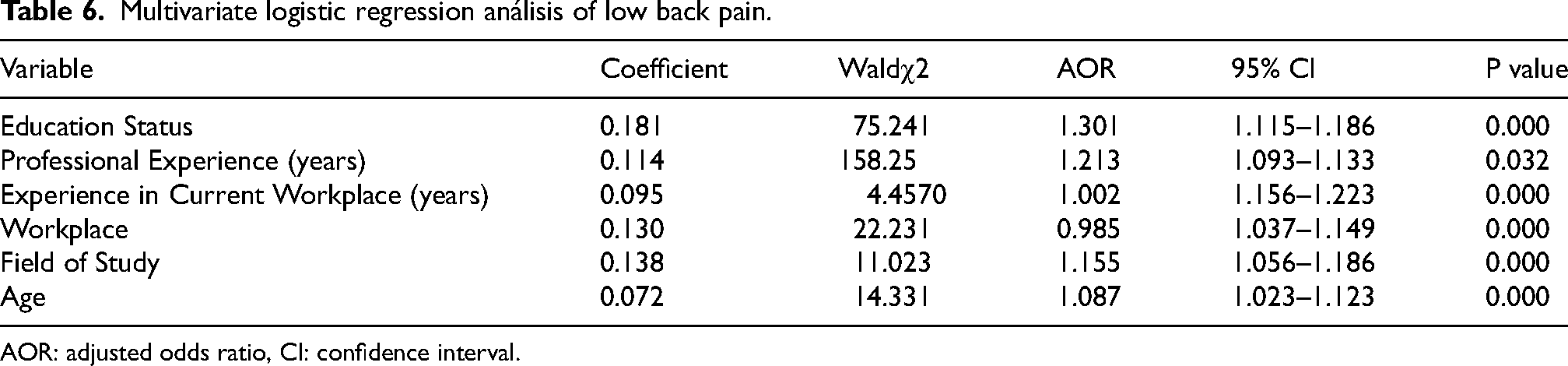
AOR: adjusted odds ratio, CI: confidence interval.
Discussion
The present study aimed to compare the prevalence of professional satisfaction, burnout, musculoskeletal pain, and pain coping strategies of physiotherapists working in general practice, orthopedics, neurology, pediatrics, and public health. Although previous studies have examined occupational injuries and burnout levels among physiotherapists in Turkey, no studies have yet explored these factors and occupational satisfaction among physiotherapists practicing in diverse fields. Accordingly, this study represents a pioneering contribution to the field. We demonstrated that physiotherapists in general and orthopedics presented a higher occurrence of low back pain than those in pediatrics and public health (p < 0.05). Also, the findings of this study indicate that neurology physiotherapists in Turkey have higher burnout with emotional exhaustion and depersonalization prevalence. On the other hand, orthopedics physiotherapists have a higher prevalence of personal achievement, occupational satisfaction, and pain coping strategies.
A recently conducted study has revealed that 42.1% of physiotherapists in Turkey have encountered musculoskeletal system problems during the course of their professional activities. Furthermore, the study findings have indicated that the most prevalent musculoskeletal issues were observed in the lumbar region, with a prevalence rate of 38%, and were subsequently followed by those observed in the shoulder and wrist regions. 20 In a different study, it was reported that physiotherapists developed musculoskeletal disorders due to maintaining incorrect body postures while standing for extended periods as a result of their demanding work schedules. As indicated by the NMQ, the participants exhibited the highest prevalence of back pain (30.7%), followed by neck pain (22.7%) and low back pain (13.3%). 21 The results of our study indicated that the most prevalent musculoskeletal disorders were observed in the neck region when all physiotherapists engaged in diverse practice areas were considered. Subsequently, it was determined that the second most prevalent musculoskeletal disorders were located in the waist region, followed by the wrist region. Given the physical demands of the physiotherapy profession and the requisite exertion involved in the work, the high prevalence of injury is an anticipated outcome, consistent with the rates observed in other literature studies.22,23 Moreover, an increase in the duration of employment has been shown to be associated with an elevated risk of lower back pain. A possible hypothesis to explain this phenomenon is that the elevated risk of lower back pian with a longer duration of employment is attributable to their prolonged exposure to occupational risk factors in comparison to those with a shorter duration of employment. 24 As in numerous preceding studies, it is postulated that the predominance of upper regions and the trunk as affected body parts in the present study is attributable to the fact that applications necessitating exertion, such as manual therapy, are conducted and that these body parts are employed more frequently in the transfer of patients. 25 Therefore, the high prevalence of lower back pain observed in orthopedics and general physiotherapists in our study is consistent with the demanding nature of physiotherapists’ work, which often requires significant effort. In terms of individual factors, the results indicated a close relationship between education status, professional experience, experience in the current workplace, and field of study, and the occurrence of lower back pain. In this study, the incidence of lower back pain among physiotherapists increased with age over 31 years. This can be explained by the presence of acute or chronic loads on the musculoskeletal tissue that can lead to the accumulation of injuries and an increased prevalence of musculoskeletal diseases over age. 26 In addition, the fact that physiotherapists rely heavily on their upper extremities and trunk during activities especially in the public health such as manual therapy and patient transfer may contribute to the high incidence of injuries in these regions.
In a recent statement, the World Health Organization (WHO) classified burnout as an “occupational phenomenon”. It underscores the importance of addressing burnout as a potential risk factor for adverse outcomes among workers, including impaired work performance and quality, and even patient safety. 27 It has been reported that burnout levels among physiotherapists working in pediatrics in Turkey are high which has been attributed to burnout resulting from a more emotional approach to patients in treatment and higher levels of mental fatigue. 28 It was observed that an increase in the weekly working hours of health workers was associated with a rise in burnout levels among the participants in Italy. 11 A study demonstrated that emotional exhaustion was higher in physiotherapists whose expectations were not met in terms of salary, indicating that economic reasons were effective on the burnout levels of people. 12 The findings of our study indicated that orthopedic and public health physiotherapists exhibited higher salaries, greater professional satisfaction, and a lower prevalence of burnout compared to other groups. The elevated prevalence of emotional exhaustion and depersonalization observed among neurology and pediatric physiotherapists point to the potential impact of occupational stressors, including prolonged standing, increased workload, work-related stress, and financial and moral expectations, on the development of burnout. Although the burnout levels of the groups in our study were similar, the higher prevalence of burnout among neurology physiotherapists may be attributed to factors such as advanced age, longer working hours, and inadequate daily sleep duration.
Occupational burnout is negatively correlated with job satisfaction in response to psychological stressors encountered in the workplace, which primarily manifest as exhaustion and disengagement.15,29,30 It was reported that the physiotherapists ‘ professional satisfaction level decreased due to an increase in burnout levels among neurological physiotherapists. 31 Similarly, emotional exhaustion and depersonalization represent the most conspicuous symptom of occupational burnout in neurology and pediatrics physiotherapists in our study. Therefore, it is of the utmost importance to monitor and promote job satisfaction among these physiotherapists to mitigate the negative impact on medical care recipients. Furthermore, although research has demonstrated that older physiotherapists exhibit greater job satisfaction than their younger counterparts, 32 another study has revealed that younger physiotherapists are more satisfied with their supervisors. 33 In this study, the orthopedic physiotherapists were older with a higher prevalence of occupational satisfaction than the others which is in line with Rostami et al. 32 Therefore, it can be reasonably deduced that the high job satisfaction of physiotherapists working in orthopedics might be a consequence of the influence of several demographic variables, including age, gender distribution, income level, and work conditions.33,34
The issue of combating pain is of significant importance in terms of enhancing the individual quality of life of employees and influencing work performance. A review of the literature revealed no previous studies on this subject among physiotherapists.35,36 A physiotherapist should have sufficient professional knowledge and experience to improve their patients’ functionality and quality of life. Therefore, the implementation of solution-oriented applications designed to prevent occupational health issues and provide suitable work environments that will eliminate or minimize physical complaints may prove an effective strategy for enhancing the professional satisfaction levels of physiotherapists. 7 The findings of this study indicate that physiotherapists working in the field of orthopedics demonstrated greater efficacy in the utilization of active pain management strategies in comparison to their counterparts in pediatrics. Therefore, this may be attributed to the fact that professional satisfaction is higher in the field of orthopedics.
It should be noted that the findings of our study are subject to certain limitations. The sample was composed of physiotherapists in Turkey which may have diminished the generalisability of our findings. Moreover, the study employed a self-assessment questionnaire, whose responses may be influenced by the potential bias of the physiotherapist. Also, the current economic difficulties in our country, the rise in unemployment among university graduates, and the standard rates of remuneration for physiotherapists are factors that warrant consideration. 20 The results of our study may have been influenced by the evolving situation and the variable income levels of the physiotherapists involved.
Conclusion
In the context of the global economic downturn precipitated by the pandemic, it is of paramount importance to underscore the necessity for robust health workforce planning to ensure the optimal productivity and performance of the health sector. 37 In light of these results, it is evident that there is a need to improve the working conditions of neurology and pediatrics physiotherapists in Turkey, particularly in terms of reducing burnout and exhaustion levels. It is of the utmost importance that future studies assess the effectiveness of interventions designed to reduce future levels of burnout and musculoskeletal pain among physiotherapists. This is not only vital for the maintenance of their well-being but also for the assurance of the superior quality of care. This information may be effective in preventing physical problems caused by working conditions, determining the changes to be made in the working environment after physical complaints and developing health policies to increase occupational satisfaction in developing countries.
Footnotes
Acknowledgements
The authors have no acknowledgments.
Ethical approval
The ethical approval was obtained from the Uskudar University Non-Interventional Research Ethics Committee with the reference number 61351342/January 2023-09.
Informed consent
An informed consent form was obtained from all participants. Participants
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.