
Abstract
Background
Upper limb pain, dysfunction, musculoskeletal disorders, and worker absenteeism result from working over-shoulder, making precision tasks, and other occupational control tasks. Researchers have shown that the physical demand is reduced when an exoskeleton is used, but the precision task's productivity and quality depend on the speed of execution.
Objective
Here, the study determined how an over-shoulder precision task and height change affect the upper extremity muscle activation behavior.
Methods
A convenience sample of sixteen participants was employed. A mix of factors intervention (without vs. exoskeleton), wrist load (with (0.5 Kg) vs. without load), and task height (three height levels) were simulated. Surface electromyography, repeated-measures analysis of variance (ANOVA) tests.
Results
Using an exoskeleton of our design for the experiment, we reduced muscle activation between 16% and 31.8% in shoulder muscles. However, the task height and wrist load factors increased muscle activation when they increased. Also, the wrist load factor significantly affected perceived discomfort in the shoulders.
Conclusions
A correlation was found between the right shoulder's RPD, and the right upper trapezius’ mean amplitude affected by increased wrist load. The mental load produced by the precision task was classified as medium, and the performance factor was the most representative.
Introduction
Upper limb pain resulting from working over-shoulder is a usual preoccupation in the modern workplace. 1 The researchers have identified some risk elements such as strength, accuracy, and task pressure as promoters of musculoskeletal disorders in upper limb work-related. 2 Precision effort is relevant in grasping, pinching, and other occupational control tasks. 3 However, manual precision tasks are causative of pain and dysfunction, reflected in increased worker absenteeism. 4 The U.S reported in 2014 the incidence rate for nonfatal occupational injuries where 32% of them corresponded to upper extremities (shoulder 8.2%, arm 4.9, wrist 4.1, and hand 12.7). 5 In Europe, between 2013 and 2018, the enthesopathy (inflamed and painful joints) grew by 12%, and mononeuropathies of the upper limb (affecting a single peripheral arm nerve, such as carpal tunnel syndrome) increased 13%. 6
The manual precision task reduces postural sway, demands visual fixation, and carries to individual adopts an inflexible posture freezing musculoskeletal system.7,8 During movement control of manual precision tasks increase the rigidity demands of the shoulder arm, causing upper limb tension. 9 Scientific tests exhibit that a rise in muscle activity correlated with increased precision demands. 10 The industry has proposed alternatives to mitigate risk factors, such as task accuracy on the musculoskeletal system. Interventions include transforming machinery work methods and getting new tools or other devices to work. 11 Many of these devices can be expensive, space occupied, and not used their capacity. Then, industrial designers have mitigated some limitations by designing industrial exoskeletons. Researchers define the exoskeleton as an outer covering of a creature to support armor, increase power or detection, and the fusion of information. 12
The purpose of the exoskeleton is to safely increase human work activities, supporting the back, feet, and arms. 13 These exoskeletons allow humans to safely generate the physical power required for a given task. 14 The researchers have classified exoskeletons according to their various states of power (active or passive) and structures (hard or soft). 15 While active exoskeletons comprise one or more actuators to increase human power, passive systems use materials, springs, or shock absorbers to collect and store energy from human movement, to then release this energy to support a posture or movement. 16 In human motion environments, the operator loads the exoskeleton, and it adapts to human flexibility and imagination and does not require programming and teaching, advantages over robotic equipment. 17
Researchers have recently evaluated different over-shoulder occupational tasks with the assistance of an exoskeleton, and most of these tasks were precision-demanding. Most of the investigations have been in the laboratory, with tasks requiring precision where a tool is held by hand and executing a maximum of two height levels. Some of the findings are listed below.
Rashedi et al. 18 established that the device's design did not allow participants to perform the job comfortably. Kim et al. 19 and Kim et al. 20 found an increase in the number of errors made during the intermittent repetitive drilling task, and reduced completion time by nearly 20% at the overhead height and a reduction of the spinal load, seeing a decrease in work at shoulder height and the drilling task, and an increased peak lateral shear force during the wiring task due to the use of the exoskeleton. Alabdulkarim et al. 21 detected that the working height with shoulder and elbow flexed at 90° and set the Maximum Acceptable Frequency (MAF), indicating potential productivity. The error generated during the additional 3-min periods after adjusting MAF was the performance index. They found the lower quality or no impact quality. Alabdulkarim et al. 22 found that precision increasing led to increases in some metrics of muscle activity. However, they did not detect significant precision effects on most physical demand metrics, potentially because such effects depend on the speed of the task as other investigations have reported. Maurice et al. 23 determined that the exoskeleton utilized does not positively or negatively affect task performance, conversely to another research. However, the exoskeleton mitigated physical strain on the shoulder where anterior deltoid activation reduced 55%. Schmalz et al. 24 found a reduction of muscle forces to perform the overhead work activities with the exoskeleton; the EMG amplitudes of the deltoid and biceps brachii muscles were the most decreased, which are the most important generators of the forces required to perform shoulder anteversion. Kim et al. 25 showed that using the exoskeleton contributed to a reduction in physical demands, Activity levels of the shoulder muscles, and the number of errors made during the drilling. Hyun et al. 26 found that the exoskeleton reduced muscle activity percentage in the overall experiment. However, the assistance percentage of the device decreases as the load on the arms increases by the design of the exoskeleton. Pacifico et al. 27 showed that activations of muscles anterior deltoid, medial deltoid, trapezius ascendant, and pectoralis major have significantly reduced physical strain when using the passive upper-limb exoskeleton. Van et al. 28 found an effect of peak torque amplitude provided by the passive exoskeleton decreased median and peak shoulder muscle activity. Gillette et al. 29 found a decrease in fatigue risk factor with the exoskeleton resulted from a reduction in EMG amplitude and a reduction in duty cycle. Furthermore, the EMG amplitude of the anterior deltoid fell below the threshold limit values. de Vries et al. 30 found that muscle activation was decreased in all tasks for most agonist muscles, especially for tasks that require less varied movements, and which involve overhead work.
Previous investigations broadly present the distinct factors evaluated with and without the assistance of an exoskeleton. However, they show that the type of exoskeleton used, the height of the task, and the kind of task (repetition, precision) change muscle activation response and the perceived discomfort. We found in this review that the tasks have been evaluated at a maximum of two heights and that the impact of the precision task on muscular activation has been little studied, as established in many investigations.31–34 Then, the objective of the present study was to investigate the effects of muscular activation, perceived discomfort, and mental workload of the repetitive precision task at three heights over-shoulder, with vs. without the exoskeleton, and with vs. without wrist load. We hypothesized that using an exoskeleton to perform a precision task with different changes in height for the task and load on the wrists reduces activation of the shoulder muscles and hand muscles to pinch grip.
Material and methods
The study was carried out to identify the behavior of muscle activation of the anterior deltoid, middle deltoid, upper trapezius, and abductor pollicis brevis in a precision electrical wiring task when intervened with a passive exoskeleton for the upper extremities. For this purpose, an experiment was proposed with three factors (with and without an exoskeleton, with and without weight on the wrists, and three execution heights). In addition, a passive exoskeleton and a structure with variable heights were designed and built to carry out the experiment. The participants performed 12 experimental levels, capturing for each of them the maximum voluntary contractions of each of the muscles of both extremities based on protocols established in the literature. The test subjects were instrumented with surface electrodes following skin cleaning and muscle localization protocols standardized in the literature. Muscle signals were captured and processed using a Noraxon Clinlical DTS Receiver 3.6 ® (Noraxon, USA Inc., AZ, USA). Additionally, an evaluation of perceived discomfort was carried out using a body map and a Borg-10 discomfort scale. The mental load was measured at the end of the experiment with the NASA-TLX methodology and compared to the execution of the task with and without the exoskeleton. Electromyography data were normalized in Noraxon® software and treated in SPSS 26® software (SPSS® Inc, Chicago, IL, USA) in several analyses of variance (ANOVA) of within-factors repeated measures.
Participants
A convenience sample of sixteen participants (male: eleven, female: 5) from the workers and students at the university was employed. Before the experiment, musculoskeletal disorders in the last year were inquired, and everyone was right-handed. After verification, the experimental conditions were approved by the Research Ethics Committee of Universidad Autónoma de Ciudad Juárez number CEI-2023-1-898, and those who met the requirements signed the consent. Corresponding means and (SD) of age and body mass of participants were 34.3 (11.4) yrs. and 78.9 (19.4) kg.
The exoskeleton
The exoskeleton designed for this research consists of an aluminum T-structure placed in the back of the participants. A couple of arm supports are placed in the extremes of the “T”. The whole structure is fixed to the body using a belt placed around the waist of each participant. Figure 1 shows the design of the exoskeleton.

Exoskeleton used in the research.
Experimental design
Twelve combinations of an overhead precision task were simulated. The combinations were obtained from the relationship between the intervention factor (with vs. exoskeleton), wrist load (with (0.5 Kg) vs. no load), and task height (three height levels). Each participant had a random sequence of execution of the next twelve combinations:
S1S Without exoskeleton, task height 1, without wrist load S1P Without exoskeleton, task height 1, with wrist load S2S Without exoskeleton, task height 2, without wrist load S2P Without exoskeleton, task height 2, with wrist load S3S Without exoskeleton, task height 3, without wrist load S3P Without exoskeleton, task height 3, with wrist load C1S With exoskeleton, task height 1, without wrist load C1P With exoskeleton, task height 1, with wrist load C2S With exoskeleton, task height 2, without wrist load C2P With exoskeleton, task height 2, with wrist load C3S With exoskeleton, task height 3, without wrist load C3P With exoskeleton, task height 3, with wrist load
The experimental design was of repeated measures to collect the data. The experimentation was conducted in at least two sessions, separated by at least one week between them. The experiment was carried out in approximately three months due to the availability and rotation of the participants to carry out all the stages proposed in the research. The first meeting took at least an hour to explain the experiment, data collect form formats, data collection teams, and practice.
A wooden structure (see Figure 2) with variable height and three positions for the task was built. The reference point to locate the first position of the task was defined at a level and 15 inches from the frontal point (frontal plane) of the participant's vision, forming an angle of 0° with the transverse plane. Then, other heights were established vertically at each participant's eye level, 7.8 (45°) and 11.8 (90°) inches. A ratcheting exoskeleton assisted with the task. The wearable (see Figure 1) was built in 3d printing with a mass = 3.0 kg, four arm positions, and adjustable components such as back width, back support, vest, and belt. The armload was simulated with a pair of dumbbells adjustable to the wrist, Jap®, and mass = 0.5 kg each.

Electrical connectors, first task height leveled at eye level, and electrical connector assembly without and with exoskeleton.
Experimental task
The experimental work was an interpretation of an electrical occupational job. These occupational jobs often involve working on the ceiling, resulting in strenuous work in positions with arms/hands above shoulder level and with the neck bent back. 35 Kim et al. 19 performed this kind of occupational task of connecting electrical wiring in his exoskeleton testing experiments. Then, a precision and repetition assembling of ten electrical connectors (see Figure 2) was executed above shoulder level. The electrical connector has two parts known as “male” and “female,” where the male is the part that is inserted as a complement to the connector. The “male” has two elements that must be inserted into the guide holes of its counterpart. The task was performed at three heights. The first height of the task was located at the level of the participant's eyes (see Figure 2), ensuring the consistency of this factor as performed. 36 Ten electrical connectors were fixed in each height position, spaced at the same distance, 2.8 inches.
Electromyography (EMG) recordings of muscle activity
Eight Covidien_H124SG® surface electrodes were distributed between the two upper extremities and positioned in the abductor pollicis brevis, middle deltoid, anterior deltoid, upper trapezius muscles following the protocol described by SENIAM. 37 Electrodes were interfaced with a wireless transmitter with a Noraxon Clinlical DTS Receiver 3.6 ® (Noraxon, USA Inc., AZ, USA). Maximum voluntary contraction (MVC) was obtained unilaterally for the abductor pollicis brevis and upper trapezius muscles and bilaterally for the middle and anterior deltoids. Still, the recording of the electromyography signal in the execution of the task was bilateral.
Rating of perceived discomfort
A questionnaire to identify bodily discomfort was applied, recognizing the location of the inconvenience on a body map. The map highlighted the following body points: left elbow (LT_Elbow), left arm (LT_ Upper arm), left shoulder (LT_Shoulder), neck (Neck), right shoulder (RT_Shoulder), right arm (RT_Upper arm), right elbow (RT_elbow), left hind thigh (LT_ Hind thigh), right hind thigh (RT_Hind thigh), left foot (LT_Foot), right foot (RT_Foot), high back (Upper back), mid back (Middle back), low back (Low back), buttocks (Buttocks), left fingers (LT_Fingers), right fingers (RT_Fingers), left wrist (LT_Wrist), right wrist (RT_Wrist), left hand palm (LT_ Hand palm), right hand palm (RT_ Hand palm), others. The discomfort was assessed under a Borg scale (0–10) of discomfort proposed. 38
Procedure
The experimentation began by placing the test structure at the level of the participant's eye. Next, the participant was instrumented. The muscles right Abductor pollicis brevis (RT_ABD_P), right middle deltoid (RT_MDEL), right anterior deltoid (RT_ADEL), right upper trapezius (RT_UPP_TRAP), left Abductor pollicis brevis (LT_ABD_P), left middle deltoid (LT_MDEL), left anterior deltoid (LT_ADEL), left upper trapezius (LT_UPP_TRAP) of each upper limb were identified. The body areas were cleaned for the location of the surface electrode. Each electrode was evaluated, and its signal was confirmed in the Noraxon 3.6 software ®. Once the electrodes were verified, each muscle's MVC measurements were carried out based on the protocols established by many researchers.39–42 Then the participant performed a random combination of the task of the twelve that were part of the experiment, and the signal from the electrodes was captured. The participant then got a break for at least ten minutes. During this break, a questionnaire to identify bodily discomfort was applied, recognizing the location of the inconvenience on a body map and assessed under a Borg scale (0–10) of discomfort proposed, 38 and if the exoskeleton was utilized in the try, another discomfort questionnaire under the Borg scale (0–10) was applied. Finally, a NASA-TLX survey was used at the end of the experiment to determine the workload with vs without exoskeleton.
EMG analysis and statistical analysis
The raw electromyography signals were smoothed with the Root Mean Square algorithm (RMS) by Noraxon 3.6 ®. Normalized EMG (nEMG) values were then obtained using corresponding maximum values obtained during MVCs. Statistical analysis was performed in SPSS 26 (SPSS® Inc, Chicago, IL, USA). A repeated measures three-factor (intervention, wrist load, and task height) analysis of variance (ANOVA) test and post hoc analyses (Bonferroni significant difference test) were performed to determine significant differences between muscles. In addition, student t-tests of independent means comparisons between similar muscles of opposite extremities were performed.
Results
Anthropometric measures
The anthropometric measurements of the right upper limb were recorded with ErgoTechMX® instruments, obtaining mean (SD) values for the body segments shoulder-width 41.6 (3.9) cm, stature 168.9 (9.6) cm, length of arm 35.1 (2.3) cm, forearm 27.6 (2.3) cm, and length of hand 18.2 (1.1) cm.
Reliability of nEMG measurements
Across the intervention, task height, and wrist load factors, the averaged mean amplitudes of the eight muscles had concordance values (ICC: Intraclass Correlation Coefficient) for single measures within the range of 0.45 (regular) to 0.99 (excellent) without the use of the exoskeleton and 0.73 (good) to 0.99 (excellent) with the help of the exoskeleton. The lowest ICC ranges from (0.28–0.73) to 95% confidence for the group of conditions S1S, S2S, S2S, S1P, S2P, y S3P.
Rating of perceived discomfort (RPD)
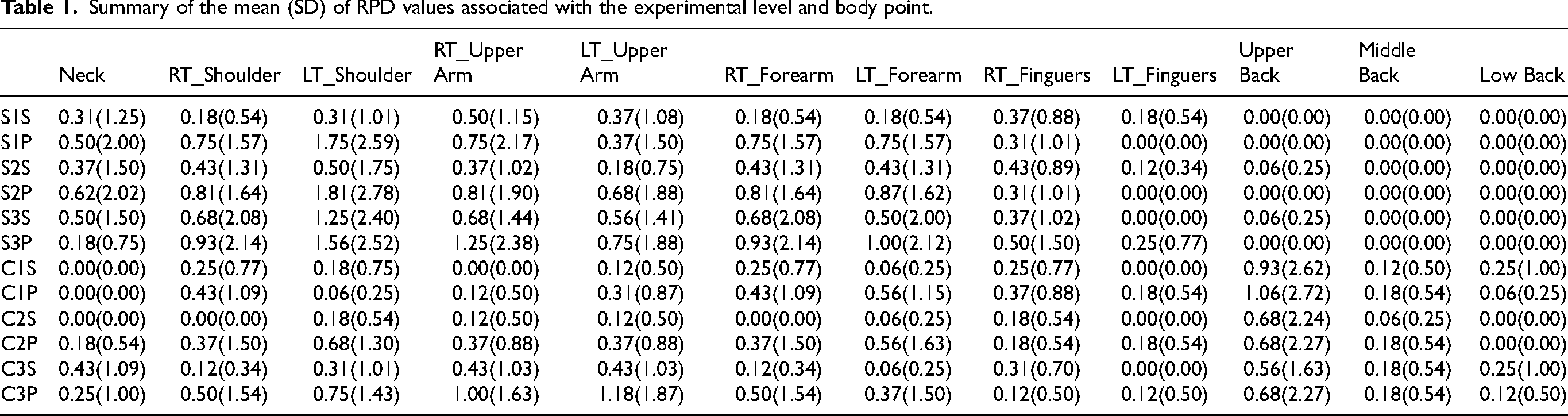
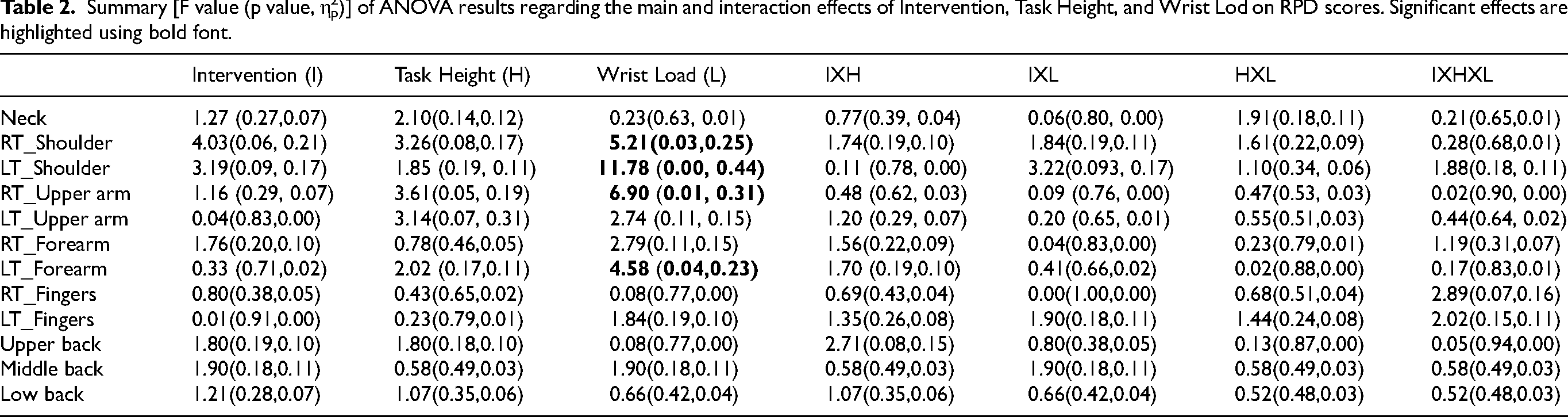
Table 1 summarizes the mean (SD) RPD values by experimental levels and body points, and Table 2 summarizes the ANOVA results for RPD assessments. For RPD of the RT_Shoulder, LT_Shoulder, RT_ Upper_Arm, and LT_Forearm, a significant main effect was found for wrist loading. In the case of the RT_Shoulder, there was a difference (SD) of 0.354 (0.155) caused by load use. Similarly, for the LT_Shoulder 0.646 (0.188), the RT_ Upper_Arm 0.365 (0.139), and the LT_Forearm, 0.469 (0.219) caused using load.
Summary of the mean (SD) of RPD values associated with the experimental level and body point.
Summary [F value (p value, η2p)] of ANOVA results regarding the main and interaction effects of Intervention, Task Height, and Wrist Lod on RPD scores. Significant effects are highlighted using bold font.
MVC statistics
Table 3 SD of the mean amplitude and the maximum of the MVC in percentage (%) for each muscle.
The mean (SD) of the mean amplitude and the maximum of the MVC in percentage (%).

Analysis of the nEMG
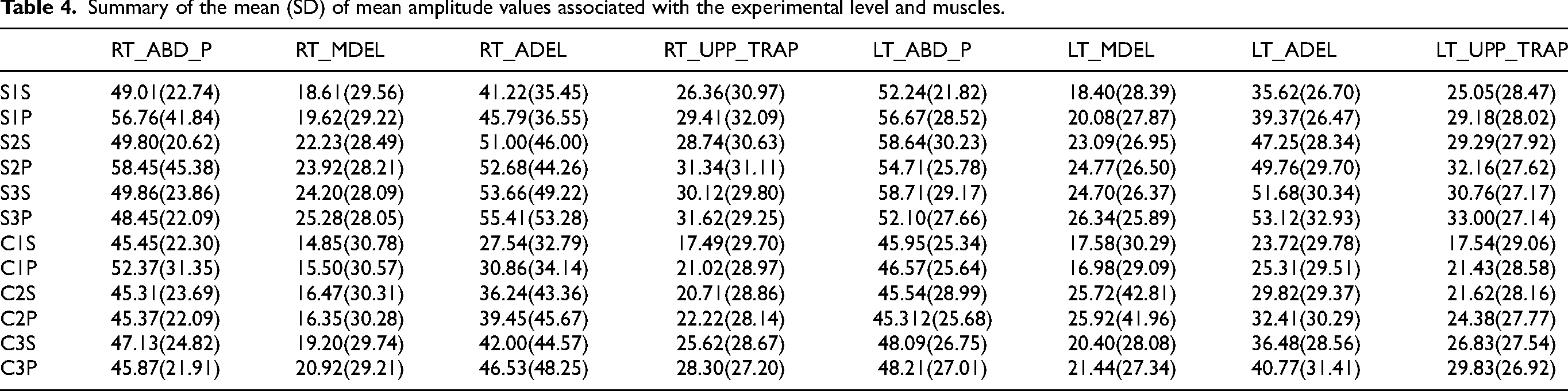
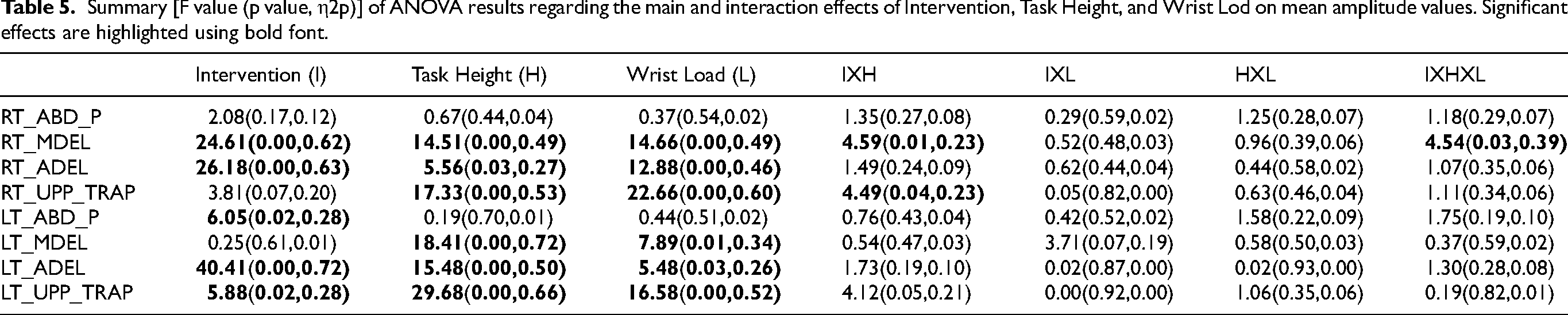
Table 4 SD of the mean amplitude of the nEMG, and Table 5 summarizes the results of the ANOVA of the mean amplitude, respectively. The main effect of I, H, L, and an interaction effect of IXH, and IXHXL was found on the RT_MDEL muscle, with a 22.8% reduction when using the exoskeleton, increases of 13.1%, 23.4%, and 11.8% between H1H2, H1H3, and H2H3, and a 4.9% increase when using a 0.5 kg wrist load. The interaction effect in IXH is caused by factor I, achieving reductions when using the exoskeleton of 20.6% in H1, 28.8% in H2, and 18.9% in H3; likewise, the interaction effect in IXHXL is caused by factor I, achieving reductions of 20.2% in the H1L1 combination, 21.0% in H1L2, 25.9% in H2L1, 31.6% in H2L2, 20.6% in H3L1, and 17.2 in H3L2 when using the exoskeleton. For the RT_ADEL muscle, the main effects of I, H, and L were found, with a decrease of 25.7% when using the exoskeleton, an increase of 9.2% between H2H3 and not significant among the other comparisons of heights, and a rise of 7.0%. when using a 0.5 kg load on the wrists. Effects of H, L, and an interaction effect of IXH were determined in the RT_UPP_TRAP muscle, with increases of 8.4%, 18.5%, and 10.9% between H1H2, H1H3, and H2H3, and a rise of 9.0% when using a load 0.5 kg on the wrists. In the IXH interaction effect, the two factors affect the interaction, but factor I is only significant in the interaction only on the H1 condition. While factor H is significant in the two states of I, with an increase of 7.1% between H1H2 without the exoskeleton, 28.6% between H1H3, and 20.3% between H2H3 with the exoskeleton. In the case of the LT_ABD_P muscle, the main effect of I was found, with a 16.0% reduction when using the exoskeleton. For the LT-MDEL muscle, two main effects caused by H and L were found, with an increase of 21.3% between H1H3 and 4.5% when using a 0.5 kg load on the wrists. For the LT_ADEL muscle, the main effects of I, H, and L were found, with a decrease of 31.8% when using the exoskeleton, increases of 22.1%, 31.8%, 12.5% between H1H2, H1H3, and H2H3, and an increase of 6.7% when using a 0.5 kg load on the wrist. In the LT_UPP_TRAP muscle, the main effects of I, H, and L were found, with a decrease of 21.1% when using the exoskeleton, increases of 13.2%, 22.6%, 10.7% between H1H2, H1H3, and H2H3, and an increase of 11.1% when using a 0.5 kg load on the wrist.
Summary of the mean (SD) of mean amplitude values associated with the experimental level and muscles.
Summary [F value (p value, η2p)] of ANOVA results regarding the main and interaction effects of Intervention, Task Height, and Wrist Lod on mean amplitude values. Significant effects are highlighted using bold font.
Workload assessment-NASA-TLX
The workload evaluation with the NASA-TLX method yielded workload indexes with a mean (SD) without the exoskeleton 44.977 (14.996) and 49.778 (13.291) with the exoskeleton. The mean values of the workload index fall in the range (26–50) of the interpretation scale, indicating that the workload is valued as mean. Additionally, a T-test for correlated samples was run to determine differences. A statistic T(15): −1.116, bilateral p-value: 0.283 was found.
A Friedman test evaluated the distributions of mental demand, physical demand, time demand, performance, effort, and frustration. The hypothesis tests generated a sig = 0.000, indicating that the distributions of factors are different. Pairwise comparison found significance between frustration-effort (0.025), frustration-performance (0.00), mental demand-performance (0.040), physical demand-performance (0.060), and time demand performance (0.010). However, the significance values were adjusted using the Bonferroni correction for several tests, determining significance only between the frustration-performance pair (0.001).
RPD and nEMG correlation
For RPD of the RT_Shoulder, LT_Shoulder, RT_ Upper_Arm, and LT_Forearm, a significant main effect was found for wrist loading.
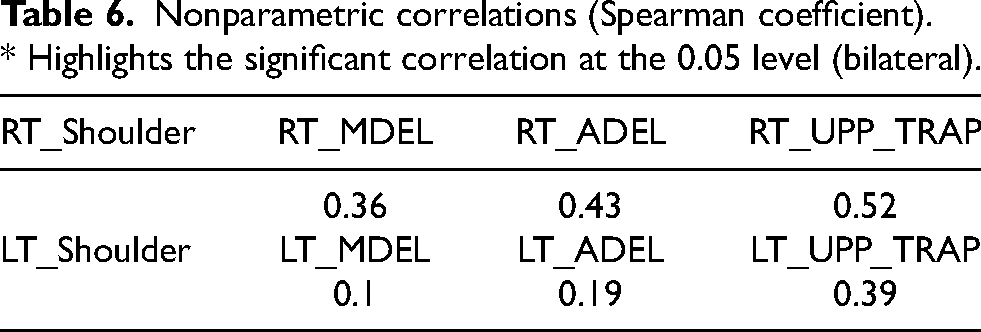
Similarly, this effect of the load on the wrist was found for the RT_MDEL, RT_ADEL, and RT_UPP_TRAP muscles and LT_Shoulder with the LT_MDEL (0.10), LT_ADEL (0.19), and LT_UPP_TRAP (0.39). The correlation between RT_Shoulder with the RT_MDEL, RT_ADEL, and RT_UPP_TRAP muscles and LT_Shoulder with the LT_MDEL (0.10), LT_ADEL (0.19), and LT_UPP_TRAP (0.52) muscles were evaluated with Spearman coefficient. Table 6 summarizes the coefficients of Spearman found for each of the relationships. A single significant correlation between RT_Shoulder and RT_UPP_TRAP was determined.
Nonparametric correlations (Spearman coefficient). * Highlights the significant correlation at the 0.05 level (bilateral).
Discussion
Previous investigations broadly present the different factors evaluated with and without the assistance of an exoskeleton. They showed the type of exoskeleton used, the height of the task, and the kind of task (repetition, precision) change muscle activation response and the perceived discomfort. Nevertheless, we found in this review that the tasks have been evaluated at a maximum of two heights and that the impact of the precision task on muscular activation has been little studied, as established in investigations.31,32 Then, the objective of the present study was to investigate the behavior of muscular activation, perceived discomfort, and mental workload of the repetitive precision task at three heights over-shoulder, with vs. without the exoskeleton, and with vs. without wrist load. We hypothesized that using an exoskeleton to perform a precision task with different changes in height for the task and load on the wrists reduces activation of the shoulder muscles and hand muscles to pinch grip.
Rating of perceived discomfort (RPD)
The result showed that the significant discomfort in the body was in the middle back when participants performed the experimental levels C1S, C1P, C2S, C2P, C3S, and C3P (see the mean (SD) of RPD values in Table 1). All discomfort appeared when participants used the exoskeleton. The exoskeleton presses the middle back. In contrast to our results, it was found a significant main effect for the intervention factor (with and without exoskeleton), managing to reduce discomfort between 27% and 29% for the shoulder, elbow, and upper back; however, this effect was only achieved by one of the three exoskeletons used in the intervention. 43 Based on the above, we could say that the design of the exoskeleton is a factor that influences the operator's performance.
Most discomforts were caused by experimental level S3P. It affected RT_Shoulder, RT_Upper arm, LT_Forearm, RT_Fingers, and LT_Fingers (see the mean (SD) of RPD values in Table 1). The mean value maximum was 1.250 (2.3) associated with RT_Upper arm. We hypothesize that the position of the right upper extremity causes the discomfort reflected on RT_Upper arm. Figure 3 shows how the joint pattern of the right limb moves as the exoskeleton is left, and the task is carried out without load, and with load, the limb reaches its maximum elevation when the load is added to the wrist.

Change of joint pattern with and without exoskeleton and load on the wrist.
The maximal values of discomfort mean (SD) are related to LT_shoulder (1.813 (2.786), S2P), and LT-Upper arm (1.888 (1.870), C3P). In the first case, we speculate that shoulder flexion angle combined with wrist load provoked a significant torque. In the second case, we observed that the exoskeleton design forced the arm to take a position that generated discomfort. Both situations can be seen in Figure 4.

Discomfort in the shoulder and left arm with and without an exoskeleton, but with load in both experimental cases S2P and C3P.
Table 5 shows highlighted using bold font significant values which correspond to the load factor on the wrist (L). The table also shows that the intervention (I) and the interaction between the intervention and the load on the wrist (IXL) did not have a significant effect. The factor Wrist Load (L) produced an effect over four body segments. The difference of means (value), with and without load, were for RT_ Shoulder (0.354), LT_Shoulder (0.646), RT_Upper arm, and LT_Forearm (0.469). Additionally, Table 1 shows us that the maximum value of discomfort was in LT_Shoulder associated with the experimental level S2P. However, when comparing our results with those of, 20 where they found that the intervention and the interaction between the intervention and the type of task had a significant reduction effect on forearm discomfort; still, it was predominant in the task where the weight (load) of the drill was used to perform the task was increased. Their results contrast with our findings. We believe that the results are opposed to others due to the type of task and the design of the exoskeleton.
MVC
The normalized average mean amplitude of practical level vs. muscle is between 58.7% to 9.3% MVC (see Table 5). Additionally, five muscles had maximal and minimal values when participants performed S3P and C1S experimental levels. However, 58% MVC was recorded in both thumb abductors muscles (LT_ ABD_P and RT_ ABD). We hypothesize that was caused for the precision task. In the case of LT_ABD_P muscle, the hand had to do a static pinch action to grab “the female” assemble component and hold the left hand immobile or rigid to align “the male” component with “ the female” assemble component the pinch and rigid cause higher muscle activation. In the same way, the RT_ABD_P muscle had a higher activation because “the male” element has a flexible pin that needs to be compressed and aligned with the component by inserting it into its “female” counterpart.
The nEMG
When the exoskeleton was used, the intervention factor had a main effect on the, LT_ABD_P, LT_UPP_TRAP, RT_MDEL, RT_ADEL, LT_ADEL and, achieving reductions in muscle activation between 16% and 31.8%. The objective of the intervention was to reduce muscle activation with the use of exoskeleton. The most considerable reductions occurred in muscles RT_ADEL and LT_ADEL, responsible for shoulder flexion. Previous studies have confirmed that Exoskeleton decreases shoulder muscle activity and fatigue; how is the case of. 44 Also, we found that the middle deltoid and trapezius significantly reduced muscle activity when wearing an exoskeleton for all plastering activities 30 ; as well, it was found a significant effect on the reduction of anterior deltoid muscle activity in the interaction of the intervention factor (with and without exoskeleton) and other factors such as gender, height, and direction of force 43 ; In addition, they found for the trapezius muscle a significant main effect caused by the intervention factor, and by the interaction of the intervention factor with the height of the task and direction of force factors; however, in the case of the middle deltoid, a significant reduction in muscle activation caused by one of the three exoskeletons evaluated was only achieved in the medium height condition. Additionally, it was determined that the physical demands were different for the same task but with different exoskeletons. Thus, we thought that the reduction of the activity of the RT_UPP_TRAP was not achieved due to the requirement of precision of the task and how the assembly must be carried out; this causes a shoulder lift and kind of exoskeleton. 21 Therefore, we believe a relationship between the task and the design of the exoskeleton affects physical demand where reductions in muscle activity using the exoskeleton where found (see Figure 5).
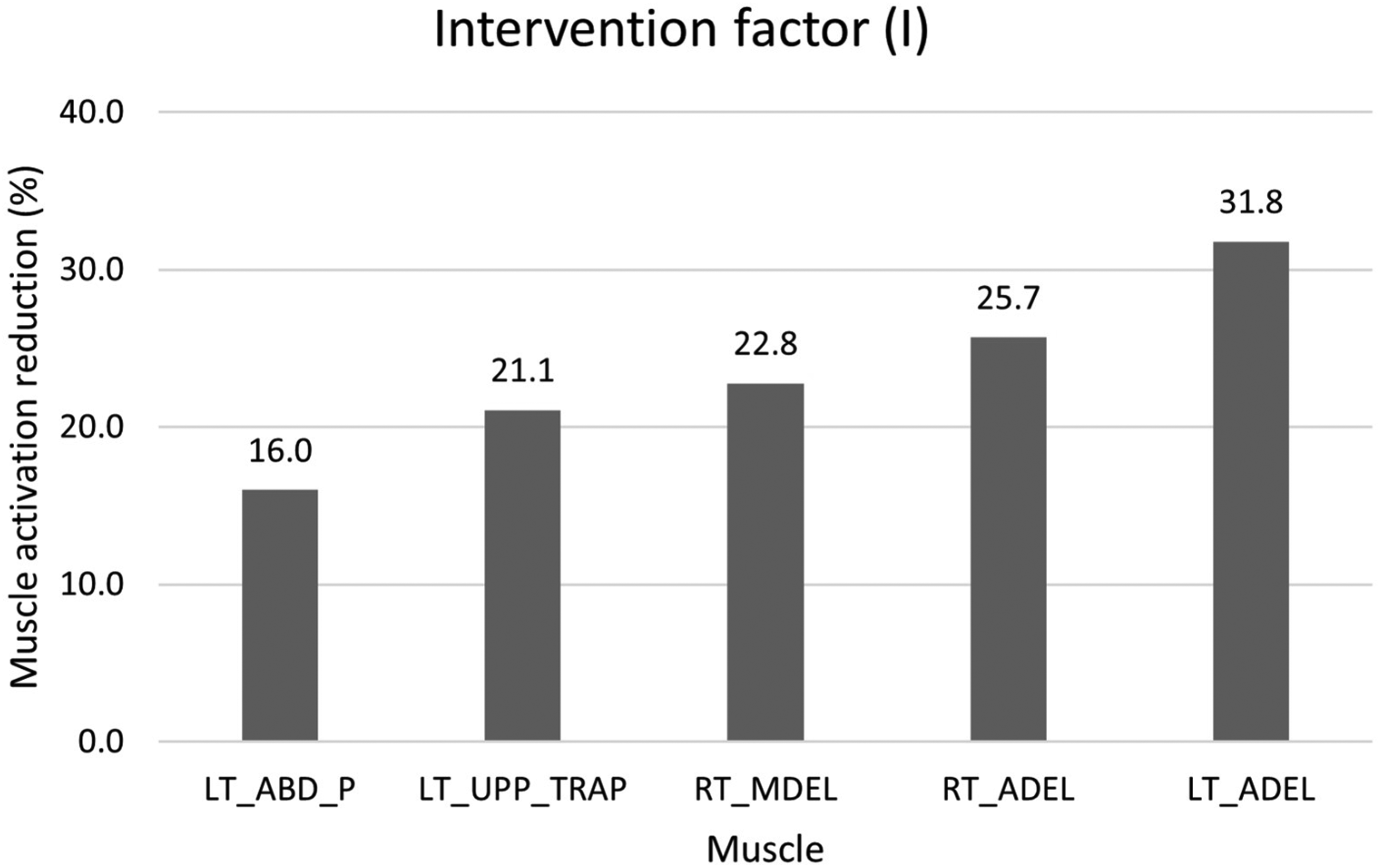
Muscle activation reduction with the use of the exoskeleton.
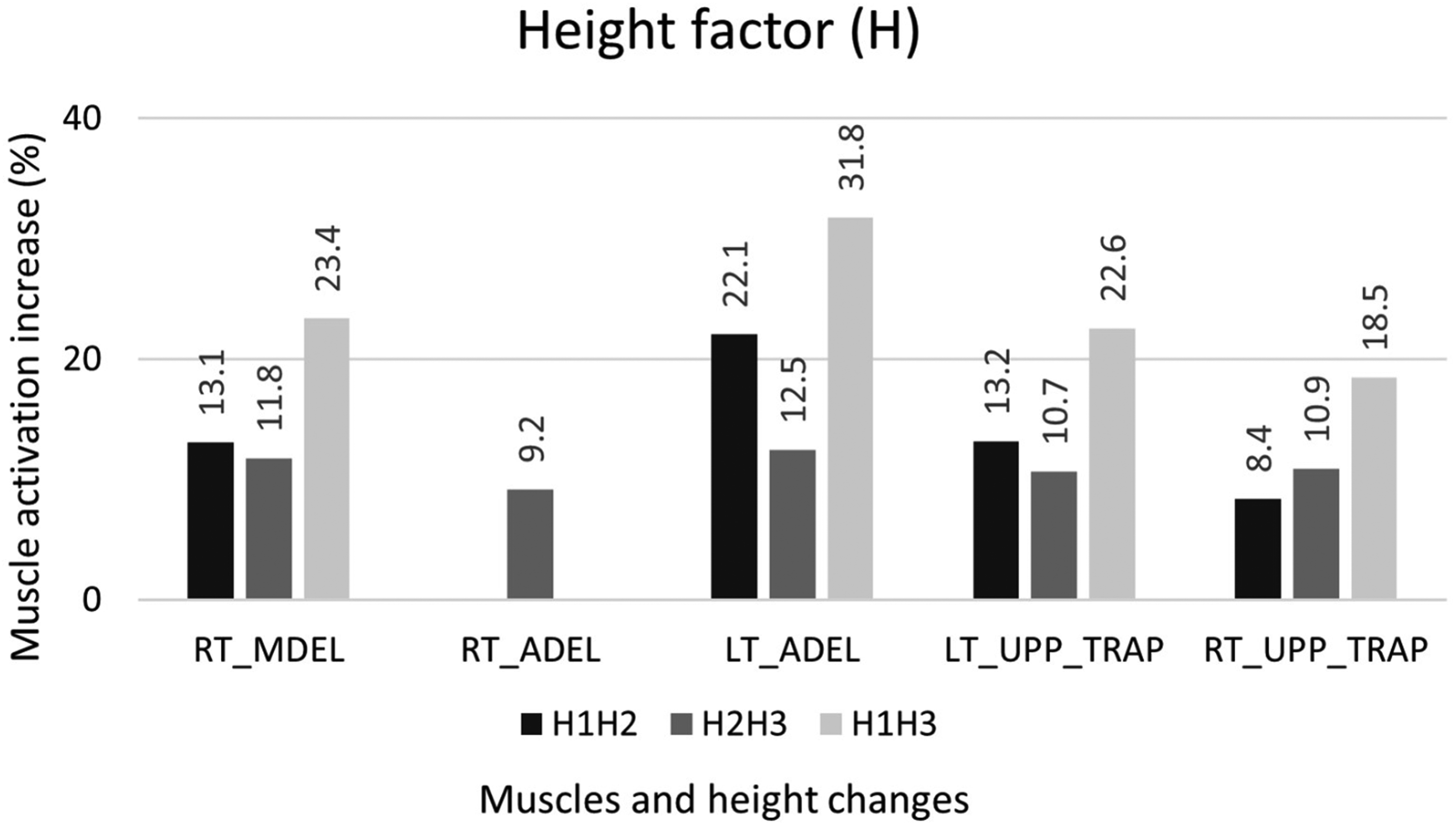
Muscle activation increases between changes in task height.
On the other hand, the height factor of the task had a main effect on the increase in the amplitude of the deltoids and trapezius of both extremities, with increases between 9.2% and 31.8% (see Figure 6). However, in Figure 5, you can see a pattern where the largest increases in muscle activation occur from height 1 to 2. In relation to the above in the evaluation of two exoskeletons, the exoskeletons were most effective at arm angles of 90 and 120 degrees and relatively ineffective at 30 degrees. 45 Then, we hypothesize that this increase is caused by the flexion angle of the shoulder (see Figure 4), which increases when changing between heights 1 and 2, which causes a greater torque at height 2. In contrast, pairwise differences were not found for a given task height between exoskeleton types and the arm-supported exoskeleton condition; however, they did determine a significant effect on the interaction between the intervention (with and without exoskeleton) and the height of the task. 43
In the same way, the load factor in the wrist increased the activation of the muscles associated with the shoulders. We associate this reaction without intervention with the mechanical effect of torque on the shoulder (see Figure 7). However, when the exoskeleton was used, we hypothesize that it was caused by the design of the equipment. The equipment uses a ratchet to change between positions, which makes its adjustment vary based on the anthropometry of the participants. On the other hand, it can be seen that the LT_ABD_P muscle had the highest percentage increase. We speculate that the cause is the static position of the left upper extremity associated with the “female” component pinched with the fingers.
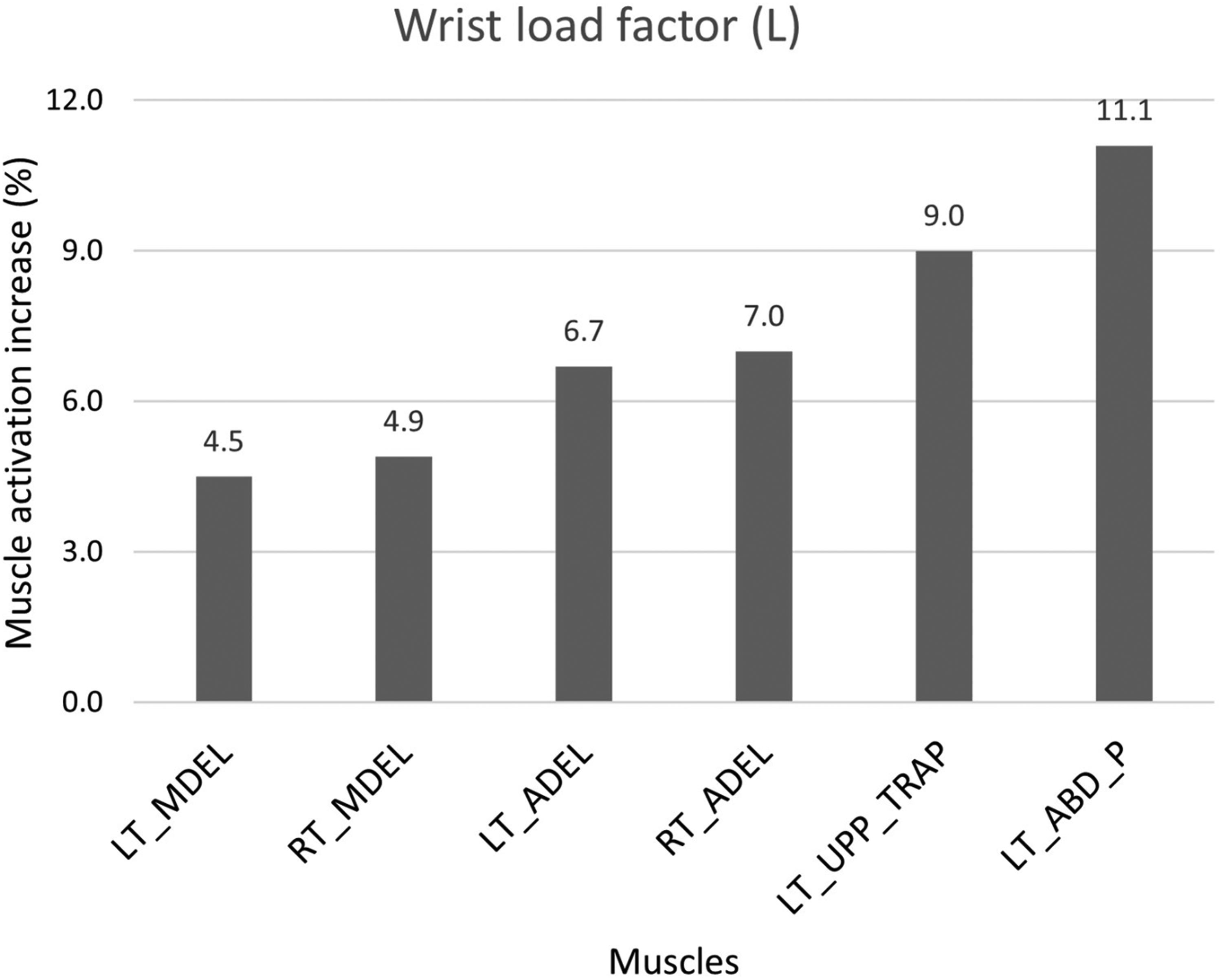
Muscle activation increases between changes in wrist load.
The interaction of the intervention factors and height had a predominant effect due to the height factor with increases in the muscle activation of the RT_UPP_TRAP of 7.1% (without) and 28.6% (with) and a decrease between 18.9% and 28.8% in muscle activation of the RT_MDEL when using the exoskeleton, and the interaction of the three factors had an effect caused by the intervention factor, generating a decrease of 20.2% in the muscle activation of the RT_MDEL when the exoskeleton was used.
Wrist loading was the incisive factor on RPD, and this factor displayed discomfort on both shoulders, right upper arm, and left forearm. Although the torques were not calculated for this purpose, we speculate that this mechanical effect caused by the increased load is the cause of the significance of the perceived discomfort. Additionally, a considerable positive correlation was found between the RPDs of the RT_SHOULDER and EMG of the RT_UPP_TRAP. We speculate that the reason is the postural load from lifting the shoulder and head when performing the precision task, although a posture study was not conducted in this investigation. For example, the body turns on the transversal plane, heel lift, back arch, angular displacement on the coronal plane, and body support on one of the lower extremities.
Workload assessment
The Nasa TLX index was interpreted as a mean value of the mental workload for both intervention situations (with and without exoskeleton). No significant differences were found between the intervention cases. Nevertheless, the significance without adjustments displays a significant association between the performance factor and the others. In addition, the interaction triangle formed between performance, effort, and frustration factors were observed. However, the post hoc test for correcting differences highlights only the significance of frustration-performance pair. We think that the reason for forming this triad is associated with trying to accomplish the task in the shortest time possible. However, the post hoc test for correcting differences highlights only the significance of performance-frustration. Also, when asking the participant about their frustration, they stated that the reason was to complete the task on time, which is associated with performance. Additionally, we believe that in our experiment, the intervention was not significant in the differences in the mean assessment of the mental workload index by type of task; our task required pinching with the hand, while in the case of the task was demanding in supporting the weight of the felling with the upper extremity. Finally, we intuit that the reason why the most relevant factor is performance is because of the task; the task required rigidity of the musculoskeletal system and concentration to be able to clamp, align and assemble the two components, which caused failed assembly attempts, which the participant perceived as a decrease in performance level, increased frustration, and effort. 23 So, we think it is why in the post-hoc evaluation, performance and frustration are associated with a significant level.
RPD and nEMG correlation
A correlation was found between RT_Shoulder discomfort and RT_UPP_TRAP. Additionally, it is known that the RT_UPP_TRAP intervenes in the shoulder's adduction, rotation, and elevation. Thus, we assume that the correlation is marked only in the RT_UPP_TRAP by the right shoulder's higher, adducted, and rotated position concerning the left shoulder.
Limitations of the study
Our results suggest that the exoskeleton decreases the physical demand. However, the study has some intrinsic limitations. The most important condition was that our participants were students and university administrative personnel, not productive system operators. A second restriction was the anthropometric difference, the age difference between participants, and the lack of motor and physical ability to perform an industrial task, while expert operators, due to their experience, perform different gestures to novices. A third delimitation was that the participants were not submitted to the conditions of noise, heat, hours, storm pressure, and temporary performance typical of the natural work environment, which means that the laboratory participants do not perceive situations of discomfort regularly of the use of the exoskeleton, repetitions of the task (concentration, clamping, alignment, and assembly) and forced body postures for long periods. Thus, the present results should be considered carefully. This is our first step in evaluating the operator performing overhead tasks with the assistance of an exoskeleton, as other research.20,24,46 Also, with non-expert participants has done, therefore, we know the next step must be taken to an approach to the evaluation of interventions with an exoskeleton in industrial environments. 27 A fourth limitation is the use of sensors to capture muscle activation signals. In our study, we appreciate the difficulty of keeping the sensors fixed and their number when using the exoskeleton, and this would be a big instrumentation problem with real operators. A fifth barrier was the design of the exoskeleton. Our exoskeleton was controlled by a four-position ratchet, limiting the upper extremities’ positions and mobility, and generating discomfort. The design of the exoskeleton is a variable of interest for future studies. Finally, some additional measures could provide valuable information in future laboratory experiments. For example, tracking postural patterns, joint geometry, plantar pressure, and monitoring of eyesight fixation adopted by the participants.
Conclusions
Overhead work remains very common in many work fields and is a frequent cause of shoulder work-related musculoskeletal disorders. Different alternatives are appearing or improving to minimize this risk; this is the case of passive exoskeletons. The objective of the present study was to investigate the effects of muscular activation, perceived discomfort, and mental workload of the repetitive precision task at three heights over-shoulder, with vs. without exoskeleton, and with vs. without wrist load. Besides, we hypothesized that using an exoskeleton to perform a precision task with different changes in height for the task and load on the wrists reduces activation of the shoulder muscles and hand muscles to pinch grip. Then, using an exoskeleton of our design for the experiment, we reduced muscle activation between 16% and 31.8% in the left abductor pollicis brevis, left upper trapezius, right middle deltoid, right anterior deltoid, and left anterior deltoid muscles. However, the task height and wrist load factors increased muscle activation when they increased. Additionally, the wrist load factor significantly affected perceived discomfort in the shoulders, and a correlation was found between the right shoulder's rating of perceived discomfort and the mean amplitude of the right upper trapezius affected by increased load on the wrist. The mental load produced by the precision task was classified as medium, and the performance factor was the most representative, but the most significant pair was frustration-performance. In general, the intervention with the exoskeleton reduces the activation of the shoulder muscles evaluated.
Future work would be to carry out the same experiment with another task with a lower degree of precision and compare, experiment by including the task duration factor, and experiment in a natural environment with real operators. Also, it is necessary to evaluate body postures when the exoskeleton is used and the correlation between task, postures, perceived discomfort, and kind of exoskeleton.
Footnotes
Acknowledgements
The authors thanks to the Universidad Autónoma de Ciudad Juárez for the equipment and labs provided during the research. Also, authors recognize to the Universidad Tecnológica de Pereira to give support to the corresponding author during the research. Finally, to ErgoTech company for the design and manufacturing of the exoskeleton and other devices provided to complete the research.
Ethical considerations
The protocol was approved by a local bioethics committee and a informed consent was signed by the participants.
Funding
Corresponding author thanks to the Mexican Council of Science and Technology (CONACYT) for the postgraduate scholarship number 705159.
Conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.