
Abstract
Background:
The Valued Life Activities Disability Questionnaire (VLA) assesses activity-related disability based on the International Classification of Functioning, Disability and Health. This questionnaire is the first to comprehensively assess the difficulties patients with rheumatoid arthritis (RA) have in performing activities and the level of support they receive.
Objective:
The aim of this study, conducted between June 2023 and September 2023, was to translate and culturally adapt the short form of the VLA into Turkish (Tr-S-VLA) and assess its reliability and validity in patients with RA.
Methods:
Ninety-three RA patients with a median age of 60.00 (8.00) years were included. Reliability was assessed using Cronbach's alpha and intraclass correlation coefficient. Construct validity was assessed using factor analysis. Criterion validity was established by comparing the Tr-S-VLA with the Health Assessment Questionnaire (HAQ), the Rheumatoid Arthritis Disease Activity Index (RADAI-5) and the Short Form-36 (SF-36).
Results:
The Tr-S-VLA demonstrated high internal consistency (α = 0.913) and excellent test-retest reliability (r = 0.750, p < 0.05). Positive correlations were found with the HAQ (r = 0.654, p < 0.05) and the RADAI (r = 0.657, p < 0.05). Negative correlations were found with physical functioning (r = −0.685, p < 0.05), physical role function (r = −0.528, p < 0.05), social functioning (r = −0.540, p < 0.05) and the general health subscale of the SF-36 (r = −0.435, p < 0.05). These correlations indicate that the Tr-S-VLA has criterion validity.
Conclusions:
The Tr-S-VLA is a valid and reliable tool for the assessment of activity-related disability in patients with RA.
Introduction
Rheumatoid arthritis (RA) is a systemic autoimmune condition characterized by inflammation of the synovium, impacting joints and extra-articular organs. Over time, this inflammation often results in joint pain and reduced mobility, significantly affecting self-care, daily activities, and professional life. 1
Instruments used in RA research often focus on assessing activities of daily living, particularly demanding tasks, and their impact on the individual.2–6 The Health Assessment Questionnaire (HAQ) is widely used to assess people with RA. However, the HAQ primarily assesses specific physical impairments rather than broader activity difficulties and thus ignores advanced functions such as social and leisure activities. 7 In addition, the HAQ assesses an individual's ability to perform specific activities without considering aspects such as the effort, pain or fatigue required to perform the task. This narrow focus limits a comprehensive assessment of patients’ functional difficulties. Similarly, the Short Form-36 (SF-36) is another tool commonly used in RA research. 8 Although it covers broader dimensions, including physical, mental and social health components, it lacks specific aspects of the difficulties faced by people with RA, particularly those related to disease symptoms and the need for task-adaptation strategies. Both the HAQ and the SF-36 primarily assess whether people can perform certain activities but often neglect how they achieve this functionality. People with RA often need assistive devices, personal assistance or behavioral changes to increase their functional capacity.
The Valued Life Activities Disability Questionnaire (VLA) is better suited to assessing the broad range of activity limitations in RA. It is developed by Katz et al., covering activities in three categories: obligatory activities, committed activities, and discretionary activities.9,10 Unlike other instruments, the VLA evaluates not only whether activities are performed but also the support individuals require while engaging in these activities, including the usage of accommodations. This aspect represents a significant innovation as behavioral accommodations are not incorporated into any other disability assessment tool.11,12
There is a need for comprehensive assessment tools that not only evaluate the challenges of performing activities in people with RA but also consider behavioral adaptations and the use of assistive devices during these activities. Effective treatment planning relies on a thorough assessment that encompasses various functional aspects, including the behavioral changes that people with RA often make to improve their functioning. VLA is therefore an important assessment tool for RA. However, concerns about the time-consuming nature of administering the original VLA in clinical and research settings have led to the development of an abbreviated version in recent years. 13 This abbreviated version retains the broad assessment of activities while providing a more practical assessment. Therefore, the aim of this study is to translate the short form of the VLA (S-VLA) into Turkish and to assess its reliability and validity in patients with RA.
Methods
Study design, ethics and participants
This observational measurement study used a test-retest and validity design, following the guidelines outlined in the Consensus-based Standards for the Selection of Health Measurement Instruments (COSMIN) and the Guidelines for Reporting Reliability and Agreement Studies (GRRAS). 14
Ethical approval for the study was obtained from the Muğla Sıtkı Koçman University Health Sciences Ethics Committee (protocol number: 230052, decision number: 79). Data collection took place at the Department of Rheumatology, Muğla Training and Research Hospital, from June 2023 to September 2023. Diagnosis and determination of inclusion and exclusion criteria for participants were performed by a rheumatologist. Inclusion criteria included individuals aged 18–60 years, with a basic level of Turkish literacy, and diagnosed with RA. Exclusion criteria included psychiatric or neurological conditions that interfered with questionnaire completion, neurological deficits due to spinal injury, and involvement in professional sports. The identification of possible psychiatric or neurological conditions in participants was determined by clinical examination and review of the patient's past medical records.
Validation studies typically suggest an item-to-subject ratio of 5:1, 10:1, 15:1 or 30:1, with the 5:1 ratio being the most commonly used. 15 Given the 14-item structure of the S-VLA questionnaire, a minimum sample size of 70 patients was set for this study. Eligible participants gave informed consent prior to participation and underwent a 15–20 min paper-and-pencil face-to-face interview. In addition, according to the COSMIN guidelines, samples of ≥50 participants are considered adequate to address construct validity and interpretability, whereas a sample of ≥30 participants is recommended to address test-retest reliability and measurement error. 16
Translation of the short form valued life activities disability questionnaire (S-VLA)
Prior to commencing the study, the researcher obtained permission from the developer of the S-VLA. The translation of the original S-VLA into Turkish followed Beaton's guidelines for cross-cultural adaptation of self-report measures. 17 First, the English S-VLA was translated into Turkish by two translators, one a physiotherapist and the other an English teacher. The two Turkish translations were then compared to create a single version. In the second stage, the Turkish version produced was independently back-translated into English by two native English speakers who were not involved in the study and had no knowledge of the original English version. An expert committee of four translators and the researchers then compared the back-translated version with the original English version via an online meeting. This review ensured that the Turkish version was semantically and conceptually equivalent to the original S-VLA.
One item was modified during the cultural adaptation phase. Item 12 was adapted to reflect current sporting activities in Turkey. To be more in line with the sports commonly practised in Türkiye, the phrases ‘….golf, bicycling, swimming, or water aerobics’ were removed and ‘….bicycling, swimming, football, basketball, volleyball’ were added. 18 No adaptation was made to the other items. Later, the validity and reliability study of the Turkish version of the S-VLA (Tr-S-VLA) was conducted.
Investigation of the psychometric properties of the short form Turkish valued life activities disability questionnaire (Tr-S-VLA)
The reliability of the Tr-S-VLA was determined by assessing test-retest reliability and internal consistency. For test-retest reliability, 40 patients who completed the questionnaire were re-interviewed 7–14 days after the initial administration and the Tr-S-VLA was administered again.
Kaiser-Mayer-Olkin (KMO) and Bartlett's Test of Sphericity (BTS) analyses were performed to assess the appropriateness of the sample for factor analysis. Exploratory factor analysis (EFA) was then conducted to assess the construct validity of the Tr-S-VLA. The S-VLA lacks a gold standard instrument to assess its criterion validity. However, in the original study, the S-VLA showed highly positive correlations with the HAQ, SF-36 and the Rheumatoid Arthritis Disease Activity Index (RADAI-5). 13 Therefore, the HAQ, RADAI-5 and SF-36 were used to confirm the construct validity of the Tr-S-VLA. We hypothesized that the Tr-S-VLA would show a positive significant correlation with the HAQ and RADAI-5 and a negative significant correlation with the SF-36.
S-VLA
The S-VLA, which consists of 14 items, is structured with 3 mandatory activities (meeting basic needs, moving within the home, walking outside the home only), 5 specific activities (preparing meals, light housework, heavy housework, caring for family members, working in a job), and 6 optional activities (gardening or yard work, participating in social activities, spending leisure time outside the home, hobbies, physical recreation, and traveling outside the city). Regarding the scoring system, the following approach is employed: activities that pose no difficulty receive a score of 0, those with a bit of difficulty are scored as 1, items with a lot of difficulty receive a score of 2, and activities that participants are unable to perform are scored as 3 points. To calculate the Total S-VLA score, the sum of the scores for all the items is determined, and this total is then divided by the number of items marked. As a result, the final score will fall within the range of 0 to 3, where lower scores indicate a higher level of functioning and fewer difficulties in executing the specified activities. 13
RADAI-5
RADAI-5 is a patient-reported disease activity assessment tool for RA. It consists of a 5-item to evaluate overall disease activity over the past 6 months, current disease activity associated with joint tenderness and swelling, arthritis pain, and the duration of morning stiffness. Scores on the RADAI-5 can range from 0 to 10, with lower scores indicating a better status of RA. 19
SF-36
The SF-36 questionnaire, comprising 36 items across 8 dimensions, was employed in this study. These dimensions include social functioning, bodily pain, physical functioning, role limitations due to physical health problems, vitality, general health, role limitations due to emotional problems, and mental health. SF-36 scores range from 0 to 100, with higher scores indicating better health-related quality of life. For this study, the physical functioning, physical role function, social functioning, and general health subscales of SF-36 were selected as they were deemed by the investigators to possess properties associated with VLA disability and general role functioning.20–22
HAQ
The HAQ is employed to evaluate disease-specific functional status. It comprises 20 self-administered questions across 8 functional categories: dressing, arising, eating, walking, hygiene, reach, grip, and common activities. HAQ scores range from 0 to 3, with higher scores indicating a greater degree of functional impairment. 23
Statistical analysis
In this research, data analysis was executed employing IBM Statistical Package for the Social Sciences (SPSS) Statistics version 26. The normality of data distribution underwent assessment via the Kolmogorov–Smirnov test. Descriptive statistics were delineated as mean ± standard deviation for normally distributed data, while data with non-normal distribution were portrayed using the median and interquartile range (IQR).
For evaluating test-retest reliability, the intraclass correlation coefficient (ICC) was computed. The interpretation of ICC values was categorized as follows: poor (<0.40), fair (0.40–0.59), good (0.60–0.74), and excellent (0.75–1.0). The internal consistency of the Tr-S-VLA was assessed using Cronbach's alpha coefficient, with results of at least 0.80 considered indicative of high consistency, values between 0.80 and 0.70 considered moderate, and values less than 0.70 considered low. 24 Reproducibility was appraised by calculating the standard error of measurement (SEM) and minimal detectable difference (MDD) values.25,26
To gauge the sample's suitability for factor analysis, KMO and BTS analyses were performed. Construct validity was determined employing maximum likelihood extraction with specific criteria to meet, including Scree Plot inflection, Eigenvalue >1.0, and variance >10%. 27 For criterion validity, the Spearman correlation coefficient was utilized, with correlation values categorized as negligible (r = 0.00–0.30), weak (r = 0.30–0.50), moderate (r = 0.50–0.70), strong (r = 0.70–0.90), and very strong (r = 0.90–1.00). 28 The statistical significance level was set at p < 0.05.
Results
Ninety-three patients with RA, with a median age of 60.00 (8.00) years, were included in this study. It took approximately 4 min to complete the Tr-S-VLA. The demographic, clinical characteristics, and outcome measures of the study population are presented in Table 1.
Participants characteristics (n = 93).
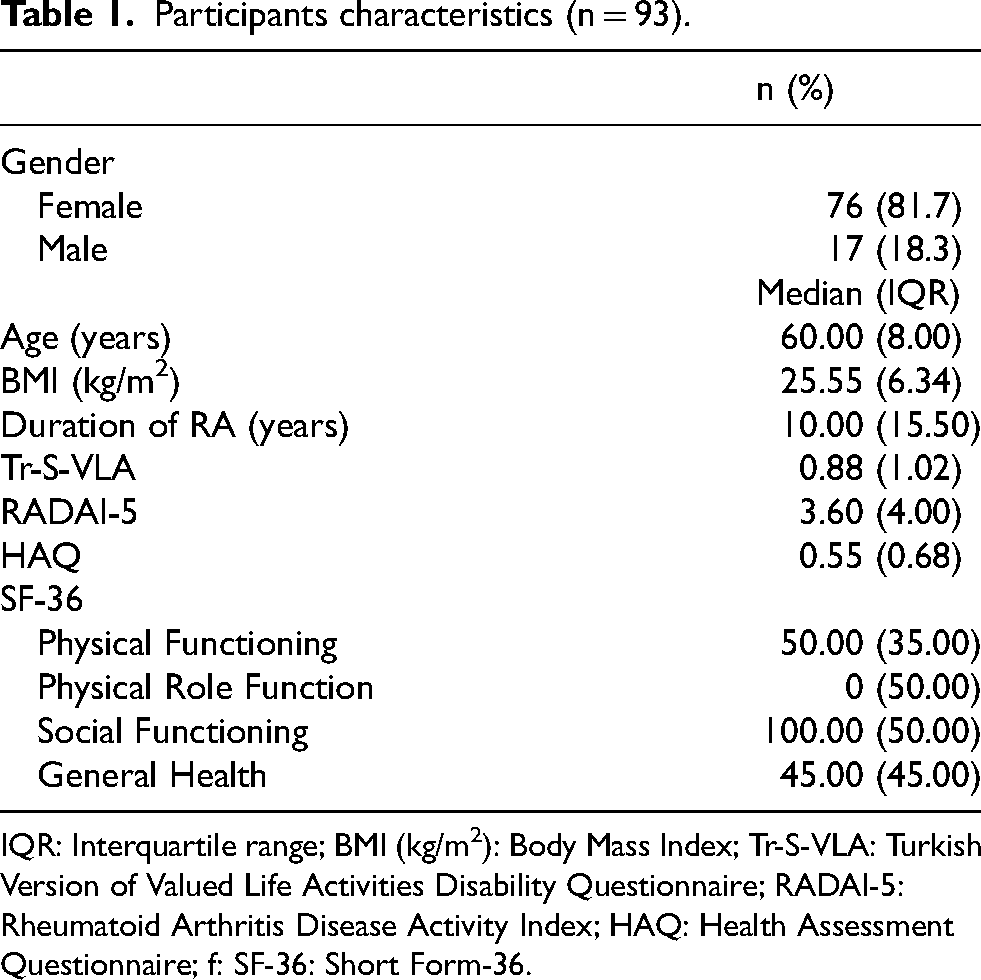
IQR: Interquartile range; BMI (kg/m2): Body Mass Index; Tr-S-VLA: Turkish Version of Valued Life Activities Disability Questionnaire; RADAI-5: Rheumatoid Arthritis Disease Activity Index; HAQ: Health Assessment Questionnaire; f: SF-36: Short Form-36.
Reliability
The internal consistency of the Tr-S-VLA was assessed using Cronbach's α to evaluate item homogeneity. The Tr-S-VLA demonstrated excellent internal consistency, with a Cronbach α of 0.913. This value falls within the 0.90 to 0.91 range, indicating robust interrelationships between the items on the questionnaire. The SEM for the Tr-S-VLA was found to be 0.072, while the MDD was calculated to be 0.199.
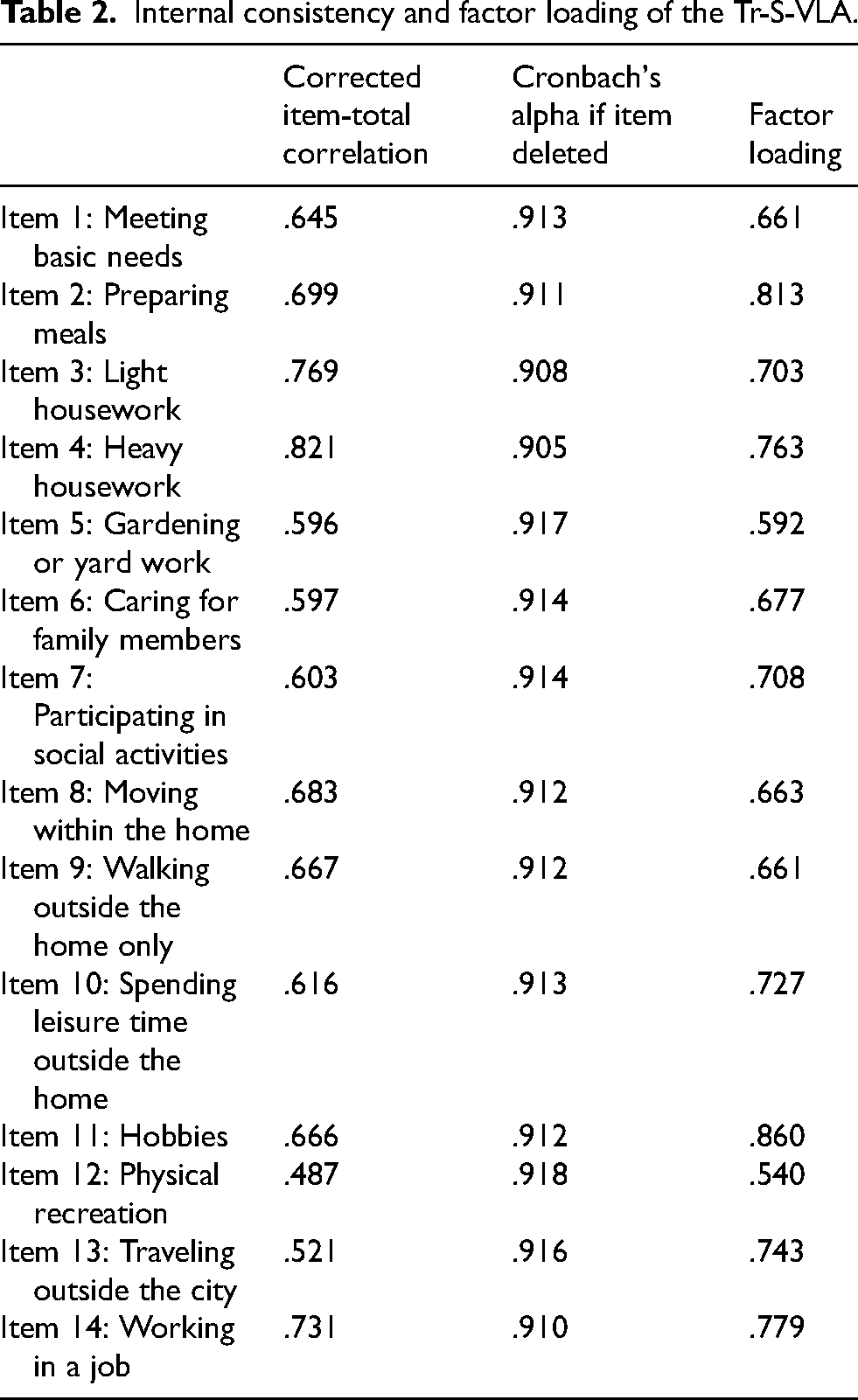
A positive and excellent significant relationship was observed between the test and retest scores of the Tr-S-VLA (r = 0.750, p < 0.05). Test-retest analysis results indicated that the ICC for each item ranged from 0.90 to 0.91 with an ICC value of 0.913 for the total score (Table 2).
Internal consistency and factor loading of the Tr-S-VLA.
Validity
Additionally, the RADAI-5, HAQ, and SF-36 questionnaires were administered to participants to assess the criterion validity of the Tr-S-VLA. The correlation between the Tr-S-VLA and the other questionnaires was evaluated using Spearman Correlation Analysis, as presented in Table 3. According to this analysis, the Tr-S-VLA exhibited a significant positive correlation of 0.657 with RADAI-5, 0.654 with HAQ, while it exhibited significant negative correlations of −0.685 with the physical functioning subscale of SF-36, −0.528 with the physical role function subscale of SF-36, −0.540 with the social functioning subscale of SF-36, and −0.435 with the general health subscale of SF-36. These results showed that the Tr-S-VLA has criterion validity.
Correlation between Tr-S-VLA and the RADAI, HAQ and subscales of SF-36.
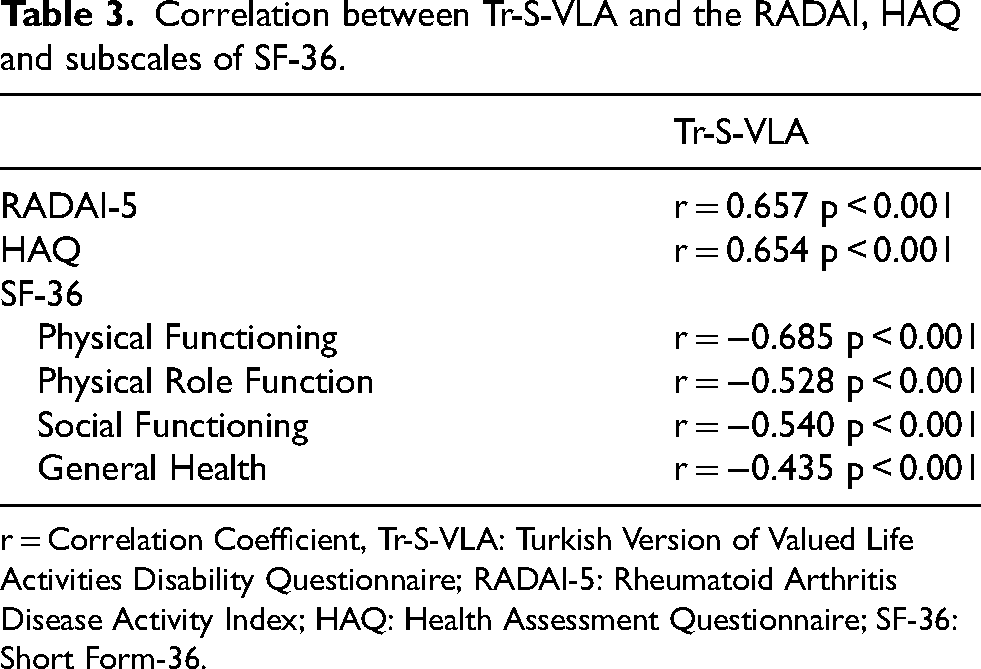
r = Correlation Coefficient, Tr-S-VLA: Turkish Version of Valued Life Activities Disability Questionnaire; RADAI-5: Rheumatoid Arthritis Disease Activity Index; HAQ: Health Assessment Questionnaire; SF-36: Short Form-36.
For the factor analysis of the Tr-S-VLA, the correlation matrix was found to be suitable based on the Kaiser-Meyer-Olkin value of 0.879 and BTS (Chi-Square 760.233, p < 0.001). The Scree Plot with Varimax rotation indicated one-factor solution, as determined by satisfying all a-priori factors, including the Scree Plot inflection point, Eigenvalue >1.0, and variance >10%. EFA revealed that the one factor explained a satisfactory percentage of the total variance (59.49%). The item loadings for the one-factor solution, as determined by the Maximum Likelihood Extraction (MLE) method. Factor loadings for all items were >0.4. Tr-S-VLA item 12 (“Participating in physical recreational activities, such as walking for exercise, playing golf, bicycling, swimming, or water aerobics”) exhibited the lowest factor loading, while S-VLA item 11 (“Working on hobbies, crafts, or creative activities, such as music, knitting, woodworking, or painting”) had the highest factor loadings. The factor loadings of the items are detailed in Table 2.
Discussion
This study represents the first cross-cultural adaptation and validation of the S-VLA. The results indicate that the Tr-S-VLA exhibits moderate internal consistency, excellent test-retest reliability, and significant correlations with other instruments. The Tr-S-VLA, which consists of 14 items, was found to have a single-factor structure, and captures a satisfactory percentage of the total variance.
Traditionally, assessments of functioning in musculoskeletal disorders such as RA have often focused on questionnaires that include predefined activities, typically centered on self-care and basic needs. Nevertheless, the S-VLA incorporates discretionary and committed activities into the assessment, aligning with the principles of the International Classification of Functioning, Disability, and Health (ICF) model. The rationale behind incorporating these activities is that as the disability levels of patients with RA increase, they tend to discontinue committed and discretionary activities. 13 Moreover, there has been a growing trend toward assessing a more comprehensive spectrum of functioning, which encompasses evaluations of various activities. 29 The S-VLA also incorporates individual preferences by permitting respondents to indicate whether an activity holds no importance or relevance to them. These stated advantages of S-VLA meet the need in this field and increase the suitability of the questionnaire for each participant.
The original S-VLA study involved 150 RA patients, with a mean age of 55.7 (SD = 14.6), and 74.0% were female. 13 In that study, the median duration of RA diagnosis was 12.7 years (IQR = 11.5). Contrarily, the Tr-S-VLA included 93 RA patients, with a median age of 60.0 years (IQR = 8.0), 81.7% were female, and the median duration of diagnosis was 10.00 years (IQR = 15.50). In particular, the literature recommends 30 participants for test-retest reliability analysis. 16 This criterion was met in the Tr-S-VLA study with 40 patients. The Tr-S-VLA exhibited moderate reliability, with a test-retest correlation coefficient of 0.750 and a Cronbach's alpha coefficient of 0.913. In comparison, the original S-VLA demonstrated excellent internal consistency, with a Cronbach's alpha coefficient of 0.950. 13 Literature suggests a Cronbach's alpha coefficient above 0.70 for good internal consistency. 30 Therefore, Tr-S-VLA shows sufficient internal consistency.
The SEM value indicates the extent of programming errors present in a survey by determining the magnitude of random error in the measurement. The MDD helps to determine whether the observed change is clinically significant and is considered a parameter indicating the reliability of the measurement. The values of 0.199 MDD and 0.072 SEM obtained in this study indicate that the Tr-S-VLA has high measurement reliability and can detect small but significant changes in patient activity level. There are no previous reports of SEM and MDD values in both the long and short versions of the S-VLA.9,13 This study is important as it is the first study in which these values were investigated. For clinicians, knowing the SEM and MDD values of a measurement tool offers an important advantage in both clinical follow-up and research by providing reliable detection of clinically significant changes.
HAQ is considered the strongest predictor of VLA disability, regardless of how it is defined. 9 In the present study, Tr-S-VLA showed a significant and moderate correlation with HAQ. This correlation is an important finding supporting the validity of Tr-S-VLA in determining disability in VLA. The original S-VLA study reported a correlation of r = 0.81 between S-VLA and HAQ in RA patients. 13 Similarly, a study in SSc patients found a correlation of r = 0.83 between VLA and HAQ. 9 The results of this study are consistent with previous studies. However, while HAQ primarily measures self-care and physical activities in the obligatory activities category, S-VLA provides significant advantages over HAQ by providing a broader assessment range, covering not only obligatory activities but also voluntary and committed activities.
RADAI-5 assesses joint swelling and tenderness, arthritis pain, duration of morning stiffness, general disease activity in the past six months, and current disease activity. 19 The correlation of Tr-S-VLA with RADAI-5 (r = 0.657) is similar to the correlation reported in the original S-VLA study (r = 0.71). 13 This correlation provides important insights into the relationship between disease activity index and activity limitation in RA. The SF-36 primarily measures the effects on quality of life by assessing a limited range of activities. Similar to the original study, the Tr-S-VLA showed negative significant correlations with subgroups of the SF-36. 13 This supports the validity of the Tr-S-VLA.
All items in the Tr-S-VLA had factor loadings above 0.30 and explained 59.49% of the total variance. This indicates that all items had sufficient factor loadings. 31 The TR-S-VLA showed a single-factor structure like the original S-VLA. The single-factor nature of the questionnaire suggests that all items of the scale assess a common underlying construct, namely the concept of ‘valued life activities’. Therefore, it can be said that the scale was designed to assess a single concept or trait.
Strength and limitation
This study has several important strengths. Firstly, the Tr-S-VLA can be used to assess a wide range of activities, including obligatory, committed, and discretionary tasks. The inclusion of committed and discretionary activities is particularly noteworthy, as these are often overlooked in most disability assessment tools, despite their apparent importance in the early stages of disability. Secondly, the compatibility of the Tr-S-VLA with the ICF functional model suggests that it may offer significant advantages in clinical practice.
However, the study has some limitations. Firstly, the responsiveness of the Tr-S-VLA to clinical change was not assessed. Additionally, the lack of subgroup analyses based on demographic and clinical characteristics (e.g., gender, disease duration) makes it difficult to assess whether the tool is equally valid across different patient profiles. Furthermore, the relatively small sample size may not be large enough to eliminate potential bias resulting from exclusion criteria. Future research should include studies with larger sample sizes and from different disease groups, as well as assess the clinical sensitivity of the questionnaire.
Conclusion
The Tr-S-VLA demonstrates its validity and reliability in assessing activity-related disability in RA patients by demonstrating strong psychometric properties such as internal consistency, test-retest reliability, and construct and criterion validity. Thanks to its comprehensive structure, it assesses not only whether patients can perform their activities, but also the level of support needed to participate in these activities, and particularly the use of accommodations, making it practical and detailed for clinical use.
For rheumatologists and physiotherapists, the Tr-S-VLA offers a structured approach that allows a comprehensive analysis of activity limitations, facilitates the creation of personalized rehabilitation programmes and has the potential to comprehensively evaluate patient outcomes. In addition, its strong psychometric properties can increase the accuracy of disability assessments, particularly in culturally diverse populations. The integration of the Tr-S-VLA into clinical applications can make a significant contribution by allowing clinicians to monitor treatment progress and provide objective data for clinical decision making.
Footnotes
Ethical considerations
Ethical approval for the study was obtained from the Mugla Sıtkı Kocman University Health Sciences Ethics Committee (protocol number: 230052, decision number: 79).
Informed consent
Participants gave informed consent prior to participation.
Author contributions/CRediT
ACP, MK: Designing this study, writing initial draft and revision, revising language. BB, KB: Content, supervision. ACP, MK: making figure and table. ACP, MK: Rechecking the manuscript and putting forward suggestions for amendment. EFT: Data collection. All authors contributed to the article and approved the submitted version.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.