
Abstract
Background
Physiotherapists play a critical role in managing musculoskeletal health, yet they remain highly vulnerable to work-related musculoskeletal disorders (WMSDs) due to the physical demands of their profession.
Objective
This study explores the awareness of strategies used in preventing WMSDs and their effectiveness, motivation, and barriers to preventing WMSDs among physiotherapists.
Methods
This qualitative study was administered among physiotherapists in Malaysia, where semi-structured interviews with a modified interview guide were used through an online platform. The interview was performed as an open conversation and follow-up questions to ensure the questions were answered in-depth.
Results
Participants were aware of a range of strategies used in preventing WMSDs and acknowledged the effectiveness of these strategies. The strategies are proper body mechanics (61.5%), exercise (23.1%), proper work ergonomics (15.4%), adequate staffing (15.4%), use of equipment (15.4%), and proper warm-up (7.7%). Clinics or hospitals well equipped with devices and equipment (53.8%), encouraging proper body mechanics and posture (46.2%), and education (30.8%) were the most common themes that motivated participants in preventive WMSDs. Several barriers to the engagement of these preventive strategies were also acknowledged, namely the availability of equipment, heavy workload, and inadequate staffing.
Conclusions
Malaysian physiotherapists recognize the importance of proper body mechanics, physical exercise, and education in preventing WMSDs. While they actively adopt strategies such as utilizing tools, promoting correct posture, and implementing preventive measures, challenges like equipment shortages, excessive workloads, and staffing issues remain significant barriers. Addressing such barriers is essential for effective and sustainable prevention strategies.
Keywords
Introduction
Musculoskeletal (MS) pain can be defined as the consequence of repetitive exertion, moderate use of the musculoskeletal system, and work-related musculoskeletal disorders (WMSDs).1,2 MS disorders are the second leading cause of disability worldwide, affecting up to one-third of the world's population. 3 Additionally, up to 50% of people with multiple morbidities have MS disorders, commonly linked to persistent pain and depression. 4 Musculoskeletal-related pain and occupational injuries are significantly associated with the work environment or work-related aetiology, which is also referred to as work-related musculoskeletal diseases. 5 WMSDs are the primary source of lost workdays, higher expenses, and occupational diseases worldwide, including in Malaysia. Based on the statistics reported by the Social Security Organization (SOCSO) Annual Report in 2018, WMSDs accounted for 57.75% of occupational disease cases recorded in Malaysia, the highest compared to other occupational disease cases such as occupational respiratory and skin disease. 6
A health professional is a highly skilled worker who works in the health or health-related fields, such as nurses, dentists, surgeons, and physiotherapists. WMSDs are common among healthcare professionals and hospital practitioners. 7 WMSDs lead to lost work time, absenteeism, job transfer, financial burden, increased work restrictions, decreased productivity, and even disability which may require long-term medical care.5,8–14 Among all the healthcare professions, nurses (55.5%) had the highest incidence of WMSDs, followed by physiotherapists (55%) and dentists (53.5%), whereas laboratory technicians (38.7%) and physicians (38%) had the lowest. 14
WMSDs are relatively common among physiotherapists, despite their substantial knowledge of body mechanics and injury prevention. Surveys undertaken in Croatia revealed WMSD prevalence rates of 63.9%. 15 Abu-Taleb & Rehan Youssef (2021) discovered that 99.5% of physical therapists suffered from WMSDs during their professional lives in Egypt. 16 In India, the figure was 92.70%. 17 The prevalence of WMSDs among physiotherapists is considered high. A recent study on ‘global prevalence of musculoskeletal disorders among physiotherapists’ reported that the prevalence rate of WMSDs among physiotherapists worldwide exceeded 80%. They further reported that lower back pain, thumb, neck and shoulder were most at risk for WMSD. 18 In Malaysia, the highest prevalence of WMSD was at wrist-hands (65.9%), neck (52.5%), lower back (41.3%), and the least, elbow (6.2%). 19 The majority of physiotherapists experienced symptoms in more than one body area. 7 Yet, physiotherapists’ self-engagement in preventing WMSDs has been the least explored.
The common occupation-related disorders among physiotherapists include low back pain and hand-related injury. These were associated with repetitive manual handling techniques and delayed in treating the pain or injury.14,20 Repetitive movement causing WMSDs is also common and reported in many other occupations as well.21–23 Although WMSD is a well-known area and much research is done to curb the issue, the risk is still high among physiotherapists. Particularly in Malaysia, there is a lack of information regarding WMSD among physiotherapists. Many factors impact physiotherapist work such as individuality, ergonomically, organization, psychosocially, and it is very important to pick out which of these factors are related to WMSD. Understanding these harmful elements and the use of effective preventative measures can significantly improve physiotherapist working performance, quality of work, and consequently, the satisfaction of patients.
There is a range of research on the risk factors for WMSDs among physiotherapists, but we did not come across any qualitative research updates on effective preventative strategies to address this problem among physiotherapists in the last 10 years. Most recent studies tend to be quantitative, focusing on prevalence rates, ergonomic assessments, or interventions like exercise programs and posture training. Therefore, exploring the viewpoints of individuals with specialized knowledge in the area may aid in identifying the challenges to WMSD prevention and novel strategies worthy of future research or clinical implementation. Thus, this study explores the awareness of strategies used in preventing WMSDs and their effectiveness, motivation, and barriers to preventing WMSDs among physiotherapists. This study is expected to contribute to the body of knowledge in terms of awareness, effectiveness, motivation, and barriers to preventing WMSDs among physiotherapists and it could become referral data to plan and implement further adjustment and improvement as a preventive intervention, especially in terms of workstation design and, individual and team adjustments to prevent WMSD.
Methods
Participants
This was cross-sectional qualitative research conducted among physiotherapists in Malaysia, stratified into less than 1 year, more than 1 year, and more than 5 years of experience or practice. A total of 13 physiotherapists participated in this study. A systemic analysis on ‘characterizing and justifying sample size sufficiency in interview-based’ studies justified that a minimum sample size of at least 12 is sufficient to achieve data saturation in qualitative studies. 24 Hence, a sample size of 13 was deemed adequate for the qualitative analysis of this study. In addition, data saturation was reached when no new themes, patterns, or insights emerged from additional interviews, indicating that further data collection would not contribute new information. This was ensured through continuous data analysis, where responses were reviewed iteratively, and recruitment was halted once redundancy was observed. This study was carried out by conducting individual semi-structured interviews online. The inclusion criteria included being qualified Malaysian physiotherapists, having a minimum of 3 months of clinical practice experience in a hospital setting and being physiotherapists from any specialization.
Procedure
Purposive sampling was conducted to recruit participants where the head of the physiotherapy department from various clinical specializations was contacted and asked to help identify suitable potential participants. An information sheet describing the study along with a consent form was sent to these staff members, and interested individuals indicated their willingness to participate via email.
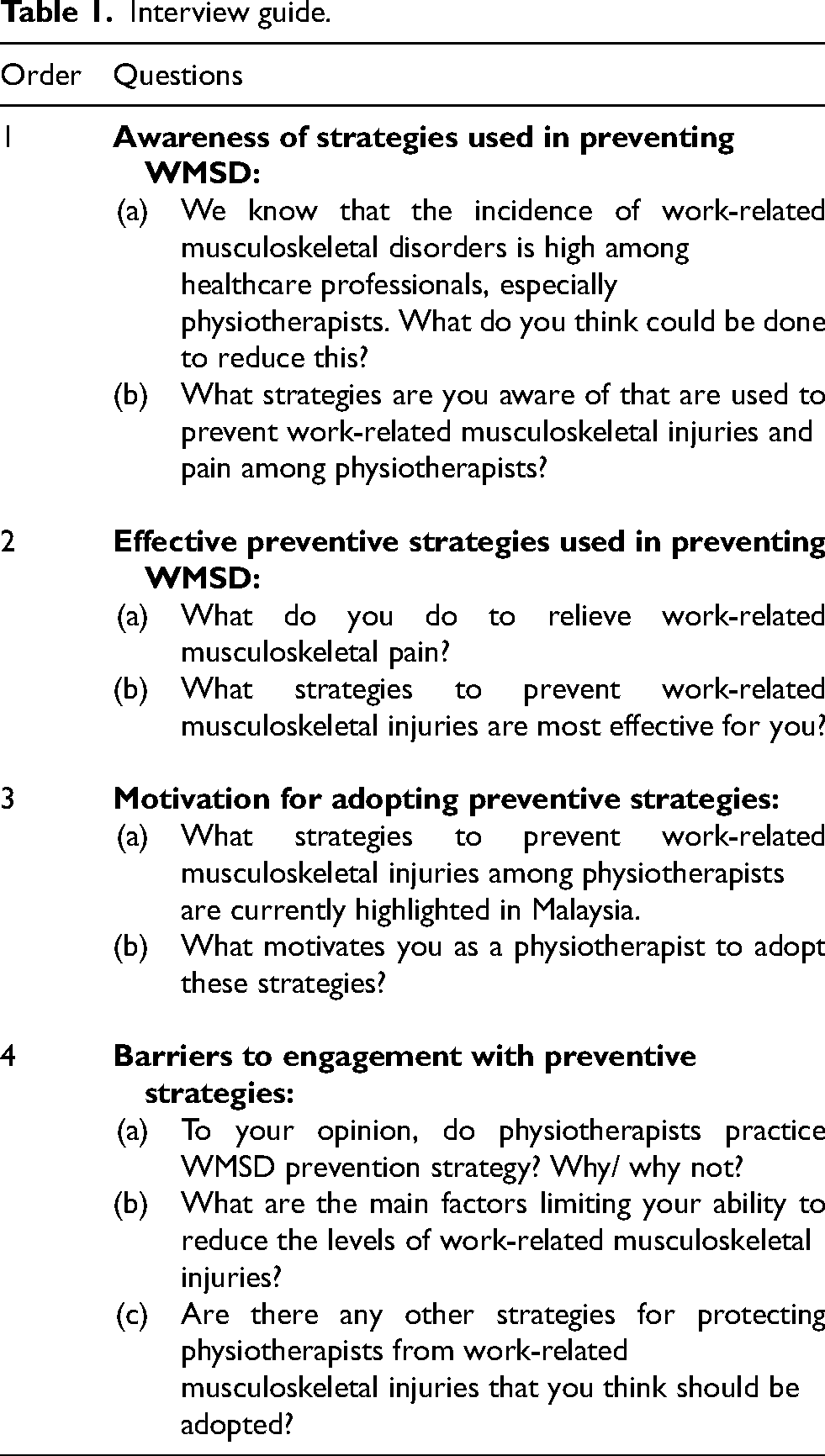
The semi-structured interviews were conducted on a one-to-one basis, ranging from 30–60 min in duration, and were audio-recorded. The sociodemographics were collected from the participants, including age, gender, their current role, and a brief description of their background in their clinical fields such as current clinical setting, working place, current fields of practice, years of practice, and hours worked per week. A modified interview guide was adapted from Oakman et al. (2019) and Richardson et al. (2019) to assess the strategies used in preventing WMSDs among physiotherapists in terms of awareness, effectiveness, motivation, and barriers (Table 1).25,26 The one-to-one interview was an open conversation with follow-up questions to ensure the research question was answered in-depth. At the end of the session, the researcher summarized the findings to confirm with participants regarding the provided information.
Interview guide.
Data analysis
Statistical Products and Service Solution (SPSS) version 25.0 was used to analyse the demographic characteristics of the participants using descriptive analysis. Next, the thematic analysis was performed to analyse the data according to the six steps specified by Braun & Clarke (2017): familiarization with the data, generating initial coding, searching for themes, reviewing themes, defining and naming themes, and writing up the manuscript. 27 To begin, recordings from interviews were transcribed to conduct a thematic analysis. The transcripts were coded throughout the data set independently by two researchers. All the codes were then compared, discussed and modified during this process. While coding words and sentences that conveyed similar meanings, the context and the primary function of the content were considered as it may carry more than one meaning. Codes were modified to avoid semantic duplication and limit ambiguity. When all of the data had been coded and compiled, the various codes were sorted into potential themes, and all of the relevant coded data extracts were compiled within the identified themes. These themes were then reviewed and refined in conjunction with a set of candidate themes. This was followed by defining and refining the themes for the data analysis. In this analysis, no software was used. Finally, thematic analysis was outlined.
During the thematic analysis, the coding process involved multiple researchers to ensure a comprehensive and unbiased interpretation of the data. Disagreements between researchers regarding the coding of data were resolved through a systematic approach. Initially, each researcher independently reviewed and coded the data, identifying key themes and patterns. When discrepancies arose, they were discussed in team meetings, where researchers presented their perspectives and rationale for their coding decisions. To further enhance the reliability of the analysis, a consensus approach was employed. This involved re-examining the data and collaboratively refining the codes until all researchers reached an agreement. In cases where consensus could not be achieved, an external expert in qualitative research was consulted to provide an objective opinion and help mediate the disagreement. This rigorous process ensured that the final themes and codes were robust and accurately reflected the data, thereby enhancing the credibility and trustworthiness of the analysis, thus, ensuring that it is reliable and consistence.
Results
Demographic details
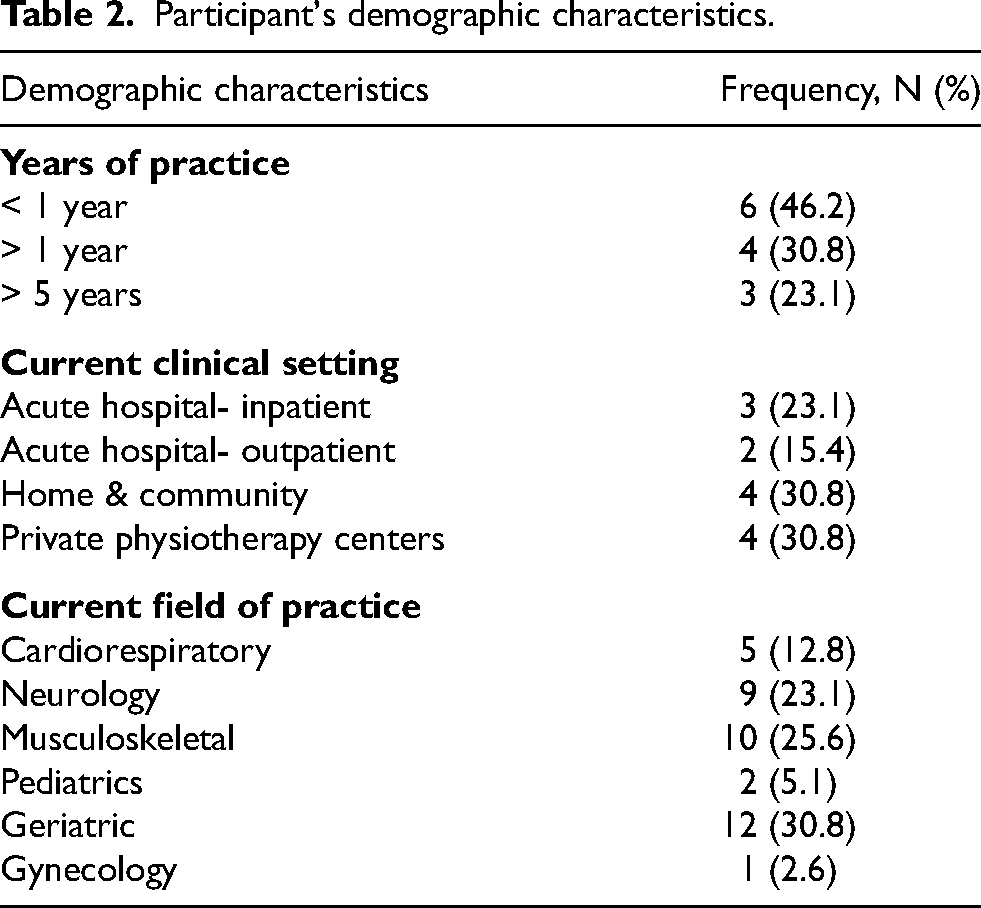
A total of 13 physiotherapists were involved in this study with 12 females and 1 male. Our participants were aged 30 to 39 years. The participants involved had a mean (standard deviation) hours worked per week of 42.38 (± 4.31). All of them had experienced WMSD symptoms and worked in the west of Malaysia. The commonly affected areas in musculoskeletal physiotherapists are the lower back, neck and thumb, as they have to perform more manual therapy repetitively and maintain static posture for a longer duration. The result in Table 2 illustrates the details of the participants’ demographics. The summary of the themes and sub-themes are as depicted in Table 3.
Participant's demographic characteristics.
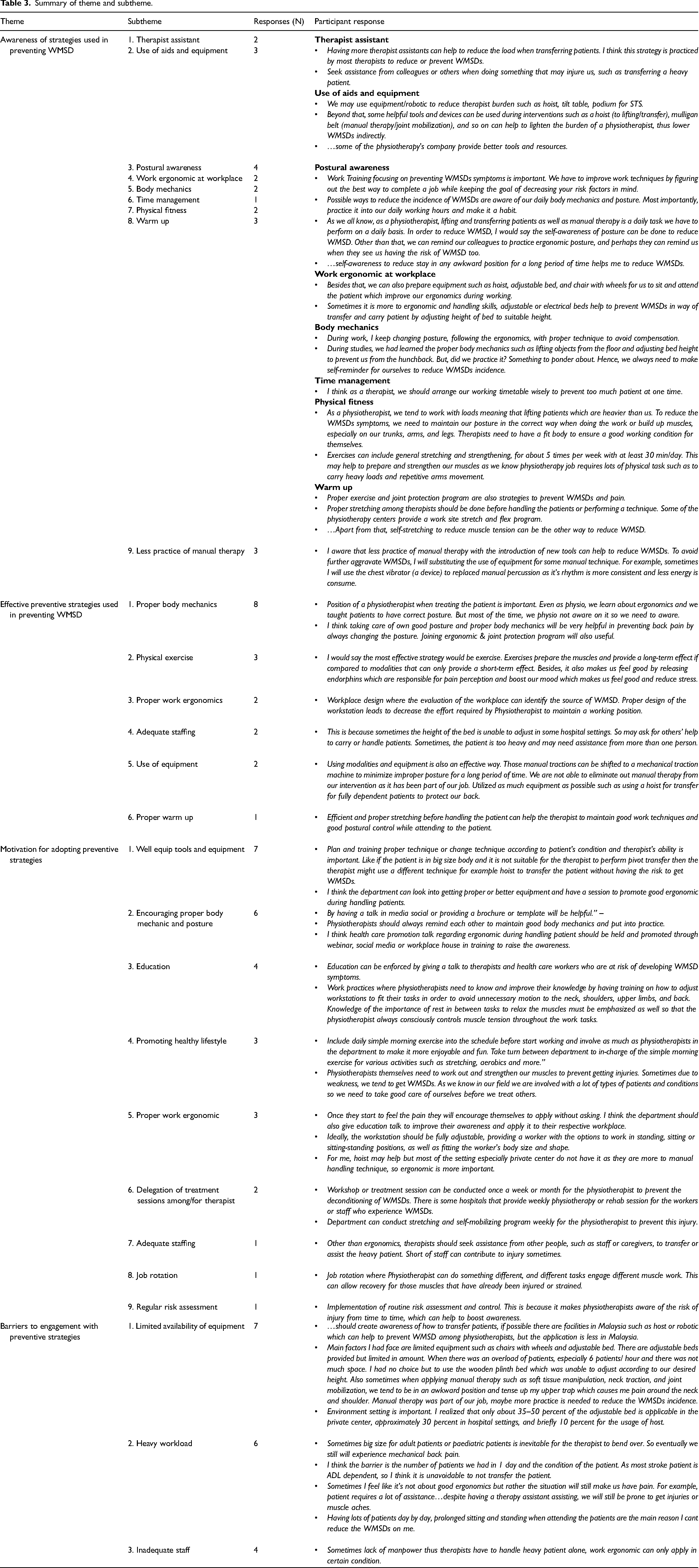
Summary of theme and subtheme.
Awareness of strategies used in preventing WMSD
Participants were aware of several strategies to prevent WMSDs. Nine (9) themes emerged from the interview data.
Therapist assistant
Several participants were aware that the aid of a therapist assistant rather than lifting alone is a safer and self-protective strategy for physiotherapists to reduce their physical demands.
Use of aids and equipment
Participants described the usage of aids and equipment as a strategy to prevent WMSDs among physiotherapists by reducing their burden during transferring or lifting clients. The aids and equipment include height-adjustable beds, hoists, lifting belts and a tilt table. However, one participant felt the equipment was not readily available in some physiotherapy centers or hospitals.
Postural awareness
The majority of the participants are aware that postural awareness and implementing them during physiotherapy sessions can prevent WMSDs. They expressed that being aware of their posture, preventing sustained awkward postures, reminding co-workers to practice proper body ergonomics, and incorporating proper postures into daily working hours were used to avoid WMSDs among physiotherapists.
Ergonomic at the workplace
Participants believed that work ergonomics is associated with WMSDs where proper work ergonomics, such as height-adjustable beds, chairs with wheels, and hoists may improve their ergonomics, thus helping with the prevention of WMSDs.
Body mechanics
Furthermore, some of the participants were aware of proper body mechanics during treatment delivery such as preventing improper posture. However, participants believe that most physiotherapists do not practice proper body mechanics during work time despite knowing how to prevent injury when transferring clients.
Time management
Participants also felt that time management could help prevent WMSDs by avoiding handling many clients simultaneously due to time constraints.
Physical fitness
A few participants thought improved physical fitness by doing exercises and self-awareness about body mechanics and posture helps prevent WMSDs.
Warm-up
Moreover, participants also expressed that proper warm-up and stretching exercises before performing manual techniques could help minimize the risk of injury.
Limiting manual therapy use
Participants explained that limiting the use of manual therapy (e.g., shorter durations, intermittent breaks) or substituting with other effective therapy methods could be a way of protecting therapists from WMSDs.
Effective preventive strategies used in preventing WMSD
Six (6) primary themes emerged from the interview data and are summarized in Figure 1.
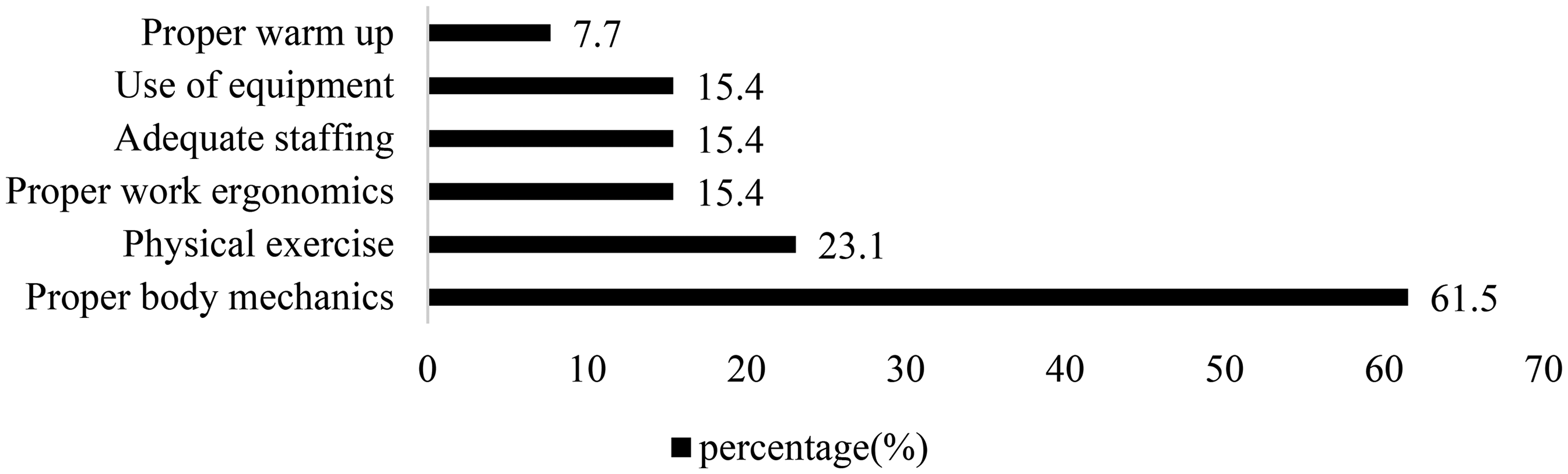
Summary of effective strategies to prevent WMSDs.
Proper body mechanics
Most participants (61.5%) believed that proper body mechanics and posture while handling clients are the most effective strategies to prevent WMSDs. They relayed that WMSD symptoms especially back pain, can be prevented by maintaining a good posture and proper body mechanics during manual handling.
Exercise
Exercise or participation in physical activity is the second most popular preventive strategy (23.1%). Participants alleged that physical exercise can help prevent WMSDs in the long run.
Proper work ergonomics
Proper work ergonomics, adequate staffing, and use of equipment have the same percentage of responses
Adequate staffing
Furthermore, extra assistance from other colleagues or staff will aid in the reduction of WMSDs. This helps in reducing clients to therapist ratio.
Use of equipment
Participants also agree that physiotherapists need to have the equipment to assist in handling clients such as a portable hoist which helps prevent WMSDs.
Proper warm-ups
Adequate body warm-ups before handling clients is the least supported strategy (7.7%) to prevent WMSDs. Participants deliberated that proper stretching before handling the clients is beneficial in taking care of their posture and preparing them for work.
Motivation for adopting preventive strategies
Some strategies are currently highlighted in Malaysia and motivate physiotherapists to prevent the onset of WMSD. The interview sought to explore the key actions that motivate participants to adopt preventive strategies from their viewpoints and is summarized in Figure 2.
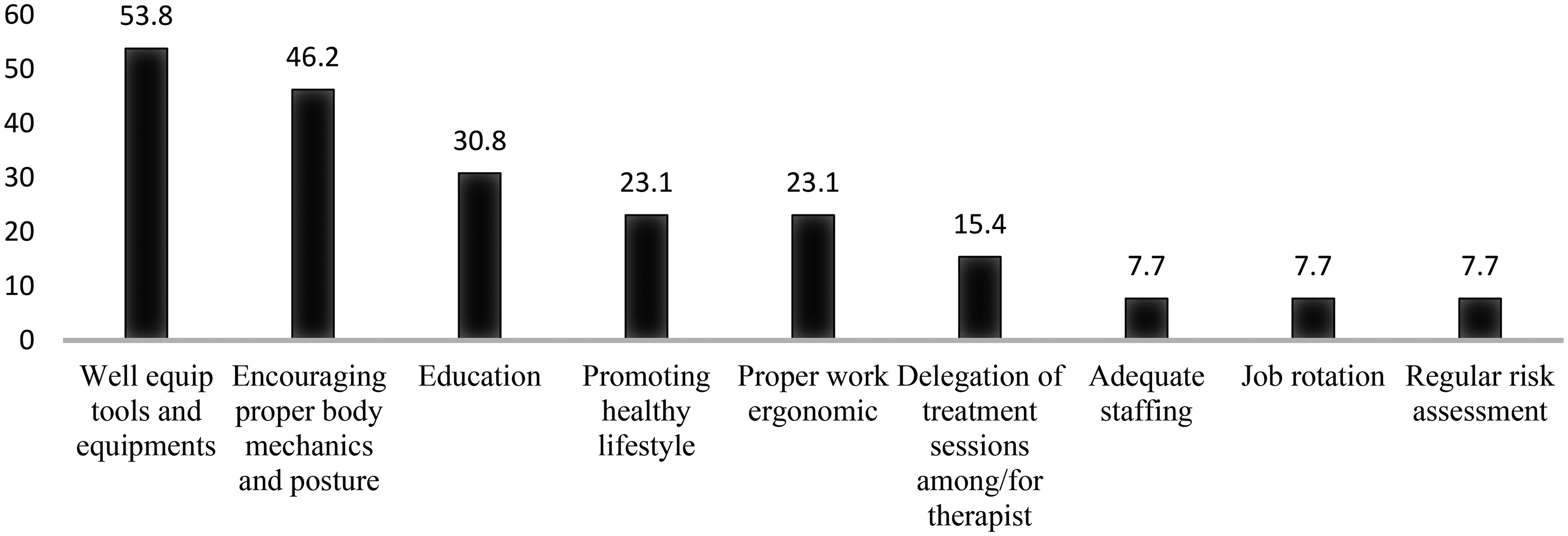
Summary of motivation for adopting preventive strategies among participants.
Tools and equipment
Most of the participants (53.8%) were aware that the introduction of devices should be adopted to prevent WMSDs among physiotherapists. They emphasized that therapists need to have assistive devices or equipment to assist them in handling and transferring clients such as a portable hoist, gliding board, lifting belt, or machines. This will keep them motivated to work safely and to prevent WMSD.
Encouraging proper body mechanics and posture
Aside from the introduction of devices, many participants (46.2%) opted for and practiced good body mechanics and posture when attending to clients as one of the WMSD prevention strategies. They mentioned the importance of proper technique when handling clients by maintaining good posture, especially during transfer clients, lifting, or performing sports massage. Proper body mechanics and posture should be motivated among therapists as it helps in preventing WMSD.
Education
Furthermore, education was the third most frequently recommended strategy (30.8%), which included descriptions of the manual handling training provided to physiotherapists and risk assessment education. Participants stated that the training program with basic knowledge of reducing the risk of WMSD symptoms, the introduction of devices or equipment, and proper practice in attending the clients should be offered to prevent WMSDs.
Promoting healthy lifestyle
A few participants (23.1%) explained that regular exercise programs should be encouraged and motivated in preventing WMSDs. Exercises that may include general stretching and strengthening can be performed in between sessions and rest time.
Proper work ergonomics
However, only about a quarter of the physiotherapists (23.1%) show their motivation for the promotion or introduction of work ergonomics in their workplace to prevent WMSDs.
Delegation of treatment sessions among/for therapist
Few participants (15.4%) proposed an equitable delegation of treatment sessions among therapists to prevent the deterioration of the WMSDs and create awareness.
Adequate staffing
Only one participant (7.7%) voiced that adequate staffing can motivate a therapist to achieve the prevention of WMSDs. This was thought to reduce the burden or load of the physiotherapist especially if someone needs to be transferred or lifted.
Job rotation
Next, the participants (7.7%) proposed job rotation as a motivation to prevent WMSD. They stated that physiotherapists can exchange workstations with other co-workers or change positions, which will allow for the engagement of different muscles and the healing of injured muscles.
Regular risk assessment
Lastly, only 7.7% of participants believed that ongoing risk assessment should be encouraged among physiotherapists in a healthcare setting to help reduce risks and thus prevent WMSDs.
Barriers to engagement with preventive strategies
The interview explored the participants’ opinions regarding the barriers to engagement with preventive strategies.
Limited availability of equipment
Participants mentioned that the main factor limiting their ability to reduce current levels of work-related musculoskeletal injuries was the unavailability of equipment. With the lack of equipment, manual handling techniques in clinical practice become more difficult as it requires more hands-on skills with clients. These include limitations of proper equipment in hospital settings such as adjustable beds or geriatric chairs with wheels. Participants also hope that the usage of robotic facilities such as a hoist or other assisting devices may be implemented in the future as ergonomics plays a vital role in hospitals in Malaysia.
Heavy workload
Despite the availability of the equipment, participants also experienced a high demand for work tasks which was one of the barriers to using preventive strategies. Participants explained that they need to handle many clients requiring transfers when there is a high workload and insufficient human resources. The imbalance of physiotherapists to client's ratio can be one of the unavoidable risk factors for WMSDs.
Inadequate staff
Inadequate staffing was also considered a barrier to an effective preventive strategy. This can place pressure on physiotherapists while handling clients, especially when the clients are heavy or have many wires attached such as clients in intensive care units. Therapists may also be too focused on meeting their workload in the working time frame and hence ignoring WMSD prevention.
Discussion
In this study, the awareness of strategies used in preventing WMSDs and their effectiveness, motivation, and barriers to preventing WMSDs among physiotherapists were explored. The study results showed that participants had a high level of awareness and recognized the importance of strategies to prevent WMSDs. Several barriers to the prevention of WMSDs were identified namely the lack of availability of equipment, heavy workload, and inadequate staffing. To our knowledge, this is the first qualitative study to explore the preventive strategies for WMSDs among physiotherapists in Malaysia.
This study demonstrated that physiotherapists are aware of the prevention of WMSDs. A survey by Major & Vézina (2015) highlighted that increasing workers’ awareness of the various strategies available is an essential tool in preventing WMSDs. 28 The physiotherapists in this study also affirmed that most therapists practice these strategies to reduce the risks of developing WMSDs. This is expected as physiotherapists are trained healthcare professionals in preventing and managing WMSDs. However, it should be noted that physiotherapists are in the workforce group that could be at high risk of WMSDs due to the nature of their job which involves repetitive tasks, application of high force and sustained prolonged postures. For instance, work tasks involving client mobilization with repetitive movements, such as lifting, transferring, and positioning clients, are frequently performed manually, necessitating an increased physical applied force that might occasionally surpass the physical capabilities of the healthcare professional. 29 It is also consistent with the finding of another study where the physiotherapists reported that conducting repetitive manual manipulation techniques for longer periods and supporting clients during gait activities were two key risk factors in their job scope that may lead to WMSDs.14,20
In the present study, physiotherapists are aware of and claim that six strategies effectively prevent WMSD. This consists of proper body mechanics (61.5%), exercise (23.1%), followed by proper work ergonomics (15.4%), adequate staffing (15.4%), and use of equipment (15.4%). Warm-ups (7.7%) were the least supported strategy in the WMSDs among physiotherapists. There are studies done among nurses that aimed to look at the knowledge and practice of body mechanics techniques. It was reported that nurses have good knowledge regarding body mechanics but fail to practice it and some even do not use body mechanics correctly with reason due to their work nature such as too many clients to handle at once.30,31 However, no studies on the knowledge and practice of body mechanics techniques among physiotherapists have been reported.
It is also important to note that body mechanics differs from ergonomics. Body mechanics means a combination of posture, balance and motion, all of which influence coordinated movement and stress placed on the body. 30 However, ergonomics is the scientific discipline concerned with the understanding of interactions among humans and other elements of a system. 32 These two play an important role in WMSD prevention among physiotherapists. Proper ergonomics prevents any adverse health issues by eliminating workplace stress, which includes dealing with tools and procedures, mainly client handling techniques that are safe and effective. 33 It is noted that ergonomic interventions can effectively prevent occupational trauma among physiotherapists, 34 yet, only 15.4% of participants are aware of its effectiveness. Thus, imparting ergonomic education to all physiotherapists is essential. Ergonomic training and ergonomic risk prevention courses should also be periodically carried out among physiotherapists.
In the aspects of motivation, tools and equipment, encouraging proper body mechanics and posture, and education were the common aspects that motivated participants to apply the preventive strategies in curbing WMSDs. Other recommendations include proper work ergonomics, delegation of treatment sessions among/for therapists, adequate staffing, job rotation, and regular risk assessment. Research by Svendsen et al. (2020) highlighted that the most common solutions used to handle and prevent WMSDs among occupational health and safety (OHS) professionals in Denmark include ‘teaching and education’, and ‘risk assessment’, followed by ‘technical assistive devices and protective equipment’ and ‘work postures and working techniques’. 35 Highlighting education, the Ergonomic Training Program was reported to be effective in improving the knowledge, self-efficacy and practice scores on preventing work-related low back pain among staff nurses. 36 Thus, education plays a crucial role in addressing WMSDs among physiotherapists. Courses focusing on WMSD preventive measures and strategies should be a compulsory part of both undergraduate study programs and lifelong learning schemes for physiotherapy professionals. Such an approach may help overcome the “this happens to other people” attitude and make education on preventive measures more popular and efficient. Additionally, increasing physiotherapists’ awareness of their risk of WMSDs and shifting the culture within health services to facilitate the use of preventative strategies are at significant needs in addressing this issue.
It should also be noted that education on its own is not enough to prevent WMSDs. Past studies have noted that physiotherapists may still face WMSDs due to the long-term, cumulative effects of repeated high-risk client-handling tasks. 37 Physiotherapists are exposed to WMSDs due to their job nature involving client care that includes transferring and lifting clients besides performing therapy. All these activities require high levels of strength, worst still when done in hazardous postures. Awkward working postures are not only reported among physiotherapists but it is also seen among dental professionals as a risk factor for WMSDs. 23 In addition, feeling responsible for the patient is another factor that can contribute to the development of WMSDs among physiotherapists. A strong sense of duty towards their patients led them to continue with patient intervention even though they knew it was putting their health at risk. This perceived moral obligation to prioritize the patient's well-being over their own can lead to poor time management and neglect of preventative strategies. Physiotherapists need to prioritize their health and well-being to provide the best care for their patients in the long term.
Provision of equipment such as sit-to-stand assist devices, lifting equipment (free-standing and ceiling mounted) and height-adjustable beds may also motivate physiotherapists to prevent WMSDs. One such effort was reported in a previous study where “zero” or minimal lifting or transfer of clients has been advocated among nurses to reduce low back pain. 38 A study by Kim et al. (2013) reported a reduction in the “worst pain” rating among physiotherapists during therapy sessions after including ergonomic interventions. 39 Thus, proper work ergonomics, along with well-equipped tools and equipment, may motivate physiotherapists to prevent WMSDs.
Other than the above, job rotations, avoiding repetitive actions and avoiding overloading on any particular anatomical area may be encouraged among physiotherapists. For example, physiotherapists may arrange appointments alternatively between more and less physically demanding clients and take breaks or recovery time between clients. Arrangements such as adjustments to work schedules were also reported as an encouragement for workers with chronic pain to return to work. 40 Such initiatives may motivate them to perform better without needing to stress both mentally and physically. In addition, stretching and strengthening exercises should be implemented at regular intervals to prevent muscle strain and soreness, as well as prevent WMSDs. 41
While several strategies are available, numerous barriers make it difficult for physiotherapists to implement them in clinical settings. It is crucial to address those barriers when designing preventive measures to increase efficiency. This study discovered three barriers to participants’ ability to reduce current levels of work-related musculoskeletal injuries. These barriers include limited availability of equipment, heavy workload, and inadequate staff. Barriers to engaging with WMSD prevention in healthcare settings were consistently identified, including age, knowledge, availability of equipment, personal and contextual factors, staffing, and time pressures. 26 The viewpoint of limited equipment availability and insufficient staff numbers is supported by the findings obtained from previous studies.25,42 This may put more weight or load on themselves during handling clients and can eventually lead to improper posture and strain of muscle as they are forced to hold the client's weight. In addition, challenges to more successful prevention implementation have been identified as a lack of awareness of the importance of addressing the risk of work-related physical and psychosocial hazards, as well as the inadequacies of established ergonomic procedures to manage such relevant hazards within the context of WMSDs risk management. 43
Other than those barriers, interpersonal, social, organizational, and environmental factors might directly or indirectly affect the implementation of preventive strategies by physiotherapists. For instance, time constraints, workload, limited mechanical equipment, understaffing, and urgent client requirements were the most notably perceived impediments to the use of assistive devices in safe client handling and mobility, which can contribute to WMSDs among healthcare professionals especially physiotherapists. 37 This is in line with the findings of a scoping review44,45 which concluded that 11 barriers and 3 facilitators were encountered during the implementation of strategies to prevent WMSDs using thematic analysis. As a result, Yazdani & Wells (2018) suggest that overcoming these barriers necessitates the expansion of the conventional OHS risk management paradigm, developing new risk management devices, and integrating WMSD prevention into a general management system approach. 45 However, there was a paucity of research outlining how the WMSD risk assessment and prevention might be integrated into management systems. 46 This may lead to difficulties in preventing WMSDs at an organizational level as the lack of information could isolate WMSDs prevention. Hence, further study is needed to integrate WMSD prevention into management systems and assess the strategy's effectiveness.
A limitation of this study is that participants’ perspectives cannot be generalized to reflect the viewpoints of all physiotherapists as the study was limited to only West Peninsular Malaysia. In addition, most of the physiotherapists who participated were females. However, note that two-thirds of the Malaysian physiotherapy workforce are females. Although we recruited physiotherapists from different specializations, some of them were practising in more than 2 areas at the time of the interview. Thus, we are incapable of discussing based on their specialization. Also, we included all participants with a minimum of 3 months of clinical practice experience and did not look further at the ‘senior junior’ effect on WMSDs. Hence, future studies on a broader perspective where different physiotherapists from different genders, specialization and work experiences need to be explored, with a bigger sample size. Another limitation is while a pilot study was not conducted for this specific semi-structured guide, it's important to note that the questionnaire was adapted from a validated past study. To acknowledge this as a limitation, we highlight that the guide may benefit from further validation through pilot testing in future research. This would help refine the questions and potentially enhance the reliability and validity of the responses.
Conclusion
The findings of this study highlight that Malaysian physiotherapists are aware of the importance of proper body mechanics when handling clients, along with incorporating physical exercise as one of the most effective approaches to preventing WMSDs. The use of well-equipped tools and equipment, promoting proper body mechanics and posture, and providing education are common preventive strategies that motivate physiotherapists to actively engage in preventing WMSDs. Furthermore, employers should adequately address the barriers, such as equipment unavailability, heavy workload, and inadequate staffing, to effectively implement the current WMSD prevention strategies. Although physiotherapist are aware of the effective approaches to preventing WMSDs, there is a significant need to overcome the barriers to their use of preventative measures in clinical practice. It is high time that the implementation and evaluation of preventative strategies should not only focus on an individual level alone but at the organizational level as well to facilitate a change within the health services to one that promotes the use of preventative strategies.
Footnotes
Acknowledgements
The authors extend their gratitude to physiotherapists for assisting in the recruitment process.
Ethical considerations
Ethical approval to conduct this study was granted by the institutional review board of the Universiti Kebangsaan Malaysia (UKM PPI/111/8/ JEP-2022-057).
Author contributions
All authors have made substantial contributions to the conception and design, or acquisition of data, or analysis, interpretation of data and drafting of the manuscript. All authors approved the final version submitted for publication and take responsibility for statements made in the published article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Informed consent
All participants gave their written consent prior to data collection.