
Abstract
Background
In Thailand's agricultural sector, physically demanding labor and a high prevalence of chronic health conditions present substantial challenges to maintaining work capacity. However, few tools are available to assess work capacity among farmers.
Objective
This study aimed to evaluate the validity and reliability of the Thai version of the Work Functioning Impairment Scale (Thai WFun).
Methods
The study involved 385 rice farmers from Prakhon Chai district, Buriram province, Thailand, during November and December 2023. The WFun was translated from Japanese to Thai using a standard translation procedure. Participants then completed questionnaires, including the Thai WFun and the Work Ability Index (WAI). The convergent validity between the Thai WFun and WAI was examined through analysis of variance with linear trend tests. The factorial validity was assessed through confirmatory factor analysis (CFA) based on a one-factor model. The reliability of the Thai WFun was assessed using Cronbach's alpha.
Results
A significant linear trend was observed, indicating that as WAI scores decreased, Thai WFun scores increased (p < 0.001). Sub-factor analyses revealed similar patterns, including the physical and mental demands of work, a comparison with highest work ability ever, and absenteeism in the past year (all p < 0.001). CFA results demonstrated a reasonable model fit. The scale exhibited moderate internal consistency, with Cronbach's alpha of 0.668.
Conclusions
The findings validate the Thai WFun as a reliable tool for assessing work capacity among rice farmers, with potential to guide tailored occupational health strategies in agriculture.
Introduction
Work capacity is a key concern in Thailand's agricultural sector. Farmers often perform physically demanding tasks with limited machinery and insufficient health protection. 1 The sector also faces challenges such as severe labor shortages and a decreasing number of younger workers. 2 As a result, the agricultural workforce increasingly comprises older farmers, many of whom suffer from chronic health conditions. 3 Illnesses such as back pain, 4 rheumatoid arthritis, 5 and chronic kidney disease 6 can significantly impair work capacity. This situation is exacerbated by the lack of social security systems, including pensions and workers’ accident compensation. 7 Therefore, maintaining work capacity has become essential to ensure individual livelihoods and the sustainability of rural agriculture in Thailand.
Research on assessing work capacity in Thailand is currently in the early stages, and few tools are available. The Work Ability Index (WAI) is the only notable tool that has been translated into Thai, although it is primarily used for academic purposes rather than practical application. 8 In addition, the complexity of the WAI and the health information it requires mean this instrument is impractical for routine use, especially in rural settings where non-medical professionals often handle data collection. 9 This highlights the need for more accessible, user-friendly tools to effectively assess and enhance work capacity among aging farmers.
The Work Functioning Impairment Scale (WFun) was developed in Japan and adapted for Chinese and English-speaking populations.10,11 The use of the Rasch measurement model is a key strength of the WFun, as it ensures consistent and reliable assessments across diverse demographic groups with high reliability (item reliability = 0.98, person reliability = 0.86) and validity. 10 This is crucial for tools used in globalized labor markets, where consistent health assessments among diverse workforces are needed. In addition, the WFun has seven questions that avoid medical queries, and is easy to use and maintains respondents’ privacy. These advantages mean the WFun offers a practical alternative to the WAI. The scale is focused on assessing comprehensive health impacts that affect work capacity, making it especially valuable for rural settings in Thailand where aging farmers frequently suffer from multiple health conditions. 12 In addition, this tool supports the implementation of targeted interventions to enhance the work capacity of these farmers. 13
Given the limitations of existing tools in rural settings, it is critical to develop a suitable assessment method for Thai farmers. Therefore, this study aimed to evaluate the validity and reliability of a Thai version of the WFun. We anticipate that the scale will provide practical insights into managing work capacity and developing tailored occupational health strategies in Thailand's agricultural sector.
Methods
WFun
The WFun was developed in Japanese by Fujino et al. in 2015, and serves as an instrument for measuring the impact of health issues on work capacity. 10 This scale stands out in the occupational health field because of its focus on health-related work impairments rather than economic productivity loss. 14 The WFun comprises seven items with no medical queries (e.g., “I haven’t been able to behave socially”). This concise format is designed for ease of use and quick completion, which enhances its practicality for regular implementation. Each item is scored on a scale from 1 (not at all) to 5 (almost every day), with a total possible score of 7–35. Scores of 21 or higher indicate significant impairment, which provides a clear threshold for identifying serious work capacity issues. 15
First phase: Translation and cross-cultural adaptation
The adaptation of the WFun to the Thai context was conducted in accordance with the assessment procedures established by Harkness and Schoua-Glusberg. 16 The final Thai version is presented in the Appendix. With permission from the original author, Dr Fujino, the process began with forward translations of the instrument into Thai by two experts. One translation was performed by a Thai professional interpreter who specialized in administrative translation from Japanese to Thai. The second was completed by an occupational health specialist familiar with psychometric scales, who translated the English version of the WFun into Thai. Subsequent reconciliation of these translations was used to address any discrepancies. Next, a different Thai professional interpreter, also specialized in administrative translation, performed a back-translation from Thai into Japanese to ensure the fidelity and accuracy. An expert panel comprising occupational health, ergonomics, rural health, and psychometrics specialists reviewed the final Thai version for conceptual accuracy and cultural suitability. Throughout this process, Japanese researchers with extensive knowledge of the WFun collaboratively deliberated with the Thai researchers to ensure the translation was consistent with the original scale's construct and its suitability for the Thai context. Finally, pre-testing was conducted with 30 farmers at the study site. This pre-testing confirmed the clarity, cultural relevance, and feasibility of the Thai WFun.
During this process, some WFun items posed translation challenges. For example, item 1 (“I haven’t been able to behave socially”) was translated as “I haven’t been able to interact socially with my colleagues.” This change was made to prevent any misunderstanding that may lead farmers to think of broader social systems. For item 3 (“I have had trouble thinking clearly”), it was hard to find an appropriate Thai equivalent for “trouble thinking clearly,” therefore it was translated as “I have felt too anxious to concentrate on my work.”
Second phase: Data collection
For assessing the validity and reliability of the Thai WFun, we conducted a cross-sectional study among 385 rice farmers in Prakhon Chai district, Buriram province, Thailand. Eligible participants were rice farmers aged 18 years and older who had been actively engaged in full-time rice cultivation for at least the past 12 months. We excluded individuals who could not understand Thai. Participants were selected using records maintained by Prakhon Chai Hospital and the 16 sub-district Health Promoting Hospitals in Prakhon Chai. Village health volunteers at each site assisted in identifying and selecting rice farmers for this study from households in these sub-districts. Stratified sampling was implemented to ensure proportional representation from each sub-district based on its contribution to the district's total rice farming population. Next, purposive sampling was used to recruit eligible farmers, with village health volunteers facilitating their participation at sub-district Health Promoting Hospitals or village meeting points.
Data were collected by trained researchers through structured face-to-face interviews. The questionnaires completed included the WFun, WAI, and demographic variables (e.g., sex, age, years of rice cultivation experience, weekly working days, daily working hours, smoking, and regular alcohol drinking).
Study site
This study was conducted in Buriram Province, which is located in northeastern Thailand. In this arid region, rice cultivation is limited to a single season each year because of the low rainfall and limited irrigation infrastructure. Furthermore, despite the flat terrain, the use of advanced agricultural technologies is not widespread. Instead, farming is performed using a combination of tractors, combines, and manual labor.
The farming cycle typically begins with land preparation from May to July, which coincides with the onset of the rainy season. Farmers generally use hand tractors to till and prepare the land for rice planting. Once the land is prepared, rice seeds are sown directly into the fields; this task is still largely performed by hand. After planting, farmers focus on crop maintenance through manual tasks such as weeding, applying fertilizers, and protecting the rice plants from pests. The harvest season in Buriram usually occurs from November to December. Harvesting primarily uses combines, after which the rice is dried in the fields before being stored.
Third phase: Data analyses
Data were analyzed to establish descriptive statistics and assess the internal consistency and convergent validity of the Thai WFun. To evaluate the convergent validity, we performed analysis of variance with linear trend tests to examine the relationship between the mean scores of the Thai WFun and the four WAI categories: excellent (scores of 44–49 points), good (37–43 points), moderate (28–36 points), and poor (7–27 points). 17 Next, we explored the relationships between Thai WFun scores and specific WAI sub-factors, including physical and mental demands of work, comparison with the highest work ability ever experienced, and absenteeism in the past year. 10
Factorial validity was assessed through confirmatory factor analysis (CFA) based on a one-factor model. The indices used to evaluate model fit were: the goodness of fit index (GFI), adjusted goodness of fit index (AGFI), comparative fit index (CFI), Tucker-Lewis index (TLI), root mean square error of approximation (RMSEA), and standardized root mean square residual (SRMR). A good fit was represented by GFI, AGFI, CFI, and TLI values >0.90, a RMSEA value <0.06, and a SRMR value <0.08. 18
Internal consistency reliability was measured using Cronbach's alpha coefficient among the scale items. An alpha level of 0.05 was used to determine statistical significance. All statistical analyses were conducted using Stata/SE 16.1 (StataCorp, College Station, TX, USA) and Amos 27.0 (SPSS Inc., Chicago, IL, USA).
Results
Participants
Among the 385 participating rice farmers, the majority were women (61.8%), the average age was 58.3 ± 10.1 years (range 30–85 years), and participants had an average of 40.2 ± 14.4 years of work experience in rice cultivation (Table 1). Examination of daily working hours showed that 49.9% worked every day of the week, and 34.8% worked 4–6 h per day. Relatively few participants reported smoking (10.9%) or regular alcohol consumption (3.1%). Participants’ mean WAI score was 36.1 ± 6.2 and mean Thai WFun score was 10.1 ± 3.5.
General characteristics of study participants.
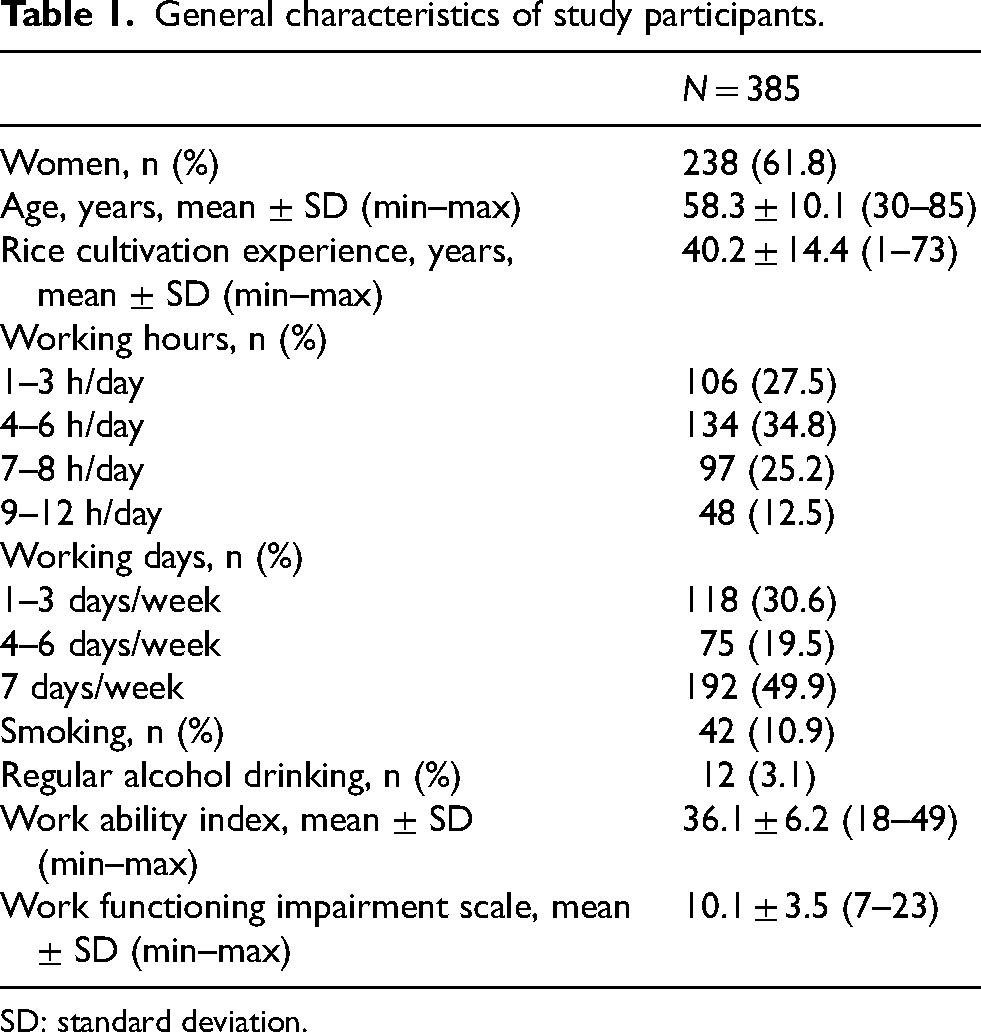
SD: standard deviation.
Convergent validity
Examination of convergent validity revealed a significant linear trend, whereby as the WAI decreased, the Thai WFun increased (all p < 0.05) (Table 2). Specifically, participants classified as having an “excellent” work ability showed the lowest mean WFun scores (mean = 7.8 ± 1.3) and those in the “poor” work ability group reported the highest mean WFun scores (mean = 13.7 ± 4.3). Further analysis of specific WAI sub-factors (physical and mental demands of work, comparison with the highest work ability ever, and absenteeism in the past year) showed similar trends (all p < 0.05).
Convergent validity of the raw scores based on Work Ability Index categories.
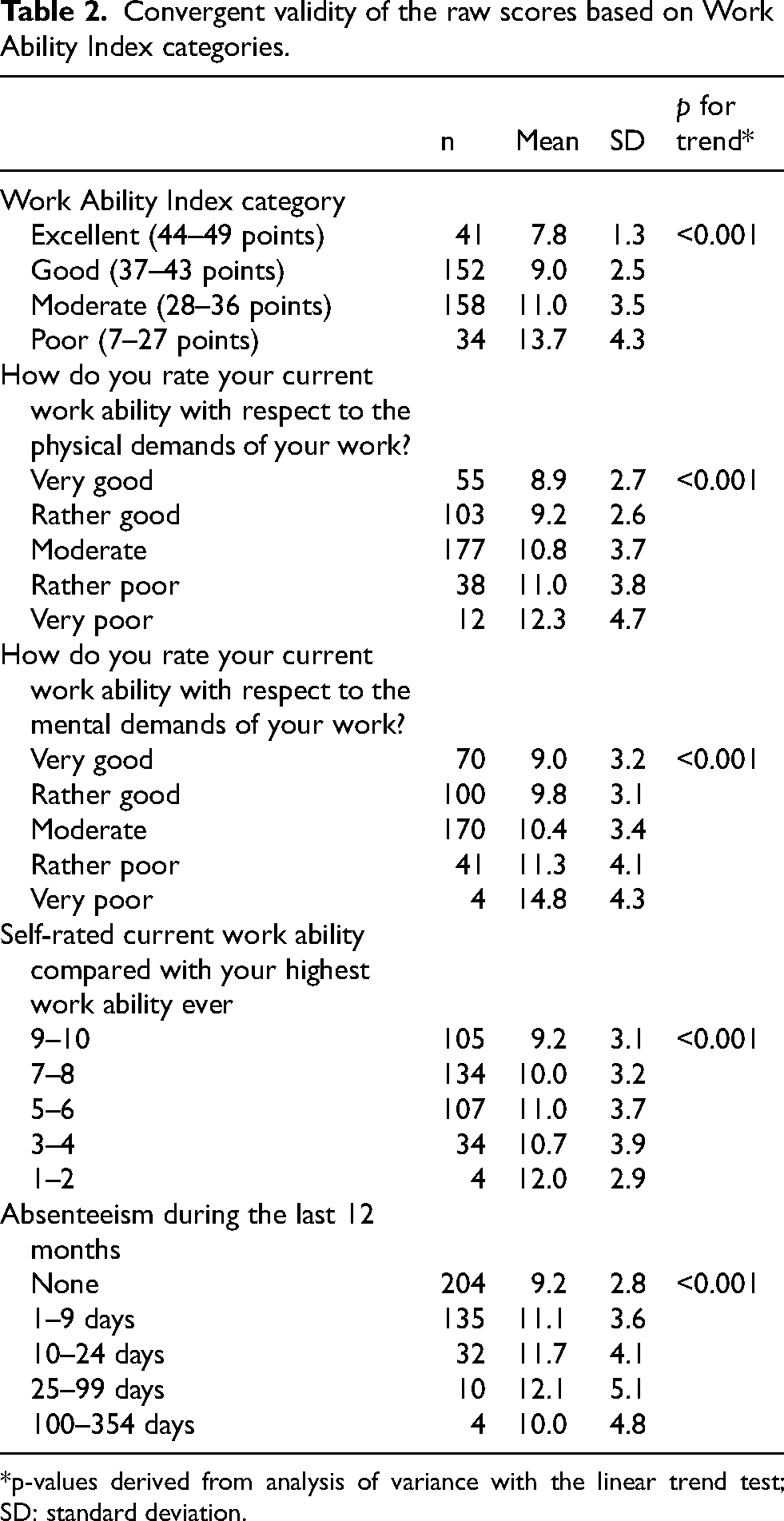
*p-values derived from analysis of variance with the linear trend test; SD: standard deviation.
Factorial validity
The CFA indicated that the one-factor model achieved a reasonable overall fit across several indices (Table 3). The GFI was 0.968 and AGFI was 0.936, whereas the CFI fell slightly below the acceptable threshold at 0.860. However, the TLI met the standard at 0.907, the RMSEA (0.078) slightly exceeded the ideal threshold, and the SRMR (0.050) was within the acceptable range.
Model fit indices from confirmatory factor analysis and reliability analysis.
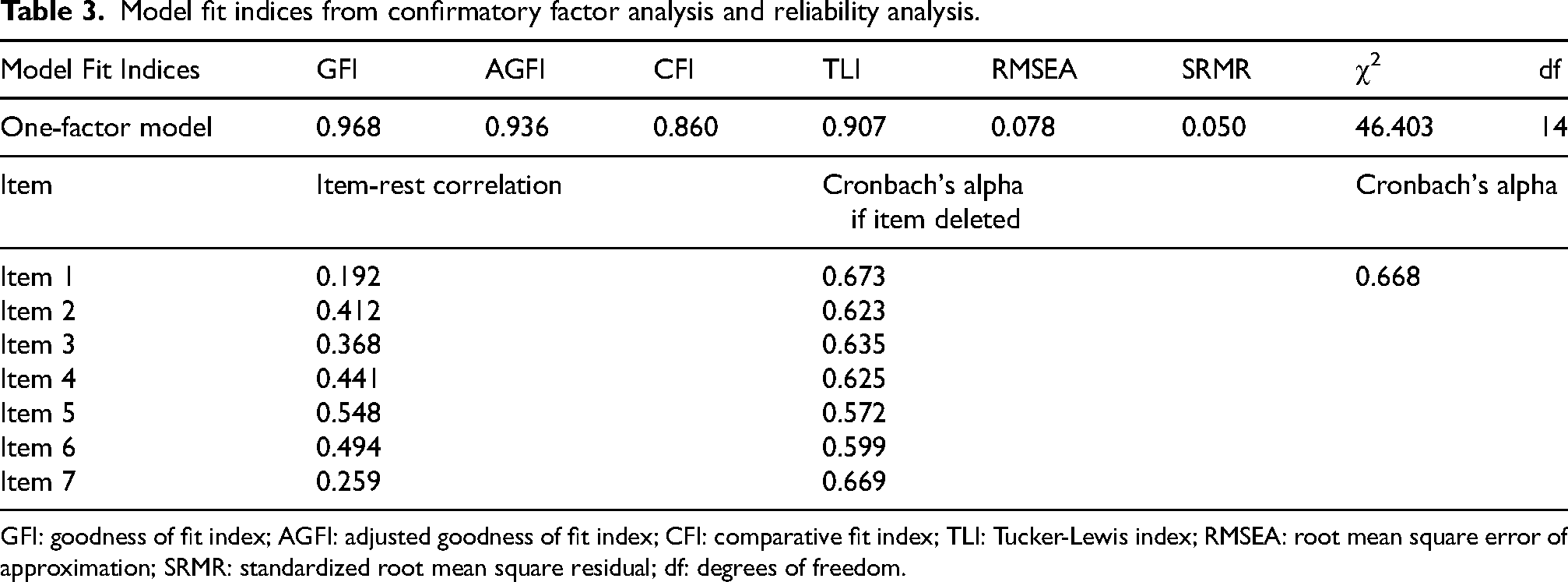
GFI: goodness of fit index; AGFI: adjusted goodness of fit index; CFI: comparative fit index; TLI: Tucker-Lewis index; RMSEA: root mean square error of approximation; SRMR: standardized root mean square residual; df: degrees of freedom.
Internal consistency reliability
Reliability analysis confirmed the overall internal consistency of the Thai WFun, with a Cronbach's alpha of 0.668 (Table 3). The item-rest correlations ranged from 0.192 for item 1 (“I haven’t been able to interact socially with my colleagues”) to 0.548 for item 5 (“I have felt that my work isn’t going well”).
Discussion
This study effectively confirmed the validity and reliability of the Thai WFun and demonstrated its effectiveness in assessing work capacity among Thai rice farmers. The convergent validity analysis showed a moderate positive correlation between WFun scores and WAI categories, with mean WFun scores gradually increasing from 7.8 in the “excellent” category to 13.7 in the “poor” category. Supporting its factorial validity, the CFA demonstrated an overall reasonable fit, although the CFI fell slightly below and the RMSEA slightly exceeded the ideal thresholds. Internal consistency, as measured by Cronbach's alpha (0.668), suggested moderate reliability. This was considered acceptable given the scale's limited number of items, which can often result in lower alpha values. 19 These results indicated the Thai WFun can be used to evaluate work capacity among rice farmers.
The present study suggested the Thai WFun may be useful in occupational health settings in Thailand. In Thailand's agricultural sector, formal occupational health support is scarce and employers often assume responsibility for making any necessary work adjustments. 12 The Thai WFun could become an indispensable tool for these employers by facilitating the evaluation and accommodation of complex health challenges faced by older farmers. Furthermore, the Thai WFun can assess the impact of workplace interventions on employee health, such as adjustments to work hours, schedules, physical environments, and job designs, along with reduction of workplace hazards. 20 Previous studies have also shown that the WFun can predict future absenteeism and occupational accidents,21,22 which highlights its potential as an assessment tool for workplace interventions. Specifically, the Thai WFun can be used to evaluate health activities at the workplace level, 23 which in Thailand would likely involve employers, as well as village health volunteers working with sub-district Health Promoting Hospitals. Further studies should explore the effectiveness of the Thai WFun in assessing workplace interventions and community-based programs.
Some fit indices in the CFA may have fallen short of ideal thresholds because of challenges posed by cultural and linguistic differences. For example, “I haven’t been able to behave socially” (item 1) was translated as “I haven’t been able to interact socially with my colleagues” to prevent misunderstandings related to broader social systems. This change was necessary to align with the social dynamics of rural Thai communities, where labor is organized through informal, egalitarian relationships rather than the hierarchical structures common in corporate settings. Similarly, “I have had trouble thinking clearly” (item 3) was translated as “I have felt too anxious to concentrate on my work,” because it was difficult to find a direct Thai equivalent for “trouble thinking clearly.” These translation choices may have contributed to the relatively low item-rest correlations observed (item 1: 0.192; item 3: 0.368). This highlighted the challenge of translating abstract cognitive concepts across languages and cultures, and potentially affected the validity of the present study.
Regarding the evaluation of internal consistency, the Cronbach's alpha could have been influenced by the limited number of WFun items and the narrow response range. Notably, 87% of participants scored 7–14 on the WFun (data not shown), indicating they had no work impairment. This proportion significantly exceeded the approximate 50% observed in general workplace settings. 10 This pattern may indicate a reduced perception of work-related health issues among Thai farmers, which could be attributable to the “healthy worker effect” or effective work adjustments for older workers. 3 These observations highlight the need for careful consideration of the social and occupational contexts in the Thai agriculture sector.
There were several limitations in this study. First, as the study relied on cross-sectional data collected at a single point in time, it was not possible to evaluate the tool's test-retest reliability or responsiveness. In addition, items 1 and 7 showed relatively low item-rest correlations, which may reflect cultural or linguistic challenges in adapting these items. Although their exclusion had little effect on the overall internal consistency, further studies should explore whether refinement or revision of these items is necessary to enhance the performance of the scale in Thai settings. Finally, the involvement of village health volunteers in participant selection could have introduced selection bias. Specifically, farmers who were more accessible to the village health volunteers might differ in psychological characteristics that could influence WFun scores compared to those less accessible. This sampling approach was chosen because all farmers are registered in the local health system, and village health volunteers are responsible for supporting the health of residents in their designated areas. Future research should incorporate repeated testing and employ strategies to minimize sampling bias, such as random sampling or stratified sampling across different areas.
Conclusions
This study successfully translated the WFun into Thai and confirmed its validity and reliability for assessing work capacity among Thai rice farmers. The results demonstrate the potential utility of the Thai WFun in occupational health settings. It is particularly effective in identifying adult farmers who often experience with various chronic conditions and highlighting necessary workplace adjustments.
Supplemental Material
sj-pdf-1-wor-10.1177_10519815251390492 - Supplemental material for Validity and reliability of the Thai version of the work functioning impairment scale (Thai WFun)
Supplemental material, sj-pdf-1-wor-10.1177_10519815251390492 for Validity and reliability of the Thai version of the work functioning impairment scale (Thai WFun) by Rachaneekorn Weeracharoen, Sara Arphorn, Chatchai Thanachoksawang, Piyaporn Chantarasri, Chalermsiri Theppitak, Teepapipat Lertvarayut, Suwatsa Punneng, Yoshihisa Fujino and Tomohiro Ishimaru in WORK
Footnotes
Acknowledgments
The authors gratefully acknowledge Mr Narong Poungdaw, Head of the Prakhon Chai District Public Health Office, for his invaluable assistance in data collection. The authors also extend their thanks to Assoc. Prof. Akiomi Inoue of the University of Occupational and Environmental Health, Japan for his invaluable support with the statistical analysis.
Ethical approval
Ethical approval for this study was obtained from the Mahidol University Ethical Review Committee for Human Research (MUPH2023-081).
Informed consent
All participants provided written informed consent before participating in this study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Japan Society for the Promotion of Science, (grant number 22K17379).
Declaration of conflicting interests
Dr. Fujino holds the copyright to the WFun with royalties paid from Sompo Health Support Inc., outside of this work. The other authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.