
Abstract
Background
Architecture students are at increased risk of musculoskeletal pain (MSP) due to extended sedentary work frequently performed in non-ergonomic postures.
Objective
This study evaluates their awareness (current knowledge, practice, and attitude) of ergonomics and the prevalence of self-reported MSP.
Methods
This descriptive cross-sectional study was applied to 123 students using a self-administered questionnaire. The questionnaire collected data on demographics, work nature, ergonomic awareness, work demands, and prophylactic remedies.
Results
Most (73.2%) lacked prior knowledge of ergonomics, with a borderline association with female gender (P = 0.07). Twenty-five % of males and 28.5% of females were unaware of work-related risks associated with poor ergonomics. Female students reported poorer ergonomic practices than males, including lower adherence (47.1% vs. 30.1%, χ²=8.57, P = 0.01), inadequate workspaces (28% vs. 13%, χ²=7.56, P = 0.01), more frequent floor sitting (31.7% vs. 8.9%, χ²=14.39, P < 0.001), and fewer work breaks (χ²=14.39, P < 0.001). Despite this, 90.2% expressed positive attitudes toward ergonomics. The prevalence of self-reported musculoskeletal pain was high, especially among females, who reported more pain in the shoulders, upper back, wrists, and hands (p < 0.05).
Conclusions
These findings underscore the need for targeted interventions, such as educational programs and ergonomic assessments, to raise awareness and prevent musculoskeletal pain among architecture students.
Introduction
Architecture students, who pursue a degree or specialization in architecture, are immersed in a physically demanding discipline. The pursuit of design excellence often entails extended periods spent working at a drafting table or in front of a computer screen. This practice involves repetitive, precise movements during activities such as sketching and model-making, which can result in specific physical strains. While this environment fosters creativity, it also presents significant challenges to the physical well-being of students.1,2
Ergonomics is the science of designing and arranging the environment to fit the needs of the individual; it focuses on optimizing human performance and reducing the risk of injuries or discomfort caused by repetitive tasks and poor body positioning.3,4 Ergonomics is a dynamic, multidisciplinary field that examines how people interact with different system elements. It is typically categorized into three main areas: physical ergonomics, cognitive ergonomics, and organizational ergonomics, each focusing on various aspects of how humans interact with systems. 4
Physical ergonomics studies how the human body structure and movement relate to physical activity and surroundings. It examines interactions with tools, equipment, and workspace design to improve comfort and efficiency. 4 Good ergonomic posture contributes to long-term health by preventing chronic conditions such as back pain, neck pain, and repetitive strain injuries. Moreover, ergonomic posture improves overall productivity and efficiency; when the body is balanced, energy is conserved, and tasks can be performed effortlessly. 5
Creating an ergonomic workstation is crucial, including an adjustable chair with proper lumbar support, a desk at the correct height, an eye-level monitor, and an ergonomic keyboard and mouse. 6 It is common knowledge in various professions that work-related injuries are a primary source of disability that poses a significant challenge to workers, society, and employers.7,8 Additionally, when musculoskeletal problems persist or worsen, individuals should seek the expertise of healthcare professionals, such as physiotherapists, who can provide valuable assistance in resolving these issues through exercises, manual therapy techniques, and lifestyle modification advice.7,9 However, the potential impact on the healthcare system must be considered, as the increased demand for their services can create a heavier workload. 10
Work-related musculoskeletal pain (MSP) can be a significant issue for architects due to their profession's physical demands; over 80% of architects suffer from MSP, primarily in the neck, lower back, and shoulders.. 11 Unfortunately, musculoskeletal problems have been reported even for architecture students. Among Pakistani architecture students, neck pain was prevalent in 70.9%, shoulders in 54.8%, upper backs in 52.8%, and lower backs in 65.8%. 1 Another study revealed that 78% of architecture students in Nigeria experience MSDs, with neck pain being the most prevalent issue, affecting 51% of the students. 2 To reduce the risk of MSP, the architecture students should adopt ergonomics early in their practice.
Health professionals such as physicians, therapists, technicians, and nurses have extensively studied their ergonomics awareness.12–15 In addition to other professions, for example, office employees, computer users,,16,17 and even children in school sitting. 18 However, architecture students’ knowledge, attitude, and awareness are sparse. Investigating the awareness level of architecture students about ergonomic posture and musculoskeletal issues underscores the need to bridge knowledge gaps and introduce strategies to enhance ergonomic practices within the architectural field.
Consequently, this study aimed to: (1) assess architecture students’ ergonomic awareness, encompassing their knowledge, practices, and attitudes; (2) examine the relationship between this awareness and the variables of age and academic level; and (3) determine the prevalence of self-reported MSP among the cohort. It was hypothesized that a significant relationship exists between ergonomic awareness (knowledge, practices, and attitudes) and both age and academic level.
Methods
Study design and setting
This descriptive cross-sectional study was conducted between January and March 2023. Using
Participants
Using a convenience sampling method, the study included students who had completed their first preparatory year at the College of Architecture and Planning at King Saud University (KSU), enrolled in the second to fifth academic year at the time of the study, aged 18 to 25 years, and represented both genders, and voluntarily consented to participate in the study
Instrumentation
A self-administered questionnaire was designed based on the literature.23–25 The questionnaire had three sections. Section A (six demographic questions: age, gender, height, weight, body mass index (BMI), and academic year), section B addressed the nature of work, assignments, and requirements (seven questions), and section C addressed awareness of the importance of ergonomics, it consists of four subtitles: knowledge (three questions), practice (eight questions), attitude (five questions), workload demand (three questions), and prophylactic remedies (four questions). Some questions required “yes” or “no” answers, while others offered multiple-choice response options.
Ten experts (five physical therapists, two faculty members of the Architecture and Building Sciences program, and three undergraduate architecture students) evaluated the face and content validity of the designed questionnaire. Their comments were all addressed. The validity was measured using the content validity index (CVI). The item-CVI, Scale-CVI/Average, and Scale-CVI/Universal agreement were 0.85, 0.98, and 0.79, respectively. The modified kappa (K*) was calculated to adjust the chance of agreement using this formula: K* = (I-CVI—Pc)/(1—Pc), where Pc = [N/A (N—A)] x 0.5N, Pc = probability of a chance, N = number of raters; A = number of agreements. The K* of each statement ranges between 0.89 and 0.99, indicating excellent validity.26,27 The questionnaire's usability, clarity, and understanding were tested on 20 students before its distribution.
Procedure
The questionnaire was administered online using the Google Forms Platform. The link to the questionnaire was emailed to the architecture students through King Saud University's Questionnaire Centre (a reminder email was sent after three weeks), through social media using the Twitter account of the architecture students’ club, and the students’ group on WhatsApp. The students were asked to provide the last four digits of their university identification numbers before starting the questionnaire. To ensure impartiality, data were collected via a standardized online survey, guaranteeing consistent questioning free from researcher influence, and analyzed using objective descriptive statistics to prevent interpretive bias.
Statistical analysis
The data from the online questionnaire were transferred and imported into a statistical analysis program using an Excel spreadsheet. An IBM SPSS Statistics for Windows (Version 28; Armonk, NY) analysis was conducted. The data normality was tested using the Shapiro‒Wilk test for age, height, weight, and BMI. Mean and standard deviation or medians (1st and 3rd quartiles) were calculated for continuous data as appropriate. Frequencies and percentages were estimated for categorical variables (gender and academic level) and ergonomic awareness, ergonomic postural questions, physical workload, and demand questions.
Pearson's chi-square (χ2) test was used to determine the association between gender, academic year, and the data obtained from awareness of ergonomics questions. Fisher's exact test was used when the variable had a cell count less than 5. The significance level was at α = .05 (95% confidence).
Results
Participants characteristics
A total of 123 of the 484 distributed questionnaires were included in the final analysis after excluding incomplete questionnaires (if 20% left unanswered) and declined questionnaires, yielding a response rate of 25.4%. Demographic details—including age, weight, height, BMI, and gender—are summarized in Table 1. None of the data followed a normal distribution (P < 0.05). Participants represented various academic years: second (30.1%), third (26.8%), fourth (30.1%), and fifth (13.0%) year students (Table 1).
Demographic characteristics of the participants (n = 123).
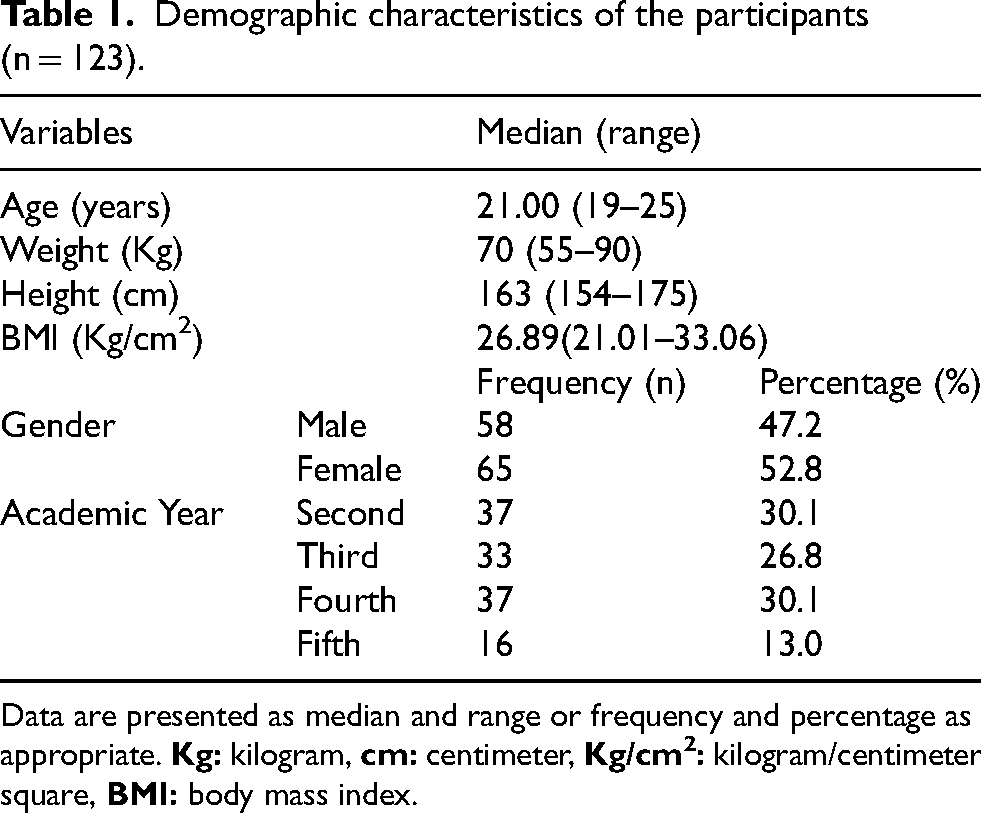
Data are presented as median and range or frequency and percentage as appropriate.
Nature of work, assignments, and academic requirements
Regarding academic workload, 56.9% of students took subjects requiring extensive paperwork—most (78.4%) were in their 2nd year (χ²=14.32, P = 0.003). Digital work was more common, with 73.2% enrolled in such subjects; 94.6% of these were 4th-year students, while 2nd-year students had the lowest proportion (64.9%) (Fisher's test = 37.41, P < 0.001). Over 43% had more than seven paper-based assignments, and 56.1% had over seven digital ones. Notably, 56.8% of 2nd-year students had more than nine paper-based assignments (χ²=29.02, P = 0.004). About 65% had a drafting table at home. Work location differed by gender: 60% of females worked mostly at home, while 51.7% of males split time between home and college (χ²=19.06, P < 0.001), and 61% reported working more than five hours daily.
Awareness of the importance of ergonomics
Knowledge
Table 2 summarizes participants’ ergonomic knowledge by gender and academic year. Most (73.2%) lacked prior knowledge of ergonomics, with a borderline association with female gender (P = 0.07). Instructors had not covered ergonomics for 33.3% of males and 43.1% of females. Twenty-five % of males and 28.5% of females were unaware of work-related risks associated with poor ergonomics. No significant association was found between academic year and ergonomic knowledge or workplace efficiency (P > 0.5).
Awareness regarding the importance of ergonomics (knowledge) and its association with gender and academic year (n = 123).
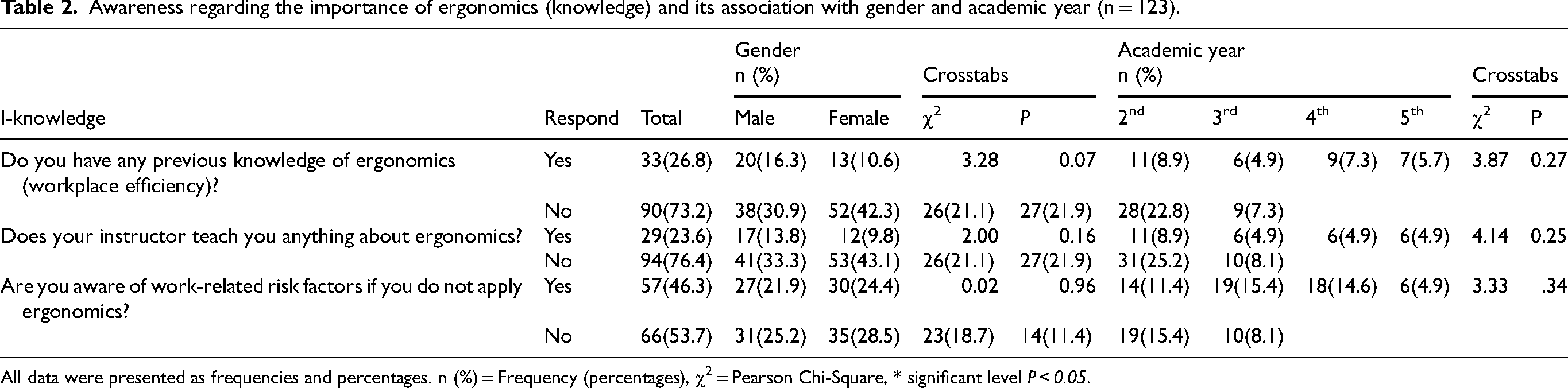
All data were presented as frequencies and percentages. n (%) = Frequency (percentages), χ2 = Pearson Chi-Square, * significant level P < 0.05.
Practice
Table 3 summarizes ergonomic practices among students. Most (77.2%) did not apply ergonomics daily, with a higher percentage of females (47.1%) than males (30.1%) (χ²=8.57, P = 0.01). More males (65.5%) than females (33.8%) agreed that the college drafting tables suited their height (P < 0.001). Comfort with tables and chairs showed no significant gender difference (P > 0.05), though more males (33.3%) reported having suitable home workspaces than females (24.4%) (χ²=7.56, P = 0.01). Second-year students reported greater comfort with drafting tables (P = 0.02) and chairs (P < 0.001).
Awareness regarding the importance of ergonomics (practice) and its association with gender and academic year (n = 123).
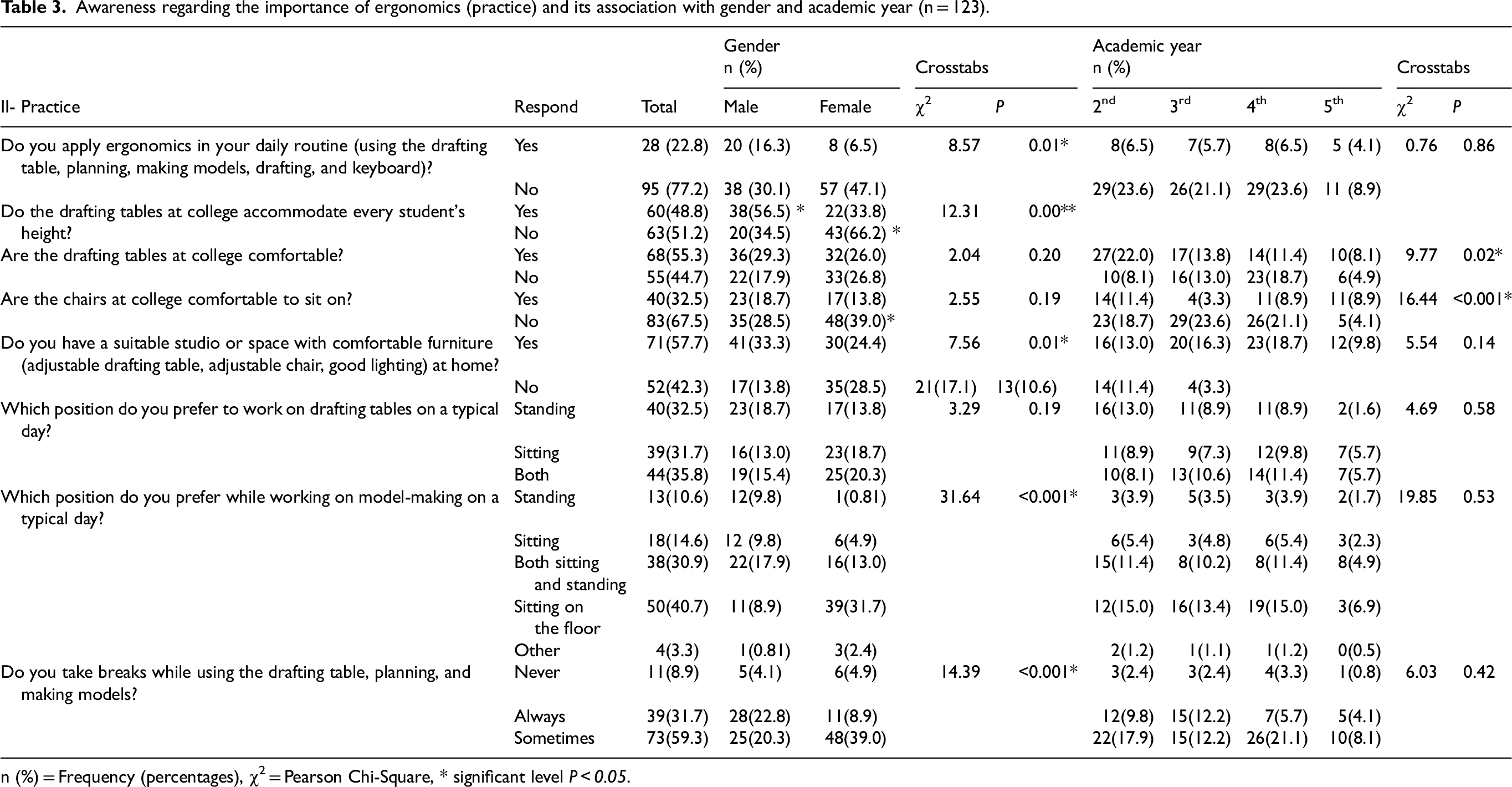
n (%) = Frequency (percentages), χ2 = Pearson Chi-Square, * significant level P < 0.05.
Drafting table posture preferences were similar across genders (P = 0.19). However, females more often sat on the floor while model making (31.7%), while males preferred mixed postures (Fisher's exact test = 31.64, P < 0.001). Break-taking habits also differed significantly: 22.8% of males always took breaks, compared to 8.9% of females (χ²=14.39, P < 0.001).
Attitude
Most participants think ergonomics is beneficial (90.2%) and believe it may improve their daily performance in modeling, hand drawing, and sketching (89.4%), with no significant association with gender or academic year (P > 0.05, Table 4). Additionally, 91.9% (41.5% male and 50.4% female) agreed that architectural work is physically demanding. A significant gender difference was found in the positions the students believe cause physical stress (χ²=17.59, P = 0.04). Standing was reported as the most stressful (62.6%), followed by sitting on the floor (60.2%) and sitting (53.7%), with females reporting higher stress levels across all positions. Most (39.0% of males and 49.6% of females) agreed or strongly agreed that proper ergonomics would improve learning outcomes with no effect of gender or academic year (p > 0.05).
Awareness regarding the importance of ergonomics (attitude) and its association with gender and academic year (n = 123).
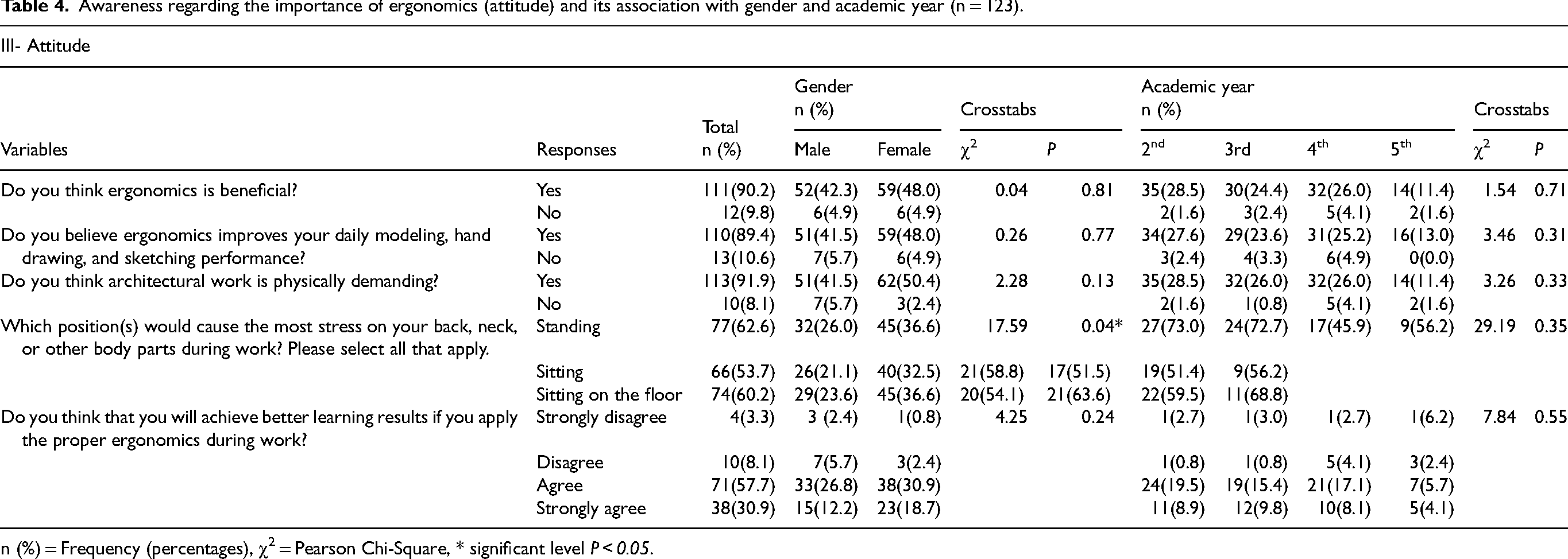
n (%) = Frequency (percentages), χ2 = Pearson Chi-Square, * significant level P < 0.05.
Workload demands
Most students (95.1%) reported feeling exhausted after tasks like manual handling, repetitive movements, or awkward postures, with no gender association (χ²=2.35, P = 0.12). However, exhaustion was significantly associated with academic year (Fisher's exact test = 6.48, P = 0.04), with 4th-year students reporting the highest percentage (29.3%). Common work-related scenarios included static shoulder/arm positions (males 55.2%, females 56.9%, χ²=0.04, P = 0.85), tensed shoulders/hands (males 46.6%, females 70.8%, χ²=7.45, P = 0.01), and inconvenient postures (males 39.7%, females 58.5%, χ²=4.34, P = 0.04). More females reported prolonged sitting or standing (66.2%) and sitting with a reclined back (73.8%) (χ²=2.06, P = 0.15, χ²=7.44, P = 0.01). A significant academic year association was observed, with more 3rd-year students reporting tensed shoulders/hands (75.8%) and repetitive movements (69.7%) (χ²=7.95, P = 0.04, Fisher's exact test = 10.33, P = 0.02).
Table 5 presents the locations of MSP reported by students. Nearly all participants (99.2%) experienced pain in one or more areas: Neck (74.8%), Shoulder (62.6%), Upper Back (61.0%), Elbows (17.9%), Wrist/Hand (50.4%), Lower Back (69.9%), Hips/Thighs (24.4%), Knees (38.2%), Ankles/Feet (30.9%).
Musculoskeletal pain sites, n = 123.
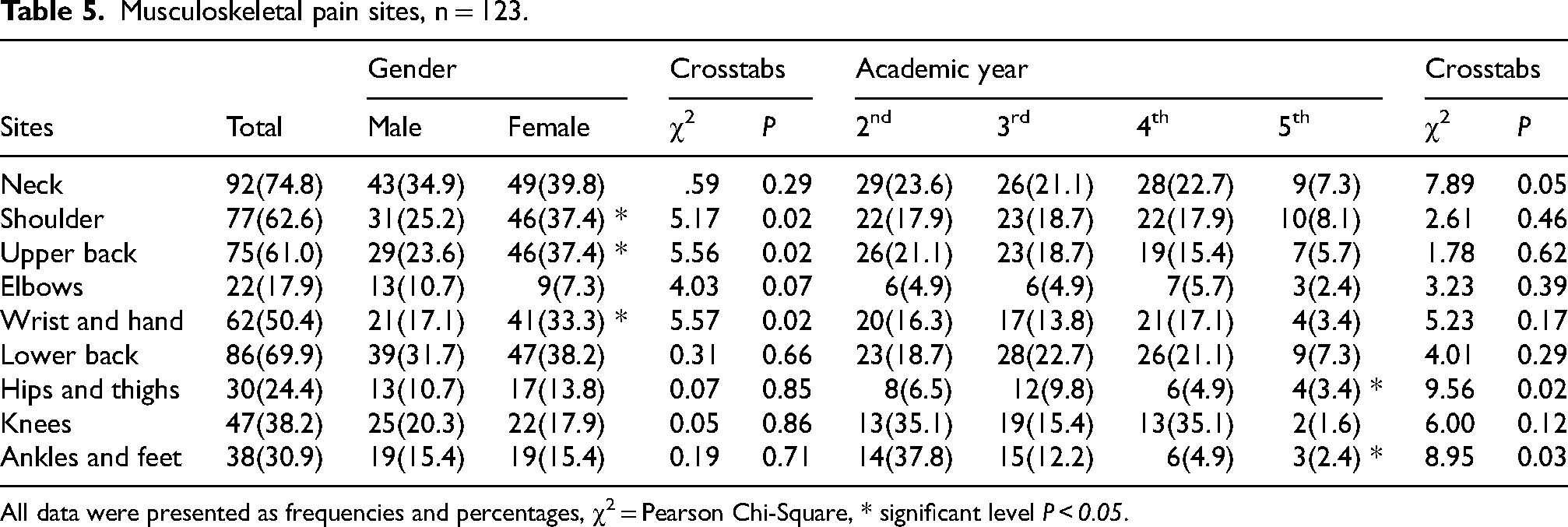
All data were presented as frequencies and percentages, χ2 = Pearson Chi-Square, * significant level P < 0.05.
A significant gender difference was observed in the prevalence of pain at specific sites. Female participants reported significantly higher rates of pain than males in the shoulder (χ²=5.17, p = .02), upper back (χ²=5.56, p = .02), and wrist/hand (χ²=5.57, p = .02).
The pain of hips and thighs is significantly associated with academic year (Fisher's exact test = 9.56, p = 0.02), with 3rd-year students reporting the highest prevalence (9.8%). Ankle/foot pain also varied significantly by academic year (Fisher's exact test = 8.95, p = 0.03), with 2nd-year students reporting the highest rate (37.8%).
Prophylactic remedies
Some participants (26.0%) experienced pain severe enough to require pharmacological treatment. The most common pain relief methods were stretching exercises (43.1%) and walking (25.2%), while hot packs and other methods were less frequently used (14.6% and 13%, respectively). Gender was associated with hot pack use, with 23.1% of females compared to 5.2% of males using them (χ²=7.87, P = 0.01). There was no association between academic year and pain relief choice. Most students (78.9%) had never seen a doctor or physiotherapist for pain, with no gender or academic year association. Additionally, 50.4% reported never engaging in physical activities, and 45.5% never performed stretching exercises during or after work, with no significant gender or academic year differences (P > 0.05).
Discussion
The study assessed the architecture students’ awareness of ergonomics, including their knowledge, practices, attitudes, workload demands, MSP, and pain relief methods. Most participants lacked prior knowledge of ergonomics, with a potential gender trend. Both genders showed low awareness of work-related risks associated with poor ergonomics. Female participants reported poorer ergonomic practices, including lower adherence, inadequate workspaces, more floor sitting, and fewer breaks, although they have a positive attitude toward ergonomics. Self-reported MSP was notably high, particularly among females, who experienced more upper-body pain.
The findings reveal a significant gap in ergonomic knowledge, poor ergonomic practices, widespread MSP, and stress linked to workload. Consistent with the present study, other research has found that students in fields requiring awkward postures, such as healthcare, often lack prior ergonomic knowledge and exhibit poor practices despite maintaining a positive attitude toward ergonomics.12,28
Jaafar et al. (2020) assessed ergonomic awareness among senior undergraduate engineering students, including those in civil engineering, a field similar to architecture. Their findings revealed a significantly higher level of ergonomic knowledge (57.7%) compared to the present study's 26.8%. This difference may be due to Jaafar et al.'s focus on final-year students, while the current research included students from all academic levels. Additionally, Tysiąc-Miśta et al. (2024) found that a significant portion of dental students exhibited “good” (47.9%) and “fair” (46.7%) levels of ergonomic knowledge related to dental practices, higher than the percentage found in this study. 29 The greater focus on health and safety in dental education may explain the higher levels of ergonomic knowledge among dental students.
Several factors could explain the high percentage of students reporting a lack of ergonomic information. One possibility is that instructors themselves may not have adequate knowledge in this area. Supporting this, Atueyi et.al. (2021) found that 26.4% of engineering faculty members were unaware of ergonomic principles. 30 Additionally, Ekechukwu (2019) showed that while 61.22% of engineers knew about ergonomics, only 45.53% practiced it. 24 However, Ekechukwu study focused on professional engineers.
Even though instructors might understand the importance of ergonomics, the structure of the curriculum could mean that essential subjects take priority, potentially causing significant topics like ergonomics to be neglected. 31
The findings of this study reveal that most architecture students are unaware of work-related risk factors when ergonomic principles are not applied. This lack of awareness poses potential long-term health risks and may impact their professional careers, as noted in previous research.11,32 A key factor contributing to this issue is the limitations of current curricula, which tend to prioritize core subjects while overlooking supplementary yet crucial topics like ergonomics.
A significant portion of students (77.2%) reported not applying ergonomic principles when using drafting tables, planning, making models, drafting, or using keyboards. This reflects the previously noted lack of ergonomic knowledge and aligns with other studies showing that, despite recognizing the importance of ergonomics, students often do not put it into practice.12,33
Males were more likely to report using ergonomic practices, such as utilizing proper furniture and taking breaks while working. On the contrary, females were more likely to work while sitting on the floor—a posture associated with musculoskeletal problems. 34 A similar study by AlHazim found that female healthcare workers were more prone to poor ergonomic practices. 12 This suggests potential gender differences in perceptions or practices, warranting further investigation.
On the other hand, nearly all architecture students in this study expressed a positive attitude toward ergonomics, believing it could enhance their daily performance. However, nearly all students reported that architectural work is physically demanding, with females experiencing a significant impact. Notably, females reported higher stress levels across all postures—standing, sitting, and lying on the floor. Gender differences in chair-and-desk posture have been explored in previous studies.35,36 These varying perceptions of postural stress may be influenced by factors such as differences in musculoskeletal structure and hormonal influences. 37
The finding that many students, especially in their early academic years, feel exhausted after studying is consistent with the considerable time and workload devoted to paper and digital-based assignments. This is consistent with existing research on student burnout and academic stress38–42 which shows that high academic demands can negatively affect student well-being.43,44 The lower levels of reported exhaustion among final-year students may be due to their improved ability to manage academic stress.
The sustained static postures and repetitive motions, mainly reported by female students, are recognized risk factors for musculoskeletal problems, aligning with current occupational ergonomics research. 36 45–48 The exceptionally high rate of MSP (99.2%) reported across various body areas, especially the neck, lower back, and shoulders, mirrors epidemiological findings in young adults, highlighting widespread ergonomic concerns.
Numerous studies have shown that females are more likely to experience MSP than males, particularly in the neck, shoulders, and lower back.49–53 This aligns with the current study's findings, indicating that the gender differences observed among architecture students reflect broader trends in MSP research. The study also suggests that poor ergonomic practices among female students may contribute to this phenomenon. Additionally, females are more likely to experience MSP due to biological differences (e.g., hormonal fluctuations, lower muscle mass), greater pain sensitivity and likelihood of reporting pain, engagement in repetitive tasks and ergonomic challenges, higher stress and caregiving responsibilities, and differences in healthcare access and response.
The findings show a significant association between academic year and hip/thigh and ankle/foot pain. Fifth-year students reported less pain than those in earlier years, possibly due to differences in workload, ergonomic practices, and the development of coping strategies, improved posture, or routine adjustments. This aligns with established pain management research suggesting that individuals can learn to manage pain over time.54–56 Students experiencing pain in earlier academic years might learn strategies to mitigate their symptoms.
The study highlights that most architecture students experience MSP severe enough to necessitate pharmacological treatment or consultation with a doctor or physiotherapist, emphasizing the significant toll that academic demands can take on their physical health. The exceptionally high rate of MSP (99.2%) reported across various body areas, especially the neck, lower back, and shoulders, mirrors epidemiological findings in young adults, highlighting widespread ergonomic concerns. Raising awareness about physical therapy in preventing and managing MSP is essential, as it helps minimize downtime, aids recovery, and promotes a healthier, more efficient workforce.
The reliance on medication indicates that preventive ergonomic strategies are often insufficient or nonexistent; therefore, enhancing ergonomic practices in architecture is vital for health, productivity, and creativity. Key strategies include: 1) Optimize Workstation Design: Use adjustable furniture, position screens at eye level, and align keyboards/mice with the body to reduce strain. 2) Embrace Digital Ergonomics: Use software shortcuts, dual monitors for efficiency, and ergonomic tools like drawing tablets to minimize repetitive stress.3) Encourage Movement: Apply techniques like Pomodoro breaks, stretching routines, avoiding prolonged sitting, and boosting creativity.4) Education and Training: Offer ergonomic workshops, include training in onboarding, and perform regular ergonomic assessments.5) Feedback and Monitoring: Use surveys, feedback loops, and health apps to track and improve ergonomic practices.
Applying ergonomic principles may reduce work-related MSP and illnesses. Organizations that emphasize ergonomics often experience lower injury rates, fewer absences, higher productivity, and greater employee satisfaction. This focus on risk reduction has also influenced the creation of regulatory standards, such as those from the Occupational Safety and Health Administration and the International Organization for Standardization, which offer guidelines for integrating ergonomics into workplace practices.
A primary limitation of this study is its reliance on self-reported data, which is susceptible to recall and social desirability biases. These may have led to inaccuracies in the reporting of ergonomic behaviors and MSP levels. Additionally, the study used questionnaires rather than objective measures of posture, workstation setup, or muscle activity. While the study acknowledges curriculum limitations, it does not examine the architecture curriculum in detail to identify specific gaps in ergonomic education or instructor knowledge. Moreover, the study did not assess instructors’ ergonomic knowledge, which could be a potential limitation. Additionally, the study was conducted at a single university, and the experiences and educational contexts of architecture students at other institutions may differ significantly. This means the results may not be representative of the broader population of architecture students.
Conclusion
This study reveals a notable gap between architecture students’ positive attitudes toward ergonomics and their lack of knowledge and poor practices, resulting in widespread MSP, particularly among females. This underscores the pressing need for comprehensive ergonomic strategies, especially education within the curriculum, and for instructors to address long-term health risks. Future research should adopt longitudinal designs to track the evolution of ergonomic awareness and musculoskeletal pain throughout architecture students’ academic careers. Furthermore, developing and evaluating targeted ergonomic intervention programs is critical for improving student well-being. Additionally, future research could build on current findings using a mixed-methods approach, where a subset of survey participants is selected for subsequent objective ergonomic testing to correlate subjective awareness with objective physical measures.
Footnotes
Acknowledgements
Thank you to Lama Aloreidi, Razan Alasiri, Shuaa Aleiaidi, and Samah Almutairi, students in the physical therapy program at KSU, who helped collect data.
Ethical approval
The Institutional Review Board of the College of Medicine, KSU, approved the study (IRB Log Number: E-22-7446).
Informed consent
At the beginning of the questionnaire, an overview of the research, its purpose, and expected completion time were clarified, along with the contact information for the principal investigator. By choosing to complete the questionnaire, participants provided their consent. Participants’ privacy and information were protected, and their names and other identifying information were not disclosed.
Author contribution
Dr Afaf Saheen and Dr Maha Algabbani contributed equally to this work through their involvement in the conception and design of the study; analysis and interpretation of the data; drafting of the manuscript; critical revision of the manuscript for important intellectual content; and final approval of the version to be published, with both authors agreeing to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data supporting the findings of this study are available upon reasonable request from the corresponding author.