
Abstract
Background
Work—family conflict is a significant challenge for nurses, as it affects both their personal and professional lives. A comprehensive understanding of the current situation and underlying determinants is essential to promote effective work—life balance.
Objective
The present study investigated work—family conflict and related factors among clinical nurses in Iran.
Methods
This cross-sectional study was conducted on 400 nurses from hospitals in Kashan, Iran, in 2023 via stratified random sampling. Data were collected using the Background Questionnaire, the Coping Strategies Questionnaire, and the Work-Family Conflict Questionnaire. Work—family conflict was rated on a scale of 9 to 45, with a 95% confidence level estimated for the target population. Data analysis was performed via SPSS version 22, employing independent t tests, Mann—Whitney U tests, one-way ANOVA, Kruskal—Wallis tests, correlation coefficients, and multiple linear regression.
Results
The work-family conflict score was 31.598 ± 6.831 (CLM95%: 30.928–32.268). A significant model explained 33.2% of the variance in work—family conflict identified by nine variables: use of coping strategies, willingness to leave the job, workload on the ward, being a native, satisfaction with performance of managers, satisfaction with physical health, job title, employment status, and type of work shift (F = 11.035, p < 0.0001). The variable with the greatest influence was “satisfaction with the performance of managers” (R2 = 0.087).
Conclusions
Work–family conflict is high among nurses in Kashan hospitals. To alleviate this conflict, it is important to improve communication, reduce workload, and provide training on effective coping strategies.
Introduction
Work–family conflict (WFC) is the negative interference between family and work roles. This conflict arises when the demands of these roles become incompatible. It often occurs when people are forced to play multiple roles simultaneously, e.g., as career professionals, spouses, and parents. 1 Achieving a satisfactory balance between these roles requires sufficient time, commitment, and energy. Therefore, people who find it difficult to balance work and family often experience disruption when work intrudes into their family life or vice versa. 2
Theoretically, WFC is rooted in role theory, which posits that conflict arises when individuals face incompatible expectations and demands from their multiple roles, such as those of employee and family member. Building on this, the conflict is often conceptualized in three primary forms, as operationalized in the instrument used in this study: time-based conflict (when time devoted to one role makes it difficult to participate in the other), strain-based conflict (when strain from one role, such as fatigue or stress, spills over and affects performance in the other), and behavior-based conflict (when specific behaviors required by one role are incompatible with behaviors expected in the other). 3 Furthermore, resource-based perspectives, such as the Job Demands-Resources (JDR) model and Conservation of Resources (COR) theory, suggest that WFC is exacerbated when job or personal resources (such as time, energy, and support) are depleted by one role, leaving insufficient resources to meet the demands of the other.4,5
Work–family conflict can be divided into family–work conflict and work–family conflict. Research suggests that work–family conflict is more common than family–work conflict is, indicating that work demands tend to have a greater impact on family responsibilities than do family demands on work commitments. 6 According to a literature review (2017), approximately 40% of employees in various fields report experiencing work–family conflict, with 20–25% reporting difficulties in balancing their family commitments. 7
Work–family conflict is widely recognized as a significant source of stress for employees and has been shown to have a negative effect on mental health, overall life satisfaction, and quality of working life. 8 In nursing, where job demands are inherently high, such conflicts are consistently linked to increased work stress, lower job satisfaction, and adverse health outcomes. These effects extend beyond the individual nurse and potentially affect the quality of patient care. If conflicts persist, they can lead to emotional exhaustion and burnout, which in turn are important predictors of lower performance, job disengagement, and increased turnover. In addition, higher absenteeism, lower organizational commitment, and lower productivity are frequently observed consequences of unresolved work–family conflict.9,10 The severity of these outcomes is often influenced by the nature and intensity of professional tasks, which are generally complex and emotionally stressful in healthcare. 11
Nurses often face conflicts between work and family responsibilities, which is a significant challenge. A study in India (2017) reported that 79.4% of nurses experience work—family conflict. 12 A survey in the United States (2016) revealed that 81% of prospective nurses reported such conflicts. 13 In addition, Sharifzadeh et al. (2014) estimated the level of work—family conflict among Iranian nurses to be 2.87 ± 0.62 on a scale of 1 to 5. 14 In further studies by Raesi et al. (2022) and Hesabi et al. (2015), the rates of work—family conflict in Iran were reported to be 32.7 ± 7.08 and 31.39 ± 7.69, respectively, on a scale of 9 to 45.10,15
Various factors can contribute to work—family conflict among nurses, including inadequate organizational support, varying work shifts, demanding tasks, and long working hours. 10 During the COVID-19 pandemic, nurses faced intense physical, mental, and psychological stress due to overwhelming work demands and concerns about compromising their own health and that of their family members. 16 This aligns with established theoretical frameworks: the Job Demands-Resources model suggests that excessive job demands can deplete available resources and lead to strain; 17 conservation of resources theory indicates that stress levels increase when valued resources, such as health and family safety, are threatened; 18 and the transactional model of stress and coping highlights that perceptions of threat in high-demand situations can trigger stress responses. 19 The high prevalence of job dissatisfaction and the desire to leave nursing during the COVID-19 pandemic highlight this problem.10,20 Accordingly, it can be assumed that nurses experienced increased work—family conflict during prolonged pandemics. This conflict can have both direct and indirect effects on personal and professional life, with implications for the individual, the family, and the organization. 21 The effects of work-family conflict include deterioration of physical and mental health, decreased performance, marital dissatisfaction, disruption of marital and parental roles, decreased life satisfaction, lower quality of personal and professional life, stress and dissatisfaction at work, decreased organizational commitment, increased absenteeism, irregular attendance at work, decreased productivity, and loss of skilled professionals.22,23 Accordingly, work—family conflicts can undermine the quality of care services provided, lead to client dissatisfaction, and jeopardize the health of care recipients. 10
Given the extensive and significant negative consequences of work—family conflict among nursing professionals, particularly in terms of its detrimental impact on the quality of community services, this issue is especially pressing in the nursing field. Policymakers and health managers should formulate and implement effective strategies to address work—family conflict in nursing, especially during the COVID-19 pandemic. In this context, it is important to assess the current situation and identify the influencing factors.
Numerous studies indicate a clear relationship between the severity of work—family conflict and various factors. For example, age, number of children,6,11,24 marital status, working rotating shifts, 15 intention to leave the job, 25 having an elderly or disabled person at home, 10 and working overtime or heavy workloads6,26 all show a positive and significant relationship with WFC. In contrast, work experience, 27 income level, 15 spouse involvement in household tasks, 10 support from colleagues, 26 and job satisfaction10,24 have significant inverse relationships. Based on the existing literature, this study identified directional associations: organizational and job-demand variables, such as heavy workload and intention to leave the job, are expected to have a positive relationship with WFC. In contrast, supportive factors, including job satisfaction and support from colleagues, are expected to have a negative association with WFC. However, the literature shows inconsistencies regarding the specific impact of several key variables. The influence of demographic factors on WFC is not straightforward. Some studies indicate that being female is linked to higher levels of WFC,24,27 while others suggest that being male may also be a risk factor.6,26 The effects of age and marital status also vary significantly across different cultural and occupational contexts. Family-related factors show similarly mixed results; for example, the presence of children is often identified as a predictor of WFC,6,11,26 but the specific influence of the age of the youngest child and the level of spousal support is not consistently defined.10,26 Additionally, the relationship between work-related factors and WFC, such as educational attainment and work experience, remains unclear. Even the type of employment, which is important for job security and stability, has shown no significant association with WFC in some contexts. 28
Given the complexity and evolving nature of nurses’ roles, particularly after the COVID-19 pandemic, identifying the key predictors of work—family conflict is crucial to promoting workforce well-being and sustainability. Considering the limited empirical evidence from hospitals in Kashan, existing discrepancies in the literature regarding influencing factors, and recent changes in clinical working conditions, this study aims to investigate work—family conflict and its related factors among nurses working in COVID-19 inpatient wards in Iran.
Hypotheses
Using role theory and conservation of resources perspectives, the following succinct, directional hypotheses were proposed regarding nurses’ WFC and its various dimensions:
Methods
Study type and design
This cross-sectional study was designed and reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 29
Participants
The sample size was calculated on the basis of the variable “Work-Family Conflict” from the study by Raesi et al. (2022), which reported a mean of 32.7 ± 3.08 using the WFC questionnaire. 15 The estimated sample size was determined via the table of Krejcie and Morgan (1970) and a precision of 0.1 standard deviations, resulting in a sample size of 400.
The inclusion criteria included at least one year of professional nursing experience, a university degree in nursing, and no known psychological disorders (based on self-reports). An exclusion criterion was withdrawal from the study during data collection or providing incomplete responses. Stratified random sampling (based on departments) was used from the clinical departments of seven hospitals in Kashan. This sampling procedure lasted approximately two months, from June to August 2023, after the acute COVID-19 pandemic phase from the participants. It should be noted that data collection scales assessed current levels of conflict, coping, and work conditions at the time of survey administration, not conditions during the pandemic.
Data collection
First, the necessary permissions were obtained from the hospital's dean and chief nursing officers. The clinical wards and nursing staff in each hospital are listed. On the basis of the sample size and the number of nurses in each department, eligible samples were selected via a simple random sampling method. The first author of the article (A.S.) visited the wards at the beginning of each shift in accordance with the nurses’ work schedules. At the end of each shift, the data collection scales were collected. If any of the data collection scales were incomplete within the given time frame, arrangements were made with the nurse regarding the timing of the collection. In addition, in cases of unavailability, lack of cooperation, or withdrawal of samples, another nurse from the same department was selected via a simple random method. Importantly, the samples completed the data collection scales via self-reports.
Data collection scales
The data collection scales included the Background Questionnaire (the possible factors of the work-family conflict), the Coping Strategies Questionnaire (CSQ), and the Work-Family Conflict Questionnaire (WFC).
The Background Questionnaire (the possible factors of the work-family conflict) consisted of three main sections: (1) Demographic characteristics (including age, gender, education level, nativity, place of residence, housing status, marital status, spouse's education level and occupation, spouse's participation in household tasks, number of children, age of youngest child, care of older adult or person with a disability at home, monthly family income, and support from relatives), (2) contextual work-related factors (including employment status, job title, department, type and predominance of work shift, frequency of overtime, workload on the ward, work experience in nursing, length of time working in the current department, work stress, job satisfaction, interest in the nursing profession, having a second job, willingness to leave the job, and professional indemnity insurance), and (3) psychological and behavioral indicators (including regular sporting activities, leisure time for recreation and outings, experiencing major stress in the past six months, participation in stress management courses, and satisfaction with physical and mental health, satisfaction with salary, and social and entertainment facilities, communication of patients and their families, and the performance of doctors, colleagues, and managers).
This researcher-developed questionnaire does not directly measure WFC; instead, it aims to capture background variables identified in the literature as potential correlates of WFC. A narrative scoping review was conducted on studies examining the predictors or correlates of WFC among nurses and allied health professionals over the past two decades. The search terms encompassed various concepts related to the population (such as nurses and health personnel), exposure (such as shift work and workload), and context (such as marital status and parenting). The analysis incorporated observational studies, systematic reviews, and guidelines that reported associations with WFC. Candidate variables were extracted and harmonized into a comprehensive item pool, providing a solid foundation for the questionnaire. An expert panel of ten faculty members with expertise in the relevant field reviewed the items for relevance, clarity, and redundancy. Based on their feedback, overlapping workload items were consolidated, and the wording was simplified, thereby confirming the content validity of the questionnaire. The reliability of the questionnaire was assessed via a test—retest method in which 10 nurses participated over one week. The consistency of response rate was 95%. In addition, “use of coping strategies” was included in the analysis as a potentially significant factor, complementing the 43 other variables included in the study.
The Coping Strategies Questionnaire (CSQ) was developed by Folkman and Lazarus in 1988. This questionnaire consists of 66 items and includes two subscales, each rated on a 4-point Likert scale. It assesses coping strategies on a scale from 0 to 198, with higher scores indicating stronger coping strategies. The construct validity of the CSQ was confirmed, and the internal consistency for the problem-focused and emotion-focused subscales was assessed, with Cronbach's alpha coefficients of 0.66 and 0.79, respectively. Alipour et al. (2010) confirmed the validity of the Persian version of the CSQ, with a reliability coefficient of 0.89. 30 Mahmoudirad et al. (2018) estimated this reliability coefficient to be 0.82. 31 In the present study, the Cronbach's alpha coefficient was 0.936.
The work–family conflict (WFC) questionnaire was developed in 2000 by Carlson et al. The WFC comprises 18 questions, which are divided into two dimensions: work interference with family (WIF) and family interference with work (FIW), with each dimension consisting of nine items. Each dimension also assesses three aspects, time, strain, and behavior, with three items assigned to each aspect. The participants responded to all the items on a 5-point Likert scale ranging from “strongly disagree” to “strongly agree”, with higher scores indicating greater conflict. The reliability coefficients for WIF and FIW are reported as 0.76 and 0.89, respectively. 32 For the present study, only the WIF dimension was used, resulting in a scale that assesses work—family conflict, with scores ranging from 9 to 45; higher scores indicate greater conflict. The translation and psychometric evaluation of the Persian version of the WFC was conducted by Hesabi et al. (2015), who confirmed content validity and reported a Cronbach's alpha coefficient of 0.77. 10 In this study, the Cronbach's alpha coefficients for the overall WIF and its dimensions (time, strain, and behavior) were estimated to be 0.884, 0.889, 0.800, and 0.784, respectively.
Ethical considerations
This study was approved by the scientific committee (Proposal No. 402050, dated June 13, 2023) and the ethics committee (Ethics Code IR.KAUMS.MEDNT.REC.1402.084, dated July 16, 2023) of Kashan University of Medical Sciences. Both verbal and written informed consent were obtained from all the participating nurses. Additionally, all participants were informed in detail about the study's purpose, the confidentiality of their data, and their right to withdraw from participation at any time.
Statistical analysis
The data were analyzed via SPSS version 22. Work—family conflict was measured on a scale from 9 to 45, with an estimated interval at the 95% confidence level for the target population. Skewness and kurtosis were used to assess the data distribution, with a range of ±2 being considered indicative of normality. A stepwise multiple linear regression analysis was performed to prioritize the dimensions of the questionnaire. This process aimed to determine the contributions of the dimensions of time, strain, and behavior to the overall work-family conflict score. The related factors were analyzed in two stages to determine the critical factors. Hypotheses were examined using univariable tests and stepwise multiple linear regression for the total WFC score and for each dimension (time, strain, behavior), with two-sided. All analyses were based on a significance level of less than 0.05.
In the first stage, each factor was analyzed separately via univariate tests. Independent t tests (and Mann—Whitney U tests for nonnormal data) were used to assess the relationships between work—family conflict and possible binary factors, such as gender. One-way analysis of variance (and the Kruskal—Wallis test for nonnormal data) was used to categorize possibly related factors, such as housing status. The Pearson correlation coefficient (and Spearman-Brown correlation coefficient for nonnormal data) was calculated for quantitatively related factors.
In the second stage, a stepwise multiple linear regression analysis was performed to identify the potential related factors and to assess the significance of each factor in explaining variations in work-family conflict scores. In this stage, the variables identified in the univariate analysis with a significance level of less than 0.2 were considered independent variables. The work-family conflict score was also included in the model as a dependent variable.
Results
The results are structured to align with the study's objective of identifying factors related to WFC. It presents descriptive findings, followed by tests of H1–H4 for total WFC and for each dimension. The first section details the characteristics of the sample, followed by a presentation of WFC scores. This is succeeded by univariable and multiple analyses of total conflict and its dimensions, with predictor factors clearly identified.
A total of 440 nurses were evaluated. Of these, 400 nurses participated in the study and completed the data collection instruments. Consequently, data from 400 samples were analyzed. The average age of the nurses was 35.07 years, with a standard deviation of 8.11 years. The nursing job experience, number of hours spent per month, and number of children among the samples were 10.45 ± 7.26 years, 60.18 ± 47.53 h, and 1.03 ± 1.11, respectively. Interest in nursing was measured as 7.12 ± 2.67 on a scale of 0 to 10. Among the respondents, 77% were female, and 23% were married (Table 1).
Work—family conflict score based on individual and occupational variables among Iranian nurses, Kashan, 2023 (n = 400).
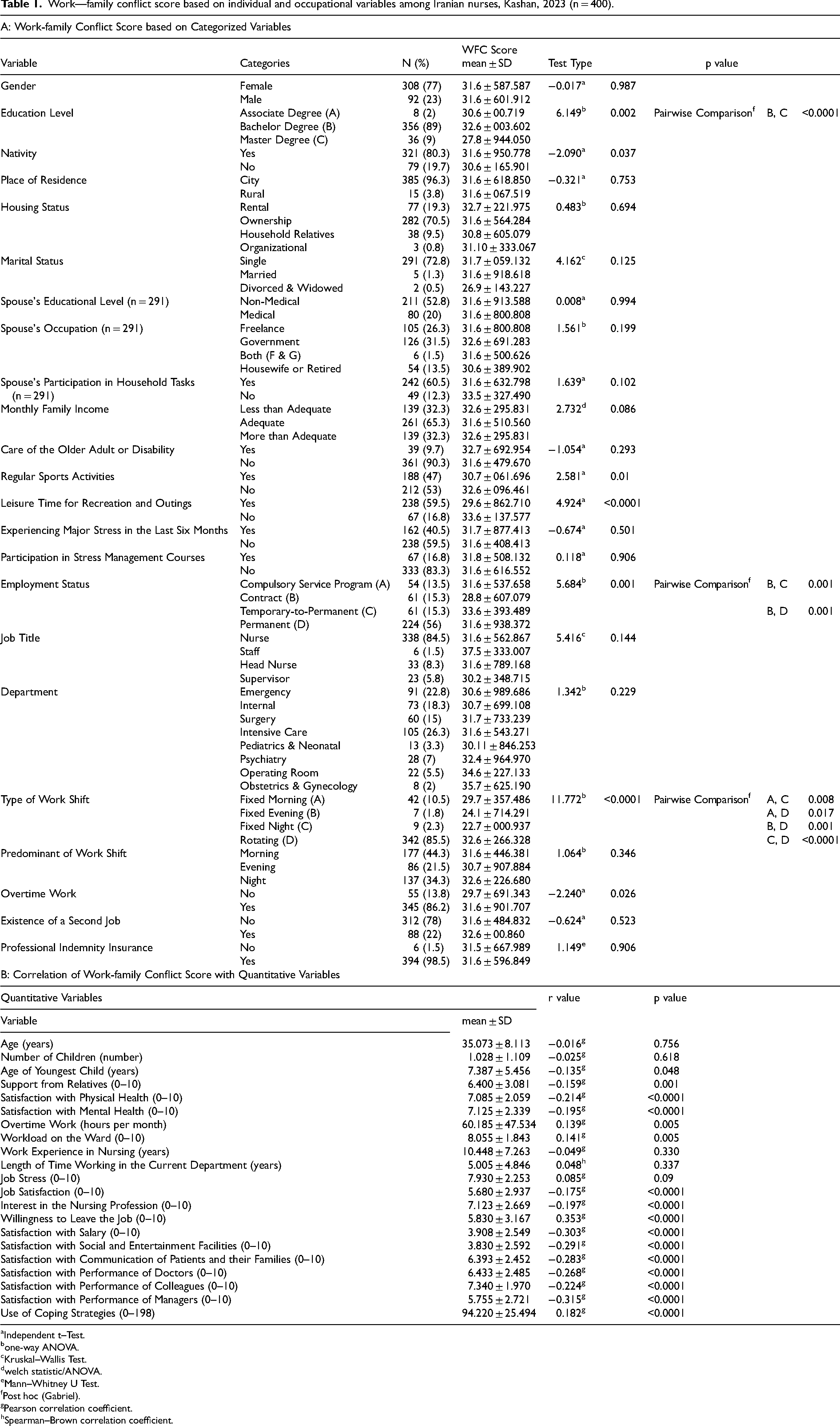
Independent t–Test.
one-way ANOVA.
Kruskal–Wallis Test.
welch statistic/ANOVA.
Mann–Whitney U Test.
Post hoc (Gabriel).
Pearson correlation coefficient.
Spearman–Brown correlation coefficient.
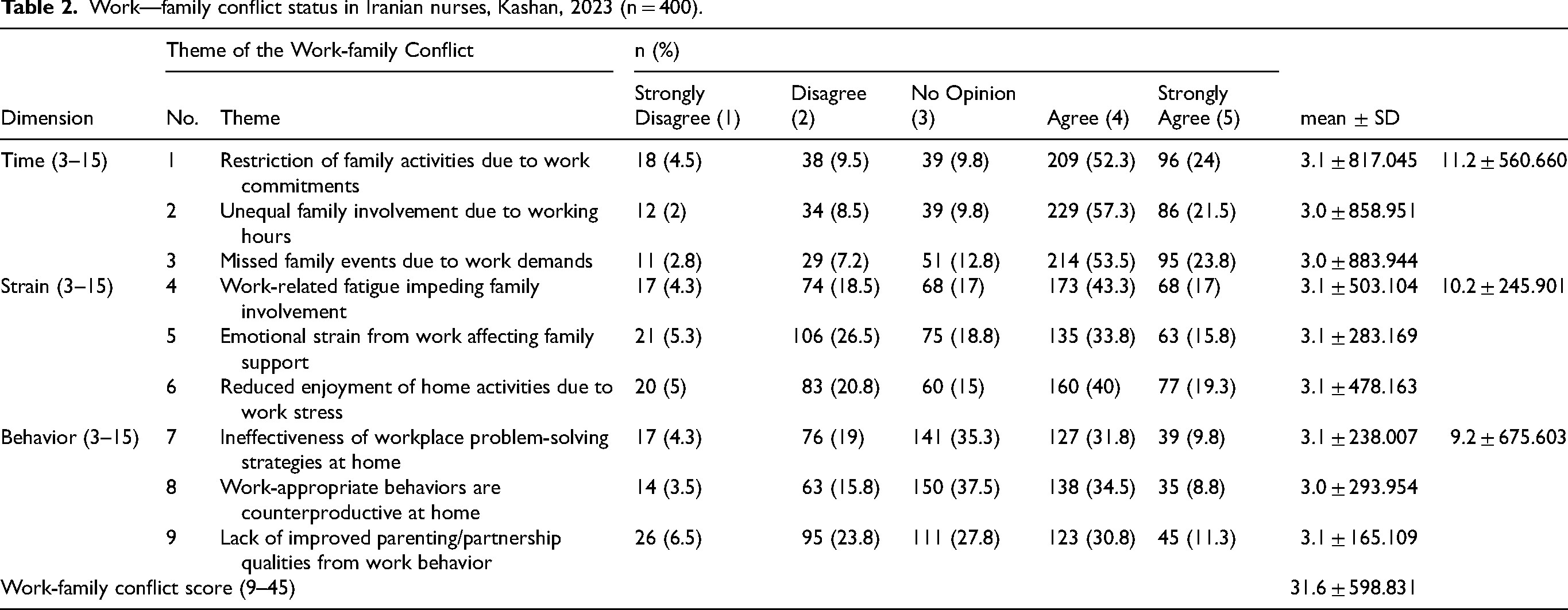
The work—family conflict score for nurses was 31.60 ± 6.83 (on a scale of 9 to 45), with a 95% confidence interval calculated for the population between 30.93 and 32.27 (Table 2). Multiple linear regression analysis revealed that the components of strain, behavior, and time accounted for 98.1% of the variance in the work—family conflict score, with corresponding contributions of 74.9%, 13.9%, and 9.3%, respectively (F = 6854.78, p < 0.0001).
Work—family conflict status in Iranian nurses, Kashan, 2023 (n = 400).
The univariate analysis revealed a significant correlation between the work—family conflict score and several variables, including education level, nativity, age of youngest child, support from relatives, regular sports activities, leisure time for recreation and outings, experience of major stress in the past six months, satisfaction with physical and mental health, employment status, work shift type, occurrence of overtime work, ward workload, job satisfaction, interest in the nursing profession, intent to leave the job, salary satisfaction, satisfaction with social and entertainment facilities, satisfaction with communication among patients and their families, satisfaction with the performance of doctors, colleagues, and managers, and using of coping strategies (p < 0.05) (Table 1 and Table 2).
A multiple linear regression analysis using the stepwise technique was performed to assess the associations between the independent factors and the work-family conflict score. The results showed that the simultaneous inclusion of nine variables related to work–family conflict in the model was statistically significant (F = 11.03, p < 0.0001). The variables of using coping strategies (β = 0.23), willingness to leave the job (β = 0.18), ward workload (β = 0.17), and nativity (β = 0.15) significantly correlate with increased levels of work-family conflict. Contract nurses (β = −0.14) who work rotating shifts (β = 0.24) experienced higher levels of work–family conflict. There is a negative correlation between satisfaction with managerial performance (β = −0.15) and satisfaction with physical health (β = −0.21) and work-family conflict. Multiple linear regression analysis revealed that these nine variables accounted for 33.2% of the variance in the work–family conflict score. The most significant contribution is attributed to “satisfaction with the performance of managers” (R2 = 0.087) (Table 3).
Multiple linear regression of factors associated with work–family conflict (n = 400).
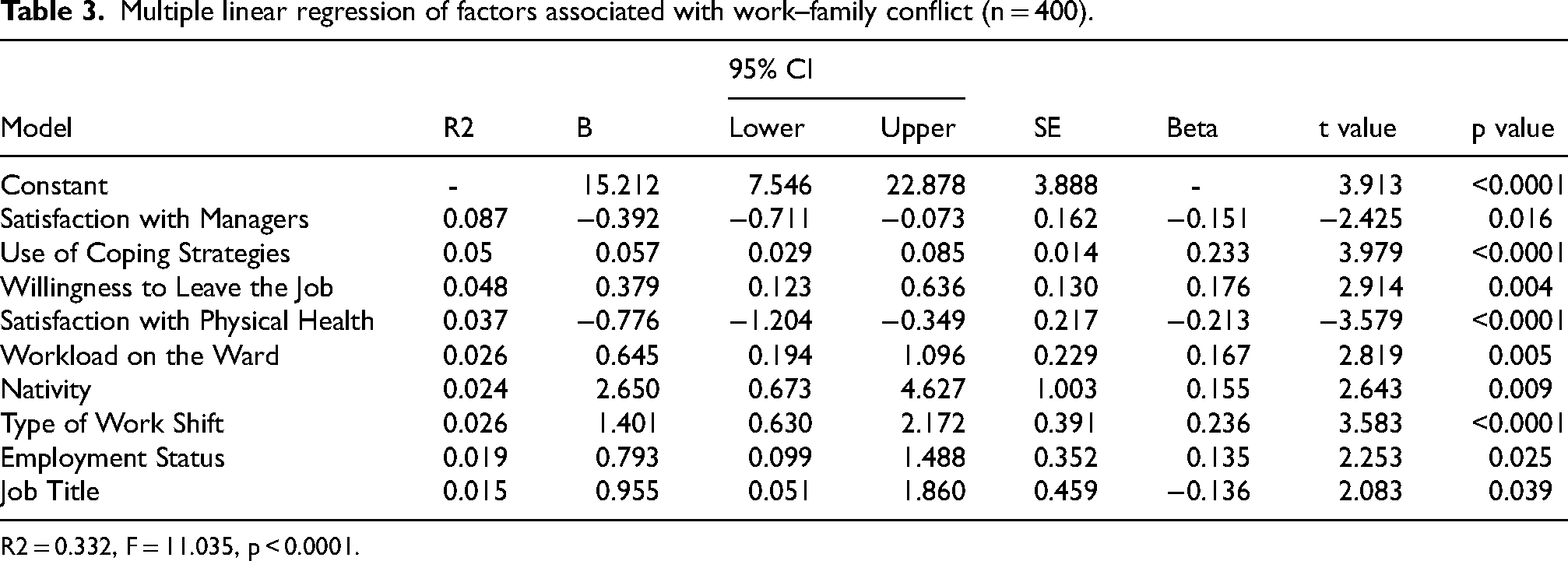
R2 = 0.332, F = 11.035, p < 0.0001.
The multiple linear regression model revealed that the simultaneous presence of seven factors in the factor model was significantly associated with the strain dimension of work—family conflict among nurses. There was a significant positive relationship between the use of coping strategies (β = 0.22), workload in the ward (β = 0.23), nativity (β = 0.15), and the outcome of the work-family conflict strain dimension score. Satisfaction with managerial performance (β = −0.25), satisfaction with physical health (β = −0.17), and monthly family income (β = 0.13) are strongly inversely correlated with the work-family conflict strain dimension score. Contractual employment status (β = 0.146) was correlated with an increased score on the work-family conflict strain dimension (F = 9.89, p < 0.0001). The results show that these seven variables account for 25.5% of the variance in the work–family conflict strain dimension score. The most significant influence is attributed to “satisfaction with the performance of managers” (R2 = 0.083) (Table 4).
Multiple linear regression of factors associated with the strain dimension of work–family conflict (n = 400).
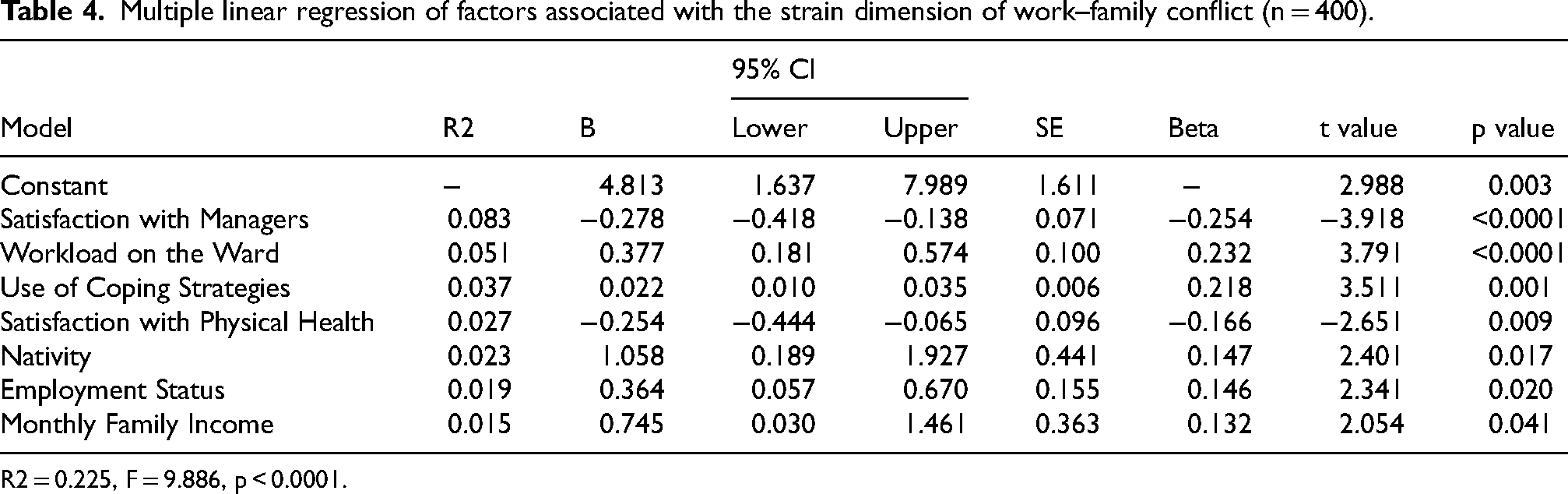
R2 = 0.225, F = 9.886, p < 0.0001.
The multiple linear regression model revealed that eight different factors were significantly related to the time dimension of work-family conflict among nurses. The results show a significant positive correlation between the use of coping strategies (β = 0.18) and willingness to leave the job (β = 0.22), as measured by the time dimension of work–family conflict. Satisfaction with social and entertainment facilities (β = −0.12), mental health (β = −0.15), regular participation in sports activities (β = −0.13), and monthly family income (β = 0.13) are inversely correlated with the time dimension of work-family conflict. In addition, contractual employment (β = 0.17) and rotating work shifts (β = 0.26) are positively correlated with increased values of the time dimension of the work-family conflict score (F = 9.07, p < 0.0001). The results show that these eight variables account for 26.5% of the variance in the time dimension of work-family conflict score. The largest contribution is attributed to the “type of work shift” (R2 = 0.084) (Table 5).
Multiple linear regression of factors associated with the time dimension of work–family conflict (n = 400).
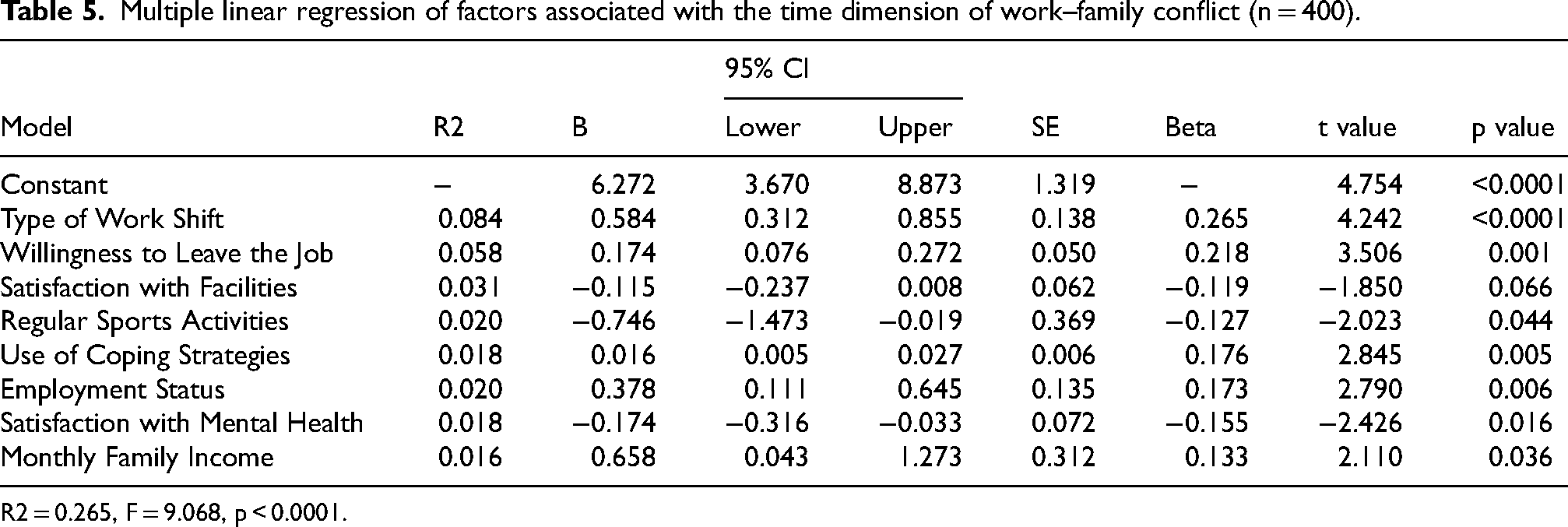
R2 = 0.265, F = 9.068, p < 0.0001.
The multiple linear regression model revealed that the simultaneous inclusion of four variables in the model was significant in relation to the characteristics associated with the behavioral dimension of work-family conflict among nurses. The variables related to the use of coping strategies (β = 0.14) and willingness to leave the job (β = 0.15) showed a strong positive correlation with the score for the behavioral dimension of work-family conflict. In addition, satisfaction with patients and their families (β = −0.17) and satisfaction with social and entertainment facilities (β = −0.19) were correlated with a lower score in the behavioral dimension of work-family conflict (F = 15.91, p < 0.0001). The results indicate that these four variables account for 13.9% of the variance in assessing the work-family conflict behavior dimension. The most significant contribution is accounted for by “satisfaction with social and entertainment facilities” (R2 = 0.054) (Table 6).
Multiple linear regression of factors associated with the behavior dimension of work–family conflict (n = 400).
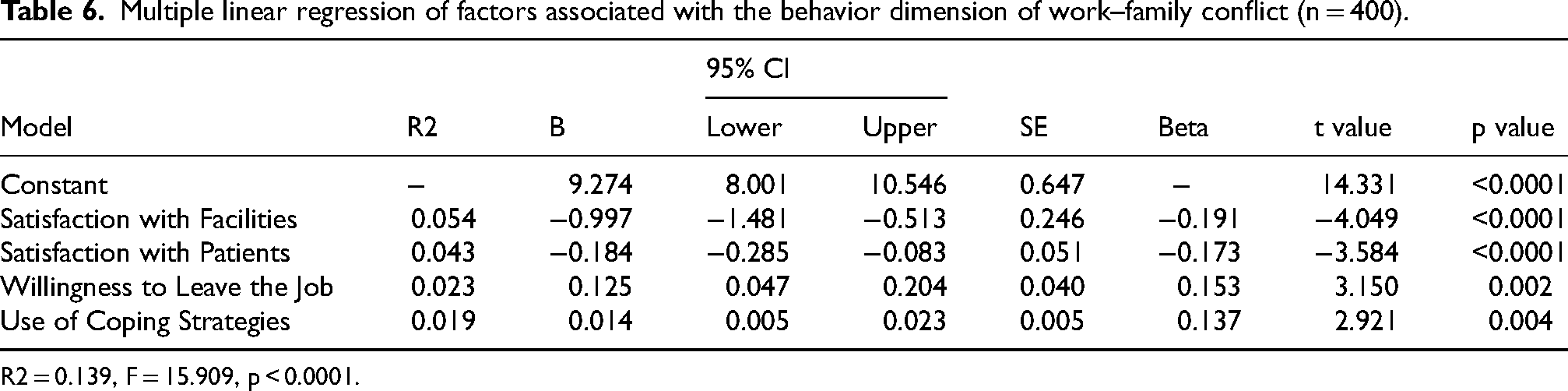
R2 = 0.139, F = 15.909, p < 0.0001.
Discussion
The present study aimed to investigate work—family conflict and related factors among Iranian nurses. This discussion interprets the key findings in relation to the study's objectives and existing literature. It begins by summarizing the main results and situates these findings within the context of relevant research. Additionally, it emphasizes their implications for both practice and policy, recognizes any limitations, and proposes avenues for future research. Finally, the discussion concludes with a concise summary that ties back to the results. These findings support H1 and H2 for the strain dimension and partially support H3–H4
Summary of key findings
The results of this study revealed high levels of work—family conflict among nurses working in COVID-19 inpatient wards. Because data were collected in June-August 2023 (post-pandemic), our findings reflect the post-pandemic landscape; therfore, results can be denote contextual interpretation of prior exposures than our data-collection window. The results is consistent with the findings of Raesi et al. (2021), 15 who reported similar stress patterns during the pandemic. In contrast, a prepandemic study conducted in Tehran in 2018 came to different conclusions, highlighting how the pandemic has exacerbated work—family conflict and its long-term effects on nursing staff. 28 The demands of professional responsibilities during this period, including extended working hours and increased clinical pressure, are likely to have limited nurses’ ability to fulfill their family responsibilities. In addition, the limited availability of supportive resources and ineffective coping strategies further exacerbated the conflict. In the current study, workload, coping strategies, and satisfaction with management performance were found to be significant predictors of work–family conflict, highlighting the interplay between organizational stressors and individual psychological responses. 15 These findings are consistent with the broader literature, highlighting the role of the pandemic in exacerbating role overlap and disrupting work—family balance for healthcare professionals. 2
Dimension-Specific insights: time, strain, and behavior
The present study suggests that the strain dimension has a significant effect on work—family conflict among nurses, who tend to experience strain more than the time and behavioral dimensions do. This finding is consistent with previous research in Iran 33 and aligns with recent global studies conducted during the COVID-19 pandemic in Turkey 34 and China. 35 In contrast, a study among Iranian nurses (2013) reported that the time dimension was rated higher than strain. 36 In contrast, Hassanzadeh et al. (2021) reported that strain had the lowest mean score before the pandemic. 37 After the COVID-19 pandemic, the strain dimension increased significantly, probably due to extended working hours, irregular work schedules, and mandatory working hours over time in Iranian hospitals. Nurses, therefore, often experience both time-based and behavior-based conflicts, even in noncritical situations. Strain conflicts arise when work-related stress interferes with family life, especially during traumatic events and crises. 38 Some psychological factors can exacerbate this conflict, including fear of contagion and the physical and psychological challenges resulting from the COVID-19 crisis. 39 These findings are therefore consistent with those of previous studies.
Predictors of WFC: univariable analyses
The results of the present study suggest that several factors contribute to greater work—family conflict among nurses, including coping strategies, willingness to leave the job, ward workload, and being a native. Conversely, satisfaction with the performance of managers and satisfaction with physical health were associated with lower levels of work-family conflict. In addition, nurses working rotational, early, and staff shifts reported more work—family conflict, whereas those employed on a contract basis experienced less conflict. Several factors contribute to the challenges nurses face in balancing work and family, including heavy workload, fixed morning shifts, irregular working hours, higher expectations placed on native nurses, limited monthly working hours for contracted nurses, and the reciprocal relationship between job dissatisfaction and the intention to leave the job. 40 Satisfaction with the performance of managers is the strongest predictor of work-family conflict, highlighting the importance of a supportive organizational culture in addressing these challenges. 41
Previous studies have shown varying results regarding the factors contributing to work—family conflict among nurses. Hesabi et al. (2015) identified several predictors, including having a second job, caring for older or disabled children, and interest in nursing, after accounting for other confounding variables. 10 Conversely, Lembrechts et al. (2015) reported that working overtime and having a heavy workload increased the level of work-family conflict. 26 AlAzzam et al. (2017) reported that younger age, more children, and lower job satisfaction were associated with higher levels of conflict in Jordan. 24 Labrague et al. (2021) reported that factors such as age, education level, hospital capacity and location, stress level, turnover intentions, job satisfaction, and quality of care influenced work—family conflict. Conversely, years of nursing experience and organizational tenure were found to have a significant negative correlation with work-family conflict. 11 Wu et al. (2021) reported that Chinese nurses in emergency care, especially those aged 25–34 years, men, married, those with a university degree, professionals with long work experience, and those who perceive a shortage of nurses or who work night shifts, experience greater levels of conflict. 6
Some studies have investigated the relationship between coping strategies and work-family conflict, emphasizing the moderating role of coping strategies.42,43 In the present study, several factors were identified as having a significant effect on work—family conflict in nurses, particularly work stress and coping strategies. Effective coping strategies can mitigate the negative effects of personal and professional stressors, thereby supporting nurses’ mental health. 34 Contrary to initial expectations, the present study revealed a direct effect of coping strategies on work–family conflict, which was evident in all dimensions of conflict. The unique challenges of the COVID-19 pandemic likely exacerbated the extent of conflict, such as increased workload and stress, fear of transmitting the infection to family members, extensive restrictions on social interactions and leisure activities, and physical and psychological consequences. 44 Although the nurses used moderate coping strategies to address stress, they relied predominantly on emotion-focused strategies during times of crisis, 45 so the amount and type of coping strategies used were probably inadequate. When interpreting these results, it is important to consider the cross-sectional nature of the study and the simultaneous completion of the data collection scales.
Predictors of WFC: multiple models
Multiple regression analysis revealed that the variables related to the extent of use of coping strategies, workload on the ward, and being a native were positively and significantly correlated with the strain dimension of work-family conflict. Conversely, there is a negative correlation between work-family conflict scores and satisfaction with the performance of managers, satisfaction with physical health, and monthly family income. Additionally, employment status is a predictor of work—family conflict; nurses with an employment contract report lower levels of conflict than do those in other employment categories. The strongest predictor of the work-family conflict strain dimension was satisfaction with performance. The results of the present study are consistent with those of Ahmadyan et al. (2016), who reported a negative correlation between work-family conflict and physical and mental health. 46 There is a bidirectional relationship between physical and mental health and work-family conflict. Poor health can exacerbate conflict, while such conflict can further impair health due to increased stress and burnout. 47
Multiple regression analysis revealed that the type of shift has a significant effect on the time dimension score of work–family conflict. There is also a direct correlation between the variables of the extent of use of coping strategies and the willingness to leave the job, as well as work-family conflict. Conversely, the time dimension of work-family conflict is negatively correlated with leisure time for recreation and outings, satisfaction with mental health, regular sports activities, and monthly family income. In addition, employment status and type of work shift were identified as predictors of this dimension of conflict among nurses. Some studies conducted in Iran have shown that the highest mean scores for work-family conflict are associated with the time dimension, especially shift work. 37 In Iranian society, many people exceed typical working hours to support themselves, which over time increases the level of conflict available for family matters. 48 While all dimensions of work—family conflict were less prevalent among contract nurses in the present study, other studies have shown that part-time employment may not be a viable solution to reduce the conflict between these two spheres of life. 26 This conflict appears to be due to inadequate income from part-time employment and the tendency to take on second and third jobs.
The present study revealed a direct correlation between coping strategies and the willingness to leave the job, specifically in terms of work-family conflict behavior. Conversely, satisfaction with communication between patients and their families, as well as leisure time for recreation and outings, showed an inverse correlation with the assessment of the behavioral dimension. Notably, leisure time for recreation and outings made the greatest contribution to the conflict behavior scores. Behavior-based work—family conflict can arise from the imbalance between work and family roles, as well as the demands and conditions in both domains. The expectation that nurses demonstrate selfless behavior and be available at all times at work may clash with their obligations to be present and engaged in family life. 38 Jung and Sohn (2022) reported that employees with heightened expectations of their work role may experience conflicts between work and family. 49 In addition, negative interactions with patients and their families can increase pressure on nurses and lead to increased conflict. 33 ]. Participation in leisure activities can effectively reduce stress and help alleviate work-family conflict. 50
Theoretical integration and putative mechanisms
The findings of the present study are consistent with theoretical perspectives on work—family conflict, including role theory, resource conservation theory, and social exchange theory. 23 With respect to the differences between the findings of the present study and those of similar studies, factors such as the timing and location of the study, the characteristics of the target population, the prevailing workplace structure and organizational culture, and the statistical analysis methods used should be considered. These findings enhance and extend the literature by demonstrating the interplay among managerial performance, the intention to leave the job, and workload in a resource-constrained postpandemic healthcare system. In contrast to studies conducted in higher-income countries, our findings emphasize the importance of contextual strain in determining the intensity of conflict. This offers a new perspective on the discussion of occupational stress and the work—family interface in global health settings.
Strengths and limitations
Although this study has several limitations, it is important to consider these limitations within the broader context of its methodological and practical contributions. Notable strengths of the study include a sampling approach stratified by department, adequate sample size, examination of multiple relevant factors, and the use of robust statistical analysis. Each of these elements increases the internal validity of the results and their relevance to nursing in Kashan hospitals. However, the generalizability of the study is limited because it relies on a random sample from a single city and uses a cross-sectional design, which limits the possibility of causal inferences. In addition, the timing of data collection, which occurred shortly after the COVID-19 pandemic, may have exacerbated work—family conflict due to exceptional stressors, including increased patient load, staff shortages, and heightened psychological strain. While these contextual factors may limit the generalizability of the results, they also reflect the real-life experiences of nurses during a crucial transition period in healthcare. To build on these findings, future research should be conducted in more stable postpandemic settings via longitudinal or intervention studies. In addition, qualitative research, particularly grounded theory approaches, could provide deeper insights into the complex and evolving nature of work—family conflict among nurses, facilitating targeted management interventions.
Conclusion
In this post-pandemic study of Iranian nurses, overall WFC remained notably high, with the strain dimension having the most significant impact on the total score's variability. In adjusted multiple models, higher ward workload and greater reliance on coping strategies were positively correlated with increased WFC. Conversely, greater satisfaction with managerial performance and better self-rated physical health were inversely related to WFC. These findings highlight a range of modifiable organizational and individual factors that contribute to WFC in resource-constrained hospital environments in the post-pandemic context.
Based on these findings, prioritizing the mitigation of ward workload in high-burden units, enhancing managerial performance and supportive supervision, and optimizing shift design are crucial organizational strategies. At the individual level, initiatives that promote more effective, problem-focused coping could help reduce work-family conflict, particularly where emotion-focused strategies are prevalent. These recommendations are intended as testable, context-specific quality improvement directions rather than definitive causal prescriptions, in line with the study's cross-sectional design.
Finally, while the findings are closely associated with the data and analyses presented, further longitudinal or intervention studies are needed to assess the causal effects of reducing workload, enhancing managerial support, revising shift structures, and strengthening coping skills on WFC and related outcomes. It is important to note that when variables showed non-significant or contradictory relationships in the adjusted analyses, this study deliberately did not suggest interventions; instead, it identified these areas as priorities for future research.
Supplemental Material
sj-docx-1-wor-10.1177_10519815251411291 - Supplemental material for Exploring work-family conflict and its determinants among nurses: A cross-sectional study in Iran
Supplemental material, sj-docx-1-wor-10.1177_10519815251411291 for Exploring work-family conflict and its determinants among nurses: A cross-sectional study in Iran by Ali Sarvarian, Zahra Tagharrobi, Khadijeh Sharifi, Zahra Sooki and Mohammad Zare in WORK
Footnotes
List of abbreviations
Acknowledgements
The authors would like to thank all the nurses who participated in the study and the Vice Chancellor for Research and Technology at Kashan University of Medical Sciences, Kashan, Iran.
Ethical approval
This study was approved by the Ethics Committee of Kashan University of Medical Sciences (Ethics Code IR.KAUMS.MEDNT.REC.1402.084, dated July 16, 2023).
Informed consent
Both verbal and written informed consent were obtained from all the participating nurses. In addition, all the participants were informed in detail about the purpose of the study, the confidentiality of their data, and their right to withdraw from participation at any time.
Author contributions
AS designed the study, collected the data, and wrote the initial draft of the article. ZT, KS, and ZS designed the study, analyzed and interpreted the data, revised the major draft of the article, and supervised the study. MZ analyzed and interpreted the data and revised the major draft of the article. All authors reviewed the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article was part of the first author's master's thesis in psychiatric nursing at Kashan University of Medical Sciences, Kashan, Iran. This thesis was financially supported by the Vice Chancellor for Research and Technology of Kashan University of Medical Sciences (Proposal No. 402050, dated June 13, 2023).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.