
Abstract
Background
The Royal Navy (RN) have recently introduced a new Physical Employment Standard (PES) based upon the most critical and physically demanding seafaring tasks.
Objective
This study quantified changes in RN trainee physical fitness during Initial Naval Training (INT) and assessed associations with the RN PES to inform the development of a pre-joining fitness test.
Methods
91 (6 F) participants completed the Chester Step Test (CST), seated medicine ball throw (SMBT), isometric mid-thigh pull (IMTP), counter movement jump (CMJ) and handgrip strength (HS) assessments at the start of both INT (Session-1) and Phase-2 (Session-2) training. During Session-2, participants also completed a Multi-Stage Fitness Test (MSFT). Participants also undertook the RN PES during Phase-2 training (Session-3). Physical fitness was compared between Session-1 and Session-2 by Paired Samples t-tests. Associations between fitness tests and RN PES performance were calculated by Pearson's correlation coefficients (r).
Results
Upper body power, lower body power, and strength increased between measurement points. However, aerobic fitness decreased. The size of correlations between physical fitness tests and RN PES test performance ranged between small (MSFT and Casualty Drag) to large (SMBT and Hand-Over-Hand Haul). Generally, muscular strength and power measures had a greater association (r = −0.221 to −0.699) with RN task performance (RN PES) than the aerobic capacity measures (r = −0.089 to −0.382).
Conclusion
These data reinforce the importance of absolute strength in critical RN task performance and will inform RN pre-joining fitness requirements.
Keywords
Introduction
Initial military training develops military skills, teamwork, basic fitness, and the core values required to be on the pathway for a successful military career. In the Royal Navy (RN), ordinary ranks are required to complete 10 weeks of Initial Naval Training (INT) ahead of moving to trade-specific training. Whilst previous literature has documented the changes in fitness during British Army and Royal Air Force (RAF) Basic Training, 1 no published data exist on the physical development of RN recruits during INT.
Previous UK military research has evidenced significant improvements in physical fitness during initial training, particularly for aerobic endurance.1,2 However, the current evidence base indicates gains in muscular strength and power are often more variable, and are impacted by initial fitness levels, training content, and programme duration. Most notably, recruits entering with lower baselines fitness typically demonstrate the greatest relative improvements, whilst those with higher initial fitness may experience limited or even negative adaptation due to an insufficient training stimulus.3,4 These observations are likely due to the delivery approach of physical training sessions within initial military training and the requirement for large groups of recruits to complete training together. This limits progressive overload for fitter recruits but also risks excessive overload for less fit recruits.
Pre-joining fitness tests (PJFT) prior to military training are often used to screen for minimum physical standards. 5 Subsequently, such tests can support training safety and contribute to the mitigation of musculoskeletal injury (MSKI) risk, provide a means to reduce the variability of recruits’ fitness when entering training, incentivise physical preparation prior to entry and reinforces physical fitness as a core value.6,7
The RN recently introduced new in-service Physical Employment Standards (PES) to better evaluate the physical capabilities required for (shipboard) operational naval tasks completed during a reasonable ‘worst-case’ scenario. The RN PES encompasses the physical demands of firefighting, casualty handling and emergency responses. Importantly, the RN PES now requires individual's to demonstrate their ability to complete a variety of manual handling tasks, the demands of which are likely to be different to that of the previous test (running focussed); this shift in focus has implications on both recruit training and selection. Thus, it is important for the PJFT to assess the physical capabilities of recruits entering service on job-relevant components of fitness. The current RN PJFT requires individuals to complete a 2.4 km run to a minimum standard, therefore there is a mismatch with pre-joining and in-service physical requirements, demonstrating the requirement to develop a more relevant testing regimen.
In recent years, several international armed forces have adopted or revised PJFT to better align entry standards with the physical demands of military training and occupational tasks. Notably, in 2019 the British Army implemented a new PJFT comprising the 2 km run, seated medicine ball throw (SMBT), and isometric mid-thigh pull (IMTP). These provide a more thorough assessment of an individual's physical capability and better reflects occupational demands. Therefore, the aims of this study were to quantify the changes in fitness during RN INT and assess associations with RN task performance to inform the development of a new PJFT.
Methods
Overview
A sample of 91 (6 female) RN recruits volunteered to participate in the study. Participants were given a verbal and written brief prior to providing their consent. As all recruits must pass an initial medical on arrival to RN Initial Training, all participants were deemed fit to take part in the testing regimen. The study was approved by the Ministry of Defence Research Ethics Committee (2252/MODREC/23).
Participants completed three testing sessions: Session-1 (at the beginning of INT), Session-2 (at the beginning of ‘Phase 2’ Trade Training, and Session-3 (during ‘Phase 2’ Trade Training. There were approximately 11 weeks between Session-1 and Session-2, with one more week between Session-2 and 3. Briefly, INT aims to transform civilians into physically and mentally resilient members of the Royal Navy, whereas Trade Training prepares sailors for their specific trade, branch, or warfare role. All participants followed their normal Initial Military Fitness (IMF) programme, led by Physical Training Instructors, between testing sessions. Specifically, IMF is completed at least three times a week and consists of group-based running activities and military circuit training, aiming to test and develop core physical skills and ability to follow commands when physically exhausted. Examples of circuit training exercises include sprinting, push ups, squats, burpees, and rope climbs.
Procedures
Physical fitness (session 1 and 2)
Participants stature, body mass, and waist circumference was measured using standard procedures. 8 Following this, participants were required to complete the SMBT, IMTP, CMJ, and Handgrip assessments in a randomised order. All assessments were completed in physical training attire (t shirt, shorts, trainers). During Session-1, participants were also required to complete the Chester Step Test (CST) to enable the estimation of maximal aerobic capacity; the CST was chosen due to RN policy at the time of testing which precluded maximal testing within the first five weeks of INT. During Session-2, participants completed both the CST and Multi-Stage Fitness Test (MSFT) (to best effort) to enable comparison between estimates of maximal aerobic capacity. Specific test procedures are detailed below.
Seated medicine ball throw
The SMBT was conducted using a 4 kg medicine ball (Origin Fitness, UK). Participants were instructed to sit against a wall with their legs placed together and straight out in front of them. Participants were instructed to throw the ball at 45° from their chest (elbows down) as far as possible. 1 Following one familiarisation attempt at ∼50% max effort, participants completed two maximal efforts separated by at least 30 s. The furthest distance achieved was recorded.
Isometric mid-thigh pull
Participants were required to perform an IMTP assessment using a bespoke rig with a dynamometer (Takei Isometric Dynamometer, Model 5402, Cranlea). Participants were asked to stand on the rig, feet shoulder-width apart with their knees flexed. The bar height was modified for each individual to acquire a hip angle between 140–150° and a knee angle between 120–135°. 9 Using a double overhand grip, with straight arms and maintaining a straight back, participants were asked to perform a maximal pull for ∼5 s to achieve a peak force.10,11 Following one familiarisation attempt at ∼50% max effort, participants completed two maximal efforts separated by at least 30 s. The highest peak force (converted to kg) was recorded.
Counter movement jump
Participants completed the CMJ from a standing position using the Just Jump mat (Probotics, USA). Participants were instructed to stand with their feet shoulder width apart with their hands placed on their hips. Upon the researchers’ instruction, participants were required to perform a maximal jump without ‘tucking’ their legs. 11 Following one familiarisation attempt at ∼50% max effort, participants completed two maximal efforts separated by at least 30 s. The highest jump achieved was recorded.
Handgrip strength
Dominant handgrip strength was assessed using a handgrip dynamometer (Takei Hand Grip Dynamometer, Model 5401, Cranlea). Participants completed the assessment in a standing position with arms by their side throughout. Upon instruction, participants were instructed to squeeze the dynamometer as hard as possible for ∼5 s to achieve a peak force. 12 Following one familiarisation attempt at ∼50% max effort, participants completed two maximal efforts separated by at least 30 s using their dominant hand. The highest peak force (converted to kg) was recorded.
Chester step test
Maximal aerobic capacity was estimated using the CST. The CST is a submaximal, multistage aerobic capacity test lasting a maximum of 10 minutes. 13 Participants were required to step up and down on a 30 cm box to a specific work-rate achieved through an audible metronome frequency; the test consists of five, two-minute stages. Heart rate (HR) was monitored throughout the assessment and recorded at the end of each stage. Maximal aerobic capacity (V˙O2max) is estimated utilising a participant's max HR (220 – age), the rise in HR at each stage, and the estimated oxygen cost of each stage.13,14
Multi-stage fitness test
Maximal aerobic capacity was assessed in Session-2 using the 20 m MSFT. Participants completed the MSFT as the final element of the testing session (after the CST and strength measures). Participants were required to run ‘shuttles’ between two markers spaced 20 m apart. An audio track denotes the pace that a single tone is sounded to correspond with reaching a marker. The pace is initially set at 8.5 km.h−1 increasing by 0.5 km.h−1 with each increase in level. Participants received a warning upon the event of missing a beep and they were withdrawn when missing two consecutive beeps. The final level and shuttle completed for each participant was recorded and used to estimate V˙O2max (Equation 1) based on available data in Table III Ramsbottom, Brewer and Williams (1988).
Royal navy physical employment standards
The RN PES is completed as a circuit, containing seven discrete stations. For the purpose of the annual fitness assessment, personnel must complete the entire circuit within 15 minutes. For this research, participants were required to complete each station in isolation. This approach was adopted to minimise the confounding effects of cumulative fatigue, pacing, and task order on performance outcomes, thereby allowing participants to produce a best effort in each task. Additionally, one task (deadlift) was omitted as it is completed to a set pacing and therefore not achievable to a best effort. One task is repeated (kettlebell carry), therefore only one iteration was included. Each individual test is detailed below in Table 1.
Overview of royal navy physical employment standard stations.
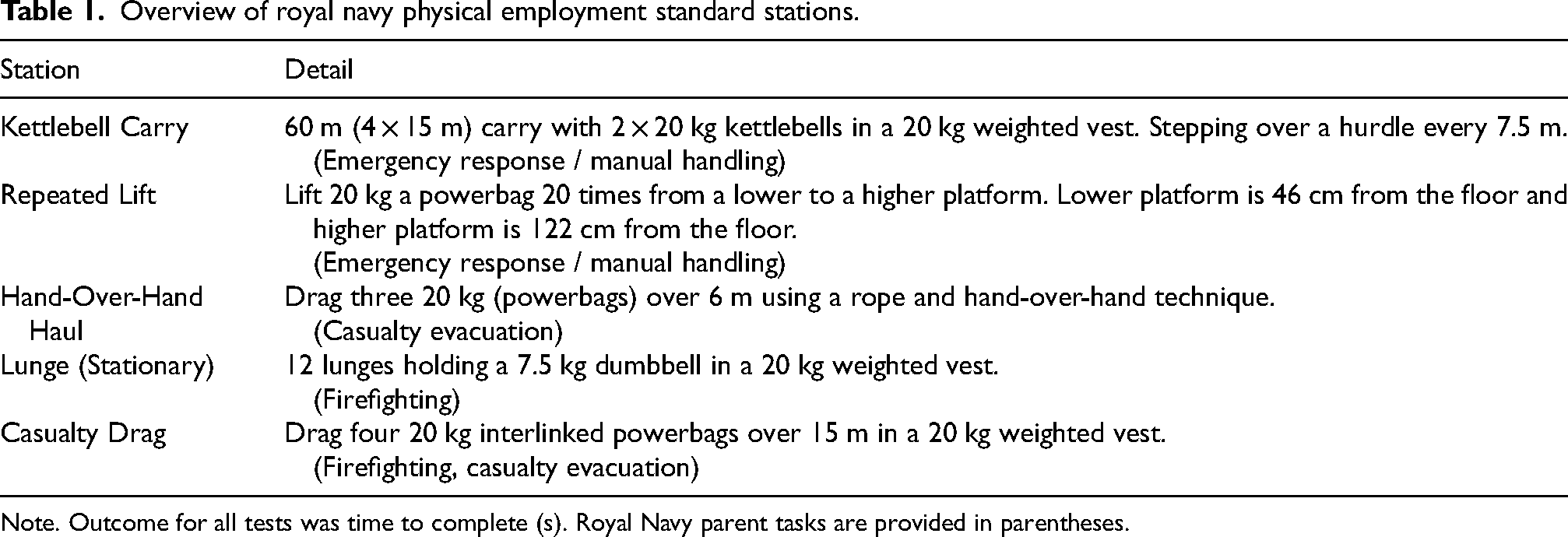
Note. Outcome for all tests was time to complete (s). Royal Navy parent tasks are provided in parentheses.
Data analysis
Statistical analysis was conducted using JASP (v0.19.3, University of Aberdeen, Netherlands) and customised Microsoft Excel spreadsheets. Data were normally distributed and are presented as mean (standard deviation) unless otherwise stated. Paired samples t-tests were used to examine changes in physical performance across INT, with effect sizes reported as Cohen's D. Interpretation of Cohen's D is as follows: ≤0.2 is considered trivial, >0.2–0.5 is small, >0.5–0.8 is moderate and >0.8 is deemed large. 16 Pearson's correlation coefficient was used to determine: 1) associations between initial fitness and changes in fitness across INT, and 2) associations between physical performance and RN PES task performance. Magnitude of correlation coefficients were considered as 0.1–0.3 small, >0.3–0.5 moderate, >0.5–0.7 large, >0.7–0.9 very large, >0.9–<1 almost perfect and 1 perfect. 17 A Bland-Altman plot was used to examine the mean bias and upper and lower 95% limits of agreement (LoA) when comparing estimated maximal aerobic capacity between the CST and MSFT in Session-2 (MSFT as criterion measure). 18
Results
Changes in fitness
Table 2 provides a summary of participant characteristics and the Session-1 and Session-2 physical performance data. Moderate to large improvements (4.9 to 11.9%; P > 0.05) in muscular strength and power were observed across INT, respectively. However, aerobic fitness, as estimated by the CST, demonstrated a moderate decrease (−5%, P < 0.05).
Participant characteristics and physical performance data in session 1 (initial naval training) and session 2 (trade training).
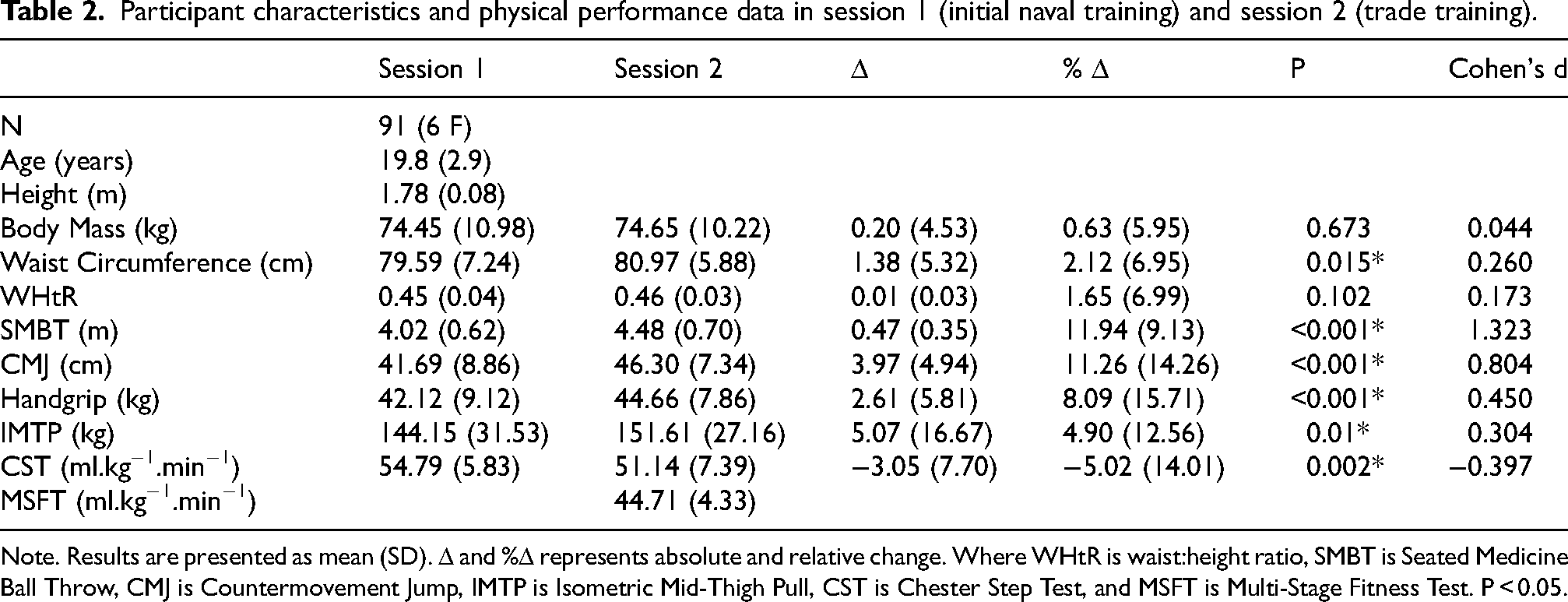
Note. Results are presented as mean (SD). Δ and %Δ represents absolute and relative change. Where WHtR is waist:height ratio, SMBT is Seated Medicine Ball Throw, CMJ is Countermovement Jump, IMTP is Isometric Mid-Thigh Pull, CST is Chester Step Test, and MSFT is Multi-Stage Fitness Test. P < 0.05.
Relationship between initial and change in fitness
Figure 1 illustrates the relationship between initial fitness and change in fitness across INT. No association was found between initial and change in SMBT performance (r = −.027 [95% CI = −.234 to 0.182], P = 0.803). However, a large association was found between initial and change in CMJ (r = −.540 [95% CI = −.678 to −.365}, P < 0.001) and handgrip performance (r = −.523 [95% CI = −.660 to −.353, P < 0.001). Additionally, a moderate association between initial and change in IMTP (r = −.492 [95% CI = −.647 to −.298], P < 0.001) and CST (r = −.430 [95% CI = −.608 to −.212], P < 0.001) performance was observed.
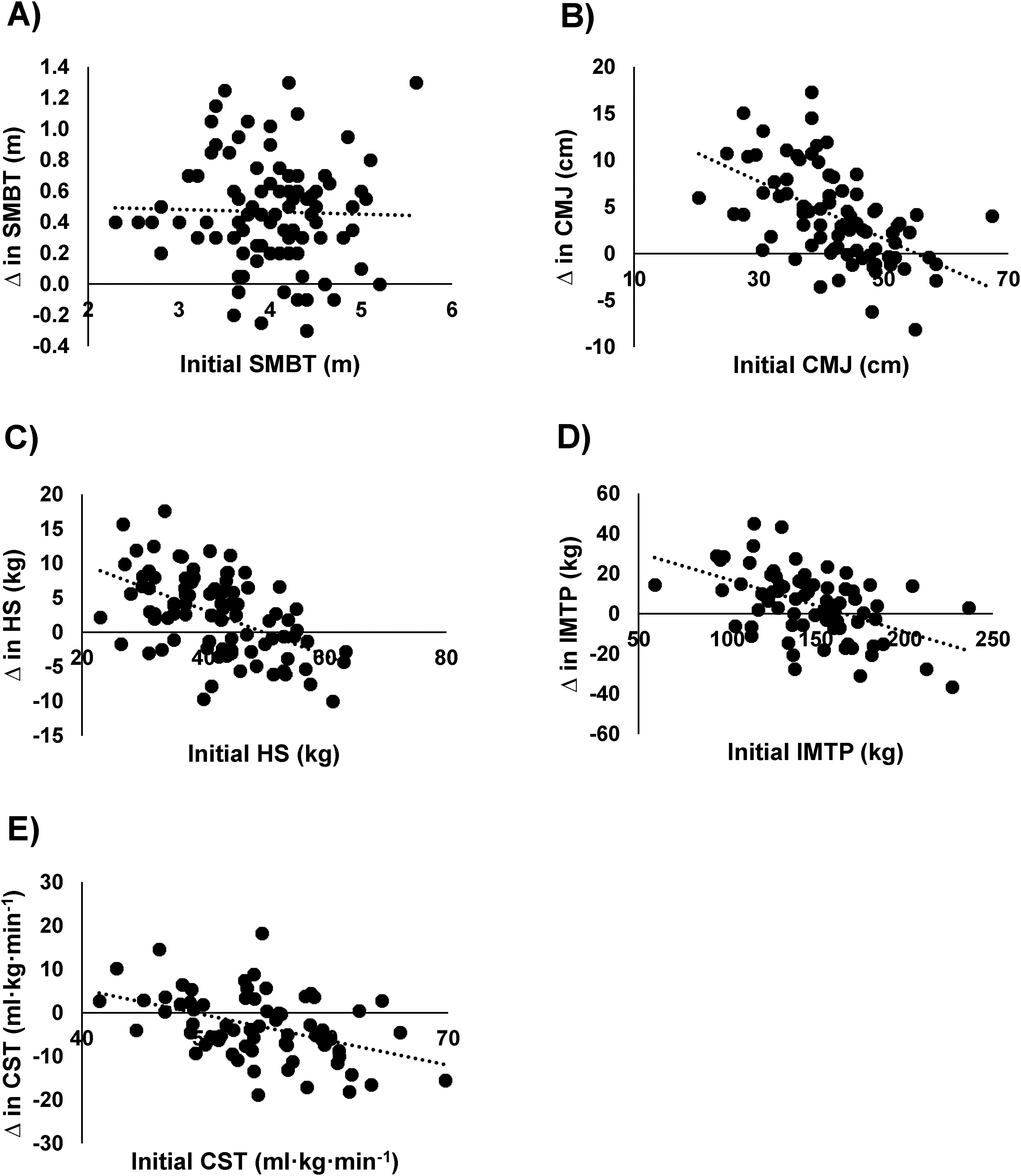
Relationship between Initial fitness and Change in Fitness across INT. Where Panel A is Seated Medicine Ball Throw (SMBT), Panel B is Counter Movement Jump (CMJ), Panel C is Handgrip Strength (HS), Panel D is Isometric Mid-Thigh Pull (IMTP), Panel E is Chester Step Test (CST) and the black dotted line is the trendline.
Relationship between physical fitness and royal navy task performance
Associations between physical fitness and RN task performance are demonstrated in Table 3. The magnitude of correlations ranged between small (MSFT and Casualty Drag; r = −0.141) to large (SMBT and Hand-Over-Hand Haul; r = −0.699). Generally, muscular strength and power measures had a greater association (r = −0.221 to −0.699) with RN task performance than the aerobic capacity measures (r = −0.089 to −0.382).
Associations between physical performance assessments and royal navy task performance.
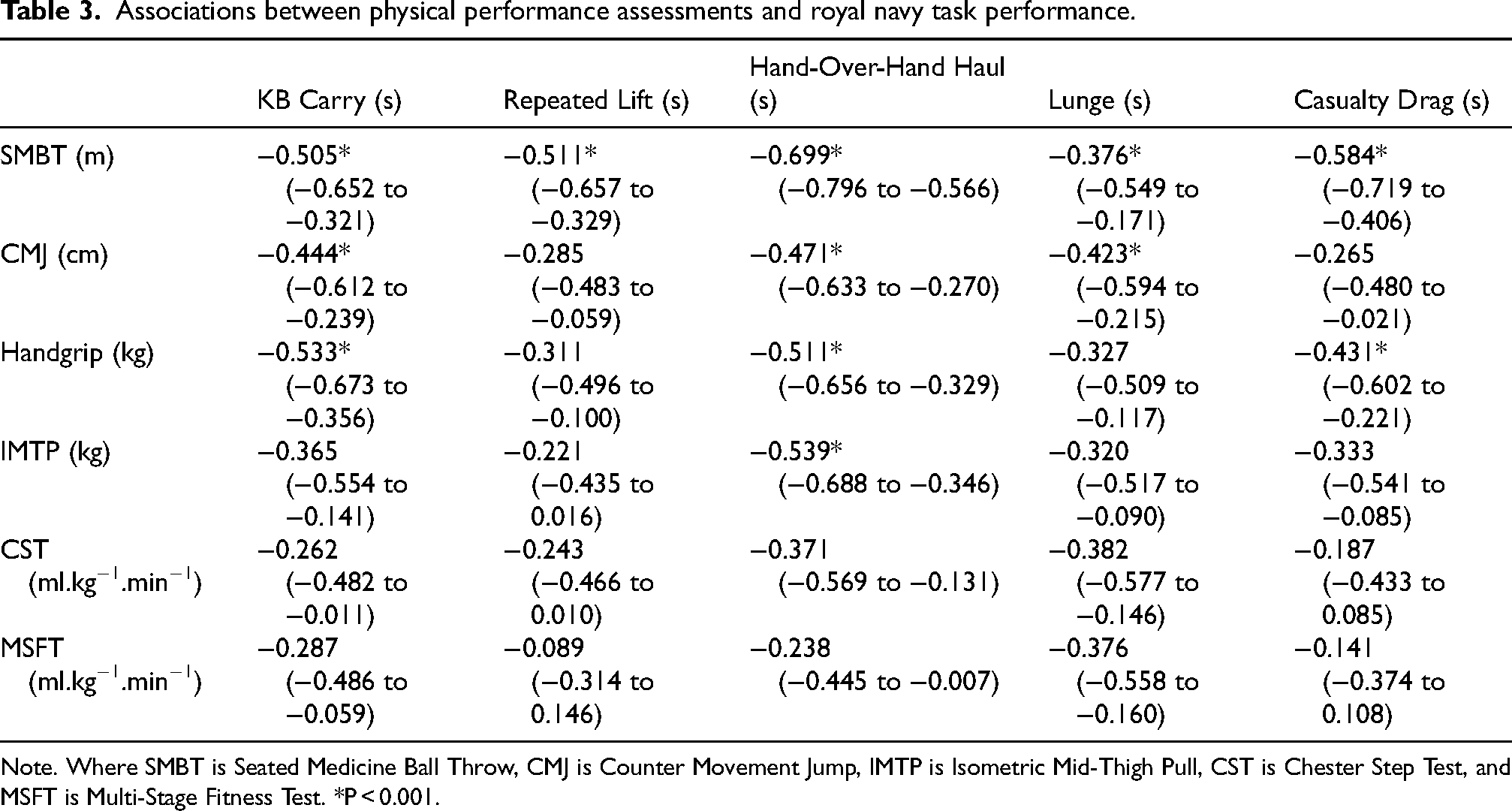
Note. Where SMBT is Seated Medicine Ball Throw, CMJ is Counter Movement Jump, IMTP is Isometric Mid-Thigh Pull, CST is Chester Step Test, and MSFT is Multi-Stage Fitness Test. *P < 0.001.
Comparison of multi-stage fitness test and chester step test
Despite a moderate correlation between estimated V˙O2max from MSFT and CST (r = 0.374 [95% CI = 0.139 to 0.569], P < 0.05), Bland-Altman analysis demonstrated the CST elicited a higher estimated VO2max by 6.26 [95% CI = −6.43 to 18.96] ml·kg−1·min−1 (Figure 2).
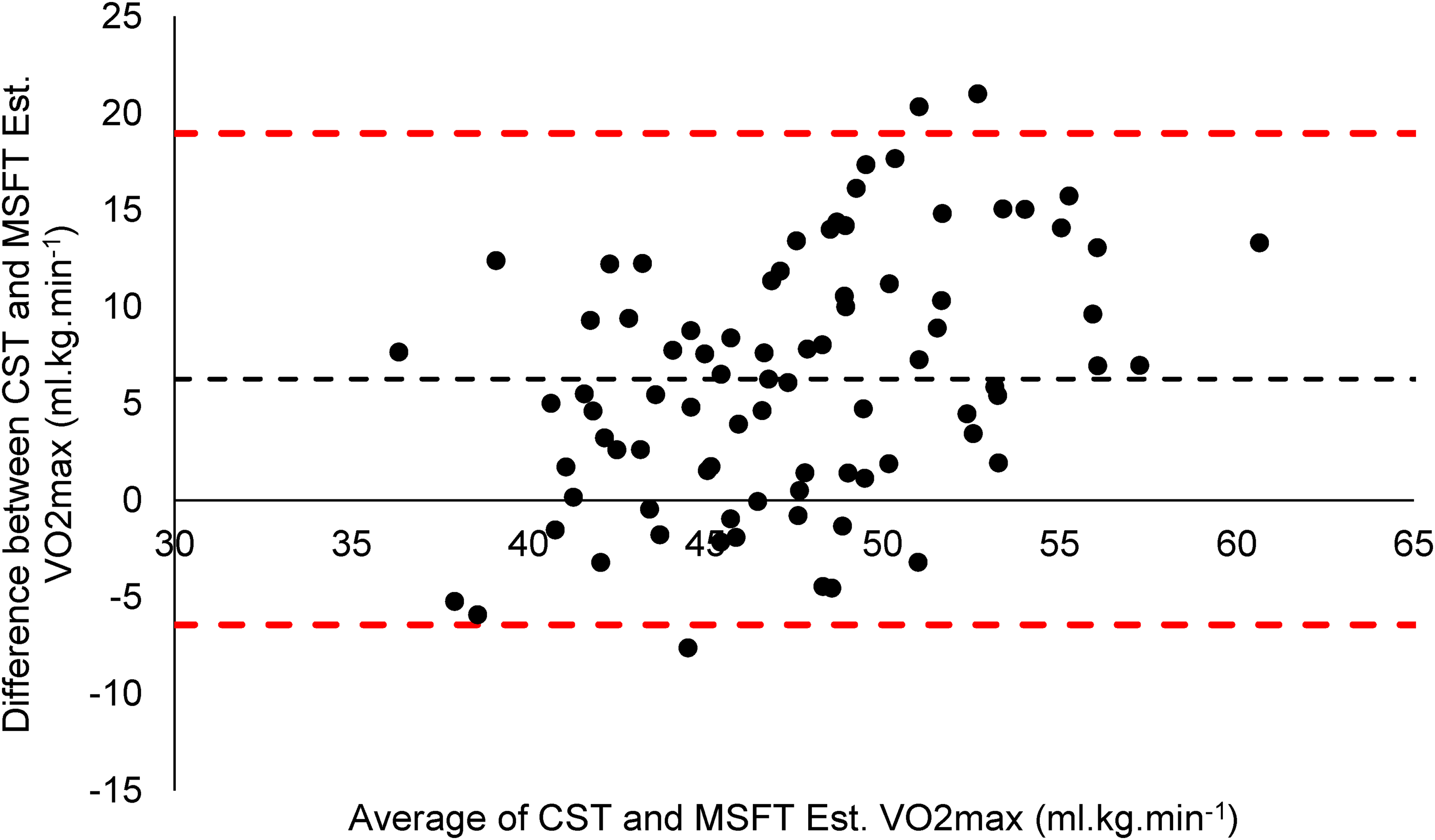
Agreement (mean (black dashed line) ± 95% Limits of Agreement (red dotted line)) between estimated V˙O2max from the Multi-Stage Fitness Test and the Chester Step Test (Color figure online).
Discussion
This study quantified changes in RN recruit fitness during INT and assessed associations between physical attributes and RN PES task performance. The findings revealed moderate to large improvements in muscular strength and power across the 10-week training period, while aerobic fitness, as estimated by the CST, declined. Additionally, measures of muscular strength and power demonstrated stronger associations with RN PES task performance than aerobic capacity. These outcomes have important implications for pre-joining fitness assessment and RN recruit training practices.
Physical development across initial naval training
On a group level, substantial improvements in upper- and lower-body strength and power were observed, specifically with significant gains in the SMBT, CMJ, handgrip strength, and IMTP. These results are consistent with previous findings from UK military training programmes, 1 albeit with some differences on the magnitude of improvement. When comparing results from the present study with data from British Army Standard Entry Basic Training, where participants are of a similar age and body size, SMBT and IMTP performance were similar post initial training (∼4.5 m and ∼150 kg, respectively). However, RN recruits demonstrated greater improvements across training. Improvements in these attributes may be attributable to the training history of the participants and the emphasis on whole-body calisthenic and resistance-based activities in RN INT potentially leading to subsequent neuromuscular adaptations.
Conversely, data from the present study show aerobic fitness, on a group level, declined by 5%, as measured by CST. This contrasts with the documented aerobic improvements (∼5%) observed during British Army and RAF initial training programmes,1,2 albeit using aerobic fitness as estimated using the MSFT as opposed to the CST in the present study. Several factors may explain this finding, such as insufficient programming of aerobic training during INT or physiological fatigue influencing post-training estimates. Additionally, the 5% decline in estimated maximal aerobic fitness is within the previously reported measurement error (11–19%) and limits of agreement for the CST, 19 therefore, this measured reduction in fitness could reflect the test's limited sensitivity rather than true physiological decrement. It should be noted that whilst the study fitness testing sessions were programmed into the training schedule, we were unable to control for physical activity or training immediately before the measurements period which may have impacted the findings. These results highlight the need to review the aerobic conditioning content of INT and the appropriateness of CST for longitudinal fitness monitoring.
Influence of baseline fitness on adaptation
This study demonstrated strong negative correlations between initial performance and changes in CMJ (r = −0.540), handgrip strength (r = −0.523), and IMTP (r = −0.492), as well as a moderate inverse association for CST (r = −0.430). These findings suggest that recruits with lower initial fitness experienced the greatest relative improvements, while those with higher initial fitness saw minimal gains or potential regression. This aligns with the principle of diminishing returns and supports existing literature indicating that standardised physical training delivery in group settings may inadequately stimulate high-fitness individuals. 4 When comparing these findings to that of Rue et al., 1 who examined this relationship in British Army Standard Entry Basic Training, a similar regression to the mean was found across changes in aerobic fitness, upper body power, and lower body strength. These findings reinforce the case for differentiated physical training, potentially through ability-based groupings or individualised programming.20,21
Associations with royal navy task performance
The data show that muscular strength and power were more strongly associated with RN PES performance than aerobic fitness. Notably, the SMBT demonstrated the strongest and most consistent correlations with all five occupational tasks (r = −0.376 to −0.699), followed by CMJ, IMTP, and handgrip strength. These associations reflect the physical requirements of the RN PES, which encompasses critical and physically demanding activities required to undertake Casualty Handling, Firefighting, and Emergency Responses, all of which demand high-intensity muscular output. By contrast, aerobic fitness showed weak to moderate associations with task performance, supporting the idea that absolute strength and power are more critical to RN operational demands. These findings align with military research which increasingly recognises the importance of muscular strength and anaerobic performance in military task simulations.22,23,24 They also support the inclusion of strength and power assessments in physical readiness evaluations. It is likely that if the PES was completed in its entirety (in a circuit) to a best-effort that there would be a greater importance of aerobic fitness, however, completing the tasks in isolation was preferred to minimise the confounding effects of cumulative fatigue, pacing, and task order on the performance of individual tasks. It is also unlikely that RN personnel would be required to complete these tasks back-to-back in an emergency situation, therefore the present study methodology provides greater ecological validity.
Comparing estimates of aerobic fitness
Despite a moderate correlation (r = 0.374) between CST- and MSFT-estimated V˙O2max, Bland-Altman analysis revealed that the CST elicited a higher estimated V˙O2max. This degree of bias and the wide limits of agreement (6.26 [95% CI = −6.43 to 18.96] ml·kg−1·min−1) suggests that the CST, completed in its current form, does not provide an accurate measure of aerobic fitness. Whilst this analysis demonstrates these methods are not equivalent, the very wide limits of agreement between estimates likely reflects the cumulative error in comparing two indirect field-based prediction methods rather than a true ‘gold standard’ measure of aerobic capacity, where previous data regarding the accuracy of the CST has elicited more favourable results. 19 Nonetheless, in the present study, the magnitude of disagreement (± 12.7 ml·kg−1·min−1) corresponds to ∼29% of the group mean as estimated by the MSFT, indicating substantial random disagreement exceeding the magnitude of typical recruit training-related changes in aerobic fitness (∼5%).1,2 While the CST remains practical and time-efficient, its validity in recruit populations may be limited, especially when precision is needed to guide individual development or inform occupational standards. Therefore, further work is justified to attempt to improve measurement estimation, where the implementation of a sub-maximal assessment of aerobic fitness would have great utility in the RN recruit space.
Implications for pre-joining fitness test development
The findings offer compelling evidence to guide the development of a revised PJFT for the RN. The strong associations between SMBT, IMTP, and PES performance support their inclusion in a PJFT as predictors of task readiness. The weak associations between aerobic tests and task outcomes likely reflect the muscular strength and endurance-dominant nature of the PES tasks, which simulate the demands of emergency seafaring tasks rather than sustained endurance. It is acknowledged that aerobic fitness is the foundation of long-term health, with higher cardiorespiratory fitness consistently associated with reduced risk of all-cause mortality, cardiovascular disease, and metabolic disorders. 25 In physically demanding occupations, greater aerobic capacity supports work tolerance, accelerates recovery, and lowers the risk of musculoskeletal injury, particularly during load carriage or repetitive tasks.26,27 Within the military, sustained aerobic fitness is also critical for deployability, operational readiness, and career longevity, as it underpins resilience to both physical and cognitive fatigue. 28 , 29 Therefore, despite the lower importance of aerobic fitness for discrete RN task performance, assessment by some means should be considered as part of a PJFT and/or annual test to reinforce its importance for general health and wellbeing.
Drawing on the precedent set by the British Army in 2019, which incorporated SMBT and IMTP into its PJFT to better reflect operational demands, the RN could similarly adopt a multi-component test to ensure new entrants possess job-relevant strength and power capabilities. Such a shift would incentivise appropriate physical preparation, support safer and more effective training progression, and reinforce the importance of strength-based attributes in naval service.
Limitations
The small number of female participants (n = 6) limits the generalisability of findings across sexes. It is also acknowledged that the sample size, whilst appropriate for this exploratory work, has limited the ability to perform stratified or multivariate analyses which would provide greater interpretive depth. With regards to the methodology, PES tasks were completed in isolation rather than as a circuit, which may influence comparability to operational delivery particularly in terms of the aerobic fitness requirements of prolonged emergency tasks. However, administering tasks independently improved construct validity for examining associations between discrete physical qualities and occupational task performance. Furthermore, as mentioned, whilst measurement serials were programmed into the training schedule, there was little control over physical activity and/or training prior to completing the testing. Lastly, the CST and MSFT were not both completed pre-training, limiting comparisons of aerobic fitness change across INT using consistent measures.
Conclusions and future directions
In summary, this study demonstrates that INT enhances muscular strength and power but may not sustain aerobic fitness in RN recruits. Muscular strength and power were more strongly associated with RN task performance than aerobic capacity, reinforcing the relevance of these attributes for occupational readiness. These findings support the development of a multi-component PJFT incorporating strength and power assessments and suggest a need to review aerobic training provision in INT. Future research should include a greater, more balanced sample and incorporate multivariate and stratified analyses to explore moderating effects, link fitness changes to injury outcomes, and assess the predictive validity of proposed PJFT elements for long-term training success and ability to deploy.
Footnotes
Acknowledgements
The research team would like to thank the Royal Navy Physical Training Staff at HMS Raleigh, HMS Sultan, and HMS Collingwood.
Ethical approval and informed consent
Participants were given a verbal and written brief prior to providing their consent. The study was approved by the Ministry of Defence Research Ethics Committee (2252/MODREC/23).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by UK Ministry of Defence.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.