
Abstract
Background
The prevalence of low back pain among office-workers is associated with prolonged sedentary behavior and improper postures. In addition to poor ergonomics, often overlooked issues such as psychological factors, sleep, fatigue, and pain can further exacerbate low back pain.
Objective
This study purposes to show whether there are differences in low back pain disability, anxiety, depression, quality of sleep, fatigue, and pain based on years of work experience among office-workers and to investigate determinants of low back pain disability.
Methods
This cross-sectional study included 212 office-workers. Office workers were divided into <10 years, 10–19 years, and ≥20 years based on work experience. Low back pain, anxiety and depression, sleep quality, fatigue, and pain were assessed.
Results
There were significant differences in low back pain complaints among office-workers based on the frequency of rest breaks (p = 0.001), the adequacy of rest areas (p < 0.001), and ergonomic education(p < 0.001). The low back pain disability score showed poor to moderate correlations with anxiety-depression (r = 0.492, p < 0.001), sleep (r = 0.427, p < 0.001), fatigue (r = 0.44, p < 0.001), and pain at various times (rest, activity, and night) (r = 0.532, r = 0.567, r = 0.567, respectively; all p < 0.001) among office workers. A multiple linear regression model found that fatigue and pain-night were determinants of low back pain disability, accounting for 42.2% of the variance (F = 18.104, p < 0.001).
Conclusion
Fatigue and night pain were found to be key predictors of low back pain disability among office-workers. These findings highlight the role of ergonomic modifications, appropriate rest breaks, and targeted strategies to manage fatigue and nighttime pain to reduce low back pain disability in this population.
Keywords
Introduction
In the present era, the prevalence of a sedentary lifestyle has escalated, with an increasing number of individuals dedicating prolonged hours to desk-bound activities during both work and leisure.1,2 This has led to a concerning rise in the prevalence of musculoskeletal problems within the working population.1,3 A growing body of evidence suggests the widespread occurrence of low back pain, making it a predominant musculoskeletal issue in both developed and developing nations. Among office workers, the combination of static sitting postures, repetitive movements, and inadequate ergonomic arrangements further heightens the risk of developing low back pain.4,5 In addition, elevated job-related anxiety in combination with prolonged sedentary behavior may further contribute to musculoskeletal disorders, resulting in a disproportionately higher prevalence among office-based computer workers compared with other occupational groups. Low back pain not only diminishes the well-being of individuals but also gives rise to various adverse consequences in the workplace.1,6,7 Beyond physical strain, low back pain is a multifactorial condition closely linked with psychological factors such as stress, anxiety, and depression, which may exacerbate pain and disability.8,9 Furthermore, sleep disturbances can impair both physical and mental health, leading to reduced daytime functionality, lower productivity, and higher healthcare costs. 10
Prolonged working hours, static sitting postures, and poor ergonomics in office environments contribute to fatigue and discomfort, increasing the risk of low back pain.11,12 Mental workload and job-related stress may further exacerbate fatigue, leading to reduced concentration and productivity.1,11,12 Although low back pain is common among office workers, existing research has primarily focused on clinical aspects rather than psychosocial or behavioral determinants. To our knowledge, no study has comprehensively examined how pain severity, fatigue, anxiety, depression, and sleep quality interact in this population. Therefore, this study aims to determine whether low back pain, anxiety, depression, sleep quality, fatigue, and pain severity differ according to years of work experience among office workers who use computers. It also aims to identify which of these factors are associated with low back pain complaints.
Methods
This cross-sectional study was carried out among office workers using computers. The study protocol was approved by the Ethics Committee of Bingöl University (E-33117789-044-122898) on 18 September 2023. All participants provided informed consent through an online form, and the study was conducted in accordance with the ethical standards of the Declaration of Helsinki.
Participants
The study population consisted of office workers who use computers. The study was conducted between September 2023 and January 2024 in Türkiye. Participants were recruited from public and private office settings through online announcements and institutional mailing lists. The inclusion criteria were: (1) adults within the age range of 18 to 65 years; (2) office workers who regularly use computers; (3) provision of informed, voluntary consent; (4) individuals with a minimum of one year of occupational experience. The exclusion criteria were: (1) individuals diagnosed with chronic diseases affecting the spine; (2) pregnancy; (3) having a diagnosis of spinal and disc infection, rheumatoid arthritis, ankylosing spondylitis, spondylolisthesis, tumor, or osteoporosis.
The post-hoc power analysis was used with G*Power 3.1.2.1 software. Two-hundred twelve included office workers were found to provide a power of 0.998, based on a Type 1 error rate (alpha = 0.05), effect size of 0.3 (considered a medium effect with d ≥ 0.3), coefficient of determination of 0.09, and a one-tailed hypothesis. Therefore, the present sample size was deemed to be sufficiently powered.
Outcome measures
Sociodemographic (gender, age, body mass index) and occupational features (daily working hours, weekly working days, rest areas, rest breaks) of all office workers were recorded. Additionally, ergonomic conditions of the working environment were assessed through standardized questions on rest breaks, adequacy of designated rest areas, which refers to rooms or spaces provided for employees to take breaks and recover, information received from specialists, workplace temperature, and computer positioning.
Quebec Back Pain Disability Scale (QBPDS): A 20-item tool assessing the impact of back pain on daily functional activities using a 6-point Likert scale (0 = no difficulty, 5 = inability to perform). Total scores range from 0 (no disability) to 100 (maximum disability). 13
Hospital Anxiety and Depression Scale (HADS): A 14-item questionnaire evaluating anxiety and depression through two subscales, HADS-anxiety (HADS-A) and HADS-depression (HADS-D). Each subscale has a cut-off score of 8, with scores interpreted as follows: 0 to 7 for normal, 8 to 10 for mild, 11 to 14 for moderate, and 15 to 21 for severe symptoms, indicating clinically relevant anxiety or depression. 14
The Pittsburgh Sleep Quality Index (PSQI): This instrument is a self-administered questionnaire comprising 24 items, which are organized into seven components, namely subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleep medications, and daytime dysfunction. Each item is rated on a scale from 0 to 3, where a score of 0 indicates no difficulty and a score of 3 reflects severe problems. Total scores range from 0 to 21, with higher scores indicating poorer sleep quality. 15
Fatigue Severity Scale (FSS): Comprising 9 items, each scored on a 7-point scale, this instrument measures the perceived impact of fatigue on daily functioning. Higher scores reflect greater fatigue severity. 16
Numerical Pain Scale (NPS): Participants rated their low back pain intensity over the past 24 h for resting, activity, and nighttime pain on a scale of 0 (no pain) to 10 (worst possible pain). 17
To minimize potential bias from self-reported measures, validated instruments were used, and participation was anonymous. Cases with incomplete responses were excluded from the analysis, and data completeness was verified prior to statistical testing.
Statistical analysis
Statistical analyses were performed using SPSS version 22.0 (IBM Corp., Armonk, NY, USA). The normality of data distribution was assessed using both visual (histograms, Q–Q plots) and analytical methods (Shapiro–Wilk and Kolmogorov–Smirnov tests). Group comparisons were performed utilizing the independent samples t-test. Comparisons of continuous variables between groups were conducted using One-Way ANOVA with Bonferroni correction.
Pearson correlation coefficients were computed to evaluate associations with low back pain disability and other variables. Correlation strength was interpreted as follows: negligible (r < 0.30), low (r = 0.30–0.49), moderate (r = 0.50–0.69), strong (r = 0.70–0.89), and very strong (r ≥ 0.90). 18 Multiple linear regression analysis using the enter method was performed to identify independent variables significantly affecting low back pain. To detect multicollinearity, variance inflation factors (VIF) were examined for all independent variables. Significance was set at p < 0.05.
Results
A total of 212 office workers using computers were included in the present study. 101 (47.6%) were female and 111 (52.4%) were male. Sociodemographic and occupational characteristics of the office workers were as follows; the mean age was 35.94 ± 8.76 years, the mean years of work experiences was 11.92 ± 8.78 years, the mean daily working hours were 9.88 ± 4.84 and the mean weekly working days was 4.82 ± .98. In the office workers, there were 99 (46.7%) < 10 work years, 67 (31.6%) 10–19 work years, and 46 (21.7%) ≥ 20 work years. The detailed demographic and occupational characteristics, along with the working environment and ergonomic approaches of the participants, are presented in Table 1.
Sociodemographic, occupational, and ergonomic characteristics of office workers.
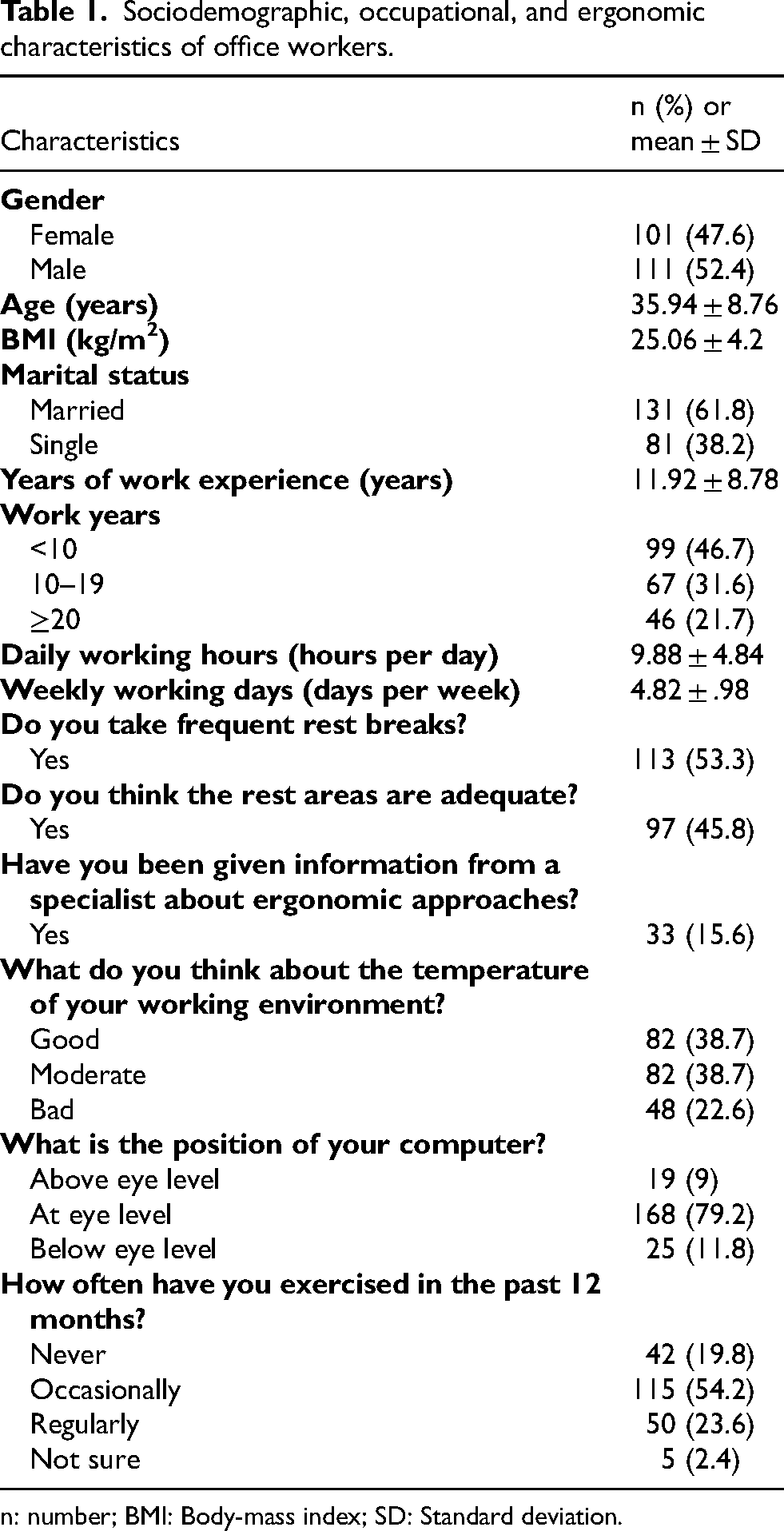
n: number; BMI: Body-mass index; SD: Standard deviation.
There were significant differences in low back pain disability scores among office workers based on the frequency of rest breaks, the adequacy of rest areas, and receiving an ergonomic education (p < .05; Figure 1). A one-way ANOVA was conducted to compare the differences in QBPDS, HADS-A, HADS-D, HADS total score, PSQI and all its subgroups (except sleep latency), FSS, NPS-resting, NPS-activity, and NPS-night between different work experience. The results indicated no significant differences between the groups for any of these parameters (p > .05; Table 2).
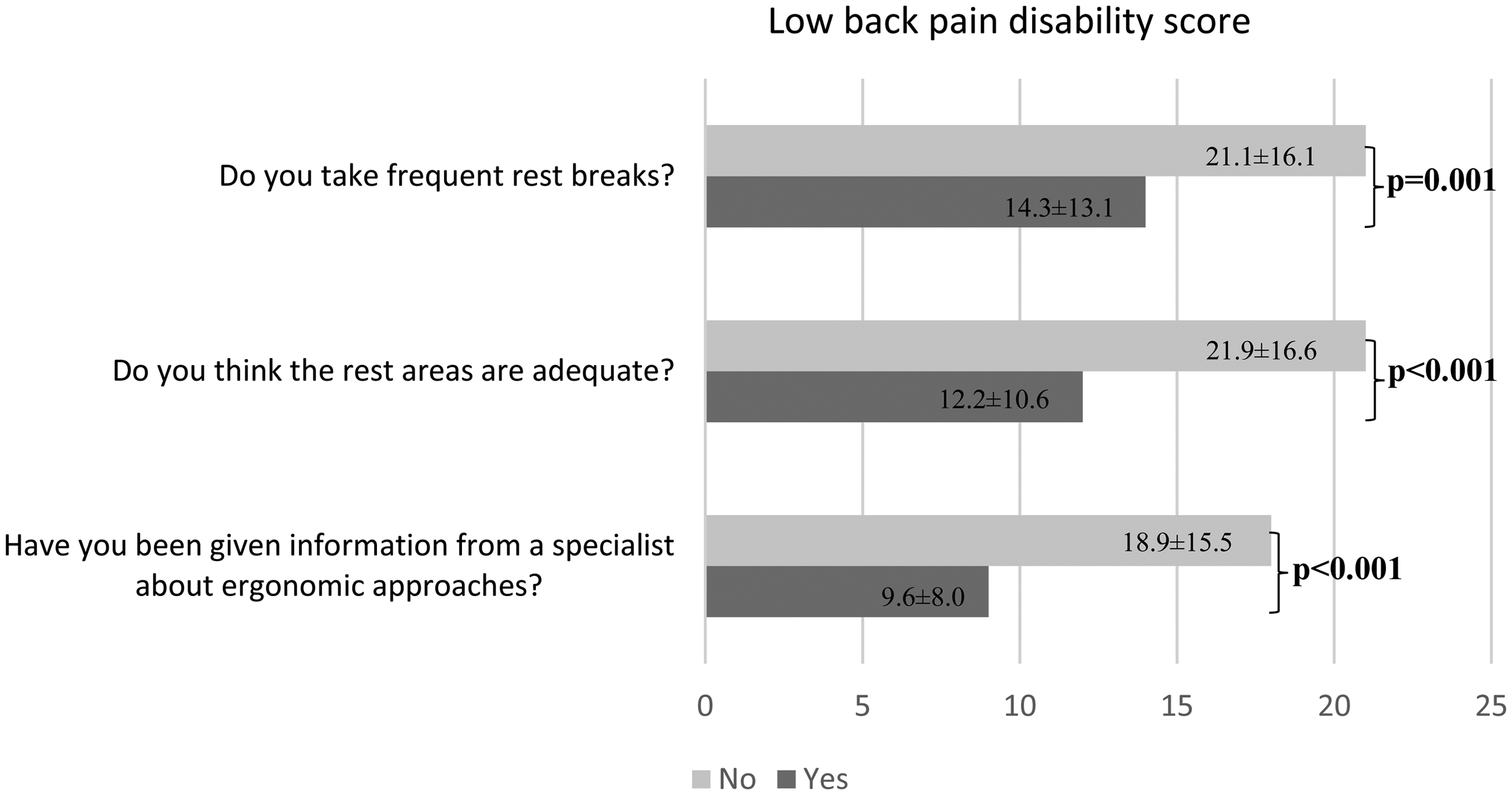
Comparison of participants’ occupational characteristics and ergonomic approaches according to low back pain.
Comparison of low back pain disability, anxiety, depression, sleep quality, fatigue, and pain in office workers according to years of work experience.
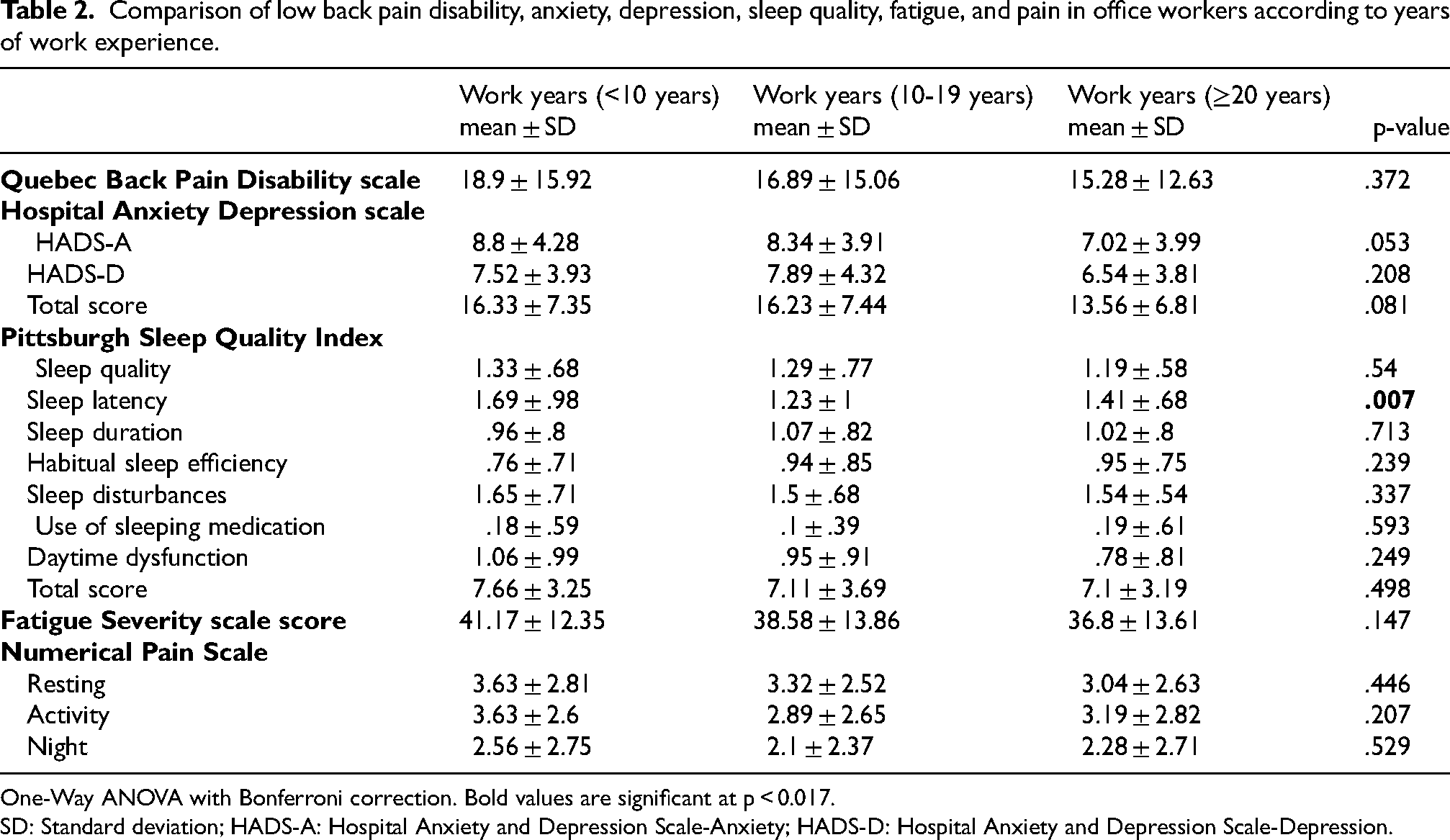
One-Way ANOVA with Bonferroni correction. Bold values are significant at p < 0.017.
SD: Standard deviation; HADS-A: Hospital Anxiety and Depression Scale-Anxiety; HADS-D: Hospital Anxiety and Depression Scale-Depression.
The low back pain disability score had poor to moderate correlations with HADS-A (r = .433, p < .001), HADS-D (r = .446, p < .001), HADS total score (r = .492, p < .001), sleep quality (r = .359, p < .001), sleep latency (r = .301, p < .001), sleep disturbances (r = .344, p < .001), daytime dysfunction (r = .373, p < .001), PSQI total score (r = .427, p < .001), FSS score (r = .44, p < .001), NPS-resting (r = .532, p < .001), NPS-activity (r = .567, p < .001), and NPS-night (r = .567, p < .001) among office workers. These results indicated that low back pain disability was associated with HADS-A, HADS-D, HADS total score, sleep quality, sleep latency, sleep disturbances, daytime dysfunction, PSQI total score, FSS score, NPS-resting, NPS-activity, and NPS-night. Table 3 shows the correlation coefficients between low back pain disability and other study outcomes.
Correlations of low back pain disability in office workers.
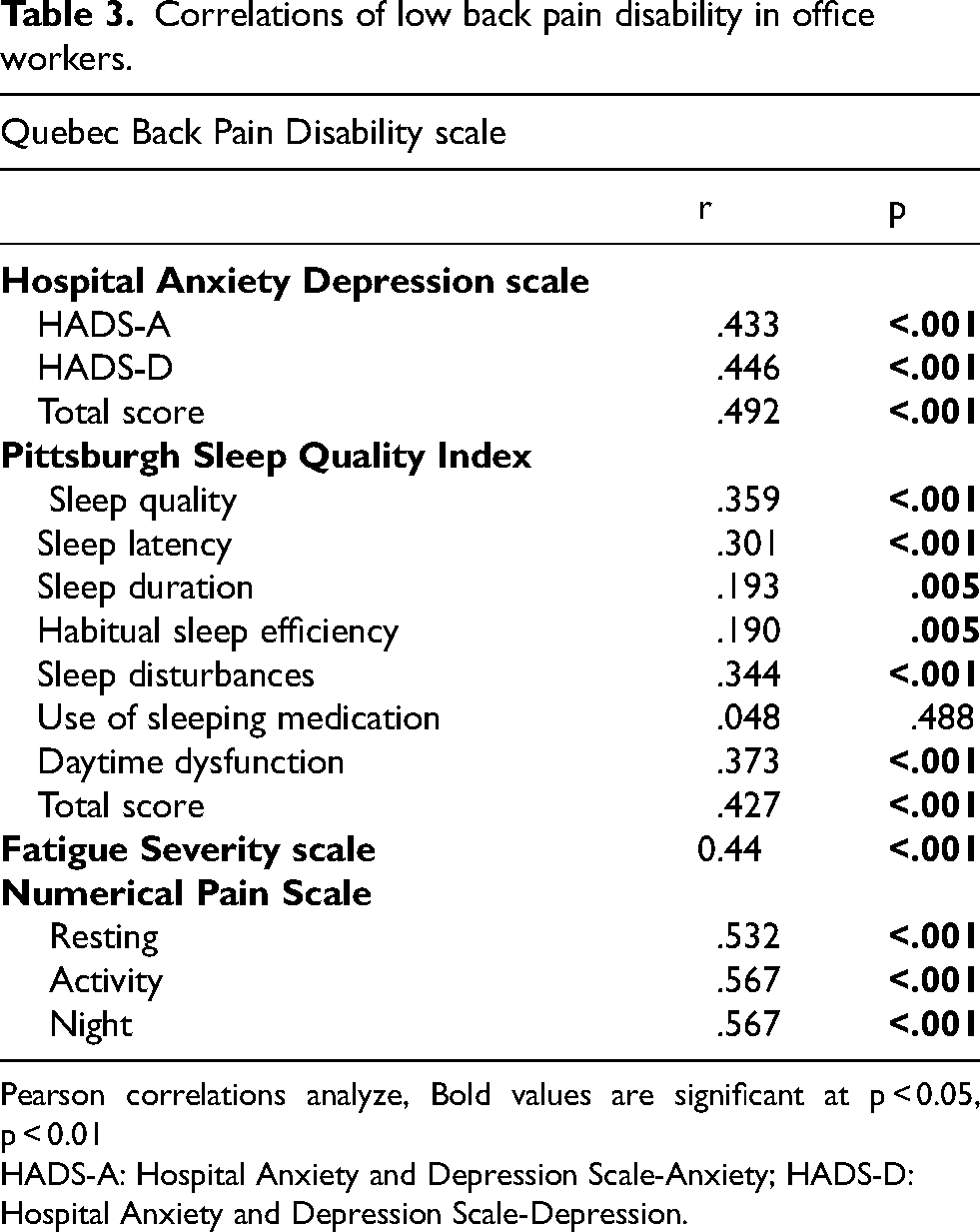
Pearson correlations analyze, Bold values are significant at p < 0.05, p < 0.01
HADS-A: Hospital Anxiety and Depression Scale-Anxiety; HADS-D: Hospital Anxiety and Depression Scale-Depression.
HADS-A, HADS-D, HADS total score, sleep quality, sleep latency, sleep disturbances, FSS score, NPS-resting, NPS-activity, and NPS-night were considered in a multiple linear regression enter model. FSS score and NSP-night were analyzed to be determinants of low back pain disability, accounting for 42.2% of the variance (F = 18.104, p < .001; Table 4).
Determinants of low back pain disability in office workers.
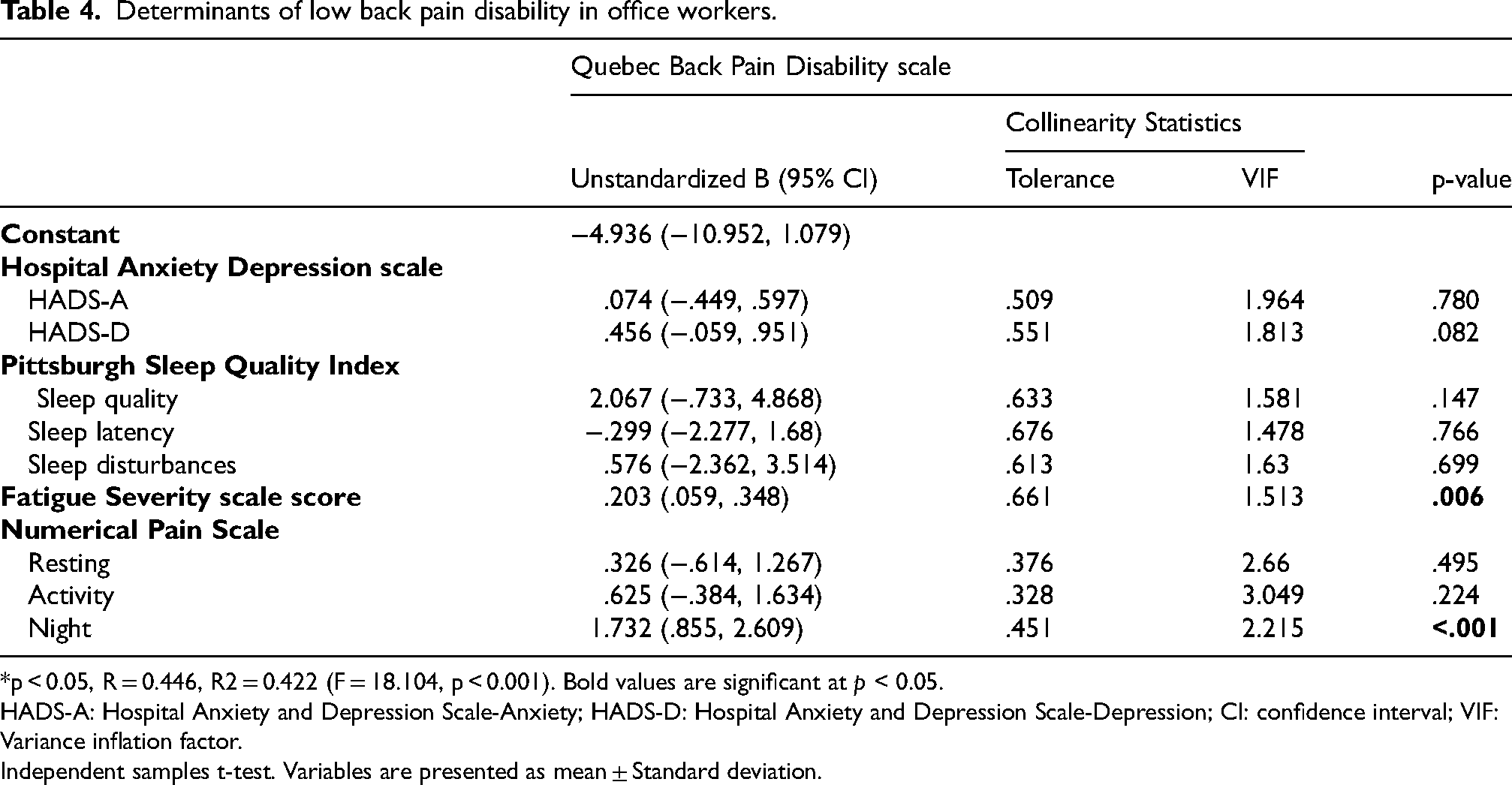
*p < 0.05, R = 0.446, R2 = 0.422 (F = 18.104, p < 0.001). Bold values are significant at p < 0.05.
HADS-A: Hospital Anxiety and Depression Scale-Anxiety; HADS-D: Hospital Anxiety and Depression Scale-Depression; CI: confidence interval; VIF: Variance inflation factor.
Independent samples t-test. Variables are presented as mean ± Standard deviation.
Discussion
This study examined whether low back pain disability, anxiety, depression, sleep quality, fatigue, and pain severity differ according to years of work experience among office workers and explored which of these factors are associated with low back pain complaints. The findings showed that frequent rest breaks, adequate rest areas, and ergonomic education were associated with lower levels of low back pain disability. The results also indicated that low back pain disability, anxiety, depression, sleep quality, fatigue, and pain severity were similar across different work experience groups. Furthermore, low back pain disability was associated with anxiety, depression, sleep quality, fatigue, and pain severity, while fatigue and night pain demonstrated stronger associations with disability.
The present study found that frequent rest breaks, adequate rest areas, and ergonomic education were effective in decreasing low back pain in computer-using office workers. Transitioning from a seated to a standing working position every thirty minutes across the workday led to a significant reduction in low back pain in office-workers, compared to seated positions. 12 A study showed that promoting active breaks or encouraging posture variations can help prevent the onset of neck and lower back pain in office workers at high risk. 19 Also, they suggested that active breaks may decrease onset of low back pain by 66%. 19 Evidence from systematic reviews supports the effectiveness of rest breaks in minimizing lower back pain and discomfort.20,21 Previous studies have shown that frequent active breaks combined with postural change are beneficial in reducing lower back pain, discomfort and fatigue.22,23 Additionally, a study identified ergonomic modifications to the workstation and practical education as the most effective strategies for preventing low back pain. 24 In another study, an inappropriate location of computer monitor was found to be a significant risk factor for low back pain in female computer-using workers in China. 25 The present study is consistent with the results of previous studies. To lower the incidence of low back pain among office workers, implementing regular rest breaks, establishing designated rest areas, and providing comprehensive ergonomic training and workspace design are considered essential.
We found that the level of low back pain did not vary by working year. Rachmawati et al. indicated that age, years of work, and posture were associated with complaints of low back pain. 26 They evaluated a smaller sample with a working year of more than and less than 5 years, which may lead to differences in the results. Another study reported that the prevalence of low back pain in office-workers by working year was higher between 10 and 19 years. 27 In this study, the predominance of female participants and their older age 27 may have contributed to the differences observed compared with our study. These results are possible to vary depending on age and gender distribution. These findings may also be attributed to the fact that office workers often begin experiencing low back pain early in their careers.
In the present study, we found that anxiety and depression scores, sleep quality, and fatigue did not differ according to total years of work experience among office workers. A study showed that staying in one's current job for more than five years was a protective factor against anxiety. 28 In a study conducted in Turkish primary health care workers, it was found that trait anxiety was similar in worker with ≤10 and ≥11 years of total working years. 29 The present study was consistent with the Picakciefe et al.'s study. 29 A study reported that sleep quality improved with increasing years of employment among hospital office workers. 30 A recent extensive study exhibited that workers with longer working hours had lower sleep quality. 31 In the present study found that scores of sleep quality by total years of work experience were similar in office workers. We think that longer working hours, rather than years, have an impact on sleep quality and that biological adaptation, which increases with working years, is responsible for this effect. A study reported that there was no relationship between working years and subjective fatigue among workers. 32 In present study, fatigue did not vary according to the working years, in line with the Yogisutanti et al.'s study. 32 The present study provided a new insight that years of work experience does not have a significant effect on levels of low back pain, anxiety, depression, sleep, and fatigue.
The present study showed that low back pain disability was associated with anxiety, depression, sleep quality, fatigue, and pain severity, and that fatigue and night pain were predictors of low back pain disability. Previous studies suggested that the scores of lower back pain were associated with risk of depression or anxiety symptoms, 33 greater sleep disturbance, 34 and increased fatigue. 35 The present study was consistent with the previous studies. Furthermore, the present study provided new insight that the determinants of low back pain disability are fatigue and night pain. Inflammatory low back pain is known to be frequently associated with night pain. 36 Night pain and fatigue in office workers should be closely monitored and should be diagnosed from an early stage. Additionally, the risks of low back pain among office-workers may be reduced by promoting physical activity, exercise, and ergonomic training.
Fatigue and night pain contribute to disability through several interrelated mechanisms. Daily musculoskeletal load can intensify night pain, disturb sleep, and impair recovery, creating a cycle of increasing discomfort.37,38 Night pain, in particular, disrupts sleep continuity by shortening the deep sleep phase, which is crucial for muscle recovery. 39 Sleep disturbances and musculoskeletal pain share a bidirectional relationship; poor sleep exacerbates pain sensitivity, and, conversely, persistent pain disrupts sleep, resulting in a vicious cycle. This interplay between sleep deprivation, pain sensitivity, and recovery processes not only heightens physical discomfort but also affects cognitive and emotional well-being, leading to greater functional disability.37,38,40 Moreover, alterations in the circadian rhythm of cortisol within the hypothalamic–pituitary–adrenal axis caused by sleep deprivation may increase pain sensitivity and fatigue, which can further exacerbate the disability associated with musculoskeletal pain. 41 This process involves a complex biopsychosocial mechanism where psychological factors (such as anxiety and stress) and physiological responses (such as the disruption of hormonal cycles) work together, amplifying the impact of fatigue and pain.42,43 While our study did not directly explore these physiological pathways, the observed associations between musculoskeletal strain, disrupted sleep, and neuroendocrine alterations are consistent with existing literature on chronic pain and sleep disturbances. This suggests that fatigue and night pain play significant roles in the disability of office workers by influencing both their physical functioning and their psychological resilience. Future studies should focus on the physiological contribution of fatigue and night pain to disability, particularly exploring pathways such as musculoskeletal load, cortisol regulation, and sleep disruption. Given the high prevalence of these issues among office workers, especially those engaged in prolonged computer use, these findings may have critical implications for workplace health interventions, such as ergonomic improvements, stress management, and better sleep hygiene practices.
Despite its contributions, this study has some limitations. Firstly, due to the cross-sectional study, correlation and multiple regression analyses were used to identify relationships and determinants among the self-reported outcome measurements. Future prospective studies are needed to confirm the results of the study. Secondly, as the study relied on self-report tools, the possibility of response bias cannot be ruled out, which may have influenced the accuracy of the reported outcomes. Thirdly, the study was performed with office workers in Türkiye. Therefore, the generalizability of the findings to other occupational groups or cultural contexts should be interpreted with caution, as low back pain attitudes, behaviors, and beliefs may be influenced by workplace conditions, cultural norms, and occupational health systems. However, unlike previous studies that primarily examined clinical variables, this study simultaneously evaluated environmental and psychosocial determinants of low back pain, including the effect of working time on disability, anxiety, depression, sleep quality, fatigue, and pain severity among office workers. These findings provide valuable insights for developing approaches to address low back pain in this population.
Conclusion
Low back pain is a common condition among office workers and is associated with reduced quality of life and occupational productivity. In this study, several factors were found to be associated with low back pain–related disability, including fatigue, night pain, sleep disturbances, general pain, anxiety, and depression. Fatigue and night pain demonstrated comparatively stronger associations with disability scores in this population. Additionally, low back pain was reported more frequently during the first decade of employment, suggesting that early career periods may require particular attention. Although the cross-sectional design prevents causal interpretations, the findings highlight meaningful correlates of low back pain among office workers. Workplace strategies such as encouraging regular rest breaks, improving rest areas, and providing ergonomic education may help mitigate these associated factors and support employee well-being. Future longitudinal and interventional studies are needed to clarify causal pathways and evaluate the effectiveness of workplace interventions.
Footnotes
Acknowledgments
We would like to thank all office workers who participated in the study.
Ethical statement
The study protocol was approved by the Ethics Committee of Bingöl University (E-33117789-044-122898) on 18 September 2023.
Informed consent
All participants provided informed consent through an online form prior to data collection.
Credit authorship contribution statement
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.