
Abstract
Background
Workplaces can present ergonomic hazards, leading to musculoskeletal problems.
Objective
This study focused on ergonomic risks and musculoskeletal disorders experienced by nurses.
Methods
This was a descriptive study. The research was conducted between January and May 2023. The sample consisted of 537 nurses. Data were collected face-to-face using a personal information form, the Questionnaire Survey of Ergonomic Risks Among Nursing Workers-TR (ErgoEnf-TR), and the Nordic Musculoskeletal Questionnaire (NMQ).
Results
Participants had a mean ErgoEnf-TR “biomechanical factors,” “environmental factors/workplace,” and “organizational and psychosocial factors” subscale score of 71.89 ± 22.48, 56.74 ± 28.33, and 67.10 ± 25.48, respectively. Participants working night and day/night shifts had a significantly higher mean ErgoEnf-TR score than those working day shifts. Participants who could not take breaks had a significantly higher mean ErgoEnf-TR score than those who could. Participants who did not adhere to the principles of body mechanics had a significantly higher mean ErgoEnf-TR score than those who did. Participants who did not exercise regularly had a significantly higher mean ErgoEnf-TR score than those who did. The ergonomic risks included musculoskeletal disorders in the lower back, back, neck, and shoulders. Furthermore, ergonomic risk increased by one unit in the presence of biomechanical, environmental, organizational, and psychosocial factors.
Conclusion
Individual characteristics and workplace factors put nurses at an increased risk for musculoskeletal problems. Working style, rest status, work stress, compliance with the principles of body mechanics, regular exercise, and pain status affect nurses’ ergonomic risk scores.
Keywords
Introduction
Ergonomics refers to achieving harmony between work and human capabilities. To ensure occupational health and safety, it is crucial to identify risk factors present in workplaces. 1 We must provide nurses with ergonomic working environments to ensure that they can deliver quality care. 2 Nursing is a high-stress profession due to inherent workplace risks and demanding workloads. Nurses face diverse ergonomic risks stemming from movements that strain their body posture, repetitive and improper motions leading to trauma, and disproportionate or unsuitable utilization of various body parts. 3 Furthermore, psychosocial stressors within the workplace disrupt the physiological functioning of the musculoskeletal system, contributing to the likelihood of injuries. 4
Ergonomic risks can cause musculoskeletal issues, which rank among the most significant occupational health concerns. Musculoskeletal disorders significantly impact people's social, functional, and economic independence. 5 Depending on the nature of care and treatment, nurses face many health problems, the most common of which are musculoskeletal disorders.6–8 The International Council of Nurses (ICN) acknowledges the workplace of nurses as one of the most hazardous occupational settings involving risks such as occupational injuries and diseases. 9 The most prevalent musculoskeletal health issues among nurses include pain in the lower back, neck, shoulders, and upper back.10–15
Nurses encounter challenges like heavy workloads, shift work,16,17 prolonged standing, 18 musculoskeletal injuries, 19 fatigue, inadequate access to materials and tools, staffing shortages, infection risks, 20 insufficient lighting, noise, radiation exposure, and instances of violent behavior. 21 Furthermore, factors like obesity and early mobilization can contribute to musculoskeletal disorders in nurses, particularly affecting the shoulders and upper extremities.22,23 Muthukrishnan and Ahmad (2021) found that 24% of nurses were exposed to low risk and 76% to moderate risk during the repositioning of patients. They also reported a significant association between nursing-specific risk exposure scores, ergonomic risk factors and prevalence of musculoskeletal disorders. 24
Nurses experiencing musculoskeletal disorders often exhibit reduced quality of life, productivity, and work performance. Musculoskeletal disorders impose a financial burden attributable to costs linked with nurses’ sick leave stemming from musculoskeletal pain.25,26 All these risk factors are associated with musculoskeletal disorders. Nursing, by its very nature, is directly related to human life, and therefore, there is no room for error.4,27 Moreover, this contributes to a rise in occupational accidents, directly exposing caregivers to risks.3,4
Recent evidence highlights that work-related musculoskeletal disorders are highly prevalent among nurses worldwide. Systematic reviews and meta-analyses report that more than 30% of nurses experience work-related musculoskeletal disorders in most body regions, 28 and overall prevalence rates often exceed 70–80% across different countries.29,30 In addition to physical workload, psychosocial factors—including job strain, inadequate staffing, and time pressure—have been linked to increased work-related musculoskeletal disorders risk.31–33 These findings underline the global significance of the problem and support the need for research in different clinical contexts.
Preventing musculoskeletal disorders and minimizing ergonomic risks play a vital role in bolstering nurses’ morale, motivation, and work performance, enabling them to safeguard their health throughout their professional careers. Individual characteristics, stressors, working conditions, and adherence to the principles of body mechanics influence ergonomic risks. Nurses need optimum ergonomic conditions to reduce ergonomic risks and musculoskeletal disorders. Identifying musculoskeletal and ergonomic risks enables us to safeguard nurses from harm, facilitating the prompt implementation of treatment protocols and discovering effective solutions to these issues. Therefore, this study aimed to achieve two objectives: 1- identifying the ergonomic risks and musculoskeletal disorders to which nurses are exposed and 2- uncovering the factors influencing various body parts. In this study, we sought to answer several important questions regarding the occupational health of nurses. What are the ergonomic risks for nurses? What musculoskeletal disorders do nurses suffer from? Do ergonomic risks affect musculoskeletal disorders?
Methods
Design
This was a descriptive and correlational study.
Setting
The research was conducted in two hospitals in the Central Anatolia Region of Türkiye.
Population and sample
The study population consisted of 4584 nurses. The target sample consisted of 550 volunteers. However, thirteen nurses were excluded from the study because they could not complete the data collection form. Therefore, the final sample consisted of 537 participants. With a known population size of N = 4584, a finite population correction was applied. Assuming 95% confidence (Z = 1.96), p = 0.5, and a margin of error of ±4%, the required sample size is approximately 531. Our final sample of 537 therefore, meets the required sample size.
Inclusion criteria: Volunteering, Being a nurse
Exclusion criteria: Declining to participate, Having disorders for pre-occupational or non-occupational reasons, Withdrawing, Failing to fill out the data collection form
Data collection
The data were collected using a personal information form, the Questionnaire Survey of Ergonomic Risks Among Nursing Workers-TR (ErgoEnf-TR), and the Nordic Musculoskeletal Questionnaire (NMQ).
Personal Information Form
The personal information form was developed by the researchers.4,34,35
Questionnaire Survey of Ergonomic Risks Among Nursing Workers-TR (ErgoEnf-TR)
The Questionnaire Survey of Ergonomic Risks Among Nursing Workers-TR (ErgoEnf-TR) was developed by Coluci and Alexandre (2014) 4 and adapted to Turkish by Ercan et al. (2021). 34 The survey consists of 32 items and three subscales: biomechanical factors (nine items), environmental factors/workplace (seven items), and organizational and psychosocial factors (16 items). Each subscale is scored individually. Higher scores indicate more ergonomic risks. The Turkish version has a Cronbach's alpha score of 0.970, 34 which was 0.969 in the present study.
Nordic Musculoskeletal Questionnaire
The original Nordic Musculoskeletal Questionnaire (NMQ) was developed by by Kuorinka et al. (1987); in this study we used the extended version (NMQ-E) by Dawson et al. (2009) 36 and adapted to Turkish by Kahraman et al. (2016). 37 The questionnaire has two functions. First, it measures the amount of activity avoidance. Second, it assesses musculoskeletal pain in nine body areas (neck, shoulders, upper back, elbows, wrists/hands, lower back, hips/thighs, knees, and ankles/feet). It illustrates the body parts in question on a body manikin. The boundaries of the areas are not strictly defined. The respondent decides on which area they have or had pain. The questionnaire poses six questions: (1) Have you had trouble in those body areas at any time during the last 12 months? (2) Have you been prevented from doing your normal work because of the trouble at any time during the last 12 months? (3) Have you had trouble at any time during the last seven days?, (4) Have you ever hurt your body part in an accident? (5) What is the total length of time that you have had trouble during the last 12 months? (6) Have you been seen by a doctor because of the trouble during the last 12 months? The result expresses the parameters, such as discomfort (pain, soreness, etc.) and inhibition of activities, as a percentage. 37 The Turkish version has a Cronbach's alpha score of 0.896, 37 which was 0.905 in the present study.
Procedure
All nurses were briefed on the research purpose and procedure. Informed consent was obtained from those who agreed to participate in the study. The data were collected face-to-face between January and May 2023. All participants were handed the data collection form, which they filled out and submitted at the end of the workday. It took each participant 10–15 min to fill out the questionnaire.
Data analysis
The data were analyzed using the Statistical Package for Social Sciences (SPSS, IBM Corp., Armonk, NY, USA, version 20) at a significance level of 0.05. Descriptive statistics (number, percentage, mean, median, and min and max) were used for demographic data. The Mann-Whitney U test was used to compare two independent groups, while the Kruskall-Wallis test was used to compare more than two independent groups. Spearman's correlation analysis was performed. Logistic regression analysis was used to identify risks. “Uni” refers to univariable models and “Multi” to multivariable models.
Ethical considerations
The ethics committee approved the study (Date: 11.01.2022 & No: 01). Permission was obtained from the hospitals. All nurses were briefed on the research purpose and procedure. Informed consent was obtained from those who agreed to participate in the study.
Results
Participants had a mean of 31.06 ± 7.78 years of age and a mean of 65.38 ± 12.59 kg of weight. The mean BMI value of nurses was determined to be 23.76 ± 3.86 (16.26–40.15). They had over eight years of work experience and worked 51.58 ± 13.64 h weekly. Most participants were women (84.4%). Half of the participants were married (50.1%). More than half of the participants had no children (67.4%). The majority of the participants were right-handed (91.6%). Most participants had bachelor's degrees (86.4%). More than half of the participants worked for intensive care units (ICUs) (52.1%). Over half of the participants worked in shifts (63.7%). More than half of the participants could take breaks during work hours (57.9%). Most participants experienced work-related stress (89.6%). The majority of the participants could not keep their bodies in the right position while working (82.9%). Most participants did not exercise regularly (83.8%). More than half of the participants had no musculoskeletal problems (60.1%). Most participants had musculoskeletal pain (85.8%). More than a quarter of the participants reported physical strain during repositioning (28.3%) (Table 1).
Demographic characteristics (n = 537).
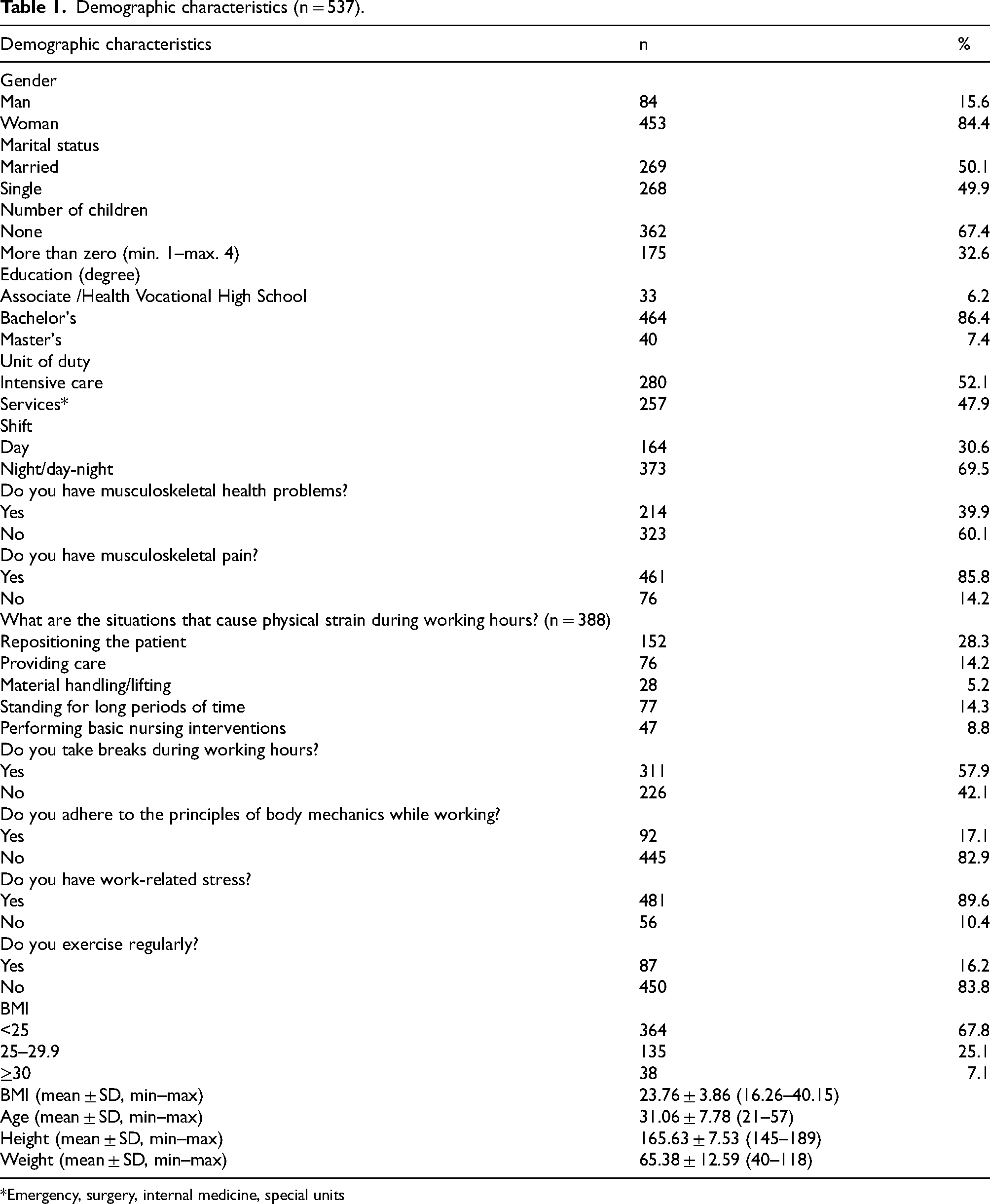
*Emergency, surgery, internal medicine, special units
Participants had a mean ErgoEnf-TR “biomechanical factors,” “environmental factors/workplace,” and “organizational and psychosocial factors” subscale score of 71.89 ± 22.48, 56.74 ± 28.33, and 67.10 ± 25.48, respectively (Table 2). Participants who worked nights had significantly higher mean ErgoEnf-TR subscale scores than those who worked shifts (p < 0.05). Participants who could not take breaks during work hours had significantly higher mean biomechanical, environmental, organizational, and psychosocial risk scores than those who could (p < 0.05). Participants who had work stress had significantly higher mean ErgoEnf-TR subscale scores than those who did not (p < 0.05). Participants who did not adhere to the principles of body mechanics while working had significantly higher mean ErgoEnf-TR subscale scores than those who did (p < 0.05). Participants who did not exercise regularly had significantly higher mean ErgoEnf-TR subscale scores than those who did (p < 0.05). Participants who had musculoskeletal pain had significantly higher mean ErgoEnf-TR subscale scores than those who did not (p < 0.05).
The distribution of ErgoEnf-TR subscale scores by some demographic characteristics.
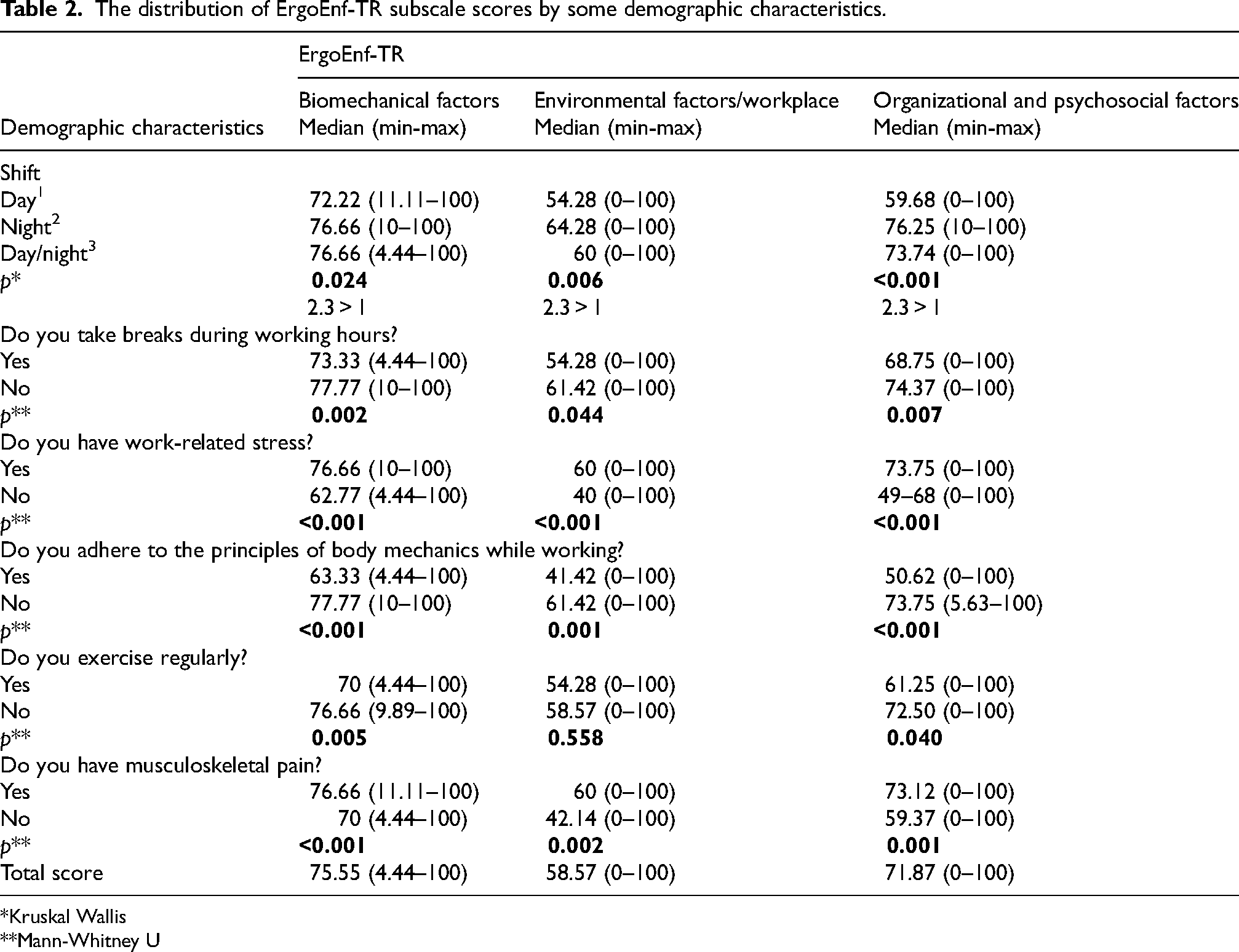
*Kruskal Wallis
**Mann-Whitney U
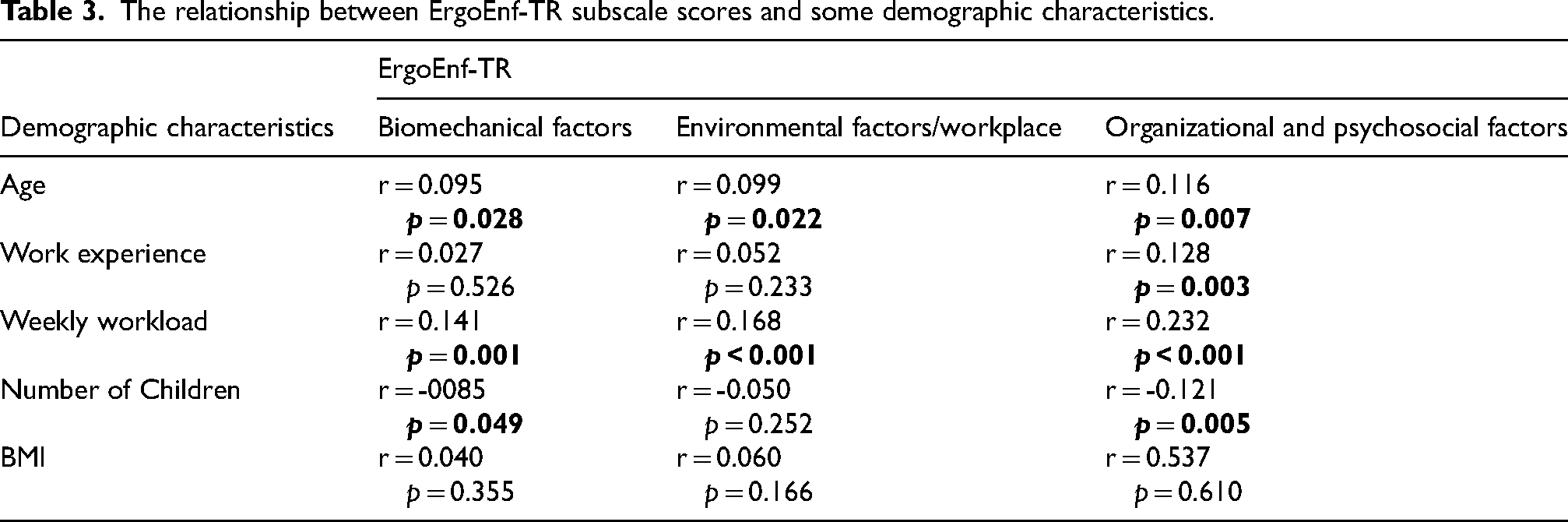
There was a weak positive correlation between age and biomechanical, organizational, and psychosocial factors. There was a weak positive correlation between weekly workload and biomechanical, organizational, and psychosocial factors. There was a weak positive correlation between work experience and organizational and psychosocial factors. No significant correlation was found between nurses’ BMI averages and ErgoEnf-TR scores (Table 3).
The relationship between ErgoEnf-TR subscale scores and some demographic characteristics.
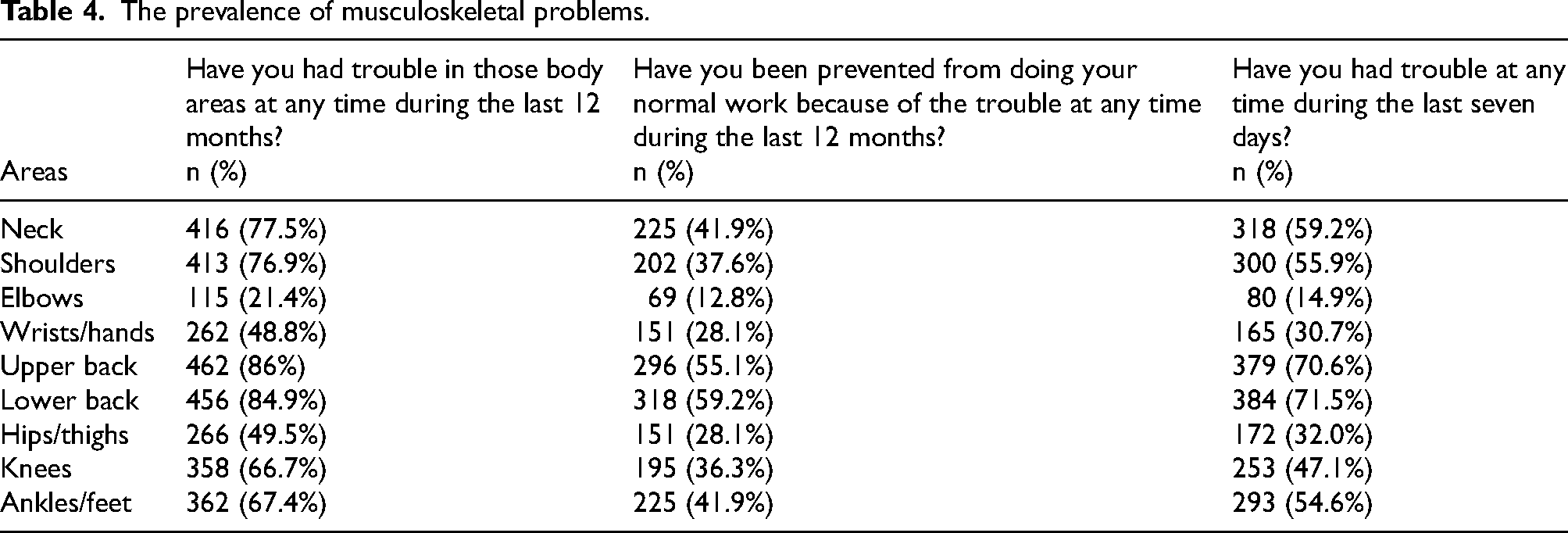
Most participants reported upper back pain in the last 12 months (86%). More than half of the participants reported that the upper back pain they experienced prevented them from doing their normal work at any time during the last 12 months (55.1%). More than half of the participants reported upper back pain during the last seven days (70.6%). Most participants reported lower back pain in the last 12 months (84.9%). More than half of the participants reported that the lower back pain they experienced prevented them from doing their normal work at any time during the last 12 months (59.2%). More than half of the participants reported lower back pain during the last seven days (71.5%). Most participants reported neck pain in the last 12 months (77.5%). Less than half of the participants reported that the neck pain they experienced prevented them from doing their normal work at any time during the last 12 months (41.9%). More than half of the participants reported neck pain during the last seven days (59.2%). (Table 4).
The prevalence of musculoskeletal problems.
As biomechanical factors increased, the risk of discomfort in the elbow area increased 1.019 times (p = 0.015). The correct classification rate was 81.7%. As organizational and psychosocial factors increased, the risk of back discomfort increased 1.025 times (p = 0.002). As organizational and psychosocial factors increased, the risk of lower back discomfort increased 1.026 times (10 odds ratios per 10-point increase) (p = 0.001). As organizational and psychosocial factors increased, the risk of knee discomfort increased 1.016 times (p = 0.011). As organizational and psychosocial factors increased, the risk of discomfort in the ankles and feet increased 1.015 times (0.017). 10 odds ratios per 10-point increase. The correct classification rate ranged between 66.7% and 86%. According to the logistic regression model, when all factors were evaluated separately, it was determined that risks would significantly affect all areas (Table 5).
Logistic regression analysis ErgoEnf-TR score by some variables.
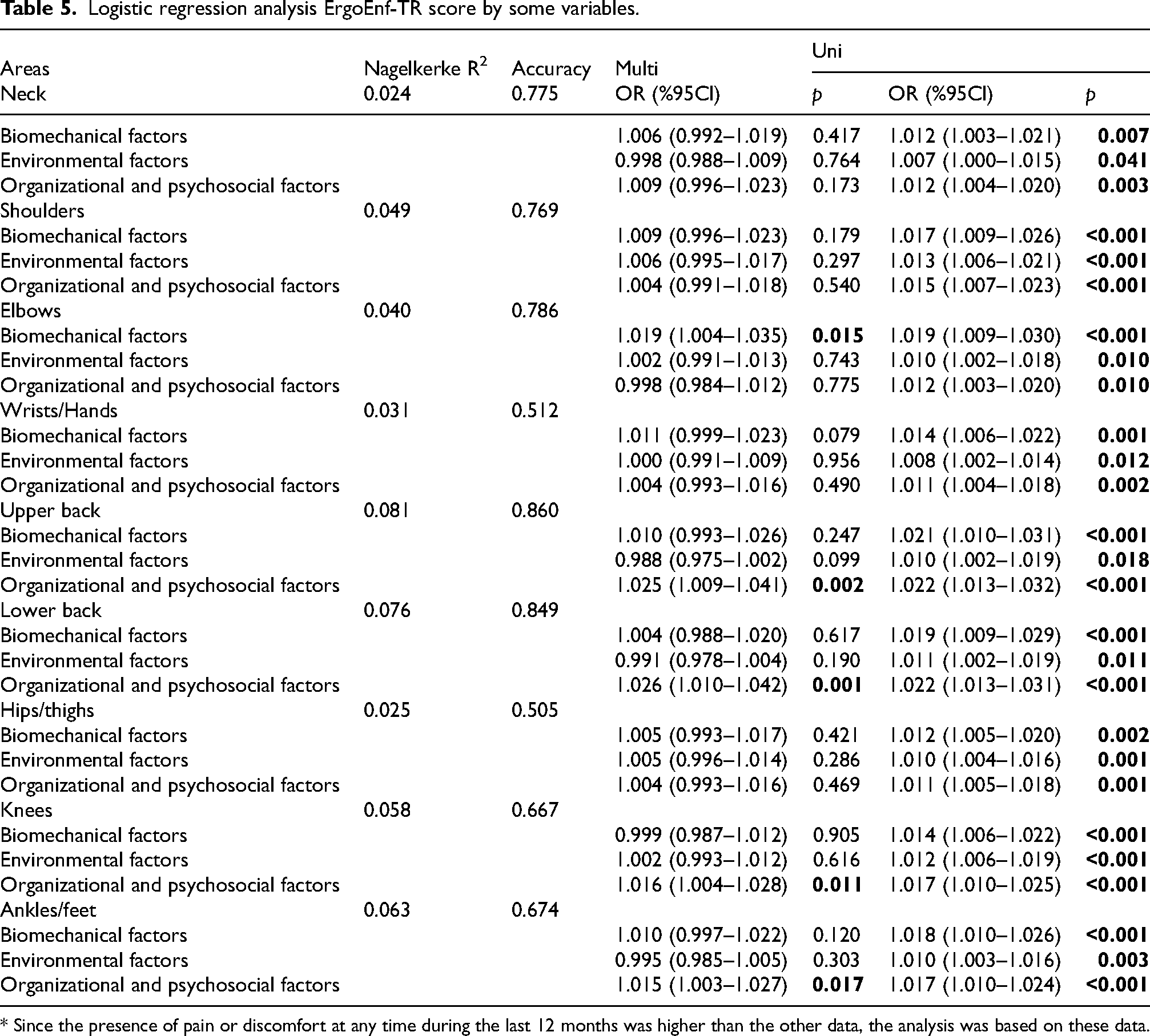
* Since the presence of pain or discomfort at any time during the last 12 months was higher than the other data, the analysis was based on these data.
No statistically significant difference was found between the ErgoEnf-TR Subscale Scores of the nurses in terms of gender, BMI and the clinic they work in (Table 6).
Differences between ErgoEnf-TR subscale scores according to some demographic characteristics.
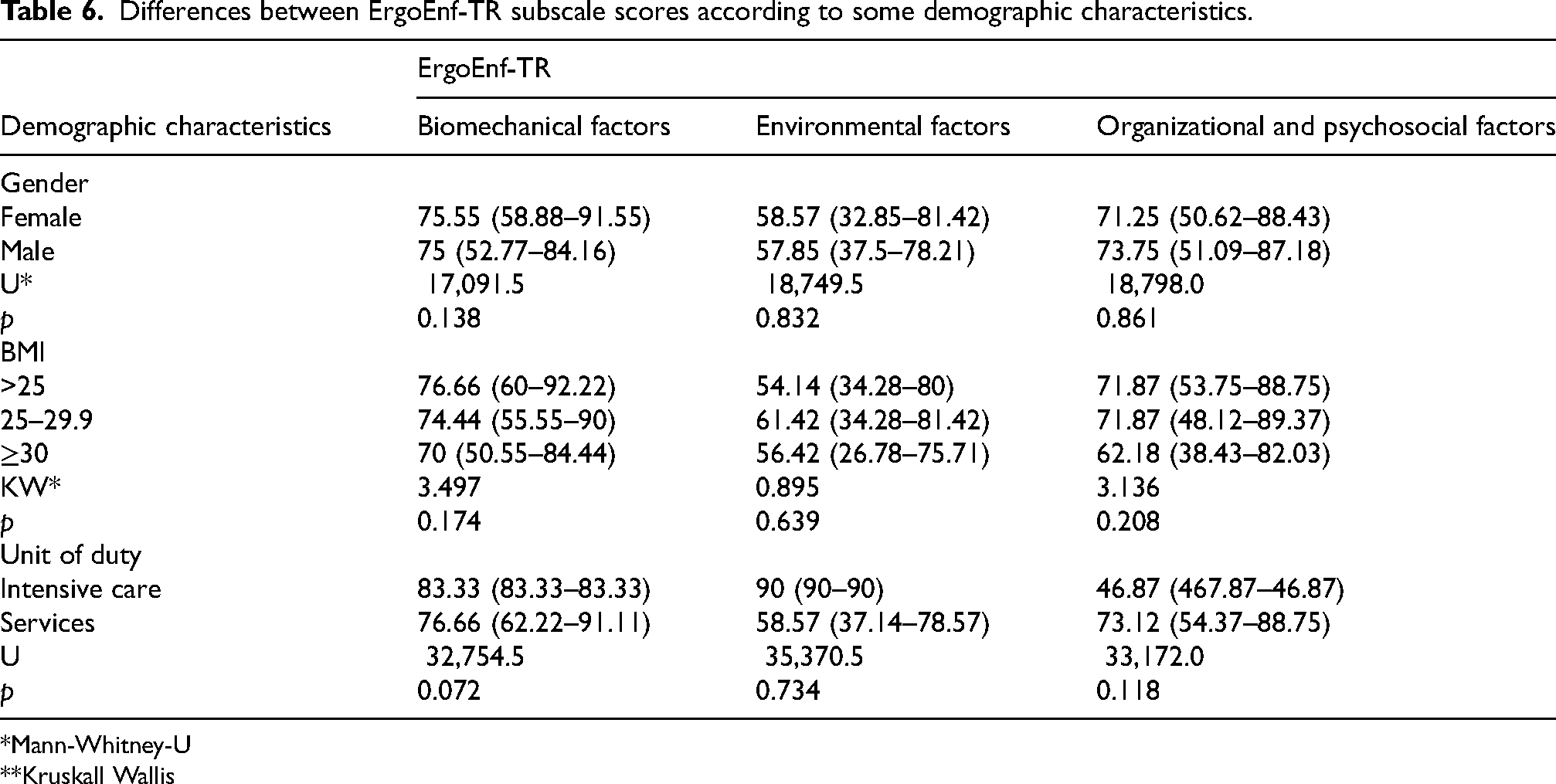
*Mann-Whitney-U
**Kruskall Wallis
Discussion
This study investigated the ergonomic risks and musculoskeletal problems experienced by nurses from the perspective of individual characteristics, stress, working conditions, and body mechanics. The study identified the areas where nurses experience musculoskeletal problems due to risk factors. In other words, unlike earlier studies, this study made a significant contribution to the literature by determining what body parts are affected by ergonomic risks.
Two out of five participants had musculoskeletal problems (39.9%). The prevalence of musculoskeletal problems among nurses ranges from 22.2% to 88.8%. Furthermore, musculoskeletal problems are more common in female nurses 30–39 years of age.14,15 Geçer and Kumsar (2024) determined that almost one out of every five nurses had a musculoskeletal disease. They also reported that the top three movements that negatively affected the musculoskeletal system were repositioning patients (42.2%), pulling them up (21.1%), and giving them care. 38 Our sample also consisted of female nurses of the same age group. Low education levels, high BMI levels, long working hours, and unhealthy lifestyles also predict musculoskeletal problems. 11
Our results showed that ergonomic risks were weakly associated with age, work experience, and weekly workload. Lin et al. (2020) found that nurses aged 50 years and older experienced more upper back discomfort compared to those aged under 30 years. 39 They also reported that nurses with more than ten years of work experience had more upper back discomfort than those with one year of work experience. Research also shows a positive correlation between prevalence of musculoskeletal problems and age and work experience.13,40
The results showed that heightened work stress and low adherence to the principles of body mechanics were associated with ergonomic risks. Research also shows that one out of five nurses suffer from musculoskeletal disorders due to inappropriate body postures 10 and heightened work stress. 41 Participants who worked nights and shifts had significantly higher musculoskeletal disorder risk scores than those who worked daytime. Participants who could not take breaks during work hours had significantly higher musculoskeletal disorder risk scores than those who could. Participants who did not exercise regularly had significantly higher musculoskeletal disorder risk scores than those who did. Participants who had musculoskeletal pain had significantly higher musculoskeletal disorder risk scores than those who did not. Ayaz and Doğan (2015) reported that only three out of ten nurses exercised regularly. 42
Research shows that nurses using heavy equipment and standing for long periods of time also have more musculoskeletal problems.10,14,43 Our participants had high risk scores for three reasons. First, most participants did not do regular exercise. Second, most participants experienced musculoskeletal pain. Third, almost half of the participants could not take breaks during work hours.
Pain is the most important indicator of musculoskeletal problems. 10 Nurses in pain find it difficult to perform basic interventions, which negatively affects care outcomes. Our results show that four out of five nurses experience musculoskeletal pain, preventing them from performing nursing interventions. They reported physical strain while providing care and positioning patients. Yılmaz and Andsoy (2022) also found that nurses who were constantly on their feet providing care for long periods, carrying heavy loads, making sudden movements, and accompanying patient transfers experienced high levels of pain. 15 Tang et al. (2022) indicated that spending time in awkward postures, manual handling of materials, and sustained squatting postures contributed to increased ergonomic risks. 44
Our results show that nurses do not adhere to the principles of body mechanics while working, which may be due to a lack of information and attitudes. Gilchrist and Pokorná (2021) demonstrated that nurses lack adequate knowledge regarding manual handling techniques and the proper use of lifting tools. 10 Nurses who do not adhere to the principles of body mechanics during care are more likely to encounter musculoskeletal disorders. During their undergraduate years, nurses learn how to protect themselves from musculoskeletal problems. Nonetheless, nurses may struggle to adopt appropriate behaviors in this context due to biomechanical, environmental, organizational, and psychosocial factors, ultimately contributing to their musculoskeletal issues.
Most of our participants reported that they had been experiencing lower back, upper back, and neck pain in the last 12 months and in the last seven days. They added that the pain they experienced prevented them from performing domestic and professional tasks. These results are consistent with the literature.10–15,35,45 Clari et al. (2021) stated that the most common areas where nurses experience work-related musculoskeletal problems are the waist, knee, shoulder, neck, ankles, back, wrist, and elbow, respectively. 46 Soroush et al. (2018) also reported that nurses experience musculoskeletal problems in the back, neck, knees, upper back, ankles, shoulders, hands, hips, thighs, and elbows, respectively. 47 All in all, research shows that the top three areas where most nurses experience musculoskeletal problems are the lower back, upper back, and shoulders.
Participants had a mean ErgoEnf-TR “biomechanical factors,” “organizational and psychosocial factors,” and “environmental factors/workplace” subscale score of 71.89 ± 22.48, 67.10 ± 25.48, and 56.74 ± 28.33, respectively. Furthermore, their subscale scores were above the average. Muthukrishnan and Ahmad (2021) found that nurses’ ergonomic risk scores were moderate, indicating a level of risk sufficient to lead to musculoskeletal disorders. 24 Canbulut et al. (2022) reported that individuals experiencing pain had significantly high biomechanical, organizational, and psychosocial factor scores. 3
The present findings show that nurses working night or rotating shifts, those unable to take breaks, those experiencing work-related stress, and those not adhering to body mechanics principles had significantly higher ergonomic risk scores, which is consistent with international evidence. Systematic reviews have shown that the prevalence of work-related musculoskeletal disorders exceeds 70–80% in many countries, with the lower back, neck, shoulders, and upper back repeatedly identified as the most affected regions.28–30 Studies from Europe, Asia, and perioperative settings similarly indicate that prolonged standing, awkward postures, high patient-handling demands, and irregular work schedules contribute to increased musculoskeletal strain.46,48 In addition, psychosocial risks such as job strain, inadequate staffing, and time pressure have been linked to upper-body musculoskeletal disorders, supporting our findings related to stress and lack of rest breaks.31–33 These international comparisons suggest that ergonomic risks among nurses are shaped by a combination of demographic factors, biomechanical load, environmental conditions, and organisational structure, and that these patterns are consistent across continents.
Our logistic regression analysis results showed that participants had high ergonomic risks. In particular, biomechanical factors (standing, bending, carrying equipment, working above physical capacity and at a fast pace) had an adverse impact on elbows. Our results showed that organizational and psychosocial factors (working hours, shifts, understaffing, time and supervisor pressure, inexperience, and lack of autonomy) increased musculoskeletal problems in the upper back, lower back, knees, and ankles. Our findings also indicated that environmental factors such as ambient temperature, noise, lighting, and equipment use contributed to an increased likelihood of experiencing musculoskeletal problems. As this study is cross-sectional and descriptive, causal relationships cannot be established; therefore, the results should be interpreted as associations rather than cause-and-effect relationships.
Data heterogeneity represents a recurring challenge in ergonomic and musculoskeletal research. In this study, differences in units, workloads, and work patterns may have contributed to variability in both exposures and outcomes. While such heterogeneity reflects real practice conditions, it may also reduce analytical precision. Future research should consider strategies such as stratification or multilevel modelling to better account for these variations.
Limitations
This study has five limitations. First, the findings are sample-specific and cannot be generalized to all nurses. Second, no lower and upper limits for age and weight were specified. Third, nurses from different units were recruited; therefore, they may have been exposed to different conditions. Fourth, some participants worked in shifts, while others worked without shifts. Fifth, data were collected from only two hospitals, and potential clustering effects were not accounted for. Future research should consider employing multi-level models or clustering adjustments to address possible intra-hospital correlations, which could provide more robust and generalizable findings.
Additionally, the cross-sectional design limits causal inference, preventing the establishment of temporal relationships between ergonomic risks and musculoskeletal disorders. All measures relied on self-reported data, which may be subject to recall bias and social desirability bias.
Conclusion
Individual characteristics and workplace-related factors make nurses more vulnerable to musculoskeletal disorders. Age, work experience, workloads, heavy shifts, work-related stress, lack of breaks, inappropriate postures, lack of exercise, musculoskeletal problems, and pain status also make nurses more open to ergonomic risks. Biomechanical, environmental, organizational, and psychosocial factors also affect musculoskeletal problems. Most nurses experience mostly upper back, neck, and shoulder pain due to those factors. Therefore, hospitals should train nurses in musculoskeletal problems and encourage them to adhere to the principles of body mechanics while performing nursing interventions. Nurses should prioritize their physical health as these risks not only impact their performance but also influence patient care outcomes and overall well-being.
Footnotes
Acknowledgments
We would like to thank all participants for their interest and contributions to the study.
Ethical considerations
The ethics committee approved the study (2022 - 079). Permission was obtained from the hospitals. All nurses were briefed on the research purpose and procedure. Informed consent was obtained from those who agreed to participate in the study.
Informed consent
Written informed consent was obtained from all participating subjects
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.