
Abstract
Background
The increase in smartphone use can potentially have negative effects on individuals, affecting musculoskeletal, posture, and sensory functions. However, the impact of this increase on proprioception and dizziness/imbalance have not been sufficiently studied.
Objective
This study aims to examine the craniovertebral angle (CVA), cervical proprioception, static postural balance, and psychometric imbalance symptoms in individuals who use excessive smartphones.
Methods
This cross-sectional study included 105 participants divided into two groups based on their median Smartphone Addiction Scale (SAS) scores: high smartphone use (HSU) group (n = 53) and low smartphone use (LSU) group (n = 52). Participants’ CVA, cervical proprioception, static postural balance, and psychometric imbalance symptoms (Vertigo, Dizziness, Imbalance-Symptom Scale (VDI-SS)) were assessed.
Results
In the HSU group, CVA (Effect size (ES) = 0.28, p = 0.005) and VDI-SS scores were worse (ES = 0.79, p < 0.01), and flexion, extension, right rotation, left rotation, and right lateral flexion cervical proprioception deviation angles were statistically significantly higher than in the LSU group (p < 0.05). Static postural balance functions of the groups were similar (p > 0.05). Also, there was a negative correlation between SAS and CVA (r = -0.277, p = 0.004) and VDI-SS scores (r = -0.440, p < 0.001).
Conclusion
HSU is related to decreased CVA and worsening of proprioception and dizziness/imbalance symptoms in individuals. The similarity in static postural balance may indicate that postural changes due to HSU, even if not apparent early, may be associated with dizziness/imbalance symptoms. Consequently, it is thought that HSU may be associated with cervical posture, proprioceptive sensitivity, and balance control in the long term. This study is submitted to ClinicalTrial (no: NCT06968078).
Introduction
Smartphones enable various functions, such as browsing the internet, reading news, playing games, conducting research, and using social media, thereby making processes in education, healthcare, business, and social interaction faster and easier. 1 Therefore, the convenience offered by smartphones has led to widespread and excessive use, especially among young adults. In a large-scale epidemiological study conducted in Turkey in 2024, it was found that approximately one-quarter of the participants used smartphones for more than 4 h a day, and approximately one-third were in the risk group for smartphone addiction. 2 Smartphone addiction is the uncontrolled use of smartphones by individuals, which results in negative effects on both themselves and others. 3 These individuals are physiologically dependent on smartphones and experience tension and restlessness when they are not using them. 4 Furthermore, this addiction significantly affects individuals by being associated with musculoskeletal problems and pain. 5
Excessive smartphones use negatively affects physical health. The most well-known of these effects are blurred vision and postural problems that occur due to long-term use. 6 Smartphone users often exhibit forward-leaning and bent-neck posture because they hold the device below eye level for extended periods. This condition leads to cervical muscle tension, which can develop into forward head posture (FHP). 7 With FHP, the head is positioned in front of the body's center of gravity. It is estimated that the effective weight carried by the cervical spine at 60 degrees of head flexion reaches approximately 28 kg. 8 Therefore, FHP causes postural problems by straining the muscles, tendons, and ligaments that support the cervical spine9,10 These problems are associated with deterioration in postural control and performance-based balance. 11
Balance and functional movement depend on the integrated interaction of information from the visual, vestibular, and proprioceptive systems. 12 Excessive smartphone use may negatively affect single-task balance and cause dizziness. In the literature, the effects of excessive smartphone use on balance and dizziness have been explained by various mechanisms.7,13,14 Excessive smartphone use has been reported to affect the visual system, potentially leading to short-term balance disorders. 13 Additionally, excessive smartphone use can lead to FHP, impairing cervical proprioception and consequently negatively affecting balance. 7 Given the importance of cervical proprioception in perceiving the correct position of the head and maintaining trunk orientation, the FHP-imbalance hypothesis seems more plausible. There are increasing studies in literature supporting this relationship.7,15,16 However, these studies did not explain how changes in neck angle alter the risk of instability.
This study aimed to investigate the craniovertebral angle (CVA), cervical proprioception, static postural balance skills, and psychometric imbalance symptoms in individuals with excessive smartphone use. Additionally, it was aimed to evaluate the relationship between neck angle and static postural balance performance and dizziness symptoms. This study hypothesizes that high levels of smartphone use may be associated with an increase in CVA, worsening of neck proprioception and static postural balance parameters, and an increase in dizziness/imbalance symptoms.
Methods
Participants
This study was conducted on university students at Karabuk University Physiotherapy and Rehabilitation Application and Research Center between May and November 2025. University students over the age of 18 who volunteered were included in the study. Students with spinning vertigo (e.g., Meniere's disease), neurological, psychiatric, systemic, orthopedic, or cardiovascular diseases, and those experiencing acute/chronic neck pain were excluded from the study. As a result of these criteria, a total of 105 university students were included in the study. The study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the University Non-Interventional Ethics Committee (2024/1914). Written and verbal consent was obtained from the participants. This study was submitted to ClinicalTrials (no: NCT06968078).
Procedure and assessment tools
Participants’ demographic information, years of smartphone use, and purpose of use were recorded. In addition, smartphone usage times were recorded as morning (06:00–12:00), afternoon (12:00–18:00), evening (18:00–22:00), night (22:00–06:00), and all day (regular usage in multiple time periods throughout the day). 17 Subsequently, smartphone addiction, CVA, cervical proprioception, symptoms of dizziness/imbalance, and static postural balance were assessed.
Smartphone addiction scale
Participants’ attitudes towards smartphones were assessed with the Turkish version of the Smartphone Addiction Scale (SAS). 18 This scale, comprising 33 items in total, is scored on a scale of 1 to 6 for each item. The Cronbach's alpha internal consistency coefficient of the scale was found to be 0.947, indicating a high level of internal consistency. SAS does not have a clinically established cut-off value for determining smartphone addiction. Therefore, to determine relative addiction levels and ensure a balanced sample distribution, grouping was performed based on the median of the scale.4, 19 Accordingly, participants were divided into two different categories based on the median value of their SAS scores4,19: High smartphone use (HSU) and low smartphone use (LSU group).
Craniovertebral angle
FHP was evaluated using the CVA method. Participants were recorded standing, maintaining their natural posture, from the right sagittal plane, with a digital camera placed at shoulder level. Before photography, anatomical markers, the ear tragus, and the spinous process of the seventh cervical vertebra (C7) were marked. CVA was calculated as the angle between the horizontal reference line passing through C7 and the line extending from C7 to the tragus. 20 A lower CVA indicated a higher FHP. 21 Measurements were performed by the same evaluator using digital goniometer software (see: https://www.ginifab.com/feeds/angle_measurement/) to reduce inter-measurement variability (Figure 1).
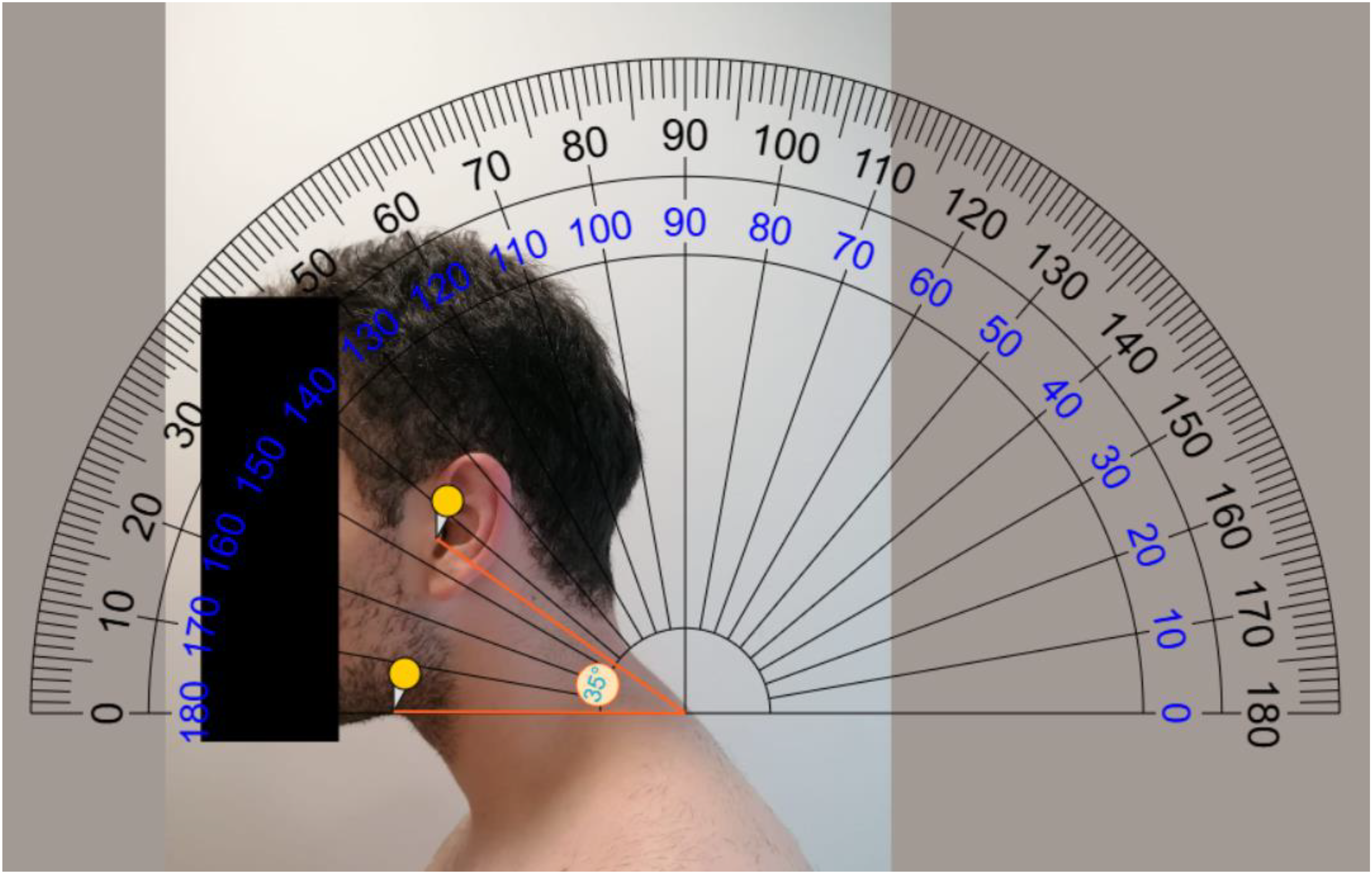
Measurement craniovertebral angle.
Evaluation of cervical proprioception
Cervical proprioception was performed using the Cervical Range of Motion (CROM, Baseline®) device. The 30-degree target angle was chosen because it represents a functional range of motion within the cervical joint and minimizes mechanical stress that could result from extremity movements. 22 To teach the test, participants were asked to perform 30° neck flexion, extension, left-right lateral flexion, and rotation with their eyes open, and to wait 3–5 s to perceive the angle. Then, their heads were brought to a neutral position. Participants were asked to position their heads at a 30° angle with their eyes closed and maintain this position for 3 s. The difference between the target position and the repositioned angle was recorded in degrees as the joint position error (JPE). Three trials were performed for each position, and the trials were averaged. Higher JPE values indicate decreased cervical proprioceptive accuracy. 22
Psychometric evaluation of dizziness and imbalance
The Turkish version of the Vertigo, Dizziness, Imbalance-Symptom Scale (VDI-SS) was used to assess Dizziness and Imbalance psychometrically. 23 The VDI-SS consists of 14 questions scored from 0 (always) to 5 (never), and the Cronbach's alpha internal consistency coefficient for the scale was found to be 0.85. A lower score on the scale indicates increased symptoms of dizziness/balance.
Balance assessment
Participants’ postural balance was assessed statically using a force platform (Bertec Corporation, Ohio, USA). Before starting the measurements, the stability area (SA) value of everyone on the firm floor was determined. For this purpose, the participants were asked to stand on the platform and move forward-backwards and right-left, respectively, in the maximum direction. Then, balance performance was recorded under four different conditions: eyes-open on a firm floor, eyes-closed on a firm floor, eyes-open on a foam floor, and eyes-closed on a foam floor. In all conditions, participants were asked to stand still in the specified position on the platform and maintain a fixed cursor on the computer screen static for 30 s. Both postural sway and stability limits (LoS) results were reported as percentages (%). 24
Statistical analysis
Statistical analysis of all data obtained from the study was performed using IBM SPSS Statistics 25.0 software. Based on the VDI-SS results obtained from the pilot study, which are the primary and clinically significant self-reported outcome of the study, we estimated that a sample size of at least 52 individuals in each group would have 80% power for an α value of 0.05 and an effect size of d = 0.56.
The normal distribution of continuous variables was assessed using the Shapiro-Wilk test. Normally distributed variables were presented as mean ± standard deviation (SD), and non-normally distributed variables were presented as median, minimum–maximum, and interquartile range [Q1–Q3]. Data showing normal and non-normal distribution were compared between groups using the Independent Samples T-test and the Mann-Whitney U test, respectively. Categorical variables were compared using the chi-square test. Relationships between continuous variables were analyzed using Pearson's correlation test for data with a normal distribution and Spearman's correlation test for data without a normal distribution. The correlation coefficients were r > 0.89 very strong correlation, 0.70–0.89 strong correlation, 0.40 to 0.69 moderate correlation, and 0.20–0.39 weak correlation. 25 Cohen's d effect size (ES) was categorized as small (0.21–0.49), moderate (0.50–0.79), or large (≥0.80). For non-parametric tests, effect size (r) was categorized as small (0.10–0.29), medium (0.30–0.49), or large (≥0.50). 26 A statistical significance level of p < 0.05 was accepted.
Results
The mean SAS score of the 105 participants included in the study was 89.49 ± 24.03, with a median value of 88 (46–154). According to the median value, participants were divided into two groups: the LSU group (SAS score<88) and the HSU group (SAS score≥88). Accordingly, 52 (49.5%) participants were in the LSU group, and 53 (50.5%) participants were in the HSU group. The mean SAS score of the LSU group was 70.42 ± 12.61, while the mean SAS score of the HSU group was 108.20 ± 16.68. Demographics and smartphone use characteristics by groups are presented in Table 1.
Comparison of demographic and smartphone use characteristics between LSU and HSU groups.
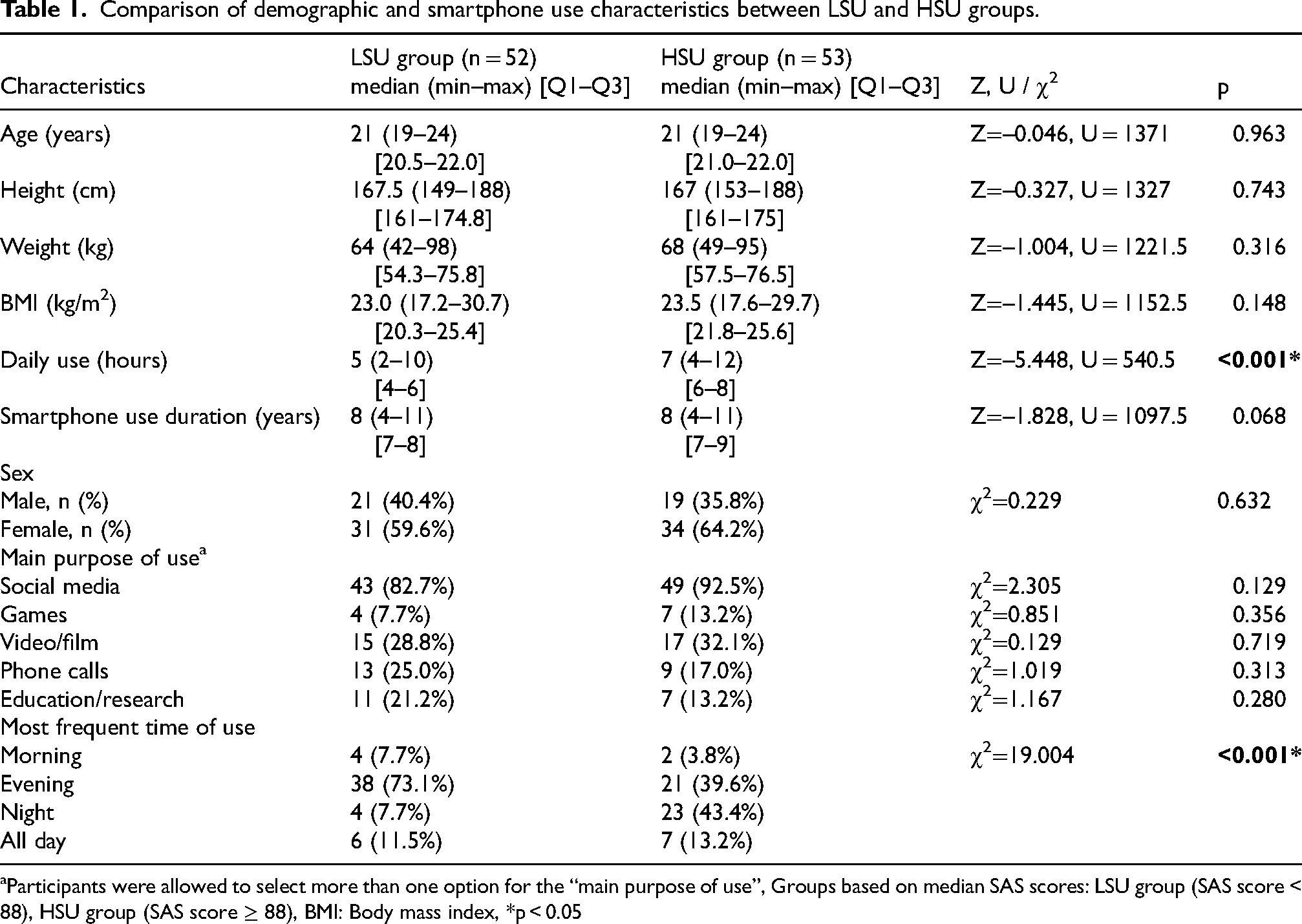
Participants were allowed to select more than one option for the “main purpose of use”, Groups based on median SAS scores: LSU group (SAS score < 88), HSU group (SAS score ≥ 88), BMI: Body mass index, *p < 0.05
The CVA was significantly lower in the HSU group compared to the LSU group (ES = 0.28, p = 0.005). Additionally, cervical proprioception sensitivity in flexion, extension, right rotation, left rotation, and right lateral flexion movements were weaker in the HSU group than in the LSU group (p < 0.05, Table 2).
Comparison of cervical proprioception measures between LSU and HSU groups.
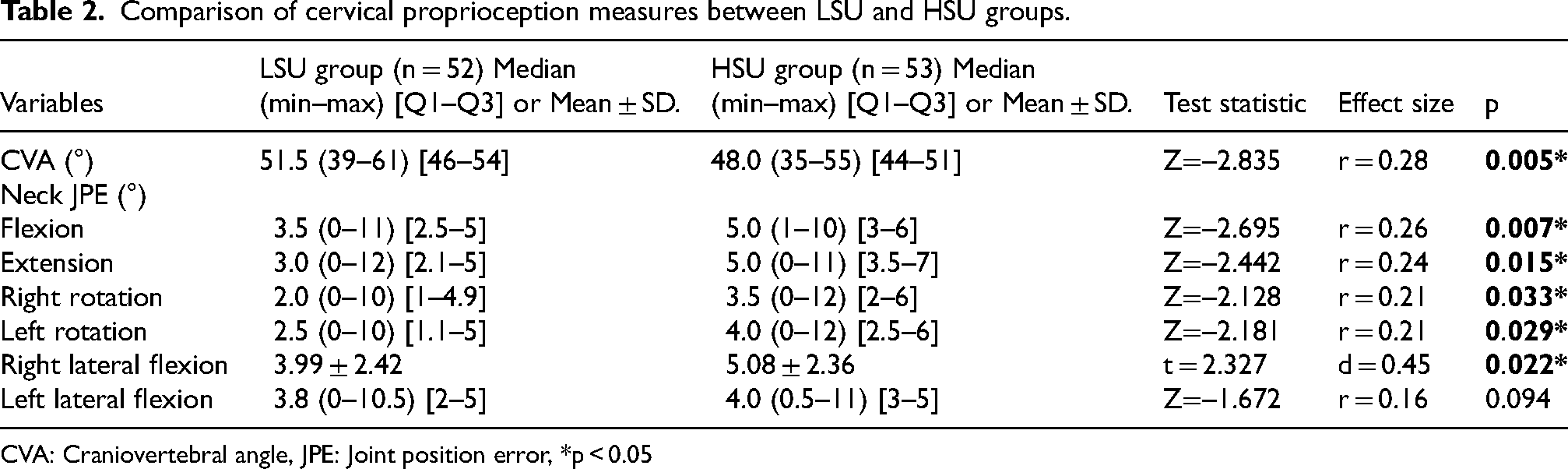
CVA: Craniovertebral angle, JPE: Joint position error, *p < 0.05
Individuals in the HSU group had worse VDI-SS scores than those in the LSU group (1-β= 96.9%, ES = 0.79, p < 0.01, Figure 2). The median value of VDI-SS was 61 (16–70), and the median value of CVA was 49 (31–61). According to risk assessment using the median value (49°), individuals with CVA <49° (n = 44) were found to be more likely to experience dizziness/loss of balance (OR = 2.56; 95% CI = 1.16–5.68). However, there was no difference between the groups in terms of LoS and other static postural balance skills (p > 0.05, Table 3).
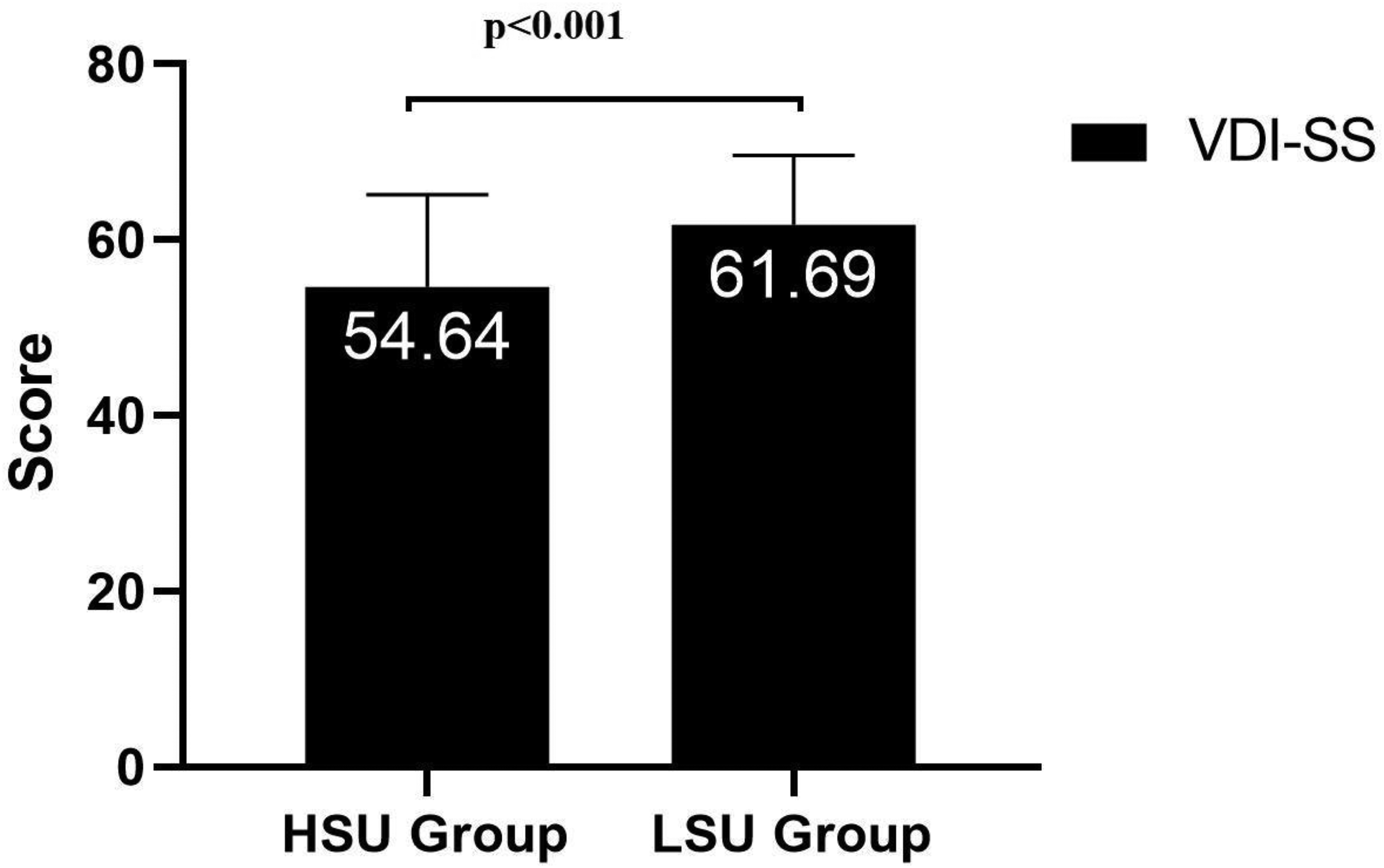
Comparison of VDI-SS scores of the groups.
Comparison of static postural balance variables according to groups.
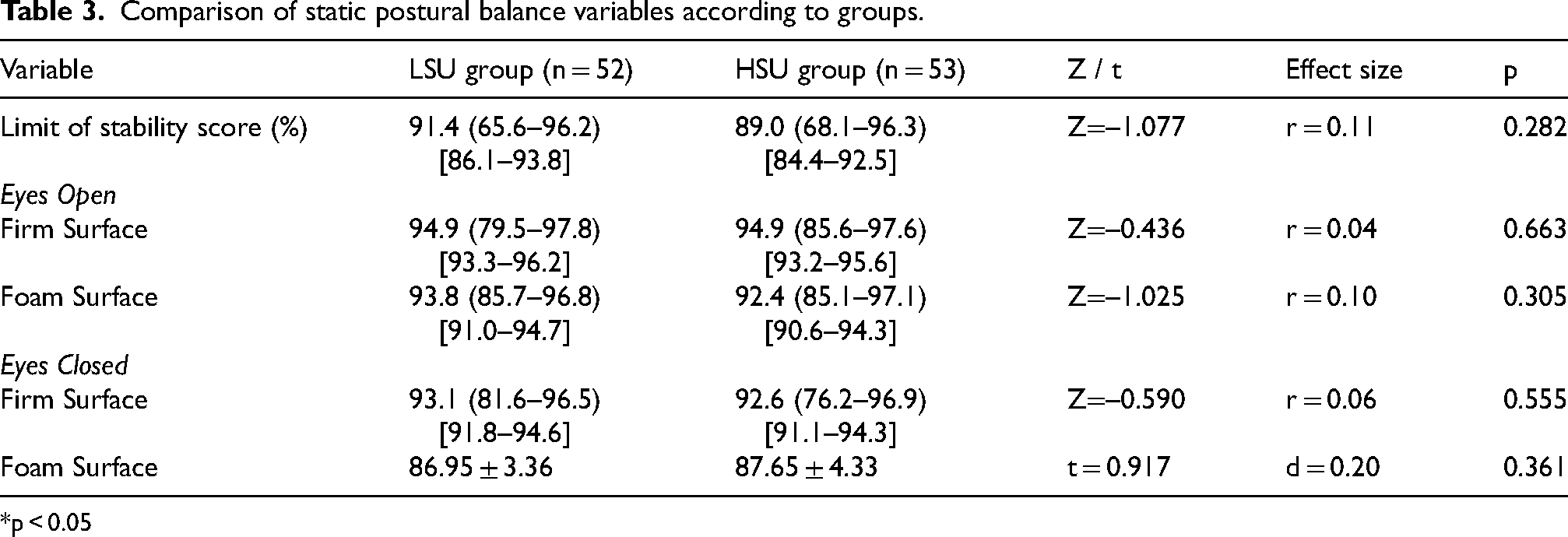
*p < 0.05
There was a negative correlation between SAS and CVA (r=–0.277, p = 0.004) and VDI-SS scores (r = -0.440, p < 0.001). CVA showed a positive correlation with VDI-SS (r = 0.281, p = 0.004). Similarly, CVA was significantly and negatively correlated with flexion JPE (r=–0.428, p < 0.001) and extension JPE (r=–0.365, p < 0.001, Figure 3). However, no significant relationship was found between cervical angle and right rotation (p = 0.208), left rotation (p = 0.326), and right lateral flexion (p = 0.399).
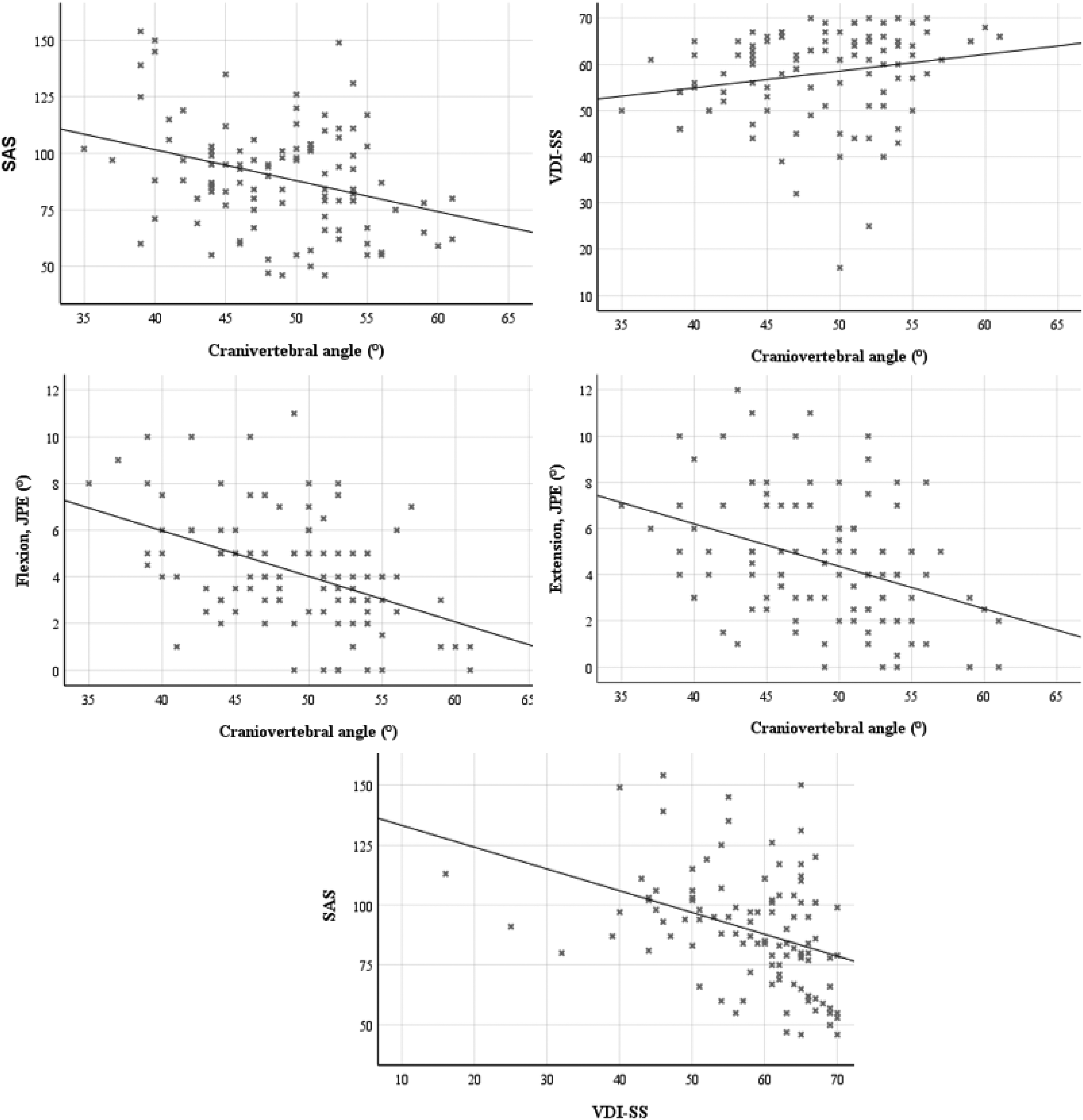
Relationship between craniovertebral angle and clinical parameters.
Discussion
This study demonstrated that HSU may be associated with a greater decrease in CVA, impaired neck proprioception, and increased symptoms of dizziness/imbalance in individuals. However, postural balance in static standing positions, as measured with the force platform, was similar between the groups.
The prevalence of FHP in university students has been reported to be between 66% and 81.8%.27,28 This high rate is attributed to the fact that students today remain inactive for longer periods and maintain static postures due to increasing academic demands. Reading books, carrying a backpack, using a computer, working while leaning forward at a desk, and adopting inappropriate sleeping positions are considered the primary factors contributing to the development of FHP.27,29 Recent studies have revealed that excessive smartphone use may also be associated with FHP and cervical proprioception impairment.21,30 Jung et al. 30 compared CVA between individuals using smartphones for more and less than four hours a day and reported that long-term smartphone use may cause FHP. Lee et al. 31 showed that as the severity of smartphone addiction increases, the deterioration in cervical proprioceptive sense also increases. During excessive smartphone use, individuals often keep their heads and necks in a forward-leaning position. As the head is tilted forward, the center of gravity shifts forward, which leads to overloading of the neck extensor muscles and disruption of the normal function of proprioceptive receptors.21,32 However, unlike these studies, Alshahrani et al. 15 reported that excessive smartphone use in university students did not significantly affect CVA but negatively affected cervical proprioception. It has been reported that the change in CVA may be related not only to the duration of phone use, but also to how the phone is used. They also stated that because the participants were university students, they frequently performed activities that required bending forward, such as reading, using computers, and writing, and that this might not have created an additional effect of smartphone use due to the already existing postural adaptation. 15
In the current study, the CVA value of the HSU group was found to be smaller than that of the LSU group, with a small effect size, and the JPE value was found to be higher. However, although there were differences between the CVA groups, the small effect size suggests that its clinical impact may be limited. However, differences between groups in CVA may indicate a possible link between excessive smartphone use and changes in posture. The weak association between SAS and CVA in the current study may also explain this situation. However, it should not be overlooked that the study's cross-sectional design prevents the establishment of a cause-and-effect relationship. Also, this relationship may be contributed to by postural changes resulting from the stress placed on the cervical region due to HSU. 21 Additionally, a moderate correlation was found between CVA and flexion–extension movements. The JPE is critical for the correct positioning of the head relative to the trunk, and an increase in deviation reflects a deterioration in afferent signals from the neck, which is interpreted as an impairment of cervical proprioception. 21 Therefore, the increase in JPE observed in the HSU group suggests that HSU may be associated with decreased cervical control and impaired sensitivity in the proprioceptive system, and this impairment may be related to excessive smartphone use. Given these results, it should be considered that decreased FHP and sensory feedback can lead to declines in both academic and work performance, as well as injuries.
Smartphone addiction can affect how and when individuals use smartphones. In this study, individuals from HSU tended to use their smartphones more at night, while those from LSU tended to use their smartphones more in the evening. It is known that phone use at night typically occurs while lying down on one's back, or on one's side. 17 Therefore, as stated by Alshahrani et al. 15 how and in which position the smartphone is used may be a determining factor on CVA. However, this study did not investigate the most common position in which smartphones were used. This may have prevented a detailed assessment of postural effects related to smartphone use by position.
The cervical region plays a critical role in balance control through both the proprioceptive senses it provides and the vestibulo-colic reflexes. 33 Some studies have examined the effects of excessive smartphone use and CVA changes on postural stability.15,16 Alshahrani et al. 15 reported that excessive smartphone use negatively affects dynamic postural balance skills by deteriorating neck proprioception. Tapanya et al. 7 reported that the postural stability of individuals with FHP, especially on a foam floor, was significantly lower compared to the control group. Wah et al. 16 reported that using a smartphone for more than 4 years and for more than 4 h a day, and having a Neck Disability Index score of ≥7, poses a serious risk for static balance disorder. The present study revealed that individuals with HSU and LSU exhibited similar postural sway and static balance performance. The difference between our study and other studies7,16 may be due to participant characteristics. This study included individuals who reported no active neck pain or clinical symptoms. Therefore, although individuals in the HSU group were negatively affected by CVA and JPE, the effect sizes were small, and thus, the changes in CVA and JPE may not have been significant enough to disrupt static postural balance. This result supports the hypothesis of Wah et al. 16 namely, that static balance impairment may become evident in the presence of clinical symptoms. Therefore, it should be considered that static postural balance assessments may have limited sensitivity in detecting mild or early balance changes in asymptomatic individuals. Furthermore, increased dizziness/imbalance in individuals with HSU suggests that possible postural balance effects may reflect subtle changes in balance control that are more likely to be revealed by task-oriented or dynamic balance tests.
Although biomechanical measurement methods are used to assess balance objectively, balance control cannot be explained solely by mechanical parameters. Balance control requires the simultaneous functioning of multiple sensory systems and the consistent interpretation of information from these systems at a central level. 34 Therefore, evaluating these neurosensory processes with psychometric assessment methods is crucial for detecting disorders that are not reflected in biomechanical parameters or compensated for by the musculoskeletal system. In the present study, the severity of symptoms related to dizziness and imbalance, as well as their impact on daily life, were evaluated using the VDI-SS. 23 This study showed that individuals in the HSU group had more dizziness/imbalance symptoms, with a moderate effect size, compared to those in the LSU group.
Several studies have shown that excessive smartphone use can lead to increased feelings of dizziness and imbalance.14,35 However, this relationship has not yet been clearly established. In a large cross-sectional study (682 individuals), individuals with HSU reported more symptoms of dizziness and imbalance compared to individuals with LSU. 14 Similarly, Lee et al. 35 stated that using a smartphone-based virtual reality system for more than 20 min can cause dizziness/imbalance in individuals. Similarly, in this study, individuals in the HSU group had increased dizziness/imbalance symptoms compared to the LSU group. Additionally, it has been stated that these symptoms may result from sensory conflict between the visual and vestibular systems. 35 In this context, the current study has demonstrated that an increase in CVA is associated with a decrease in symptoms of dizziness/imbalance. Furthermore, individuals were grouped according to the median value of CVA, as HSU and imbalance may also be related to CVA. Thus, the present study showed that the risk of dizziness/imbalance is higher in individuals with a CVA<49° (the median value in our study also corresponds to the recommended cutoff value for FHP). 27 Similarly, cervicogenic dizziness and impaired cervical proprioception have been reported in patients with radiculopathy who exhibit an FHP. 36 These results suggest that symptoms of dizziness and imbalance associated with HSU may also be linked to the development of FHP. However, this hypothetical relationship is unclear and cannot be causally established due to the cross-sectional design. Further research is needed to establish a definitive cause-and-effect relationship for this mechanism.
Cervicogenic dizziness results from impaired integration of faulty sensory input from cervical proprioceptors with the vestibular and visual systems. 33 This may lead to a feeling of uncertainty in the individual's perception of head position and instability in balance tasks. Although static postural balance performance was similar in the current study, cervical muscle fatigue and postural changes in individuals with HSU can negatively affect sensory integration with the vestibular system, creating a sense of imbalance that may be detected by psychometric scales but is not evident in force platform measurements. A previous study similarly reported an increased incidence of dizziness/imbalance symptoms in individuals with HSU, 14 and it was hypothesized that this could be influenced by abnormal proprioceptive input from the cervical region due to prolonged neck flexion associated with HSU. 16 Therefore, it may be assumed that excessive smartphone use does not directly disrupt static balance but may be related to early neurosensory symptoms such as cervicogenic dizziness and proprioceptive imbalance. Consequently, dizziness/imbalance symptoms in individuals with excessive smartphone use should not be ignored, as this can lead to subjective feelings of unwellness and, in the long term, decreased performance.
This study has several limitations. First, participants were grouped based on the median value because the cut-off value for SAS was not specified. While this approach provides some balance between groups, it requires careful interpretation of the results. Furthermore, this grouping system may have reduced statistical power and limited the detection of finer relationships across the variable's overall distribution. Additionally, smartphone addiction was assessed using self-report questionnaires. This may have created a potential source of social bias among participants. Therefore, evaluating smartphone addiction using more objective measures (e.g., screen time) could clarify the results. Furthermore, because this study is a cross-sectional study, a cause-and-effect relationship between smartphone addiction and clinical parameters cannot be established. Therefore, longitudinal studies are needed to establish a definitive cause-and-effect relationship between HSU and impaired postural and sensory awareness. Although static postural balance was found to be similar among the groups, differences in dizziness/imbalance symptoms suggest that the dynamic components of postural balance may be affected; therefore, comparing individuals using objective measurement tools that assess dynamic balance could yield important results. Finally, the fact that the participants were students and their average age was low may limit the generalizability of the findings.
Conclusion
In conclusion, HSU was associated with a greater decrease in CVA and a greater increase in JPE, as well as symptoms of dizziness/imbalance, in individuals. However, static postural balance, as assessed with the force platform, was similar in both groups. This suggests that cervical changes associated with HSU may not initially be significant enough to affect biomechanical balance, but may subjectively affect individuals in relation to dizziness/imbalance symptoms. In conclusion, increased smartphone use is associated with negative effects on cervical posture, proprioceptive sensitivity, and postural balance control. Therefore, given smartphone use and related symptoms, early planning of preventive approaches for young university students, such as posture awareness, posture and ergonomics training, and instilling the habit of taking regular breaks during prolonged screen use, may be beneficial. Additionally, early inclusion of proprioceptive exercises targeting the neck can help prevent dizziness/imbalance symptoms by increasing sensory awareness. These strategies can help reduce and prevent physical and cognitive strain associated with smartphone use.
Footnotes
Ethical approval
The study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Karabuk University Non-Interventional Ethics Committee (2024/1914). This study was submitted to ClinicalTrials (no: NCT06968078).
Informed consent
All participants gave informed consent to participate in the study.
Consent for publication
Informed consent was obtained for publication of data and photographs.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by a grant from Karabuk University Scientific Research Projects Coordination Unit. Project Number: KBÜBAP-25-DS-118.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available from the authors upon reasonable request.