
Abstract
Keywords
Introduction
Digital Health is a field of study that lies at the intersection of health and digital technologies, encompassing topics such as mobile health, wearable devices, telehealth, health information technologies, personalization of care, Robotics, Internet of Things, Cyber-Physical Systems (CPS), Augmented Reality, Additive Manufacturing, Big Data and Analytics, Systems simulation, Machine learning, and Cloud Computing. 1 This area is explored by several disciplines, whose first reference in the PubMed database dates back to the 1990s when this concept was used mainly for digitizing health information in libraries. 2 In the 2000s, with the dissemination of the Internet and the advancement of information technology and its applications, there were several new components in the innovation ecosystem in digital health.3–12
Although technologies related to digital health have the potential to increase effectiveness, reduce patient isolation, guarantee access to health equipment, reduce intervention costs, promote scalability in health promotion actions and monitoring of people with chronic conditions, the comprehensive assessment of their impacts and the identification of potential challenges associated with their implementation remain underexplored areas of research. 2 Despite the promising benefits of digitalization in healthcare, there is growing concern about the well-being of healthcare professionals.13,14 Among the challenges are issues related to privacy protection and data security, the impact on healthcare workers’ health, and inequalities stemming from regional disparities in digital health investments. 15
Previous reviews that investigated the impact of digital technologies in healthcare focused on health informatics, e-health, acceptance, telemedicine, and security.12,16 Studies have shown that digitalization is beneficial for healthcare and favors patient participation. They also identified the potential of digital technologies for improving the health workforce, covering training, communication, support, and management of professionals, especially in remote contexts. Nevertheless, the authors highlighted the need for large-scale demonstrations of the benefits and safety of these technologies. 12
Studies have shown that the introduction of digital technologies into the daily routines of healthcare providers has led to both beneficial and adverse outcomes for their mental health. The introduction of technological tools, such as electronic health records and digital communication systems, has contributed to greater efficiency and improved access to information. Yet, it has also brought new challenges, including increased cognitive load and stress. Studies indicate that the excessive use of digital technologies can trigger emotional and physical exhaustion among healthcare professionals, contributing to the development of conditions such as burnout and anxiety. The constant need to adapt to new systems, along with the pressure for productivity, further aggravates these issues, directly affecting the well-being of workers.17–20
Furthermore, the growing reliance on technology can intensify feelings of social disconnection and heighten perceptions of work overload, particularly among workers who struggle to adapt to digital tools or who operate in settings with limited human or technological resources. The growing reliance on technology can intensify feelings of social disconnection and increase perceptions of work overload, particularly among workers who struggle to adapt to digital tools or work in environments with limited resources.17–20
Also inadequate training in new technologies can heighten stress related to task performance. Burnout and anxiety may result from the constant updates in hardware and software, requiring professionals to stay continually updated to avoid ‘technological lag.’ Policies that balance technology use with psychological support and proper training are essential to mitigate these effects and promote a healthier work environment.17–20
Moreover, it is important to note that the adoption of digital technologies has accelerated due to the covid-19 pandemic. However, their effects on work processes, patient safety, and workers’ health remain insufficiently explored in the literature. This knowledge gap underscores the need to clarify key issues in order to support governments, unions, and the working class in developing public policies and protective measures that safeguard the mental well-being of healthcare professionals within the context of digital health. To this end, it is necessary to understand what is already known - and what remains opaque - about the relationship between digital health tools in the workplace and the mental health of health workers. In this context, this study aims to collect and analyze evidence on the effects of digital health on work processes and on the mental health of workers in the health sector.
Methods
The mixed method systematic review (MMSR) was carried out following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 21 recommendation to answer the following research question: how does digitalization affect work processes and the mental health of healthcare professionals?
This review is registered on the International Prospective Register of Systematic Reviews (PROSPERO) platform under code CRD42023468903.
Eligibility criteria
The eligibility criteria chosen for this study were based on the following inclusion criteria: (a) articles published openly and in full; (b) cross-sectional or cohort studies; (c) focus on health workers; (d) examination of the use of digital technologies in healthcare work processes—including mobile health, wearable devices, telehealth, health information technologies, personalized care, robotics, Internet of Things (IoT), cyber-physical systems (CPS), augmented reality, additive manufacturing, big data and analytics, systems simulation, and cloud computing; and (e) assessment of the effects of digitalization on workers’ mental health.
The search was limited to English-language literature, with peer-reviewed studies within the pre-established period, with pre-defined population and setting. Study reviews, letters to the editor, experimental preclinical studies, case series, and experience reports were not eligible.
Sources of information and search strategy
The search strategy was initiated through a primary search in MEDLINE, using the terms’ Digital Technology’ (MeSH) and ‘Digital Health’ (MeSH) to evaluate the breadth of relevant bibliography and guide the choice of descriptors for the primary research.
Eligible studies were identified in electronic databases: Pubmed via NLM, EMBASE via Elsevier, CINAHL/SocIndex via EBSCO, PsycINFO via APA, PsyArxiv, Web of Science via Clarivate Analytics, and Scopus via Elsevier. Table 1 presents the sources of information and search strategy.
Sources of information and search strategy.
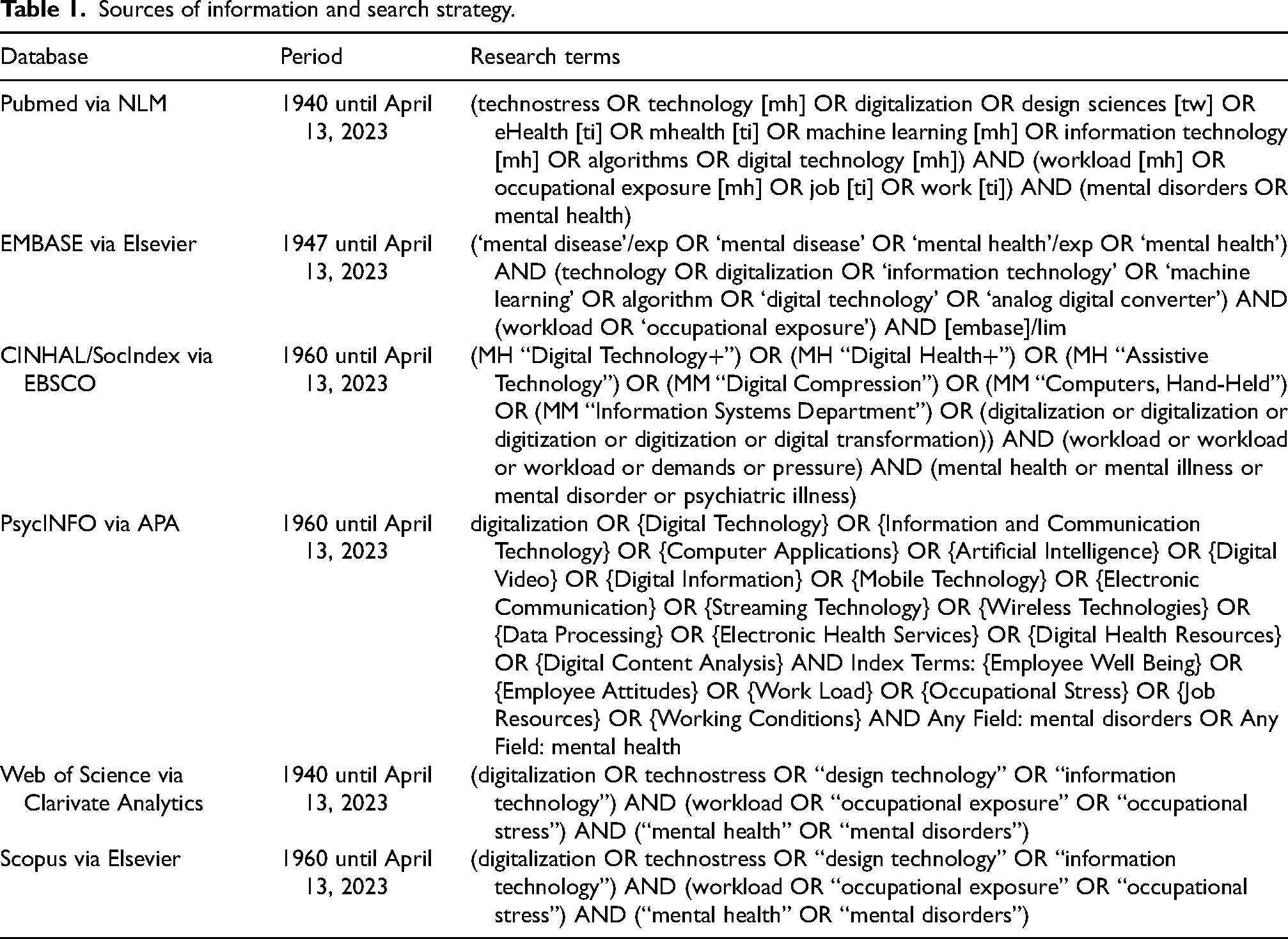
Database selection was carried out by a library professional based on specific inclusion criteria: (a) relevance to the topic; (b) coverage and comprehensiveness; (c) multidisciplinarity; (d) quality and reliability; (e) frequency of updates; and (f) availability of advanced search and filtering tools. Additionally, databases were selected according to the area of knowledge, with the following distribution: (1) for Health and Medical Sciences: PubMed and Embase; (2) for Social Sciences and Psychology: PsycINFO, Scopus, and Web of Science; (3) for Engineering and Technology: Scopus; and (4) for Computer Science: Scopus
Selection process and data collection process
The primary search was conducted by two individuals (AC and BB), one of whom was a professional in information systems - library science and the other a researcher with extensive experience in systematic review. After this stage, one of three independent researchers rigorously conducted the entire selection process to identify publications relevant to this study. The Rayyan web application was used to select the titles and abstracts of the studies retrieved from the search strategy performed by (AC and BB). Any discrepancies were resolved through discussion among the other reviewers.
The process of selecting study titles and abstracts for eligibility was carried out independently by two researchers (LZ and SC), with a referee (TS) to resolve discrepancies; full-text screening was carried out by (BB and SC). All disagreements were resolved by consensus in a meeting or by the referee (DR), using the eligibility criteria, with clear reasons provided for exclusion. Two researchers (CA and TS) extracted the data using data extraction software, using a spreadsheet as a resource that mapped the secondary data for this research; a fourth member (LZ) and the methodologist (DR) resolved inconsistencies.
List of data and synthesis methods
Two reviewers (CA and TS) independently extracted information from each study. A data extraction form was used that contained the following topics: general characteristics of the study (research team, country, year of publication, study design, sample characteristics, method, mental health problems that were described from digitalization, and the main impacts of digitalization on workers’ mental health).
For the quantitative component, data from quantitative and mixed methods studies were extracted by two independent reviewers (AC and BB) using the standard JBI data extraction tool in JBI SUMARI. For the qualitative component, data was extracted from qualitative studies included in the review by the same two independent reviewers (AC and BB) using the standardized data extraction tool from the JBI Critical Appraisal Tools - Checklist for Qualitative Research. 22 The extracted data included specific details about the population, context, culture, geographic location, study methods, and the phenomena of interest relevant to the purpose of the review.
Assessment of risk of bias, effect measures, and synthesis methods
The JBI Critical Appraisal Tools - Checklist for Qualitative Research 22 tool was used to analyze the quality of the selected qualitative articles. This checklist aims to evaluate the methodological quality of a research study and examine the extent to which a study addressed the possibility of bias in its design, conduct, and analysis. In this research, all articles selected for inclusion in the systematic review underwent rigorous evaluation by two authors; however, only articles with qualitative methodology could be grouped and analyzed by a tool.23,24
Integration of quantitative evidence and qualitative evidence
Data synthesis and integration in this review followed a convergent integrated approach, as outlined in the JBI methodology for MMSR, using JBI SUMARI. 25 This approach involves combining extracted data from both quantitative and qualitative studies. Quantitative data were ‘qualitized'—that is, translated into textual descriptions—to allow integration with qualitative data and enable narrative interpretation. Consequently, it was carried out an aggregation and synthesis of these results to generate a set of statements representing this aggregation by combining the results and categorizing them based on the similarity of meaning. These categories were then subjected to synthesis to produce a comprehensive set of synthesized results, which can be used as a basis for evidence-based practice. All four articles with a qualitative approach that went through this process presented sound synthesis and interpretation results and were included in this research. 26 The findings were extracted and given a high level of credibility.
Finally, the findings of each synthesis of the method included in this review were configured, merging quantitative evidence and qualitative evidence juxtaposed and organized/linked in a line of thought, where a global analysis was produced and configured in detail in the results and discussion of this article.25,26
Results
In this review, 1130 articles were retrieved from the databases investigated. The description of the process of choosing these documents is recorded in Figure 1, which illustrates the procedures used to select the 15 articles that constitute the final sample of this research.
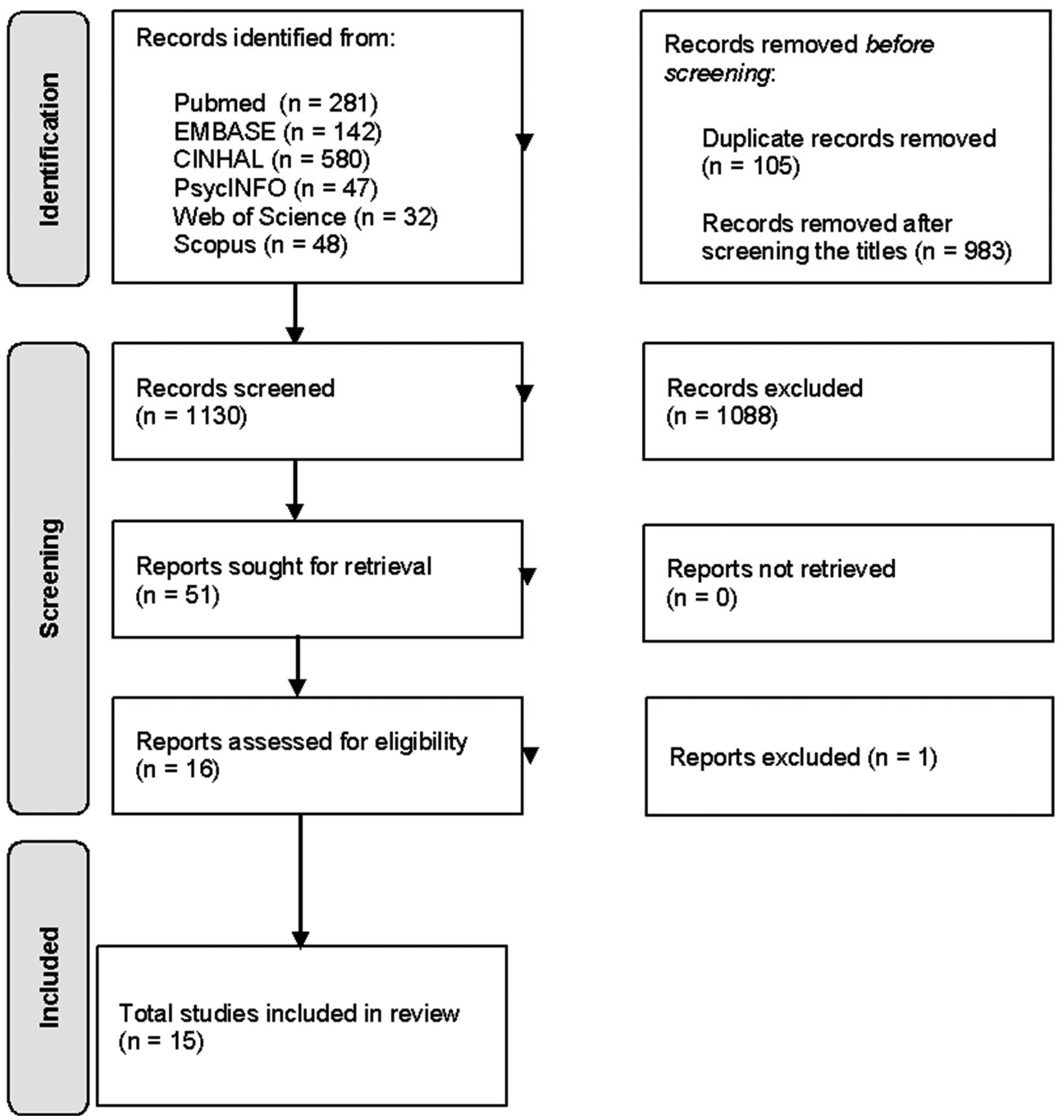
Diagram for the first phase of the selection process.
Table 2 presents the set of included studies and provides a detailed description of their characteristics and design. Figure 2 shows the geographical distribution of these studies.
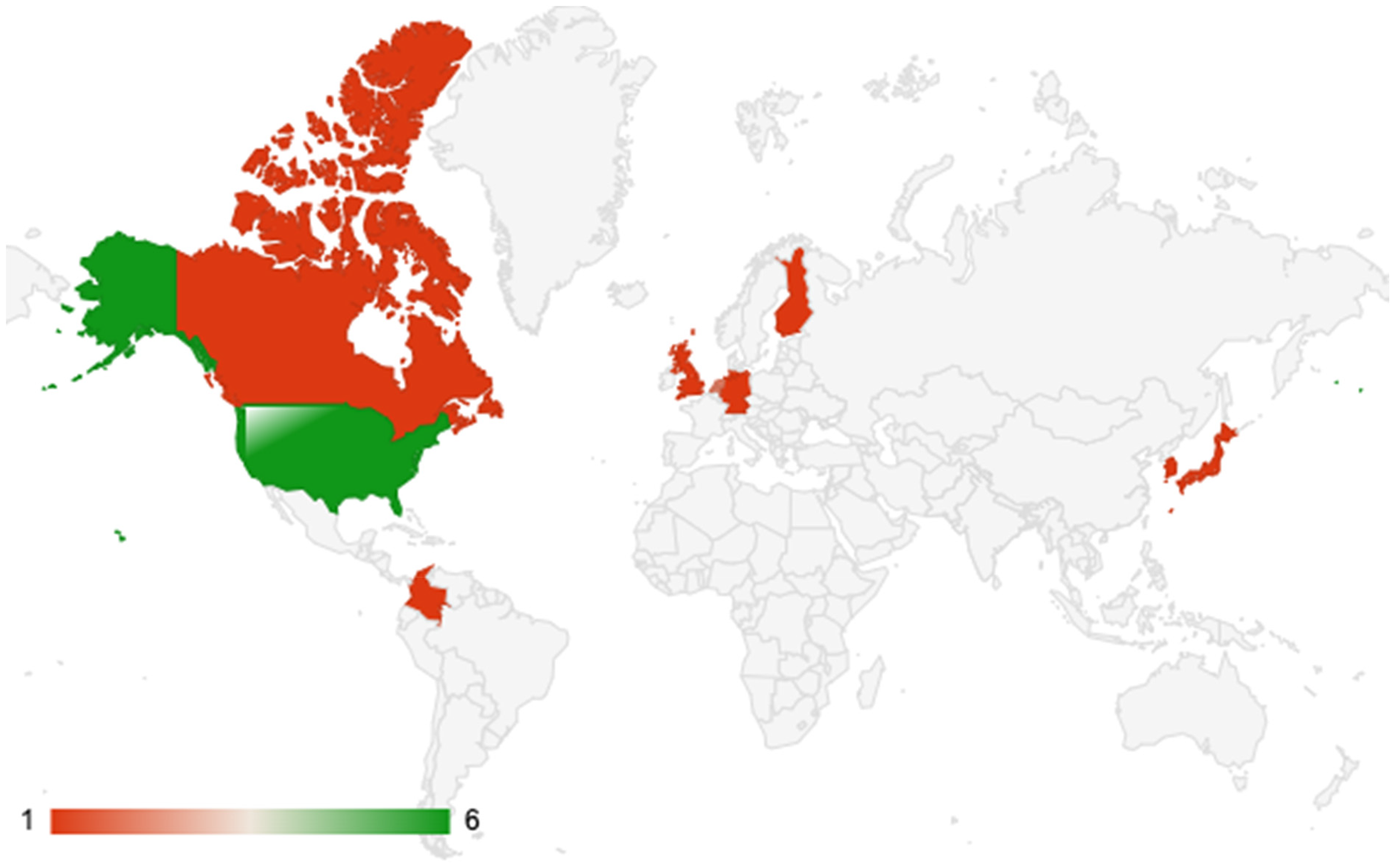
The geographical distribution of studies included.
The studies included.
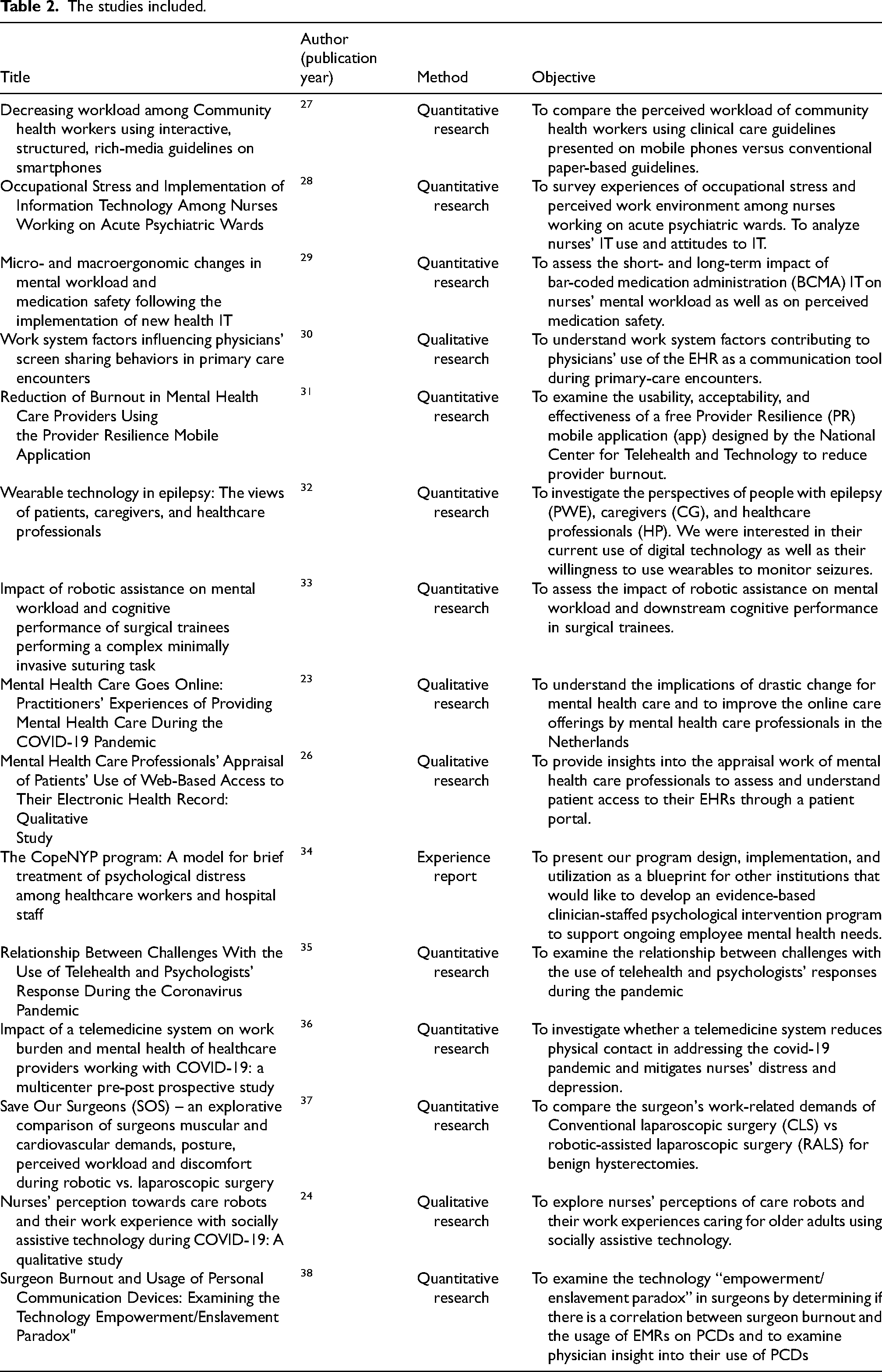
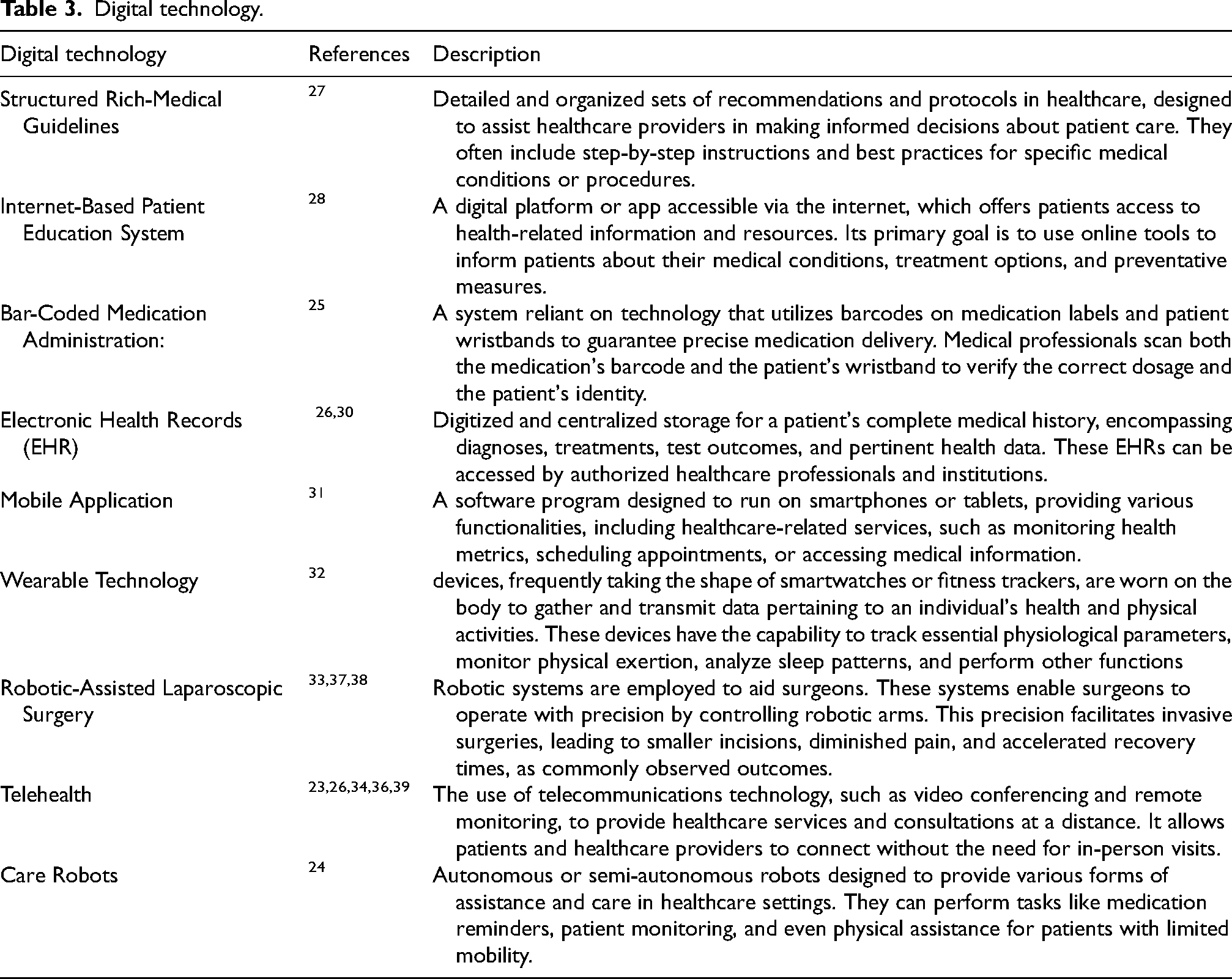
Furthermore, there have been comprehensive studies of the mental health system (n = 2),26,31 consultations in a virtual environment (n = 3)23,35,36 and the use of technologies by patients at home (n = 2).24,32 The digital technologies addressed in the studies in this review are presented in Table 3.
Digital technology.
The main results of the articles analyzed, which relate to the objective of this study, have been grouped into three thematic categories discussed below.
Effects of digital health on professionals’ performance at work to achieve patient care objectives
The use of interactive medical guidelines did not change the perceived performance in achieving patient care goals. 27 There was no difference in task completion time between traditional and robot-assisted laparoscopic surgery by junior residents, but robot-assisted laparoscopic surgery took longer and performed worse in senior residents. 33
Regarding the use of digital health devices in care, health professionals have highlighted the advantages and disadvantages. Advantages include strengthening trust and collaboration when sharing screens with patients, contributing to patient monitoring and management, 32 and self-management of health. 23 In online mental health care, convenience for professionals and patients was highlighted, 33 but disadvantages include misinterpretations of information by patients and a greater demand for clarifications. 30
The introduction of technologies such as care robots has increased the workload for nurses due to additional tasks. 24 While some articles indicate reduced mechanical overload and daily tasks, the need for technology supervision and educational actions with patients also emerged. To optimize the results of digital technologies in health care processes, the active participation of professionals in developing, implementing, and incorporating these technologies is essential. 26
Effects of digital health on the cognitive and mental demands of work
The studies analyzed indicate that the effects of digital health on the cognitive and mental demands of work have variable results. Teleservice impacts the mental health of psychologists depending on the challenges faced. Lesser challenges are associated with lower stress levels, ability to self-care, positive work-life balance, and a lower propensity for burnout. 35
Some studies have suggested that reducing stress or mental demands, for example, through the use of the Interactive Structured Rich-Medical guidelines (ISRMGs) interface on cell phones, resulted in statistically significant decreases in perceived mental demand (cognitive load), frustration, and general workload.27,28 The ISRMG was developed to support professionals in carrying out tasks, guiding them according to the sequence of their activity. 27 Furthermore, regarding mental demands, after a month of using an application to increase self-awareness of current burnout levels, the results of a sample composed of mental health professionals indicated that the size of the effect in reducing burnout and compassion fatigue was substantial, suggesting the potential for a significant impact related to use of the app use. 31 Nurses indicated a reduced workload and relief using an autonomous vital signs assessment system when monitoring covid-19 patients. However, measures related to distress and depression showed no significant difference with or without the system. 24
From this perspective, there was no difference in mental and cognitive load when comparing standard laparoscopic surgery with robot-assisted laparoscopic surgery in junior residents or senior trainees. However, when comparing groups, junior residents reported a significantly higher overall load in physical demand. 33
In a study that evaluated the use of Personal Communication Devices (PCD) to access Electronic Health Records (medical records), no direct association was found between frequent access to devices and mental exhaustion. Residents and those who overestimated PCD use had higher burnout scores. These results suggest that perceived workload may influence burnout. Although PCDs are helpful in healthcare, they can also cause distractions and expectations of constant availability. 38
On the other hand, studies have suggested increased mental work demands, as reported by healthcare professionals. This increase is related, for example, to the more significant time needed to review data and to deal with patients’ anxiety about their data 32 and the perception that video conference sessions during teleservice are more demanding and tiring than face-to-face sessions.23,37
Professionals’ concerns and perceptions about work regarding digital health
Regarding the challenges and concerns associated with digital health, studies have highlighted the technological infrastructure and communication aspects, 23 the use of collected information, 32 and maintenance and cleaning of devices used by patients. 24 In mental health care carried out remotely, the speed and instability of internet connections, as well as the harm to non-verbal communication, the lack of organizational support for the use of available software and devices, and guidelines on which tools comply with Privacy regulations make it difficult to establish a connection with the patient and communicate clearly. Furthermore, professionals assessed that some exercises used in face-to-face sessions are prevented from being carried out via teleservice, for example, dramatization or collaborative design of models. 23
Discussion
This article collected and analyzed evidence on the effects of digital health on work processes and the mental health of healthcare workers. A total of 15 original articles were included, with a predominance of quantitative studies conducted in high-income countries and focused mainly on physicians. The quantitative approach can provide valuable insights into the adoption of these technologies, assessing their efficiency and their outcomes for both patients and workers. However, it may limit a comprehensive understanding of the phenomenon, as digitalization also involves important qualitative dimensions, such as the experiences of healthcare professionals and the ethical challenges associated with technology use.
Among the various digital health technologies examined in the studies included in this review, the most prominent were Electronic Health Records (EHR), robotic-assisted laparoscopic surgery (RALS), and telehealth. Regarding the settings, the hospital environment was the most frequently explored, particularly in the context of surgical procedures and teleconsultations. 40
It is worth noting that during the period in which there was a greater concentration of studies in this review, between 2020 and 2022, the world faced the covid-19 pandemic, which required the expansion of intensive and emergency care to respond to the high demand from the population due to health complications generated by the coronavirus.23,24,36 It is assumed that the increase in digital technologies in work processes during this period may be related to the consequences of the pandemic and the protective measures to try to control contagion, which accelerated the spread of telehealth care.
Regarding the effects of introducing digital technologies in patient care, the results of the research analyzed in this review are diverse, including positive and negative aspects and even the absence of significant effects, which is in line with the conclusions of other research.41,42 As for the positive aspects, they highlighted improvements in the professional-patient relationship, the humanization of care, health self-management, and the flexibility of staff time.
Nonetheless, the results of this review reinforce the negative aspects identified in previous studies, highlighting new organizational demands that may lead to task overload for healthcare professionals.6–9 This situation reflects a shift in the care provision paradigm, as digitalization in healthcare transforms face-to-face care into information intended for the self-management of patients’ health conditions. This transformation is referred to as the biopsychosocial-digital approach, which is considered an expansion of the biological self through the use of technology and online networks. 43
Regarding the effects of digital health on the mental health and cognitive load of healthcare workers, studies showed that professionals’ perception of stress about the use of digital health devices was associated with access and frequency, the thorough review of care data, and the feeling of constant availability, which results in burden. Furthermore, health professionals are experiencing new cognitive demands since, in addition to the need to study and improve the management of information and communication technologies, 44 they need to pay attention to behavioral dynamics during virtual interventions and deepen discussions about this.45–47
The difficulty in adapting to new technologies can cause mental suffering for workers. How people respond to integrating technology and decision-making situations in their work routines differs according to capacity, skill, and previous experiences. 48 These processes are often technology-centered rather than problem-centered, frequently failing to provide solutions to the actual challenges faced by healthcare professionals.
Professionals’ concerns about digital health devices highlighted communication, the use of collected information, and the maintenance of patient devices.43,49 The technological challenges related to digitalization that become barriers in patient care are the infrastructure offered to professionals, variations in internet speed, and the different devices used by patients with other software depending on each device that can compromise the safety of patients’ data and quality of care.50,51
The importance of regulating and standardizing good practices in digital health is emphasized, with a focus on responding to client demands and ensuring information security, privacy, and confidentiality. 52 In this context, providing training in digital technologies and promoting peer-to-peer knowledge sharing can help mitigate challenges and support professionals in adapting to care delivery.29,34,39,53–56
Most studies included in the review were cross-sectional or short-duration. The lack of longitudinal studies limits the assessment of digital health's long-term effects on healthcare professionals’ mental health. Additionally, the studies evaluated and discussed aspects that relate to the results of digital health innovations and workers’ mental health, such as performance measures, effects on patient monitoring, new mental demands, and time constraints. Still understanding the outcomes of health digitalization on the work process and in workers’ health, especially in mental health, has not been addressed in depth or in an integrated manner, considering its multiple dimensions.
Conclusions
This systematic review aimed to investigate the effects of digitalization on the mental health of healthcare workers across different professional categories and work settings. The studies analyzed addressed multiple dimensions of healthcare provision, including patient care quality, workload management, and communication among professionals. The review also highlighted strategies aimed at mitigating the harmful effects of digitalization on mental health in the workplace.
The findings contribute to a broader understanding of how digital technologies are reshaping healthcare delivery. Evidence from the selected studies indicates that digital tools can generate both benefits and challenges, influencing variables such as stress, job satisfaction, and the onset of burnout. In particular, the assessment of physical, cognitive, and mental workload has emerged as a common approach to measuring the impact of these technologies on health professionals. The results also point to the relevance of incorporating workers’ experiences into the development and refinement of digital solutions. For digitalization to effectively support care provision, it must be accompanied by dialogue within services and the active participation of professionals whose practices are being transformed.
Despite its contributions, this review presents some limitations. The heterogeneity of the included studies—regarding methodology, mental health measures, types of digital health interventions, and professional groups—makes it difficult to directly compare results or produce a unified synthesis. Additionally, only studies published up to June 2023 were included, which may exclude more recent developments in this rapidly evolving field. Research focused specifically on digital mental health interventions for healthcare professionals was excluded, as it did not align with the review's objective.
Finally, this review underscores the need for future research that deepens the investigation into how digital health affects professionals’ mental health. It is essential to conduct longitudinal studies and meta-analyses that explore variables such as professional categories, work contexts, technology use, and possible cases of work absenteeism linked to digitalization. As digital health continues to evolve, the long-term implications of integrating technology into healthcare routines must be critically assessed, balancing innovation with the well-being of those who deliver care.
Footnotes
Acknowledgements
Not applicable
Ethical approval
Not applicable
Informed consent
Not applicable
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.