
Abstract
Background
In recent years, the increasing demand for educational innovation and quality has created multiple occupational stressors for teachers. Long-term exposure to these stressors increases the risk of burnout, which influences mental and public health. Although numerous studies have evaluated the effectiveness of stress reduction interventions for educators, a gap exists in evidence-based research on mindfulness-based interventions (MBIs), specifically targeting this professional group.
Objects
This study aims to evaluate the overall effects of MBIs on teachers’ work stress.
Methods
This systematic review and meta-analysis focused on randomized controlled trials (RCTs) to evaluate the effectiveness of MBIs in alleviating teachers’ work-related stress. Following the Preferred Reporting Items for Systematic Reviews and Meta-analyses 2020 guidelines, we searched five databases (PubMed, EMBASE, Cochrane, Web of Science, and PsycINFO) for relevant RCTs up to July 2025. We assessed the risk of bias using Cochrane RoB 2 tool.
Results
Pooled data from 13 trials (N = 2119) showed that, compared with the waitlist control group, perceived stress significantly decreased after intervention (standardized mean difference, SMD = −2.37, 95% CI = [−4.40, −0.35]. Additionally, mindfulness levels increased (SMD = 0.59, 95% CI = [0.39, 0.79], p < 0.001), and negative emotions decreased (SMD = −0.95, 95% CI = [−1.27, −0.62], p < 0.001). However, the presence of methodological and clinical heterogeneity requires a cautious interpretation of these results.
Conclusion
Findings suggest that MBIs serves as an effective tool for reducing general perceived stress and improving teacher well-being. Results also emphasize the need to design and conduct studies with long-term follow-up.
Keywords
Introduction
Work-related stress poses a significant and widespread challenge in the teaching profession. Research indicates that the vast majority of teachers experience considerable psychological strain. 1 Theoretically, this phenomenon occurs when objective job demands, or stressors, exceed an individual's adaptive capacity, thereby triggering detrimental physical and psychological responses termed strain, which increases the risk of adverse health outcomes.2,3 Maintaining a clear conceptual distinction between these external stressors and the internal strain they induce remains crucial, as articulated by Rohmert. 4 In the contemporary educational landscape, these objective stressors continue to diversify and intensify; teachers grapple with heavy instructional workloads; the continual pressures of educational reform and standardized assessments; and the complexities inherent in managing relationships with students, parents, and colleagues.5,6 Specifically, social stressors in the workplace involving relational devaluation serve as powerful antecedents to strain, a conclusion supported by Gerhardt and colleagues. 7 When these pervasive professional demands intersect with personal life and health responsibilities, they form a potent combination of stressors that significantly impact teachers.8,9 The resulting strain manifests as a debilitating negative emotional syndrome characterized by anger, despair, anxiety, and reduced self-esteem, all of which are mediated by threats to core well-being.10,11 This profound strain extends beyond individual suffering, posing a serious threat to the educational system by diminishing teaching quality, increasing the loss of talented educators, and hindering student development.12,13
Therefore, effective stress management strategies are crucial. Researchers have developed various intervention measures, including leadership and communication skills training, cognitive behavioral therapy (CBT), mindfulness-based interventions (MBIs), inquiry-based stress reduction training, and rational emotive therapy.12,14–16 Among these strategies, MBIs demonstrate considerable promise. 17 MBIs ground themselves in the concept of mindfulness, defined as the ability to observe one's current thoughts, bodily sensations, and perceptions with an open and accepting attitude. 18 The therapeutic efficacy of mindfulness in alleviating anxiety, depression, chronic pain, and insomnia has established its importance in psychology and medicine. 19 This foundation has led to the integration of MBIs into mental health therapies and broader applications in education, business, and sports.17,20–23 Evidence suggests that these interventions particularly suit individuals in high-stress professions, including teachers, healthcare workers, and financial practitioners. Research shows that MBIs effectively reduce stress levels by improving awareness of current experiences, enhancing coping skills, and improving psychological flexibility. Specifically, teachers report reduced stress and improved mental health after participating in MBIs.24,25 Medical workers effectively alleviate pressure in high-burden situations through digital or guided MBIs (e.g., mindfulness-based cognitive therapy for life).26,27 Furthermore, workplace mindfulness practices support employee recovery, enhance adaptive responses to stressors, and reduce burnout and work-related pressure.28,29
Although several systematic reviews confirm the efficacy of MBIs in alleviating teacher stress,30,31 key limitations persist. First, prior reviews have frequently included multimodal interventions combining MBIs with other psychotherapeutic approaches (e.g., CBT or relaxation techniques), thereby obscuring the distinct contribution of standalone MBIs and precluding a focused examination of their specific effects. Second, while the review by Klingbeil et al. 32 was pioneering in focusing on MBIs for teachers, its literature search concluded in April 2018, necessitating an update to incorporate substantial research developments over the subsequent seven-year period. In addition, a lack of meta-analyses based on randomized controlled trials (RCTs) limits the availability of high-quality evidence. To bridge these gaps, we synthesized recent RCT evidence on MBIs. We aim to quantitatively explore the multidimensional mechanisms of mindfulness and the temporal trajectory of its effects, thereby providing a theoretical basis for optimizing consolidation strategies in clinical practice.
Methods
We adhered to the methodological guidelines established by the Preferred Reporting Items for Systematic Reviews and Meta-analyses. 33 This study is registered with the International Prospective Register of Systematic Reviews under registration number CRD42024501682.
Search strategy
We performed systematic searches in PubMed, EMBASE, Cochrane Library, Web of Science, and PsycINFO from database inception through July 2025. Using MeSH terms and keyword variants related to MBIs, occupational stress, and educators, we identified RCTs assessing therapeutic efficacy. The search parameters focused on articles published in English. Additionally, we conducted in-depth examination of reference lists from the included studies to ensure no pertinent research was omitted. We tailored the search strategies to align with the unique characteristics of each database, thereby ensuring the comprehensiveness and precision of the outcomes (detailed in Supplementary File 1).
Eligibility criteria and study selection
We evaluated the efficacy of MBIs in alleviating occupational stress among educators using the PICOS framework 34 to guide our selection. Inclusion criteria required: (1) a focus on RCTs; (2) research subjects from various educational settings, including teachers, lecturers, special education educators, and similar educational personnel; (3) interventions limited to mindfulness therapy; and (4) publication up to July 30, 2025.
We excluded studies that: (1) combined mindfulness with other therapies (e.g., mindfulness-based cognitive intervention); (2) incorporated diverse intervention types or provided vague descriptions; (3) consisted of reviews, editorials, conference summaries, texts, and meta-analyses; (4) exhibited poor quality or apparent data inaccuracies; and (5) lacked accessible full texts or raw data that could be converted for analysis.
Following these criteria, we imported relevant citations into EndNote and performed deduplication. Two researchers independently screened titles and abstracts to determine eligibility, with a third-party review resolving any disagreements. The same two researchers thoroughly assessed the full texts for final inclusion based on the predefined criteria. We maintained objectivity and accuracy throughout the selection process, resolving any discrepancies through third-party consultations.
Data extraction
We extracted key study data and organized them into a structured table, including investigator identities, subject characteristics, intervention specifics, and outcome measures. A third researcher arbitrated extraction disagreements to ensure consistency and data accuracy. This approach enhances the study's rigor and supports later analyses.
Quality assessment
Two reviewers independently assessed the risk of bias based on the Cochrane Handbook, 35 using the RoB 2 tool 36 for RCTs. We classified each criterion by risk level, from high to low, with an “unknown risk” category used when insufficient information was available. A third reviewer resolved any discrepancies to ensure credible evaluations.
Statistical analysis
We used Review Manager (Cochrane Collaboration in Oxford, UK) for the meta-analysis. Our analysis synthesized mean values, standard deviations, sample sizes for intervention and control groups at the final follow-up, and changes from the baseline. We employed two methods to assess pooled effect sizes for continuous variables: mean difference (MD) and standardized MD (SMD). Descriptive analysis was conducted when data did not meet the criteria for pooling. We used the I2 statistic and P-value to assess heterogeneity. Given the presence of heterogeneity, we applied a random effects model to analyze the data, ensuring the accuracy of our analysis. We performed sensitivity analysis was performed by sequentially omitting each study to confirm the stability of the results and the robustness of the pooled findings. This approach identifies studies that significantly influence the overall conclusion and evaluate their contribution to the pooled effect size. According to the Cochrane Handbook, when a meta-analysis includes at least 10 RCTs, we employed Egger's regression test to assess funnel plot asymmetry for potential publication bias. Concurrently, we performed meta-regression and subgroup analyses to investigate possible sources of statistical heterogeneity. If a synthesis includes fewer than 10 RCTs, then we omitted these statistical tests to avoid unreliable conclusions.
Results
Literature search
A systematic search across PubMed, EMBASE, Cochrane Library, Web of Science, and PsycINFO using the keywords “psychological intervention,” “teacher,” and “random” yielded 4378 documents. Following deduplication, the screening of 1986 titles and abstracts resulted in the exclusion of all non-mindfulness studies. Of the remaining records, 103 underwent a rigorous full-text review, with 13 trials ultimately meeting the inclusion criteria. Figure 1 shows the selection process.
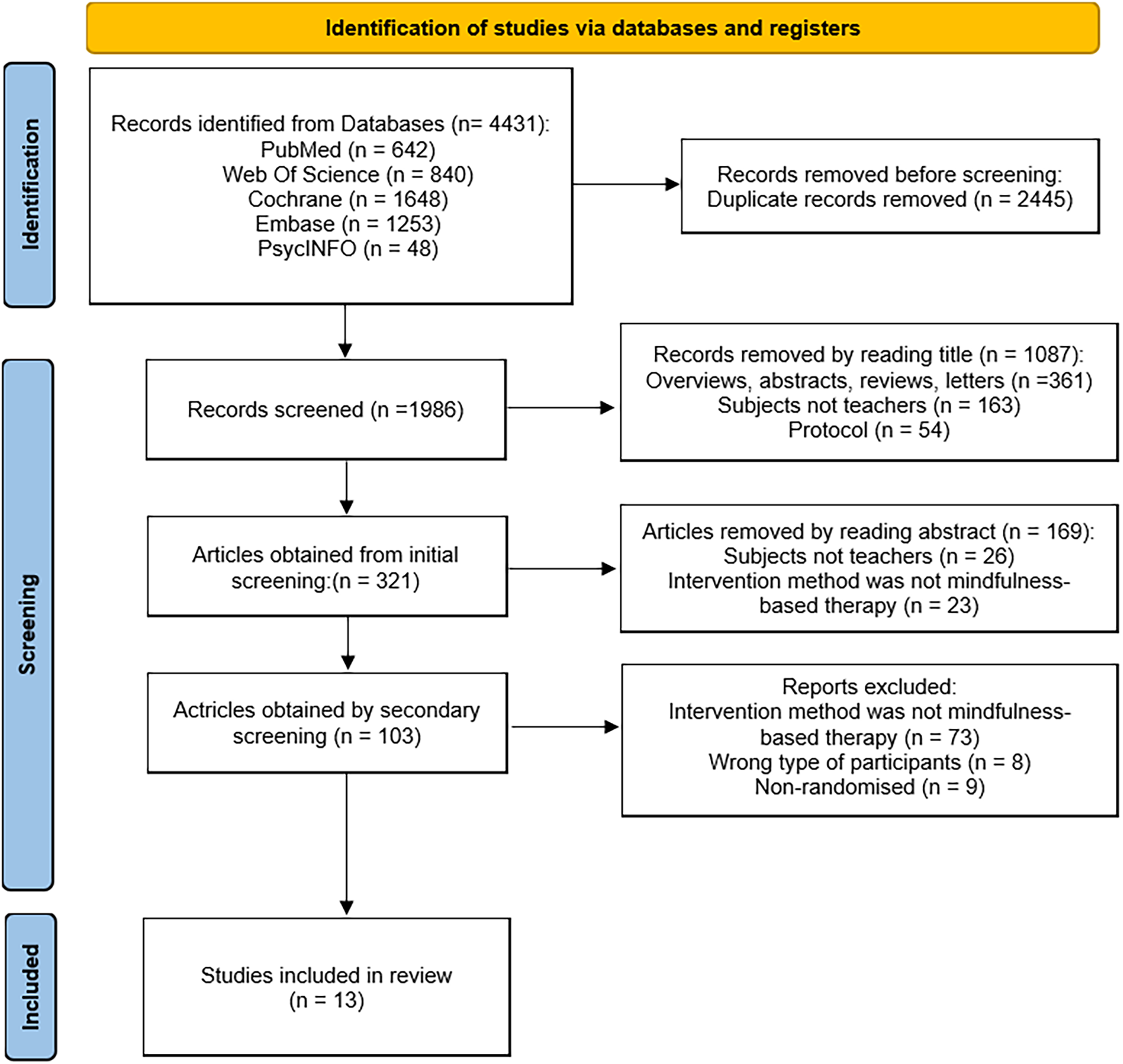
Flow of studies through the review.
Study characteristics
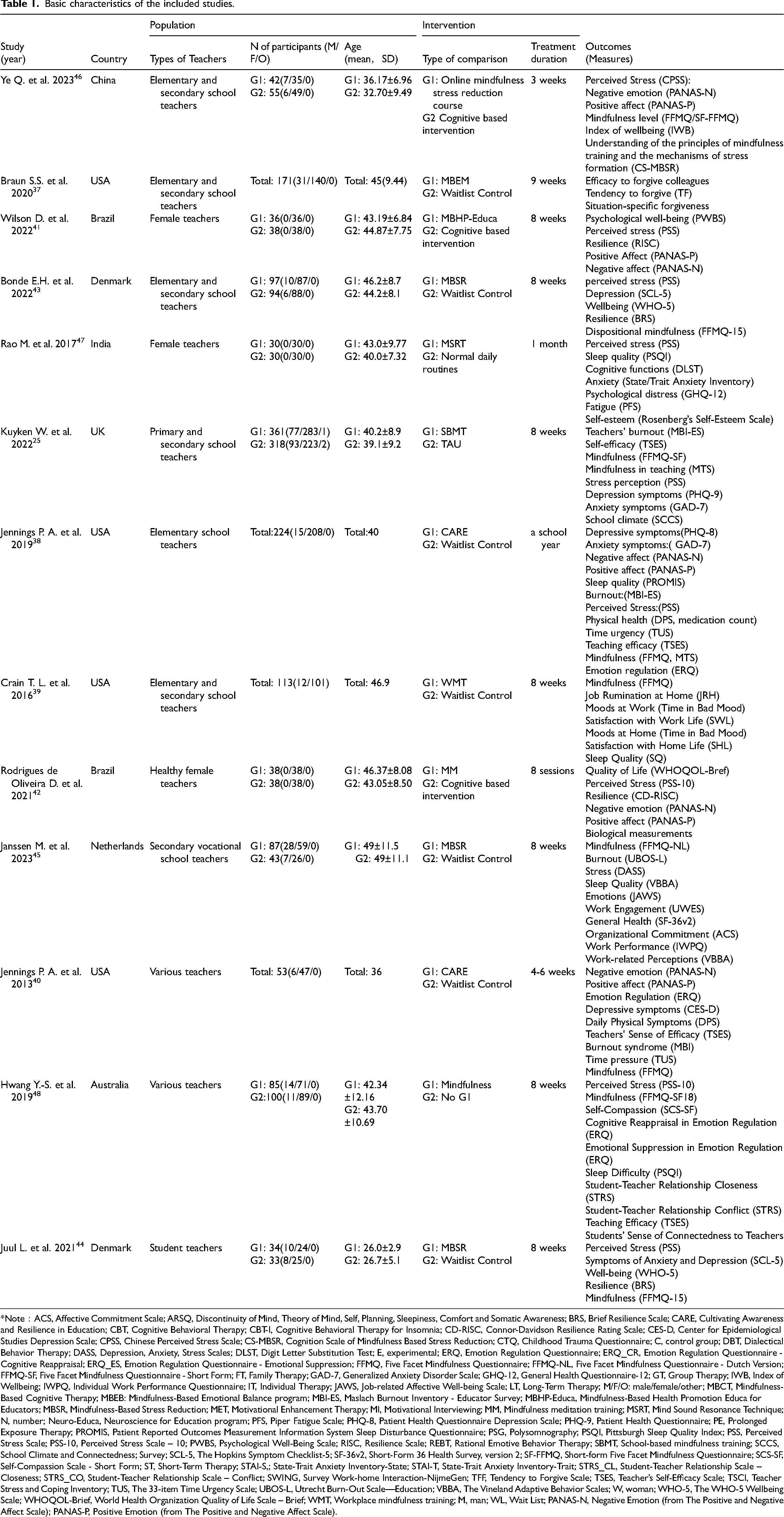
Thirteen publications investigating interventions that affect teachers’ work stress met the criteria for this study, as detailed in Table 1. The included research originated from the USA,37–40 Brazil,41,42 Denmark,43,44 the Netherlands, 45 China, 46 India, 47 the UK, 25 and Australia. 48 Published from 2013 to 2023, these trials involved a total of 2119 participants, with individual sample sizes ranging from 25 to 679. Participants were recruited from primary and secondary schools, including teachers reporting sleep disturbances. Random sampling was conducted at either the school or individual level, and all studies included male and female teachers, with ages ranging from 25 to 49 years.
Basic characteristics of the included studies.
*Note:ACS, Affective Commitment Scale; ARSQ, Discontinuity of Mind, Theory of Mind, Self, Planning, Sleepiness, Comfort and Somatic Awareness; BRS, Brief Resilience Scale; CARE, Cultivating Awareness and Resilience in Education; CBT, Cognitive Behavioral Therapy; CBT-I, Cognitive Behavioral Therapy for Insomnia; CD-RISC, Connor-Davidson Resilience Rating Scale; CES-D, Center for Epidemiological Studies Depression Scale; CPSS, Chinese Perceived Stress Scale; CS-MBSR, Cognition Scale of Mindfulness Based Stress Reduction; CTQ, Childhood Trauma Questionnaire; C, control group; DBT, Dialectical Behavior Therapy; DASS, Depression, Anxiety, Stress Scales; DLST, Digit Letter Substitution Test; E, experimental; ERQ, Emotion Regulation Questionnaire; ERQ_CR, Emotion Regulation Questionnaire - Cognitive Reappraisal; ERQ_ES, Emotion Regulation Questionnaire - Emotional Suppression; FFMQ, Five Facet Mindfulness Questionnaire; FFMQ-NL, Five Facet Mindfulness Questionnaire - Dutch Version; FFMQ-SF, Five Facet Mindfulness Questionnaire - Short Form; FT, Family Therapy; GAD-7, Generalized Anxiety Disorder Scale; GHQ-12, General Health Questionnaire-12; GT, Group Therapy; IWB, Index of Wellbeing; IWPQ, Individual Work Performance Questionnaire; IT, Individual Therapy; JAWS, Job-related Affective Well-being Scale; LT, Long-Term Therapy; M/F/O: male/female/other; MBCT, Mindfulness-Based Cognitive Therapy; MBEB: Mindfulness-Based Emotional Balance program; MBI-ES, Maslach Burnout Inventory - Educator Survey; MBHP-Educa, Mindfulness-Based Health Promotion Educa for Educators; MBSR, Mindfulness-Based Stress Reduction; MET, Motivational Enhancement Therapy; MI, Motivational Interviewing; MM, Mindfulness meditation training; MSRT, Mind Sound Resonance Technique; N, number; Neuro-Educa, Neuroscience for Education program; PFS, Piper Fatigue Scale; PHQ-8, Patient Health Questionnaire Depression Scale; PHQ-9, Patient Health Questionnaire; PE, Prolonged Exposure Therapy; PROMIS, Patient Reported Outcomes Measurement Information System Sleep Disturbance Questionnaire; PSG, Polysomnography; PSQI, Pittsburgh Sleep Quality Index; PSS, Perceived Stress Scale; PSS-10, Perceived Stress Scale – 10; PWBS, Psychological Well-Being Scale; RISC, Resilience Scale; REBT, Rational Emotive Behavior Therapy; SBMT, School-based mindfulness training; SCCS, School Climate and Connectedness; Survey; SCL-5, The Hopkins Symptom Checklist-5; SF-36v2, Short-Form 36 Health Survey, version 2; SF-FFMQ, Short-form Five Facet Mindfulness Questionnaire; SCS-SF, Self-Compassion Scale - Short Form; ST, Short-Term Therapy; STAI-S,; State-Trait Anxiety Inventory-State; STAI-T, State-Trait Anxiety Inventory-Trait; STRS_CL, Student-Teacher Relationship Scale – Closeness; STRS_CO, Student-Teacher Relationship Scale – Conflict; SWING, Survey Work-home Interaction-NijmeGen; TFF, Tendency to Forgive Scale; TSES, Teacher’s Self-Efficacy Scale; TSCI, Teacher Stress and Coping Inventory; TUS, The 33-item Time Urgency Scale; UBOS-L, Utrecht Burn-Out Scale—Education; VBBA, The Vineland Adaptive Behavior Scales; W, woman; WHO-5, The WHO-5 Wellbeing Scale; WHOQOL-Brief, World Health Organization Quality of Life Scale – Brief; WMT, Workplace mindfulness training; M, man; WL, Wait List; PANAS-N, Negative Emotion (from The Positive and Negative Affect Scale); PANAS-P, Positive Emotion (from The Positive and Negative Affect Scale).
In this cohort of 13 studies, we found that six trials utilized the Five Facet Mindfulness Questionnaire (FFMQ) to quantify mindfulness levels, whereas another six employed the Perceived Stress Scale (PSS) to assess stress. Four studies used the Positive and Negative Affect Schedule (PANAS) to evaluate emotional states. Additionally, we observed the use of the Resilience Scale (RISC), Work Stress Recovery Scale (BRS), Symptom Checklist-5 (SCL-5), and World Health Organization Well-Being Index (WHO-5) in two studies to measure resilience, depression, well-being, and work stress.
Risk of bias
We assessed meta-analysis quality using strict criteria. About 53.84% of studies had minimal bias risk, indicating robust methodology. Studies25,38,39,41,43,45,48 attained low-risk status due to rigorous randomization, blinding, data integrity, and transparent reporting. Conversely, Ye et al. 46 and others37,40,42,44,47 lacked details for reliability assessment, resulting in a moderate risk classification (Figure 2).

Risk of bias summary.
Meta-analysis
Effect on perceived stress
Our meta-analysis of PSS scores pre-and-post intervention revealed that MBIs significantly reduced stress perception in the intervention group compared to the control group (SMD = −2.37, 95% CI = [−4.40, −0.35], I2 = 97%, Figure 3(a)). In a comparative meta-analysis with the cognitive-based intervention group, the participants in the MBI group also showed significantly lower stress perception levels (SMD = −2.48, 95% CI = [−4.34, −0.61], I2 = 96%, Figure 3(b)).
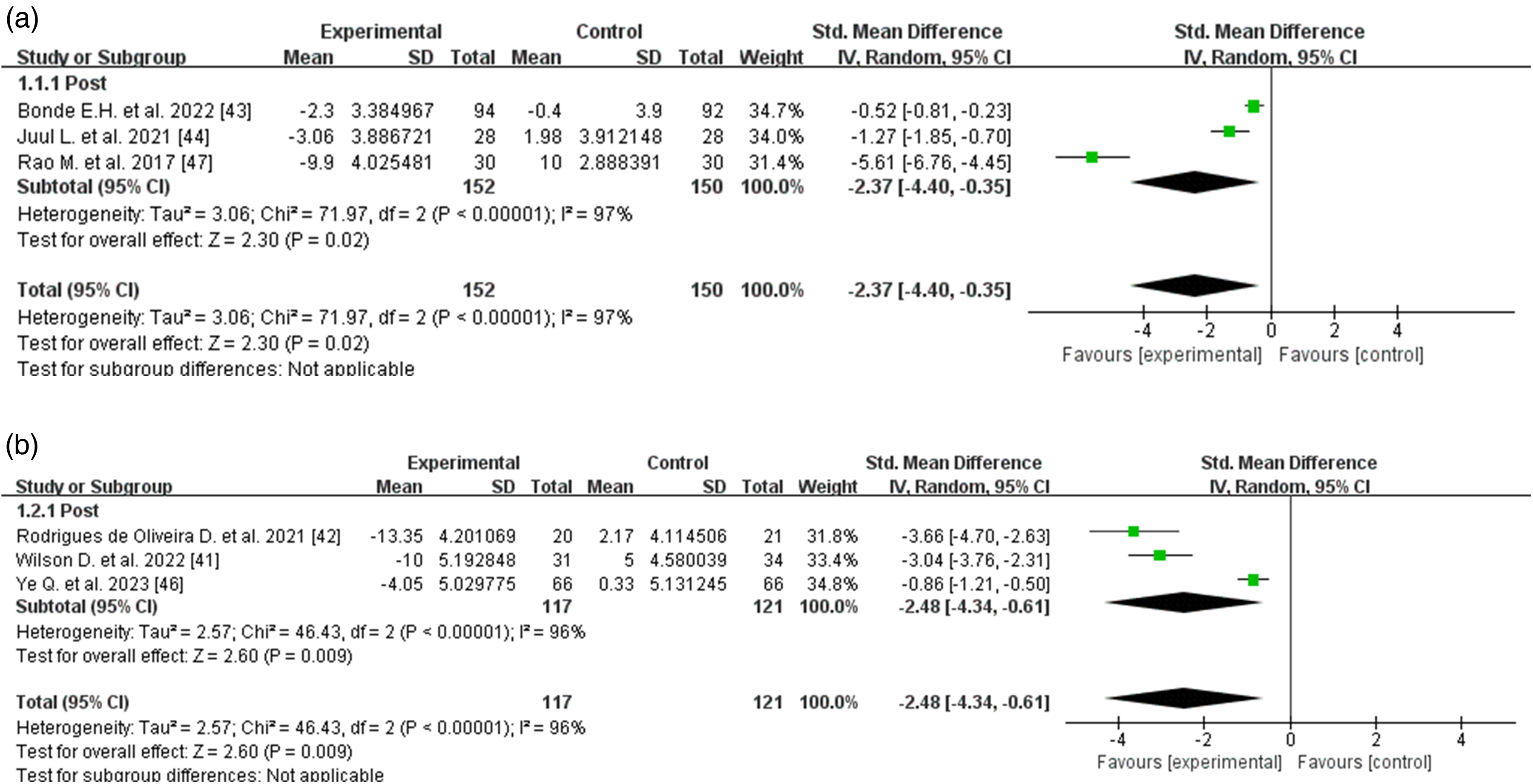
Forest plot of the meta-analysis for perceived stress (PSS). (a) Comparison between the MBI group and the waitlist control group at post-test. (b) Comparison between the MBI group and the cognitive-based intervention group at post-test.
Effect on mindfulness level
We systematically evaluated the efficacy of MBIs on educators’ metacognitive capacities using six RCTs that employed the FFMQ. Four trials used the 39-item FFMQ (FFMQ-39),38–40,45 whereas the remaining two utilized the 15-item FFMQ (FFMQ-15).43,44 Although all FFMQ-39 studies assessed total scores, only 50% examined Observing, Describing, Acting with Awareness, Non-judging, and Non-reactivity.40,45
Meta-analysis of pre-post intervention FFMQ total scores demonstrated significant improvements in the intervention group (SMD = 0.59, 95% CI = [0.39, 0.79], p < 0.001) compared to the control group (Figure 4(a)). The three-month assessment revealed sustained treatment effects (SMD = 0.90, 95% CI = [0.58, 1.22], p < 0.001), although substantial heterogeneity emerged (I2 = 73%). The nine-month follow-up also showed sustained effects (SMD = 0.57, 95% CI = [−0.02, 1.16], p = 0.06, I2 = 73%).
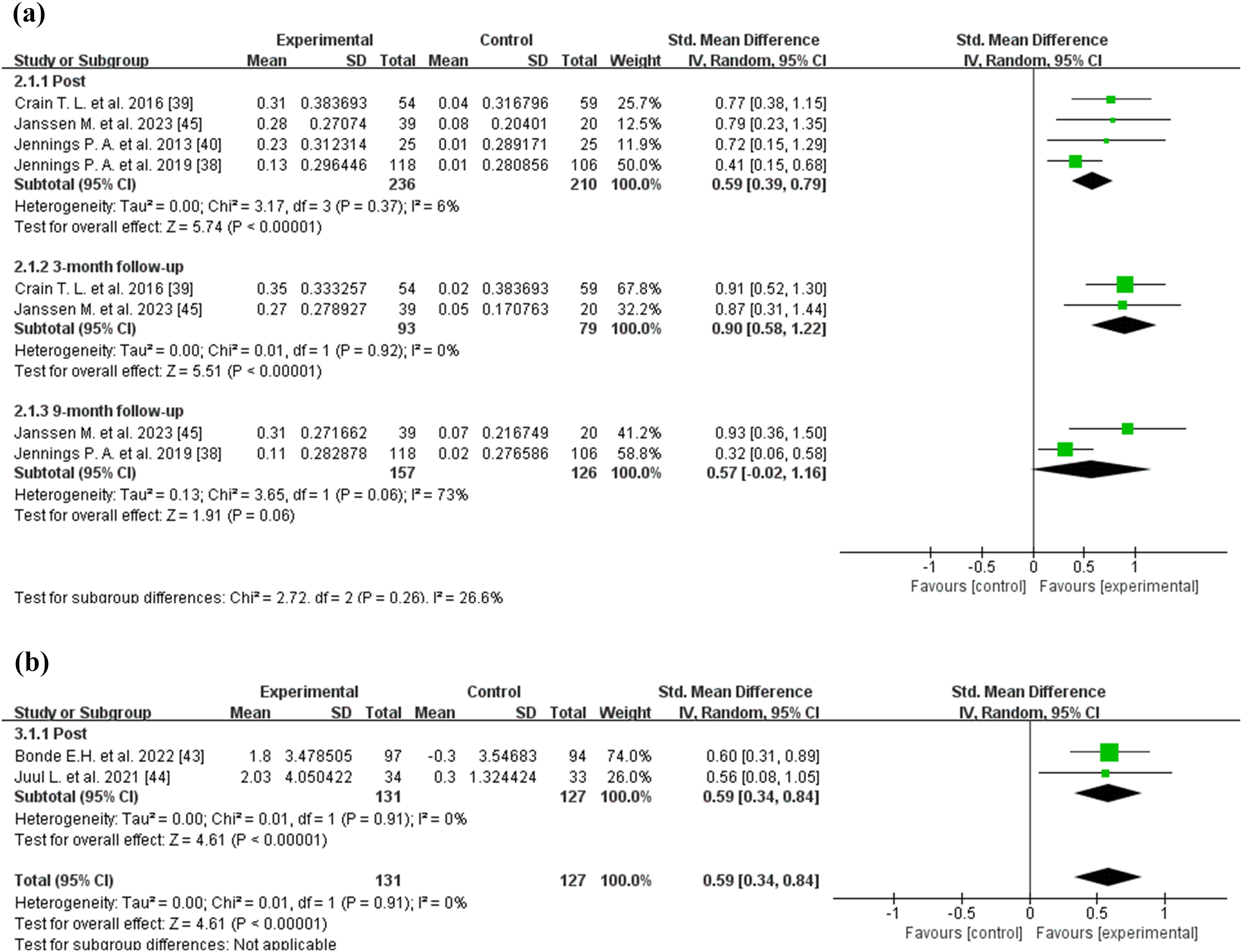
Forest plot of the meta-analysis for mindfulness facets (FFMQ). (a) Pooled effect on the total score of the FFMQ-39 at post-test and follow-up. (b) Pooled effect on the total score of the FFMQ-15 at post-test.
Analyses of FFMQ-39 dimensions revealed differential outcomes. The Observing capacity showed enhancement (SMD = 1.01, 95% CI = [0.33, 1.69], p = 0.004; I2 = 58%), and Describing ability demonstrated moderate improvement (SMD = 0.47, 95% CI = [0.08, 0.87], p = 0.018; I2 = 0%). Non-reactivity exhibited the strongest intervention effect (SMD = 0.90, 95% CI = [0.49, 1.31], p < 0.001, I2 = 0%). Conversely, the Acting with awareness (SMD = 0.22, p = 0.26) and Non-judging (SMD = −0.28, p = 0.55) dimensions showed insignificant changes (Supplementary File 3).
For the FFMQ-15, two RCTs revealed significant differences in total mindfulness scores (SMD = 0.59, 95% CI = [0.34, 0.84], p < 0.001, I2 = 0%, Figure 4(b)).
Effect on emotional affect
MBIs produced an enhancement in positive affect (SMD = 1.79, 95% CI = [0.86, 2.72], p < 0.001) alongside extreme heterogeneity (I2 = 87%). Intervention participants also showed a reduction in negative affect (SMD = −0.95, 95% CI = [−1.27, −0.62], p < 0.001, I2 = 24%, Figure 5).
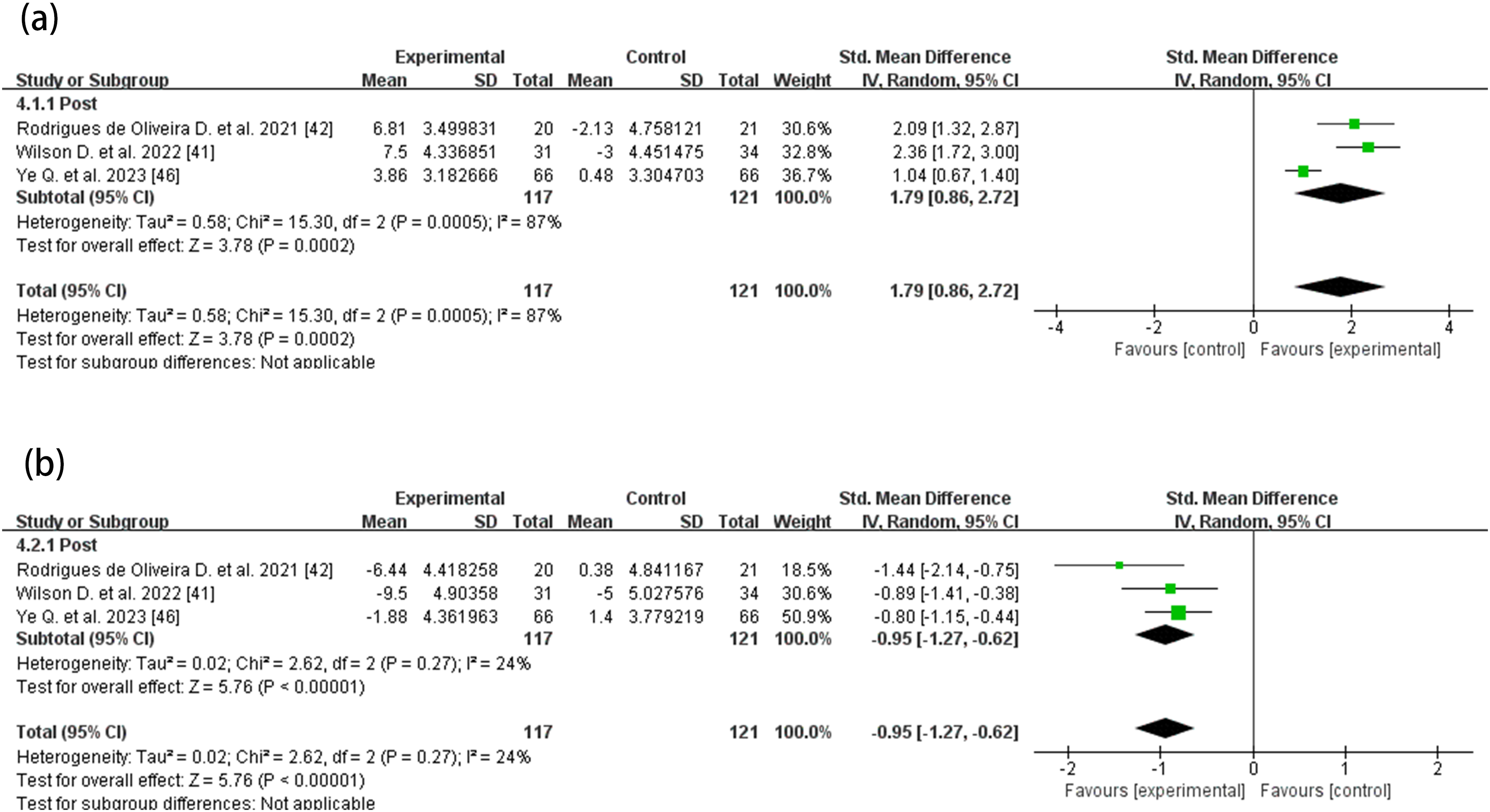
Forest plot of the meta-analysis for affect (PANAS). (a) Pooled effect on positive affect scores at post-test. (b) Pooled effect on negative affect scores at post-test.
Effect on resilience, depression, and well-being
Regarding other psychological metrics, RISC data demonstrated substantial intervention effects (SMD = 2.61, 95% CI = [1.96, 3.26], I2 = 33%). BRS analyses revealed moderate treatment effects (SMD = 0.50, 95% CI = [0.01, 0.99], p = 0.008, I2 = 0%). Furthermore, MBIs reduced depressive symptomatology, as measured by the SCL-5 (SMD = −0.84, 95% CI = [−1.47, −0.22], p = 0.008, I2 = 74%). MBIs also produced improvements in wellness (SMD = 0.94, 95% CI = [0.01, 1.88], p = 0.047, I2 = 88%), according to theWHO-5 (Supplementary File 3).
Sensitivity analyses
We noted considerable heterogeneity in the nine-month follow-up for FFMQ-Total, as well as in the domains of Observing, PSS, PANAS positive emotions, RISC, SCL-5, WHO-5, and BRS. We conducted sensitivity analyses on indicators represented by at least two studies, namely, FFMQ-39-Total, PSS, and PANAS, by sequentially omitting each study. We detected no reversal of outcome measures, suggesting stability across the included studies. The results are detailed in Supplementary File 2.
Adverse events
A systematic assessment of safety information across the included studies revealed that the majority did not report on adverse events. Only two studies mentioned such events: one outlined a management protocol without reporting actual occurrences, whereas the other documented two adverse events judged to be unrelated to the MBI.
Discussion
This systematic review synthesized evidence from 13 RCTs, demonstrating that MBIs effectively alleviate perceived stress among frontline teachers. Our meta-analysis revealed significant decreases in perceived stress and improvements in mindfulness skills, particularly within the Observing and Non-reactivity dimensions of the FFMQ. These cognitive enhancements facilitate better emotion regulation, thereby reducing anxiety, depression, and emotional exhaustion—all of which constitute key dimensions of job burnout. In meta-analytic research, findings of high or unclear risk typically indicate methodological flaws (e.g., inadequate allocation concealment, a lack of blinding, incomplete outcome data, or reporting bias). Such flaws may introduce systematic bias into the results. However, we assessed the studies included in our analysis as having low or moderate risk, ensuring their influence on the results is minimal. Overall, MBIs are effective tools for promoting the physical health and well-being of the teaching community.
Role of MBI in alleviating teachers’ work stress
The findings of this systematic review align with previous meta-analytic studies,30–32 demonstrating that MBIs significantly reduce perceived stress and enhance mindfulness levels among teachers. However, caution is warranted when interpreting this result, as the PSS is not a work-context-specific instrument. This implies that the intervention influence on job-related stress per se may not be fully captured, or alternatively, that the benefits of mindfulness generalize to overall stress perception. Furthermore, MBIs show positive effects on improving well-being and alleviating symptoms of depression. From a psychological perspective, MBIs foster metacognitive awareness, enabling individuals to reframe stressors cognitively and reduce automatic negative evaluations.49,50 Emerging evidence also highlights that the improvements in self-compassion and bodily awareness associated with MBIs serve as key resilience factors in managing occupational stress.51,52 The cross-diagnostic efficacy of MBIs observed across teachers, healthcare professionals, and students further underscores their broad applicability.44,53–55 These insights hold significant implications for the implementation of MBIs within educational contexts. Notably, we extend prior meta-analytic research by incorporating a multidimensional assessment of mindfulness and examining outcomes across multiple follow-up time points, thereby enhancing the understanding of the long-term effects of MBIs.
Furthermore, prior meta-analytic studies30,31 primarily examined the overall intervention effect of MBIs. By contrast, we clarified the differential responsiveness of each FFMQ dimension to MBIs. By moving beyond the general conclusion of “overall improvement in mindfulness levels,” our findings offer more precise evidence regarding the developmental mechanisms underlying MBIs. Our results indicate that MBIs did not achieve statistical significance in improving the Acting with Awareness (p = 0.26) and Non-judging (p = 0.15) subscales of the FFMQ. We attribute this to the possibility that short-term interventions may be insufficient to alter long-standing cognitive patterns and intrinsic psychological mechanisms.56,57 The primary challenge in enhancing Non-judging abilities lies in habitual tendency to evaluate internal experiences (e.g., emotions and thoughts)—a pattern closely linked to the amygdala-driven emotional processing pathway. 58 Conversely, Acting with Awareness involves the prefrontal cortex's ability to actively regulate attentional resources. 59 Neuroimaging evidence suggests that MBIs require at least 8 weeks to induce structural changes in the brain, whereas short-term interventions only produce temporary functional adaptations. Therefore, improvements in Acting with Awareness and Non-judging require sustained training to reconstruct neural network response patterns. 56
In addition, our findings indicate that short-term follow-up (<3 months) is associated with significant improvements in the total FFMQ-39 score, whereas long-term follow-up (3–9 months) does not demonstrate a statistically significant advantage. This absence of sustained benefit at 9 months may stem from insufficient sample sizes and potential declines in practice maintenance over time. In the long run, individuals may fail to maintain their initial practice frequency and intensity, leading to a gradual decline in mindfulness skills. 60 Furthermore, emotion regulation is a complex process, and MBIs likely represent only one component of the relationship between stress regulation and depressive symptoms. 61 As time progresses, other factors not adequately addressed by MBIs may influence stress regulation abilities, potentially contributing to the observed decline in FFMQ indices. Exploratory analyses also suggest a potential role for individual differences, as engagement, motivation, and personal traits may influence intervention effectiveness. 62 Although we based these results on a limited quantitative synthesis involving only two studies, the findings of Paudel et al. corroborated a similar trend. 31 However, these findings are hypothesis-generating and require cautious interpretation due to the limited data available. Critically, the evidence base for effects beyond 3 months is currently extremely limited and heterogeneous. These longer-term findings should be interpreted as exploratory only, highlighting the need for future research with larger samples, longer follow-ups, and dedicated maintenance strategies.
Identification of potential heterogeneity sources
Although our pooled quantitative results from the meta-analysis suggest that MBIs effectively reduce perceived stress among frontline teachers, we must acknowledge the presence of substantial to extreme statistical heterogeneity. Notably, this heterogeneity prominently appears in the comparisons of PSS between MBIs and the control group (I2 = 97%, Figure 3(a)) and between MBIs and cognitive-based intervention groups (I2 = 96%, Figure 3(b)). Moreover, significant heterogeneity exists in other outcomes, including positive affect (I2 = 87%, Figure 5(a)) and FFMQ-39 scores (I2 = 73%, Figure 4(a)). Due to the limited number of studies (n < 10), we could not perform subgroup analyses or meta-regression to determine specific sources of heterogeneity. Nevertheless, the results of our sensitivity analysis (Supplementary File 2) offer a foundational basis for qualitatively exploring potential sources from clinical and methodological standpoints.
Sensitivity analysis initially identified “geographic region” as a potential source of heterogeneity. As detailed in the sensitivity analysis results (Supplementary File 2), excluding the study by Qun Ye et al. 46 results in a dramatic decrease in heterogeneity from I2 = 96% to I2 = 0% for the comparison of perceived stress between MBIs and the cognitive-based intervention group. Qun Ye et al. 46 conducted their study in China, whereas the other two studies in this comparison involved research teams in Brazil. This marked geographic difference suggests that sociocultural contexts may act as a moderating factor in intervention effects, thereby constituting to the observed heterogeneity. 63 Core values differ markedly across sociocultural contexts. For instance, family often plays a central role in collectivist cultures, whereas individual autonomy receives higher value in cultures emphasizing personal choice.64,65 For interventions like MBIs, collectivist settings may more readily leverage core mechanisms, including context reappraisal and acceptance, to circumvent resistance driven by moral or role conflicts, thereby potentially enhancing effectiveness. 63 Moreover, geographic differences often accompany varying socioeconomic conditions, policy environments, and implementation resources, all of which profoundly influence the delivery pathways, acceptability, and ultimate effectiveness of MBIs. For instance, research on other interventions, such as a study promoting HPV vaccination among Hispanic populations in California, has demonstrated that language preference, socioeconomic status, and healthcare accessibility significantly influence outcomes. 66 These findings illustrate the broader impact of contextual factors, suggesting that MBIs may be similarly sensitive to cultural nuances. However, to definitively establish cultural moderation, studies directly comparing MBIs across diverse cultural contexts are essential. Consequently, researchers must adapt MBIs to the specific cultural background of the target population to ensure the alignment of core components with local values and practices. This imperative for cultural adaptation explains why the effects of a standardized MBI protocol exhibit variation across diverse geographic and cultural contexts. In addition to these factors, variables such as intervention duration and participant gender may also contribute to heterogeneity. We recommend that future research employ rigorous, well-powered subgroup analyses to more precisely examine the effects of these moderating factors.
In addition to clinical sources, methodological differences among the included studies may contribute to variations in the observed results. We applied the RoB 2 tool to assess the methodological quality and identify potential risks of bias. Our assessment revealed that five studies exhibited a moderate risk of bias in the domains of “Deviations from intended interventions” and “Measurement of the outcome.” Given the lack of adequate allocation concealment and blinding procedures in these studies, the risk of deviation from the intended intervention during implementation may increase. Specifically, none of these five studies reported a clear allocation concealment strategy, raising concerns regarding the “Deviations from intended interventions” domain. Allocation concealment is a critical mechanism for preventing selection bias. Its absence may introduce systematic errors through various pathways, thereby compromising the validity and reliability of study findings. 67 Failure to implement allocation concealment increases the likelihood of selection bias, which may distort the true effect of the intervention. 68 Furthermore, none of the five studies employed adequate blinding procedures, thereby increasing the risk of performance and detection biases. 69 This absence of blinding may inflate the perceived effectiveness of the intervention due to subjective influences from participants, researchers, or outcome assessors—particularly regarding subjective outcome measures. This significantly elevates the risk of bias within the “Measurement of the outcome” domain. In addition to procedural limitations, variability in measurement instruments contributes to the risk of bias. For instance, in the comparison of PPS (Figure 3(b)), all three studies used the same scale, but Ye et al. employed a Chinese-translated version. Although this version underwent reliability and validity testing, cultural adaptation may still introduce measurement bias, thereby increasing the risk of deviations in outcome measurement. 70 Collectively, methodological shortcomings may lead to trial results that deviate from true intervention effects. This could result in the inappropriate promotion of ineffective interventions or the underestimation of effective ones. These limitations also provide a plausible explanation for the extreme heterogeneity observed in the pooled quantitative results.
Application prospects
Follow-up assessments reveal that the positive effects of interventions remain evident 3 months post-intervention but tend to diminish by 9 months.38,45 These findings suggest that although MBIs provide significant short-term benefits for teachers’ mental health, researchers and practitioners must implement additional reinforcement measures to sustain long-term effects. Accordingly, educational authorities and school administrators should regularly incorporate MBIs into professional development plans and provide ongoing resource support. 21 Empirical evidence indicates that online MBIs can significantly reduce stress levels. 46 Accordingly, institutions should implement online MBIs as a cost-effective method to alleviate teacher stress, particularly in resource-constrained areas. These measures support teachers’ mental health while enhancing job satisfaction and teaching effectiveness, ultimately yielding positive effects on student education. 71
Strengths and limitations
We ensured research credibility through a comprehensive examination and analysis, employing strict inclusion and exclusion criteria while collecting RCTs from five databases (i.e., PubMed, EMBASE, Cochrane Library, Web of Science, and PsycINFO). Given that RCTs provide robust evidence for the effectiveness of MBIs and assist in controlling confounding variables at baseline, we only included RCTs. This study focused on the efficacy of MBIs in reducing stress levels among educators. These methods ensured conclusion validity through quality assessment and data integration. The necessity of this update is further underscored by the fact that 8 of the 13 included trials were published after 2019, demonstrating the rapid expansion of evidence since the last systematic search in 2018. Building on this fresh evidence, we moved beyond the global effect sizes reported in earlier syntheses by applying the FFMQ framework to quantify how individual mindfulness facets contribute to stress reduction. This approach replaced earlier coarse estimate with a precise multidimensional map, in which Observing and Non-reactivity emerged as the principal pathways. We extended the temporal horizon by tracking outcomes beyond the immediate post-intervention moment, which uncovered a time-dependent decay: the largest alleviation of stress occurred at the end of the program, remained robust within 3 months, and approached the threshold of significance by 9 months. These findings suggest that practitioners should schedule reinforcement strategies between 3 and 9 months to sustain clinical benefits. Nevertheless, this study has limitations. First, the PSS measures general perceived stress rather than specific occupational stress. This limits the precision with which we can attribute observed improvements solely to a reduction in professional strain. However, this limitation may be less pronounced in a teacher population, where work is a predominant stressor, resulting in a substantial overlap between general and work-related stress perceptions. Second, we limited the review to RCTs from five databases, which might have led to the exclusion of studies in other repositories. Due to the limited number of documents, we did not examine publication bias. This limitation suggests that future research should adopt more rigorous methodological criteria.
Conclusion
Our systematic review and meta-analysis of 13 RCTs indicate that MBIs significantly reduce teachers’ perceived stress and yield positive outcomes by enhancing mindfulness levels, improving emotional regulation, strengthening psychological resilience, and increasing overall well-being. Although short-term effects appear relatively stable, we find that the sustainability of long-term benefits requires further enhancement. Notably, substantial heterogeneity accompanies this conclusion, likely stemming from geographical and cultural differences, methodological variations, and other moderating factors. Furthermore, current evidence is limited by insufficient sample sizes, short follow-up durations, and a lack of demographic and contextual diversity in participant representation. Therefore, we recommend that future research prioritize enlarging sample sizes, extending follow-up periods, and incorporating diverse teacher populations across varied educational settings. Such efforts will enable a more comprehensive evaluation of the long-term efficacy of MBIs, help identify key moderators of intervention outcomes, and ultimately contribute to the development of robust, evidence-based strategies for supporting teachers’ mental health.
Supplemental Material
sj-docx-1-wor-10.1177_10519815261435990 - Supplemental material for Effects of mindfulness-based intervention on teachers’ work stress: A systematic review and meta-analysis of randomized controlled trials
Supplemental material, sj-docx-1-wor-10.1177_10519815261435990 for Effects of mindfulness-based intervention on teachers’ work stress: A systematic review and meta-analysis of randomized controlled trials by Zhixin Yan, Lei Wang, Binglin Chen and Jiabao Guo in WORK
Supplemental Material
sj-docx-2-wor-10.1177_10519815261435990 - Supplemental material for Effects of mindfulness-based intervention on teachers’ work stress: A systematic review and meta-analysis of randomized controlled trials
Supplemental material, sj-docx-2-wor-10.1177_10519815261435990 for Effects of mindfulness-based intervention on teachers’ work stress: A systematic review and meta-analysis of randomized controlled trials by Zhixin Yan, Lei Wang, Binglin Chen and Jiabao Guo in WORK
Supplemental Material
sj-docx-3-wor-10.1177_10519815261435990 - Supplemental material for Effects of mindfulness-based intervention on teachers’ work stress: A systematic review and meta-analysis of randomized controlled trials
Supplemental material, sj-docx-3-wor-10.1177_10519815261435990 for Effects of mindfulness-based intervention on teachers’ work stress: A systematic review and meta-analysis of randomized controlled trials by Zhixin Yan, Lei Wang, Binglin Chen and Jiabao Guo in WORK
Footnotes
Acknowledgements
The authors gratefully acknowledge Dr Deng Hongyong for providing the Python module for meta-analysis, which facilitated the conduct of sensitivity analyses. We also extend our sincere appreciation to all members of the research team for their valuable contributions and support.
Ethical approval
Not applicable.
Informed consent
Not applicable.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: General Project for Philosophy and Social Science Research in Universities of Jiangsu Province (grant. no. 2024SJYB0812, 2025SJYB0824).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.