
Abstract
Background
Researchers often file unsolicited comments included in data collection in the bottom drawer and exclude them from data analysis, despite such comments capturing raw and unfiltered perspectives. Research on psychological reactance often relies on direct measures, such as surveys or self-reports. While useful, these methods overlook spontaneous unsolicited comments, which are a critical source of unfiltered emotional insight that provides the explanatory context necessary to interpret observed outcomes, rather than merely describe them.
Objective
The aim of this study was to analyse unsolicited comments from employees in a workplace behavioural change intervention that used a choice default option design.
Method
The study sample comprised 139 desk-based employees working across government sites. The data consisted of unsolicited comments included in email correspondence from employees requesting withdrawal from the study.
Results
We identified two themes that reflected the presence of reactance motivation. These were negative cognitions (e.g., thoughts of unfairness) and anger (e.g., aggressive feelings towards the nudge), which are consistent with reactance models. Various sub-themes such as hyperbolic discounting and anxiety indicated the various emotional pathways for the development of reactance.
Conclusions
Our findings indicate that the use of a choice default option nudge as a design to bridge the gap between intention and action to change health behaviour can trigger negative spill-over effects which led to non-compliance. Given the unsolicited comments were accrued over a 12-month period, the trade-off between perceptions of a loss of freedom of choice and improved health might be acceptable to some individuals.
Keywords
Introduction
Workplace health interventions are increasingly recognised as vital opportunities to influence individuals’ health choices. While quantitative outcomes such as biometric changes and absenteeism rates are commonly used to evaluate these programmes, qualitative insights provide an added dimension to evaluation. 1 One often overlooked source of qualitative insight are peoples’ unsolicited comments (USC) regarding their experiences associated with participation in research projects. 2 USC constitute a unique non-traditional type of data. Often, individuals have a desire to narrate their experiences, context, cognitions, and feelings. These aspects of participation extend beyond the scope of traditional methods such as surveys or interviews. 2 USC are a form of communication that aligns with the idea that people make sense of their experiences by spontaneously constructing and sharing their stories. 3 As such they can reveal nuanced perceptions, emotional responses, and unintended consequences that forced-choice surveys and exit interviews often fail to capture. 2
These comments can include informal feedback, offhand remarks, or spontaneous reflections. USC are typically offered outside of formal evaluative structures. As such, USC analysis can provide insights into underlying organisational dynamics, employee sentiments, and cultural norms.4,5 Moreover, USC offer the potential to explore the gap between individuals’ self-perceptions and their actual behaviours.6,7 These data can give a more complete picture of how workplace health interventions impact individual health behaviour change.2,8 For example, examination of USC contained in travel diaries provided researchers with rich insights into children's lived experiences, emotions, and perceptions of mobility 8. Furthermore, in a health context, 87 per cent of patients in treatment for prostate cancer included USC on their survey forms. These data provided researchers with contextual depth, clarified survey responses, and revealed emotional and experiential nuances of cancer treatment not captured by structured items. 9 These examples demonstrate that analysing USC uncovers hidden contextual and social dimensions, offering a deeper understanding than structured surveys alone. This understanding, in turn, empowers health researchers to design interventions that are grounded in peoples’ own perceptions and emotional experiences. 10 Yet, few studies have systematically analysed USC to assess the broader psychosocial and behavioural outcomes of workplace health interventions. This study addresses that gap by examining USC collected during a nudge-based workplace health intervention designed to decrease prolonged occupational sitting. By analysing these narratives, we aim to uncover latent themes that reflect lived experiences and perceived value of the intervention beyond formal evaluation metrics.
While USC data offer a valuable window into people's research experiences, their use is constrained by several methodological limitations. A primary weakness is the predominant reliance on USC harvested from online comments, 11 survey questions, 2 and end-of-survey text boxes. 12 This approach introduces systematic sampling bias, privileging individuals who are digitally literate, highly engaged, and sufficiently motivated to provide retrospective or prompted commentary, while under-representing those who are less vocal or confident.13,14 Second, restricting lived experience data collection to structured interviews risks overlooking individuals’ in-situ expressions of meaning-making associated with everyday experiences of intervention involvement. USC data from informal workplace conversations, internal communications, or spontaneous reactions occurring during an intervention offers a unique perspective11,15,16 of psycho-social outcomes.
A current workplace health issue where USC data might provide beneficial insights about the effectiveness or otherwise of interventions is prolonged occupational sitting. 17 Prolonged occupational sitting refers to continuous periods of seated work, typically lasting one hour or more, performed as part of one's job duties.17–19 This occupational behaviour is associated with a range of health risks.20–22 Recent research highlights that prolonged sitting results in endothelial dysfunction and blood pooling which are physiological changes that increase risks for heart disease, diabetes, obesity, hypertension, and thrombosis. 21 These factors collectively contribute to elevated all-cause and cardiovascular disease mortality. 23 Prolonged occupational sitting is most prevalent among desk-based workers whose roles require sustained computer use, desk work, or other seated tasks. 24
Among a number of strategies to change workplace sitting habits25–28 one promising intervention strategy involves incorporating low-intensity physical activity (LIPA) breaks every hour into desk-based workers sitting habit. LIPA has been shown to mitigate the endothelial risks. 24 Moreover, there is the added benefit of a possible cross-over effect into leisure-time behaviour.23,24 Typically, workplace LIPA interventions incorporate a nudge in their design25,26 because occupational sitting is cue-contingent, rather than a voluntary behaviour. 29 Thus, prolonged sitting is a habit as it represents behaviour that is anchored in environmental and contextual cues, resulting in unconscious enactment. 30
Cue-contingent strategies are often superior for modifying habits because they disrupt automatic cognitive processes, reduce reliance on willpower, and can be sustained over time with minimal conscious effort. 31 Nudge-based health interventions are theoretically grounded in behavioural economics, which posits that human decisions are systematically influenced by cognitive biases and the design of the choice environment. 32 A nudge is aspect of the choice architecture that predictably alters people's behaviour without forbidding any options or significantly changing their economic incentives.32,33 By using simple prompts to disrupt habitual decisions, nudge interventions leverage the same cue-response architecture that underpins automatic habit formation, making them particularly effective for modifying habitual behaviours.34,35 For example, using a simple colour-coded prompt in a hospital cafeteria significantly increased the purchase of the highlighted healthier food options from other choices. 36 Consequently, cue-contingent strategies, which work with rather than against automatic cognitive processes, often demonstrate superior sustainability for long-term behaviour change compared to interventions reliant on willpower.37,38
Although nudges share a common theoretical foundation in behavioural economics they constitute a heterogeneous set of interventions, each operating through distinct psychological pathways. 33 Nudge categories reflect a soft paternalism approach, 32 which allows individuals to reject the preferred option and maintain their habitual choice. 34 Major categories include salience nudges (e.g., visual or auditory prompts), social norm nudges (e.g., peer comparison messaging), framing nudges (e.g., gain- or loss-framed information), and default option nudges (e.g., pre-selected options requiring opt-out). 33 While nudges are effective behaviour change tools, studies report heterogeneous treatment effects, 37 unexpected outcomes, 38 and negative spill-over effects. 39 In response to this variability, some advocate for more paternalistic nudge designs such as choice defaults.40–42
Choice defaults that use an opt out design capitalise on status quo bias and the tendency toward effort minimisation, effectively automating choice to the desired behaviour by pre-setting it as the standard option.42,43 This design removes preference uncertainty because individuals are automatically assigned to the preferred behaviour choice, ceding almost all of their decision-making autonomy and potentially forming a bridge between intention and action. 43 While compliance rates are often higher in a choice default design, there are also negative spill-over effects similar to those observed in nudge designs that use an opt in mechanism. 39 For example, using an opt out mechanism can result in people perceiving a loss of autonomy in decision making, which can trigger feelings of psychological reactance, leading to the rejection of the preferred behaviour choice.44,45
Reactance is a motivational state that occurs when individuals perceive their freedom of choice threatened or eliminated. 46 In response, individuals may engage in non-compliance or adopt the opposing attitude or behaviour, a phenomenon known as the boomerang effect. 47 For example, a study on organ donation registration 43 employed a choice default strategy, in which citizens were automatically enrolled as donors unless they actively opted out. This approach triggered reactance in individuals with a high need for autonomy. Consequently, these individuals intentionally opted out, even if they otherwise held positive attitudes toward donation, as a means of reasserting their perceived freedom of choice.
Although a later study 48 reported that participants did not feel their autonomy was compromised and consequently exhibited low levels of reactance. The authors concluded that well-designed opt-out systems for organ donation can be implemented without backfiring, as they do not cause widespread feelings of coercion or rebellion, thereby preserving a sense of autonomous choice among the public. These contrasting findings suggest that while choice default nudges with opt-out mechanisms risk triggering reactance in autonomy-focused individuals, careful policy design can mitigate this effect and preserve public perceptions of autonomous choice.
Yet, measurement of reactance feelings is challenging. One major issue is its conceptual complexity as reactance encompasses both affective components (i.e., anger) and cognitive elements (i.e., counterarguing). 49 Many early measures of reactance failed to capture this multidimensionality.49,50 There is also ongoing debate about whether reactance should be assessed as a stable personality trait or as a situational state, 49 with tools like the Hong Psychological Reactance Scale (HPRS). 51 Though this scale has low internal consistency and limited construct validity. 51 Additionally, self-report measures can inadvertently provoke reactance themselves, introducing bias into the data. 52 Cultural variability further complicates measurement, as expressions of reactance may differ across cultural contexts, raising concerns about the cross-cultural applicability of existing instruments. 52 Moreover, most tools are static and retrospective, which is problematic given the dynamic and often short-lived nature of reactance. There is growing support for multi-method approaches to improve the assessment of reactance.53–55
Serendipitously, the authors were made aware of the existence of USC derived from a broader intervention study, 26 where volunteer government desk-based participants were exposed to a choice default option nudge during the workday. The nudge automatically assigned participants to the preferred behaviour of taking an hourly movement break from their prolonged sitting position. The design included an opt out trigger whereby participants could send an email to the researchers requesting removal of the e-health application from their computers. An unintended outcome of this protocol was some include USC in the emails, which provided, unplanned insights into their experiences. Following a preliminary analysis of the USC data, the authors identified an opportunity to contribute to scholarly calls for multi-method approaches by using USC to elucidate both individual responses to a choice default nudge and the emergence of reactance.
Thematic analysis was used to explore participants’ lived experiences as expressed via their USC. This approach captured the voices of participants directly, free from interviewer bias, providing unique insights into their reactions to a workplace intervention designed to change their workplace health behaviour to mitigate a health risk. Despite the insights generated through qualitative approaches, much of this research relies on data elicited through structured questioning. As a result, responses may be influenced by the framing of interview protocols and the assumptions embedded within the research design. An alternative and complementary source of insight may be found in the USC offered by participants involved in workplace interventions designed to reduce their occupational sitting habit. Because these remarks arise spontaneously, often outside the formal structure of survey items or interview prompts, USC may capture reflections, frustrations, and practical experiences that participants themselves perceive as salient within their work environment.
Analysing USC generated during workplace interventions may therefore provide a more nuanced understanding of how participants negotiate attempts to modify sitting behaviour within organisational settings, including unexpected spill-over effects. In this way, USC may reveal dimensions of the workplace experience that more structured qualitative approaches do not readily capture. Consequently, our understanding of the individual impact of such interventions has a risk of being superficial. By analysing USC collected in a primary study, we aim to uncover latent themes that reflect participants’ lived experiences and perceived value of the intervention beyond formal evaluation metrics.
The analysis underscores the importance of incorporating a multi-dimensional approach53–55 to explore individual perspectives in an attempt to provide a nuanced understanding of perceptions, emotional responses, and unintended consequences of changing workplace health behaviour. 2
Methods
This analysis draws on USC provided by staff during a workplace health intervention. Accordingly, from this point forward we refer to participants as “employees” or “employee” to emphasise that their spontaneous remarks arise from, and speak to, their lived experiences within the occupational setting and thus offering insights that extend beyond what traditional data can capture. The term employee (s) also humanises the data.
Ethical and moral protocols
Transparency and openness
We followed the Standards for Reporting Qualitative Research. 56 Data collection for the primary purpose of this study proceeded in line with ethical approval from the University of Tasmania (Ref# H0018075). Our ethics included permission to use data from all employees’ communications. Deidentified data are available upon reasonable requests. As part of the ethical protocol to ensure transparency,56,57 desk-based employees were informed of the link between prolonged occupational sitting and possible deleterious health outcomes. 21 All employees voluntarily agreed to participate.
Ethical and moral protocols
Consistent with ethical and moral protocols for nudge interventions57,58 the researchers informed employees about the behaviour change strategy of a choice default option design. In the intervention design, employees consented to be automatically assigned to the preferred behaviour until they decided to opt out. 55 To opt out of the study, employees had to make a conscious decision to send an email to a research assistant requesting their withdrawal from the study. No other information was requested by the researchers in these emails. This procedure was required to enable the research assistant to remove the e-health application from employees’ computers. Having an opt out mechanism was consistent with previous choice default designs to allow autonomy and to take into consideration the context of the environment.57–59
Sample and dataset
The data for this study were derived via purposive sampling from a broader project, 26 specifically from self-reported USC within opt-out emails. These anonymised data were identified post hoc during broader project's finalisation processes, rendering them a serendipitous dataset. Consequently, this is a secondary analysis that is inherently exploratory and does not support causal inference, comparative assessment, or experiential verification.
Behavioural design
Nudge theory underpinned the intervention's protocol, 32 which posits that subtle changes in choice architecture can effectively influence behaviour. To enhance the nudge's effectiveness, we employed a choice default, with an opt out frame condition. As with previous studies25,26,43 this design reflects a minimum commitment requirement with active decision making to opt out. The nudge automatically allocated employees to the choice of hourly short movement breaks, which consisted of LIPA of their choice. To enhance the preferred choice, employees’ computer screens, which are a contextual cue, were deactivated until employees self-reported their movement activities. This altered the choice architecture by introducing decision-making friction. 31
Consequently, the addition of the new behaviour option to the existing sitting habit became the path of least resistance for employees seeking to resume their primary task.30,31,35 The intervention design was presented to employees as a gain-framed intervention by emphasising the health benefits of taking a movement break comprised of LIPA. 24 Given that habit formation requires consistent cues and repetition, 34 58–60 the nudge was delivered by e-health software hourly during work hours.
Researcher positionality and reflexivity
In qualitative research, the researchers themselves are instruments of analysis, making it essential to acknowledge their positionality. 1 The analysis team comprised four researchers with backgrounds in sport science, health psychology, and organisational behaviour. All authors shared an interest in behaviour change interventions but brought different perspectives on their application in workplace settings. To manage the influence of these preconceptions, each author maintained a reflexive journal throughout the analytical process, documenting their thoughts, assumptions, and interpretations. 61 These journals were discussed during team meetings to surface and bracket potential biases. This practice aligns with recommendations for ensuring rigour in qualitative thematic analysis.1,61
Coding procedures
After all authors had read the data, they agreed to employ thematic analysis 1 with elements from grounded theory, 61 specifically theoretical sensitivity. 62 Open coding followed four guidelines: (1) asking consistent questions of the data, (2) analysing data minutely, (3) writing memos and conducting checks during coding, and (4) avoiding assumptions about traditional variables. 1 All data from the opt-out emails were included in the initial analysis; no data were discarded a priori as outliers, given that in qualitative research, every data point is considered potentially meaningful.61,62
Triangulation and validity
We established validity through triangulation between the authors,1,61 with team members independently verifying themes and interpretations. Reliability was ensured through two key processes: first, by organising and consistently updating the data in MS Excel, which facilitated the clear construction of emergent themes supported by evidence; and second, by employing theoretical triangulation to cross-reference our findings with existing literature.1,61 The updated tables allowed quick interpretation of the results to aid the concise construction of matching emergent themes with evidence. Reliability was ensured through theoretical triangulation,61,62 where findings were cross-referenced with existing literature to support data interpretation. Determining sample size was guided by the principle of saturation. 63 But this was problematic as the data were serendipitous and thus, we had no prior opportunity to establish relevant numbers or obtain further commentary from employees. 63
A review of previous literature regarding the analysis of USC revealed no established protocols. 8 Therefore, we adopted a nuanced approach to saturation. 63 We assessed two types of saturation. Code saturation, defined as the point when no new themes or codes emerged from the data; and meaning saturation, defined as the point when we, as researchers, felt we had a comprehensive understanding of the dataset. 63 Given that USC are typically fragmented and short, we decided that to ensure qualitative rigour, we used a numerical saturation whereby a theme would require inclusion in a minimum of 50 comments, and a subtheme in a minimum of 10. This numerical framing positions our 50/10 rule not as arbitrary, but a deliberate, justified methodological choice suited to the unique data type. 64 We selected these thresholds through an iterative consensus process among authors, based on our collective reading of the dataset and the need to balance inclusivity with meaningful pattern detection, a decision consistent with guidance on establishing rigour in unconventional qualitative datasets. 65
Thematic development
For all coding (see Appendix 1), the first 3 authors kept a journal of their thoughts and reflections while coding the data. This journaling provided contextual reference for each author in the final meeting. In Phase 1, before commencing, all authors examined that data set and agreed that analysis could provide additional understanding of the intervention. 26 All authors agreed on the aim of the project and the methodology for analysis. In phase 2, the first author independently read all data for each time point (i.e., 3-, 6-, 9-, and 12-month intervals). Using an inductive process, he sorted the data into four codes by identifying the main idea or ‘relevance’ expressed in each statement. Coded data were transferred to a second spreadsheet. In phase 3, the first and second authors met to discuss the coded data on the second spreadsheet and explore a range of possible theories that might fit the codes (i.e., substantive content). Both authors were familiar with social psychological theories used to explain people's reactions to nudge interventions. 61 The first and second authors agreed that coded USC reflected elements of reactance theory. 46
In particular, the intertwined model of reactance 50 was selected as it defines reactance as a latent motivational state, whereby it is an internal, unobservable drive, that emerges from the interaction of negative cognitions (e.g., counterarguments) and negative affect (e.g., anger) in response to perceived threats to freedom. Moreover, the model posits various combinations of components can combine to trigger reactance motivation resulting in behavioural outcomes, such as resistance or defiance. This model highlights the dynamic interplay between cognitive and emotional responses in shaping reactions to persuasive attempts.47–50 We therefore used the model's components as an analytic framework to guide further coding. This abductive approach of moving between data and theory, is well-established in qualitative research and strengthens the theoretical grounding of findings while remaining responsive to the data. 65
In phase 4, the first two authors developed a framework of definitions to categorise the data set. The factors contained in the intertwined model for reactance served as the definitions. 50 The first and second authors then analysed the data set developed in phase 2 using the agreed definitions. Once completed, the spreadsheet analysis was sent to the third author, who independently checked the data analysis and confirmed or highlighted any issues of ambiguity and inconsistency. No data were treated as missing in the conventional sense,62,63 as USC were voluntarily provided; however, we acknowledge the absence of data from those who opted out but provided no USC as a key limitation in Section 2.8.
Subsequently, the first three authors met and discussed the same spreadsheet data analysis, agreed on the categorical sort, discussed any issues, identified emergent themes, and discarded data that did not fit the agreed theoretical categories (i.e., analytic usefulness). 61 Once agreement had been reached, the data set was sent to the fourth author (Phase 5). This author was independent of all previous analysis phases. The fourth author acted as an independent moderator to conduct a check by engaging with the spreadsheet data set, the agreed categories, the naming of themes, and the evidence for each theme. 61 In phase 6, all authors met and agreed upon themes and which narratives would be used to support their conclusions. Major themes were negative cognitions and negative affect. Sub-themes included hyperbolic discounting, counterarguments, anxiety, irritability, and derogation.
Limitations
Using USC as a source for determining meaning has inherent limitations. 8 USC are fragmented, irregular in content, and in this case, obtained serendipitously. 9 As the USC were submitted and underwent an anonymising process, the researchers were precluded from the opportunity for follow-up questions or probing for deeper explanation.1,61 This is a recognised constraint of using USC data compared to interactive methods like interviews or focus groups. 61 Consequently, the analysis is necessarily confined to the provided textual data, without the ability to clarify ambiguities or explore emerging themes in greater depth with the employees.64,65 Similarly, there is no comparative data to refute the USC used in the analysis. 1 Thus, the transferability is only applicable to the context of the research intervention and limited generalisability to employees who chose to withdraw and submitted USC with the email request. 65 Hence, these data offer rich and authentic insights into the experiences and perspectives of only this specific group of employees.
Readers can assess the relevance of these themes to their own contexts based on our description. In conclusion, while the unsolicited nature of the comments presents specific limitations regarding depth and follow-up, we have endeavoured to analyse the data with maximum rigour. 62 Thus, the conclusions presented are our best interpretation of the salient themes present within the dataset; grounded in employees’ own words and derived through a transparent and systematic analytical process.
Results
Descriptive statistics
From the broader study, Mainsbridge et al. 26 of the 3922 employees available from office sites, most (94%) worked in single-storey buildings, with the remaining working in multiple-floored buildings such as urban office centres or hospitals. Recruitment focused on desked-based workers who responded to an email invitation to participate in a study designed to reduce prolonged sitting. Response to the email realised 228 (85% female aged 45 + 10.5) consenting adults for the study. Baseline measures indicated a range of diseases/disorders: chronic pain (34.6%), respiratory disease (28%), gastrointestinal issues (20.2%), and hypertension (8.8%), with 18 taking hypertensive medication. A number (82%) indicated wanting to lose weight as the primary reason for being in the study. This potential outcome was not mentioned in the study's ethical preamble. Across all sites, total recruitment at baseline was 228.
Over the 12-month trial period of the broader study, Fifolt et al. 2 there was attrition (55 at baseline, 42 at 3 months, 21 at 6 months, and 16 at 12 months). Out of the total number of withdrawals (n = 134), some included USC (N = 328) in their withdrawal emails. In many cases, people included multiple comments in their emails. For example, if an employee made a salutation and referred to another issue not associated with the study, each was counted as a distinct comment, thus explaining the high number of USC. After removing unusable comments (n = 196) for various reasons (e.g., technology issues, ad hoc salutations), 132 USC formed the data for analysis. These comments were reported across all time points: 45 at 3 months, 31 at 6 months, 41 at 9 months, and 15 at 12 months. The discrepancy between numbers and total comments for the analysis exists because some people (n = 34) provided multiple email communications.
Qualitative results
In our reporting, the primary themes have been designated unique numbers, with sub-themes designated continuous letters to reflect the intertwined nature of cognitions and feelings. We have included extra contextualisation to enhance understanding by illustrating the depth, nuance, and complexity of findings, to allow an appreciation of the employees’ perspectives and the impact of emergent themes within their real-world context.60,62
The analysis revealed evidence supporting the presence of reactance motivation as a precursor to some employees’ decisions to opt out of the intervention. These findings align with the intertwined reactance model, 50 which operationalises a reactance motivational state as an amalgamation of negative cognitions and feelings of anger, leading to behavioural responses of negative cognitions and feelings of anger that leads to a behavioural response.66,67 Using the operational definition 65 and the subsequent outcomes,66,67 the data were coded into two primary themes: negative cognitive thoughts (n = 58) and anger feelings (n = 56). Data that did not fit the coding criteria (n = 18) were re-examined for possible coding into sub-themes but were ultimately discarded due to ambiguity.
The core proposition emerging from the analysis modifies the traditional adage: “The doctor knows best” 68 to “the doctor knows best but only up to a point”. This proposition unites the two themes of negative cognitions and anger, reflecting employees’ implicit acceptance of being automatically opted into the preferred behaviour initially. Nonetheless, over time some employees developed negative cognitions and feelings of anger toward the nudge, rejecting the trade-off between a perceived loss of freedom and the promise of distant health benefits. This loss of acceptance occurred across various time points, but when it did, it manifested in people taking positive action and opting out of the default behaviour. All themes and sub-themes met the pre-determined numbers for acceptance.
Theme 1: Negative cognitions
Sub-theme A: Hyperbolic discounting
This cognitive bias reflects impulsive decision-making wherein individuals prefer smaller, immediate rewards over larger, delayed ones, with the perceived value of future outcomes decreasing sharply over time.69,70 This pattern emerged as employees explicitly recognised the intervention's long-term benefits yet withdrew in favour of short-term convenience. A characteristic tension was observed: while employees acknowledged the programme's effectiveness, they prioritised immediate comfort over sustained health gains. This dynamic was evident in USC (n = 15) that devalued the target behaviour (taking active breaks) while overvaluing the alternative (continuing to sit). For example, one respondent who opted out after three months articulated this conflict clearly: The program has got me thinking more about how long I have been sitting. In the past when I have been busy, I could have sat for several hours without taking a break. This would result in me having a stiff back and not being able to straighten up until I had walked for a few minutes. This has not occurred while I have been on the program. I also have had significant lower back pain in the past … It was as a result of one of these episodes that I decided to enrol into the program. I can’t remember having any back pain during the program … the program is very annoying during work, please remove it.
Hyperbolic discounting
69
was also evident when employees reframed their withdrawal as a positive outcome, effectively enjoying the partial benefits to justify ending their participation. This pattern represents a subtle form of discounting, where the immediate reward of ending an intrusive programme is preferred over the future benefits of continued engagement. As one employee remarked after nine months: … in its current form I’m finding it more intrusive than useful. So, thank you so much for the opportunity to be involved. Even though I won’t be using it again (… can you arrange to have it taken off the PC?) it has definitely made me more mindful of exercise, and more active in the workplace.
Sub-theme B: Counterargument
Counterarguing 71 represents a cognitive and rhetorical strategy where individuals mentally refute persuasive messages to resist attitude change. In the context of this intervention, employees employed counterarguments not merely to reject the programme's premise, but to actively defend their existing behaviours as a means to possibly reassert autonomy. This process often involved acknowledging the intervention's logic while simultaneously dismantling its personal relevance, which is a form of motivated reasoning that served to protect behavioural freedom.
This pattern emerged clearly in withdrawal comments (n = 43) where employees contested the necessity or added value of the nudge, despite recognising its underlying health rationale. For example, one employee wrote after three months: After participating in the study, I am much more aware of how and when I move at work. I now much better understand when activity will occur naturally in the course of my day, and when it won’t. I now know when I need to take action myself to ensure I move frequently, even relatively minor movements such as standing up to take phone calls (so, I learnt that I move quite often already – even in a changed & more sedentary role; when I started the study, I don’t think I sat for more than 30 min at a time! it's still an office job, with lots of sitting, but mostly quite broken up rather than long stationary durations. I almost always walk briskly and take stairs whenever possible – but I couldn’t credit the study for this, sorry!.
Theme 2: Anger
As conceptualised within the intertwined model of psychological reactance 50 people's feelings of reactance may emerge from an anger response. This is in line with the original description of the relationship between nudging and reactance 45 and included in the intertwined model.50,71 Anger encompasses a range of hostile or aggressive feelings, which can be connected to the source that is perceived to be removing freedom rather than to the message itself. 71
Sub-theme C: Anxiety
The experience of anxiety emerged as a noteworthy barrier to sustained engagement, particularly when the intervention was perceived as threatening cognitive or emotional security.
70
Anxiety responses, often triggered during periods of work pressure, transformed the choice default option nudge from a helpful decision prompt into a stressor that some employees actively sought as a reason to opt out of the study.
72
This pattern was reflected in withdrawal messages (n = 19) where anxiety was directly attributed to the intervention itself. As one employee explained when opting out at the six-month stage: … I have had the program taken off my machine … The behaviour was ‘creating’ anxiety when I was under pressure, and it interrupted stream of thought … The program irritated me and certainly did not encourage me to move more. Another employee opting out after 3 months wrote: Could you please remove the program from my computer, I have found it very distracting and breaks my concentration, there are times it increases my stress levels rather than lower! Please remove it!
Sub-theme D: Irritation
Irritation is a state of annoyance closely intertwined with anger.71,72 The experience of irritation represents a key affective component of psychological reactance, arising when individuals perceive their autonomy threatened by external messages or intervention.
73
The affective feeling emerged as a common employee emotional response to the choice default option nudge that pre-selected a preferred behaviour choice. For some employees, the hourly movement commitment disrupted established work rhythms, gradually transforming the initial disruption to the sitting habit into sustained irritation. This escalation was particularly evident when the nudge design conflicted with some employees’ immediate work task demands, framing the nudge as an arbitrary obstacle rather than a supportive strategy. For some, this developed into irritation over time. This dynamic was captured in USC (n = 21) where irritation was explicitly linked to mounting frustration. As one employee noted after six months: I actually found it very annoying … when I would get back to my desk it would be wanting me to do something and so I would be having to make something up to log in the record because I wouldn’t then have the time to do something else as well … having some more flexibility about postponing or indicating that you didn’t need to for some other reason would have made it more user friendly for me. Thanks, I still think it is a worthwhile program.
Sub-theme E: Self-derogation
Self-derogation, the tendency to disparage oneself, where perceived standards feel unattainable74,75 emerged as an outcome for some (n = 16). This negative state has not been previous reported in the reactance literature, but it is particularly salient in controlling or prescriptive intervention environments. In such contexts, where people perceive an undermining of personal efficacy beliefs, negative personal evaluations might drive a desire to reject the imposed behaviour. 75 Within this study, some employees reported experiencing feelings of self-derogation did not merely express difficulty with being automatically allocated to the preferred behaviour, but internalised the struggle as a personal failing, framing their inability to adhere as a characterological deficit.
This internalisation of failure was evident in some employees’ USC (n = 16) where they attributed their withdrawal to perceived personal inadequacy rather than the intervention design. One respondent articulated this self-critical narrative after nine months: 1 found it really disruptive to my working day and I didn’t do enough activity when I did the program to make any difference to my health in my opinion … this made me feel guilty about doing the program … If I smoked, I would get more exercise during my working day.
Discussion
This study explored employees’ lived experiences of a workplace choice default nudge intervention aimed at reducing prolonged sitting, focusing specifically on the psychological processes that led them to opt out. Overall, our findings reveal a paradox: even when advice and intentions are sound, employees who develop negative cognitions and emotions toward the intervention strategy may ultimately resist the very behaviour intended to benefit them. This emphasises our core proposition that the doctor knows best but only up to a point. 68 There were three key findings to support this proposition. First, USC represent a unique form of qualitative data, capturing employees’ lived experiences in an unfiltered and spontaneous manner, free from researcher-induced bias.8,9 Second, the USC provided valuable insight, into the negative emotional and cognitive responses consistent with reactance theory. 50 Moreover, the pattern of USC and opting out was not homogeneous. Third, some employees experienced a negative spill-over effect, which manifested in opting out as a possible means of restoring their freedom of choice. 57 These findings underscore a fundamental tension in workplace health intervention design. Automatically nudging employees toward a preferred behaviour, though intended to bridge the intention-action gap, 35 may simultaneously restrict autonomy and disrupt work routines, generating possible resistance motivation. 45
In addition to its substantive findings, this study offers a methodological contribution to the field of workplace health intervention research. The analysis and findings demonstrate that USC represent a valuable data source for revealing unintended outcomes.53–55 Unlike surveys or interviews, which can impose researcher-defined categories and risk social desirability bias, USC capture employees’ lived experiences spontaneously, in their own words, and at the moment of meaning-making.4–6 Collecting and analysing these data responds directly to calls for greater diversity in the assessment of psychosocial outcomes. 15 For workplace practitioners and researchers, this methodological approach suggests that embedding opportunities for employees to make anonymous comments during data collection may hold untapped potential for detecting unanticipated responses to intervention designs. Attending to such data could provide early warning signals of problematic dynamics and inform more attuned workplace health strategies.5,57
Workplaces are ideal settings for changing individual health behaviours due to the time people spend at work and the high potential for crossover impacts to leisure time behaviour.23,24 Prolonged sitting poses unique health risks for desk-based employees,17,19,21 which can be mitigated by breaking up sitting time with periodic LIPA. 24 A cue-contingent strategy of choice default nudging 33 is designed to bridge the intention-action gap and engineer behaviour change without disrupting work routines. Building on the emotional and cognitive responses identified in our second key finding, the USC provided a novel, micro-level perspective on the outcomes associated with the intervention strategy. 7 The outcomes were not dissimilar to those previously reported for choice default nudge strategies.25,26 Such a strategy can inadvertently create negative emotional and cognitive outcomes in employees39,40 but consideration of potential benefit should also be included in any assessment of effect. 38 Choice default nudge designs are a common strategy in public health and clinical campaigns.40,41 The application to workplace interventions that target employee health behaviour choices is less common. Our results indicate that a choice default strategy can be simultaneously effective for some and problematic for others. 35
The effectiveness of the choice default nudge was not formally assessed in this analysis in terms of adherence. Nonetheless, it is noteworthy that only just over half of the employees opted out during the 12-month trial period, which may be interpreted positively. This result is not an endorsement of the strategy,41–43 but it does indicate that some employees are willing to tolerate being automatically allocated to a preferred individual health behaviour. Notably, even among employees who ultimately opted out, several remained in the intervention for up to 12 months before discontinuing. This sustained participation, persisting through the 9- or 12-month milestones, reflects a meaningful period of engagement and aligns with the temporal development of reactance motivation. 50
This pattern is consistent with theoretical accounts distinguishing between the experience of reactance and its behavioural expression.35,40,41,43 According to the intertwined model, 50 reactance motivation is the behavioural outcome the presence of various constituent parts.50,53,55 The presence of the constituent parts does not invariably lead to behavioural non-compliance, rather the conversion of reactance motivation into action depends upon contextual factors, including personal motivation, the availability and perceived feasibility of freedom-restoration pathways. 46 Our findings possibly suggest the default behaviour aligned with employees’ motivation. Our study was presented to employees with a gain-framed emphasis. As participation was voluntary, it is possible that employees were expecting a health benefit. Some employees’ USC indicated they were experiencing positive health changes. Nonetheless, these benefits were intertwined with the presence of negative components (i.e., hyperbolic discounting, counterarguments), which is reflective of the model. 50 In our study, as with previous studies, 48 the opt out frame provides a pathway to resolve the conflict between benefit and loss.
An intriguing possibility raised by our findings is that some employees who opted out after prolonged engagement may have done so because they believed they had successfully modified their sitting habit to include taking LIPA movement breaks. Some USC contained examples of employees indicating that they were aware of the importance of taking movement breaks but preferred to initiate the break on their own terms. From a reactance perspective, 46 once behaviour becomes automatic, 60 continued nudging may shift from being perceived as supportive to being experienced as autonomy-infringing and unnecessary. 67 This could have transformed our well-intentioned nudge into a freedom threat, triggering reactance and motivating withdrawal.44,45 Consistent with goal-directed reactance, 76 employees may have opted-out as a means of restoring autonomy precisely when there was no need to be continually nudged. For occupational health practitioners, this finding suggests choice defaults may be efficacious39–42 when the targeted behaviour aligns with employees’ existing motivation 77 as a strategy to overcome the intention-action gap. However, once goal directed behaviour has become habitual, continual nudging may be counterproductive.44,47
Problematic to our interpretation, employees’ USC indicated that, at a certain point, their experience of a range negative emotions and cognitions consistent with motivational reactance resulted in opting out. This finding is consistent with previous studies.43–45 We interpreted this finding as revealing a sequence whereby employees who recognise a workplace habit as a health risk may initially accept a choice default as a motivational mechanism to translate intention to action. 38 In doing so, employees temporarily ignored the presence of negative cognitions and emotions to reduce their health risk.67,78 This trade-off of momentarily accepting reduced autonomy to achieve a health goal reveals the complexity of workplace behavioural decision-making. It suggests that while some employees may be motivated to change, their path to action is not straightforward; it is negotiated against a backdrop of default choices76,79,80 and potentially competing pressures, such as workplace culture or the demands of completing work tasks.81,82
Our interpretation of employees’ USC is that their experience of the choice default nudge resulted in the development of negative cognitions and anger, which align with the intertwined reactance model. 50 This interpretation of a causal pathway, however, remains largely speculative, as no USC explicitly mentioned a desire to regain autonomy as the foundation for opting out. Furthermore, nor did any indicate that opting out reflected the establishment of a modified habit, such as having embedded LIPA movement breaks into their work routine. Rather, the data suggest a negative pathway consistent with the intertwined reactance model. 50 For workplace health intervention design, this finding sounds a note of caution. Employers and workplace health professionals who design and implement choice default interventions aimed at shaping employee habits, whether health-related or otherwise, must weigh the potential for unintended consequences that could offset the intended benefits.
Further to these problematic issues, our third finding was interpretive but speculative. Emerging from the analysis, employees’ USC, voluntarily given at the point of opting out, were suggestive of attempts at freedom restoration. 46 This interpretation is consistent with the intertwined model, 50 but we identified no causal pathway. Rather, the USC signalled the presence of constituent components of the reactive state.69–75, 78 For workplace intervention design, the third finding sounds a note of caution. While these constituent components trigger reactance, 50 alternative explanations warrant consideration. Withdrawal may also reflect cognitive dissonance reduction, dispositional trait reactance, or legitimacy perceptions regarding the intervention source. 77 Employers and workplace health professionals who design and implement choice default interventions to shape employee habits, whether health-related or otherwise, must weigh the potential for unintended consequences that could offset their intended benefits. 79 Similarly, a strategy of choice default with an opt in frame might lessen the risk of adverse negative reactions such as reactance.55,57,59
While the findings provide valuable insights into desk-based workers, the relatively small and homogeneous nature of the group limits the generalisability of the results to the broader, more diverse population. Nonetheless, our findings contribute to a growing body of evidence on the effectiveness of default nudges, implying that strategically designed choice architectures can be generalised to influence outcomes in other areas where a specific option is preferred for the majority of individuals.
Conclusions
Notwithstanding the identified limitations of our data, our findings hold relevance amidst a growing pandemic of poor health, driven by widespread suboptimal voluntary health choices. Workplace contexts contribute to this health landscape, especially those with sedentary work environments and prolonged occupational sitting. 18 Consequently, organisations with sedentary workforces are not merely settings for employment but critical sites for population health intervention. 22 But what happens when the cure becomes a source of resistance? As our analysis of USC reveals, a possible answer lies in the use of choice default nudge strategy with an opt out frame.38,40,42
The insights gained through this study regarding choice default nudges have particular relevance for workplace representatives who are held accountable for employee health (i.e., employers and occupational health and safety staff). Like public health and medical authorities, workplace health stakeholders possess influence, not control. 83 As this study demonstrates, well-intentioned interventions can possibly trigger psychological resistance precisely because authority, whether clinical or organisational, is never absolute. 46 Workplace employers should not reject choice default nudges with opt-out framing for behaviour change interventions. The choice default strategy can facilitate the development of long-term preferred health habits. Workplace health intervention designers need to heed the psychological boundaries this study reveals. For workplace health stakeholders, the lesson is clear: effective intervention requires not only good intentions but also deep respect for the autonomy of those they serve. Workplace interventions that use nudge designs to change employee health behaviours but ignore this dynamic risk becoming nothing more than another workplace demand to be resisted, ironically by those who have the most to gain.
Footnotes
Ethical statement
We followed the Standards for Reporting Qualitative Research. Data collection for the primary purpose of this study proceeded in line with ethical approval from the University of Tasmania (Ref# H0018075). Our ethics included permission to use of data from all communications. All participants voluntarily agreed to participate.
Informed consent
All participants signed consent forms in accordance with ethical approval.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Appendix 1: Analytical table for coding for phase 2,3,& 4 analysis.
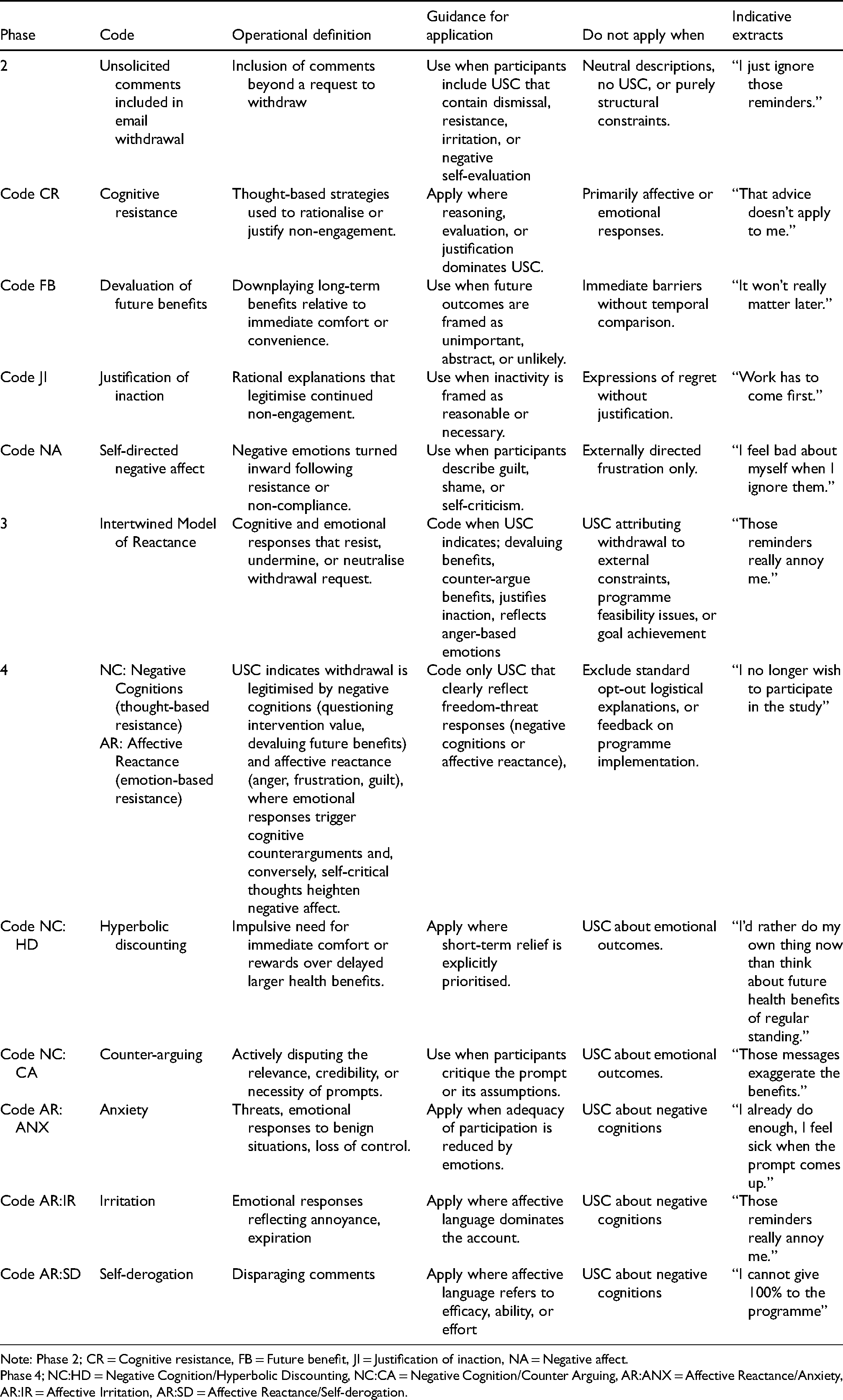
| Phase | Code | Operational definition | Guidance for application | Do not apply when | Indicative extracts |
|---|---|---|---|---|---|
| 2 | Unsolicited comments included in email withdrawal | Inclusion of comments beyond a request to withdraw | Use when participants include USC that contain dismissal, resistance, irritation, or negative self-evaluation | Neutral descriptions, no USC, or purely structural constraints. | “I just ignore those reminders.” |
| Code CR | Cognitive resistance | Thought-based strategies used to rationalise or justify non-engagement. | Apply where reasoning, evaluation, or justification dominates USC. | Primarily affective or emotional responses. | “That advice doesn’t apply to me.” |
| Code FB | Devaluation of future benefits | Downplaying long-term benefits relative to immediate comfort or convenience. | Use when future outcomes are framed as unimportant, abstract, or unlikely. | Immediate barriers without temporal comparison. | “It won’t really matter later.” |
| Code JI | Justification of inaction | Rational explanations that legitimise continued non-engagement. | Use when inactivity is framed as reasonable or necessary. | Expressions of regret without justification. | “Work has to come first.” |
| Code NA | Self-directed negative affect | Negative emotions turned inward following resistance or non-compliance. | Use when participants describe guilt, shame, or self-criticism. | Externally directed frustration only. | “I feel bad about myself when I ignore them.” |
| 3 | Intertwined Model of Reactance | Cognitive and emotional responses that resist, undermine, or neutralise withdrawal request. | Code when USC indicates; devaluing benefits, counter-argue benefits, justifies inaction, reflects anger-based emotions | USC attributing withdrawal to external constraints, programme feasibility issues, or goal achievement | “Those reminders really annoy me.” |
| 4 | NC: Negative Cognitions (thought-based resistance) | USC indicates withdrawal is legitimised by negative cognitions (questioning intervention value, devaluing future benefits) and affective reactance (anger, frustration, guilt), where emotional responses trigger cognitive counterarguments and, conversely, self-critical thoughts heighten negative affect. | Code only USC that clearly reflect freedom-threat responses (negative cognitions or affective reactance), | Exclude standard opt-out logistical explanations, or feedback on programme implementation. | “I no longer wish to participate in the study” |
| AR: Affective Reactance (emotion-based resistance) | |||||
| Code NC:HD | Hyperbolic discounting | Impulsive need for immediate comfort or rewards over delayed larger health benefits. | Apply where short-term relief is explicitly prioritised. | USC about emotional outcomes. | “I’d rather do my own thing now than think about future health benefits of regular standing.” |
| Code NC:CA | Counter-arguing | Actively disputing the relevance, credibility, or necessity of prompts. | Use when participants critique the prompt or its assumptions. | USC about emotional outcomes. | “Those messages exaggerate the benefits.” |
| Code AR:ANX | Anxiety | Threats, emotional responses to benign situations, loss of control. | Apply when adequacy of participation is reduced by emotions. | USC about negative cognitions | “I already do enough, I feel sick when the prompt comes up.” |
| Code AR:IR | Irritation | Emotional responses reflecting annoyance, expiration | Apply where affective language dominates the account. | USC about negative cognitions | “Those reminders really annoy me.” |
| Code AR:SD | Self-derogation | Disparaging comments | Apply where affective language refers to efficacy, ability, or effort | USC about negative cognitions | “I cannot give 100% to the programme” |
Note: Phase 2; CR = Cognitive resistance, FB = Future benefit, JI = Justification of inaction, NA = Negative affect.
Phase 4; NC:HD = Negative Cognition/Hyperbolic Discounting, NC:CA = Negative Cognition/Counter Arguing, AR:ANX = Affective Reactance/Anxiety, AR:IR = Affective Irritation, AR:SD = Affective Reactance/Self-derogation.