
Abstract
Background
Health is a fundamental human right that must be protected without discrimination, and ensuring equal access to healthcare, especially for migrants, is a core principle of modern health systems.
Objective
This study aims to examine health professionals’ intercultural competence and investigate how this competence influences their attitudes toward immigrants.
Methods
Data were collected using two validated instruments: the Intercultural Competence Instrument for Health Professionals (20 items, for subscales) and the Determining Attitudes of Health Professionals Toward Immigrants Scale (14 items, three subscales). The study sample consisted of 353 health professional working in two public hospitals in Kocaeli, Türkiye. Data were analyzed using descriptive statistics (frequency and percentage), the relationships between participants’ demographic and professional characteristics and their intercultural competence and attitudes towards immigrants were examined using Pearson correlation analysis, and the effect of intercultural competence on attitudes towards immigrants was evaluated using multiple linear regression analysis.
Results
The findings revealed significant differences in intercultural competence scores according to professional role, educational level, and experience working with immigrant populations. Attitudes toward immigrants also differed significantly depending on whether participants had experience providing care to immigrant patients. Correlation analysis showed a strong and statistically significant negative relationship between intercultural competence and negative attitudes toward immigrants.
Conclusion
The findings highlight the importance of improving intercultural competence among health professionals to promote more positive attitudes toward immigrant patients and to enhance the quality of culturally responsive healthcare services.
Introduction
Health is universally recognized as a fundamental human right that must be ensured without discrimination based on race, ethnicity, religion, political affiliation, or socioeconomic status. A core principle of contemporary healthcare systems is the equitable provision of services. This principle ensures that all individuals have access to healthcare regardless of time, location, or personal background. 1 According to the International Organization for Migration (2019), a migrant is defined as an individual who relocates from their habitual place of residence—either temporarily or permanently—for various reasons, within national borders or across international boundaries. The World Migration Report (2024) estimates that the global migrant population has reached approximately 281 million individuals.2,3 Since 2015, Türkiye has become one of the leading host countries for large migrant populations. The majority of these individuals originate from Syria, with substantial numbers from Afghanistan, Iraq, and Iran. 4 To facilitate migrants’ access to essential healthcare services, 185 Migrant Health Centers have been established across 29 provinces in Türkiye. 5
These transformations create new challenges for healthcare systems and require health professionals to develop competencies that enable them to provide culturally sensitive care to diverse populations. Migration influences society on multiple levels—physically, socially, and culturally— significantly altering community environments and dynamics. These demographic and cultural shifts impact both the delivery of healthcare services and migrants’ access to care. 6 In multicultural settings, healthcare providers frequently navigate complex interactions by shared and divergent cultural values and practices. The concept of cultural competence was initially articulated by Madeleine Leininger through her theory of ‘Culture Care Diversity and Universality’ which defines cultural competence as the ability of health professionals to understand and integrate cultural dimensions into care practices. 7 Cultural competence includes the knowledge, awareness, and skills necessary to provide care that is respectful of and responsive to the cultural values, beliefs, and practices of diverse populations. 8 In today's globalized world, cultural awareness is an essential competency that facilitates effective engagement within multicultural environments and encourages creativity and innovation in care delivery.9,10 Cultural diversity underlines the need for health professionals to deliver services with cultural sensitivity, particularly when caring for individuals with differing beliefs, values, communication styles, and behavioral norms. In this regard, culture and care are intrinsically linked and play a vital role in individuals’ overall well-being and survival. 11 Several theoretical perspectives explain the relationship between health and culture. The absolutist perspective asserts that health and illness concepts are biologically determined and independent of cultural influence. However, the relativist perspective emphasizes that cultural context fundamentally shapes individuals’ understanding of health and illness, with each culture holding distinct beliefs and practices. The universalist perspective acknowledges that while certain health-related experiences are shared across cultures, their interpretation and management are culturally mediated. 12
Previous research highlights the challenges faced by health professionals in delivering culturally competent care. For instance, Ceylan and Çetinkaya (2022) reported that nursing students often lack formal education in cultural competence, leading to communication difficulties in clinical settings, particularly due to language barriers with patients. 13 Koçan et al. (2017) concluded that immigrant patients’ participation in healthcare poses significant biopsychosocial and cultural challenges for both health professionals and immigrant populations within host countries. 14 Similarly, Çal et al. (2022) identified that nurses experience difficulties in recognizing and effectively communicating the cultural practices of immigrant patients. 15
In increasingly multicultural societies, cultural competence has become an essential component of effective healthcare delivery. Cultural competence enables health professionals to understand patients’ cultural backgrounds, beliefs, and communication styles, thereby facilitating patient-centered care and improving health outcomes. Previous studies have shown that insufficent cultural competence among healthcare access among migrant populations. 16 Morever, healthcare systems that promote intercultural competence among professionals are more successful in adressing the complex needs of culturally diverse populations. Migrant populations frequently encounter multiple barriers when accsessing healthcare services. Language differences, unfamiliarity with healthcare systems, and cultural misunderstandings often limit migrants’ ability to receive adequate care. Studies conducted in different healthcare settings indicate that health professionals’ cultural awareness and communication skills play a critical role in reducing these barriers and improving the quality of care provided to migrant patients. 17
Health professionals’ attitudes toward immigrants can significantly influence healthcare experiences and outcomes. Negative attitudes may leed to reduced quality of care, communication difficulties, and decreased trust between patients and providers. Conversely, research suggests that higher levels of intercultural competence among healthcare professionals are associated with more positive attitudes toward migrant populations and improved patient-provider relationships.18–20 Educational interventions focusing on intercultural competence have been increasingly implemented in healthcare education programs. Evidence suggests that structured training programs that integrate cultural knowledge, communication skills, and reflective practice can enhance health professionals’ cultural sensitivity and improve their attitudes toward culturally diverse patients. 21
This study is expected to contribute to the literature by providing empirical evidence on the relationship between intercultural competence and attitudes toward immigrants among health professionals. Despite the growing number of studies examining cultural competence in healthcare, limited research has focused on how health professionals’ intercultural competence influences their attitudes toward immigrant populations, particularly within countries hosting large numbers of migrant such as Türkiye. Understanding this relationship is essential for improving healthcare delivery in increasingly multicultural healthcare environment. Therefore, the primary aim of this study is to examine the extent to which health professionals’ intercultural competence influences their attitudes toward immigrants. In addition, the study seeks to explore how these attitudes may impact the quality and effectiveness of healthcare delivery to immigrant populations. Given the increasing cultural diversity within healthcare settings, the findings of this study are expected to highlight the critical role of intercultural competence in clinical practice. Specifically, the results may inform the integration of intercultural competence into continuing professional development programs and contribute to the advancement of more inclusive, equitable, and patient -centered healthcare practices.
Method
Study design
A quantitative, cross-sectional research design was used to examine the relationship between health professionals’ intercultural competencies and their attitudes towards immigrants. This design was found suitable for evaluating the relationships between variables at a single point in time within a specific population. The research was guided by the following hypothesis:
H1: Higher levels of intercultural competence among health professionals are associated with more positive attitudes toward immigrants (Figure 1).

Research model.
Research setting
Two hospitals in Kocaeli were selected as research sites based on key contextual factors: a high concentration of migrant populations, varied levels of access to healthcare services, the presence of multidisciplinary healthcare teams, and the influence of local health service policies. According to local demographic data, the district of Gebze hosts approximately 14,000 migrant residents, while Darıca is home to an estimated 11,464 migrant individuals. These hospitals were selected because they serve districts with relatively high migrant populations and provide healthcare services through multidisciplinary professional teams, making them suitable settings for examining intercultural competence in healthcare delivery.
Participants
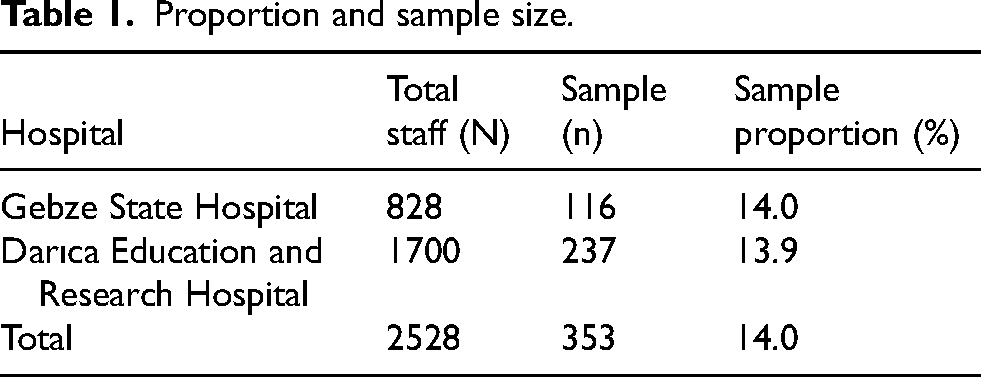
The study population consists of a total of 2528 healthcare professionals working in two public health institutions in Kocaeli, Türkiye: a state hospital in Gebze (N = 828) and a education and research hospital in Darıca (N = 1700).
Inclusion Criteria: Being a healthcare professional actively working in the two selected hospitals Agreeing to participate in the study voluntarily
Exclusion Criteria: Healthcare professionals who were on leave during data collection Healthcare professionals who could not be reached during the data collection period
The sample was determined using convenience sampling due to time constraints and ease of access to participants, and data collection was applied proportionally to ensure representation among professional groups. The sample size was determined using the tables proposed by Yazıcıoğlu ve Erdoğan (2004). For a population of 2,500, a minimum sample size of 334 participants was required. The final sample consisted of 353 participants (Table 1).
Proportion and sample size.
Data collection
Data collection was carried out by the research team between August and October 2024 using a structured face-to-face survey method. The questionnaires were administered by members of the research team who were trained regarding the purpose of the study and standardized data collection procedures. Prior to data collection, members of the research team were trained by the principal investigator to ensure consistency in the administration of the questionnaires. This training aimed to ensure consistency and reliability in data collection process. Participation in the study was voluntary, and each questionnaire took approximately 8–12 min to complete. A total of 420 questionnaires were distributed, and 353 valid responses were obtained (response rate: 84.0%).
Data collection instruments
Data were collected using a face-to-face survey method, employing a convenience sampling approach. Two psychometrically validated instruments were used to assess health professionals’ intercultural competence and their attitudes toward immigrant populations. Detailed descriptions of each instrument are provided below.
Intercultural competence instrument for health professionals
The Intercultural Competence Instrument for Health Professionals, originally developed by Bernhard et al., was adapted and psychometrically evaluated for Turkish health professionals by Çınar et al. (2020). 22 The scale comprises 20 items across four subscales: intercultural skills, intercultural attitudes, intercultural emotions/empathy, and intercultural motivation/curiosity. Responses are rated on a five-point Likert scale, ranging from 1 = Strongly disagree to 5 = Strongly agree. Items in the intercultural attitudes and intercultural emotions/empathy subscales are reverse-coded. Item-total correlation coefficients for the Turkish version ranged from 0.62 to 0.90, indicating acceptable internal consistency. The Cronbach's alpha coefficients for the subscales were 0.90, 0.66, 0.69, and 0.62, respectively. The overall scale demonstrated good reliability, with a Cronbach's alpha of 0.85.
Determining attitudes of health professionals toward immigrants scale
The Determining Attitudes of Health Professionals Toward Immigrant Scale was developed by Karagöz & Karaşin (2024) to evaluate health professionals’ attitudes toward immigrant populations. 23 The instrument includes 14 items across three subscales: negative attitude, obstructive attitude, and positive attitude. All items are scored on a five-point Likert scale (1 = Strongly disagree to 5 = Strongly agree), and none are reverse-coded. Item-total correlations ranged from 0.70 to 0.87. The Cronbach's alpha coefficients for the subscales were 0.85, 0.75, and 0.70, respectively. The overall scale demonstrated high reliability, with a Cronbach's alpha of 0.87.
Data analysis
All collected data were entered and analyzed using IBM SPSS Statistics for Windows, version 27.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics (frequency and percentage) were used to summarize the demographic and occupational characteristics of the participants. Independent samples t-tests were used to compare variables between two groups, and one-way analysis of variance (ANOVA) was used for comparisons among more than two groups. The relationships between the participants’ sociodemographic and occupational characteristics, intercultural competence, and attitudes towards immigrants were examined using Pearson correlation analysis. The effect of intercultural competence on attitudes towards immigrants was evaluated using multiple linear regression analysis.
The normality of the data distribution was assessed using skewness and kurtosis values. Values between −1 and +1 were considered indicative of a normal distribution. 24 The skewness and kurtosis values were −0.033 and 0.090 for the Intercultural Competence Scale, and −0.325 and 0.271 for the Attitudes Towards Immigrants Scale, respectively, indicating that the data met the assumption of normality. 25
Ethical considerations
Ethical approval for the study was obtained from the Ethics Committee of Selçuk University. Faculty of Health Sciences (Non-Interventional Clinical Research Approval No. 2024/658). In addition, written permissions were obtained from the Kocaeli Provincial Health Directorate and the administrative bodies of the participating hospitals.
Results
The socio-demographic characteristics of the 353 health professionals who participated in the study are presented below.
According to Table 2, 26.3% of the participants (n = 93) were between the ages of 32 and 35. The majority were female (73.9%, n = 261), and 68.0% (n = 240) were married. More than half of the participants held a bachelor's degree (56.1%, n = 198), and 52.7% (n = 186) reported earning an income equivalent to approximately three times the national minimum wage. In addition, 55.2% (n = 195) reported having no proficiency in a foreign language. In terms of professional roles, 43.6% (n = 154) were nurses or midwives. The majority (60.1%, n = 212) indicated that they had no prior experience working with immigrant populations, while 62.3% (n = 220) reported having a moderate level of knowledge regarding cultural diversity.
Demographic characteristics of participants (N = 353).
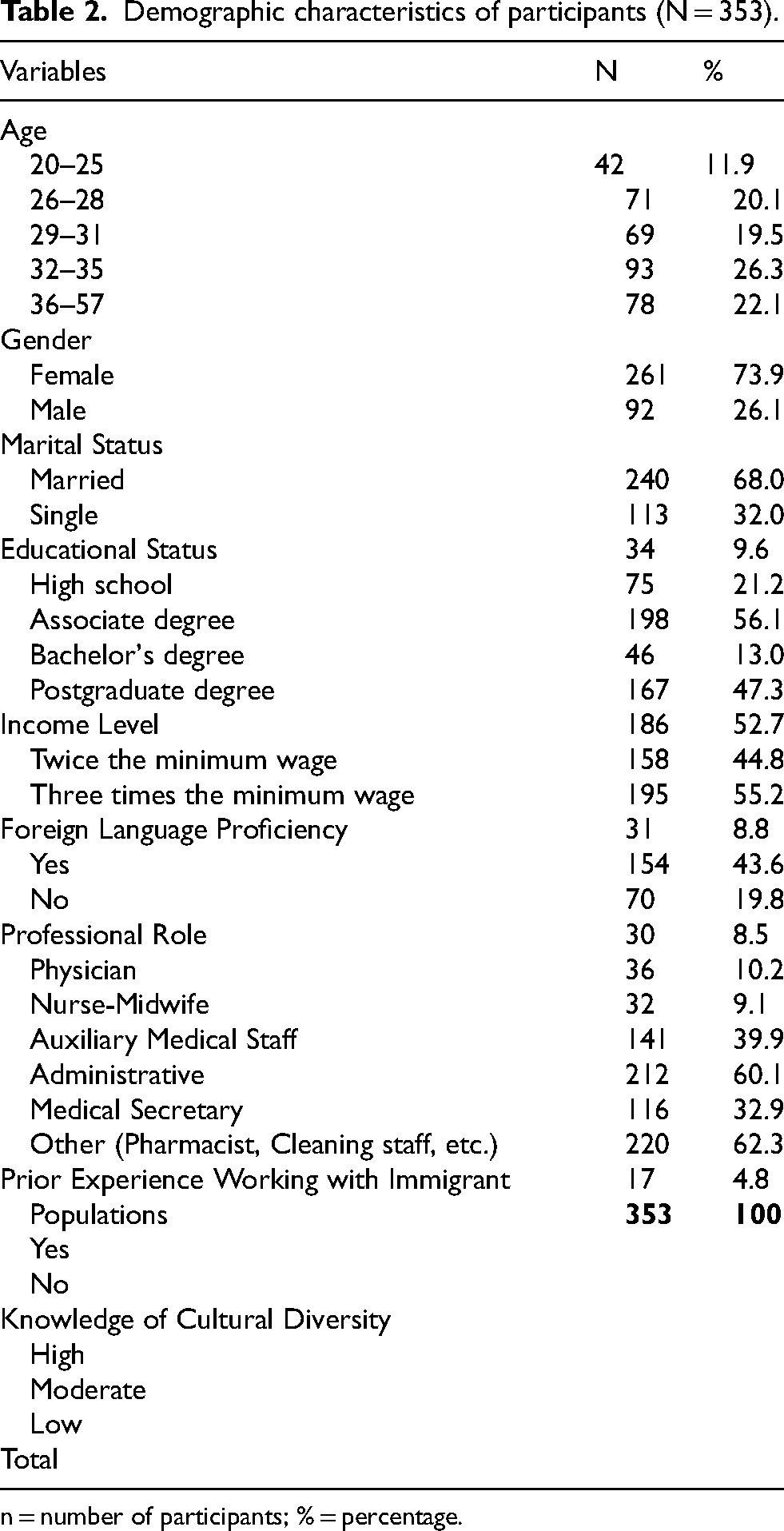
n = number of participants; % = percentage.
An examination of Table 3 indicates that health professionals with a high school education reported higher intercultural competence scores compared to those holding associate or bachelor's degrees. In addition, the intercultural competence scores of auxiliary health personnel were found to be lower than those of other professional groups. However, no statistically significant differences were observed between intercultural competence scores and participants’ age, gender, marital status, income level, or foreign language proficiency (p > 0.05). A statistically significant difference was found between prior experience working with immigrant populations and both intercultural competence and attitudes toward immigrants (p < 0.05). Health professionals with such experience demonstrated significantly higher levels of intercultural competence and more positive attitudes compared to those without prior exposure. However, attitude scores toward immigrants did not significantly differ according to age, gender, marital status, income level, professional role, or foreign language proficiency (p > 0.05).
Comparison of scale scores by participants’ sociodemographic and professional characteristics (N = 353).
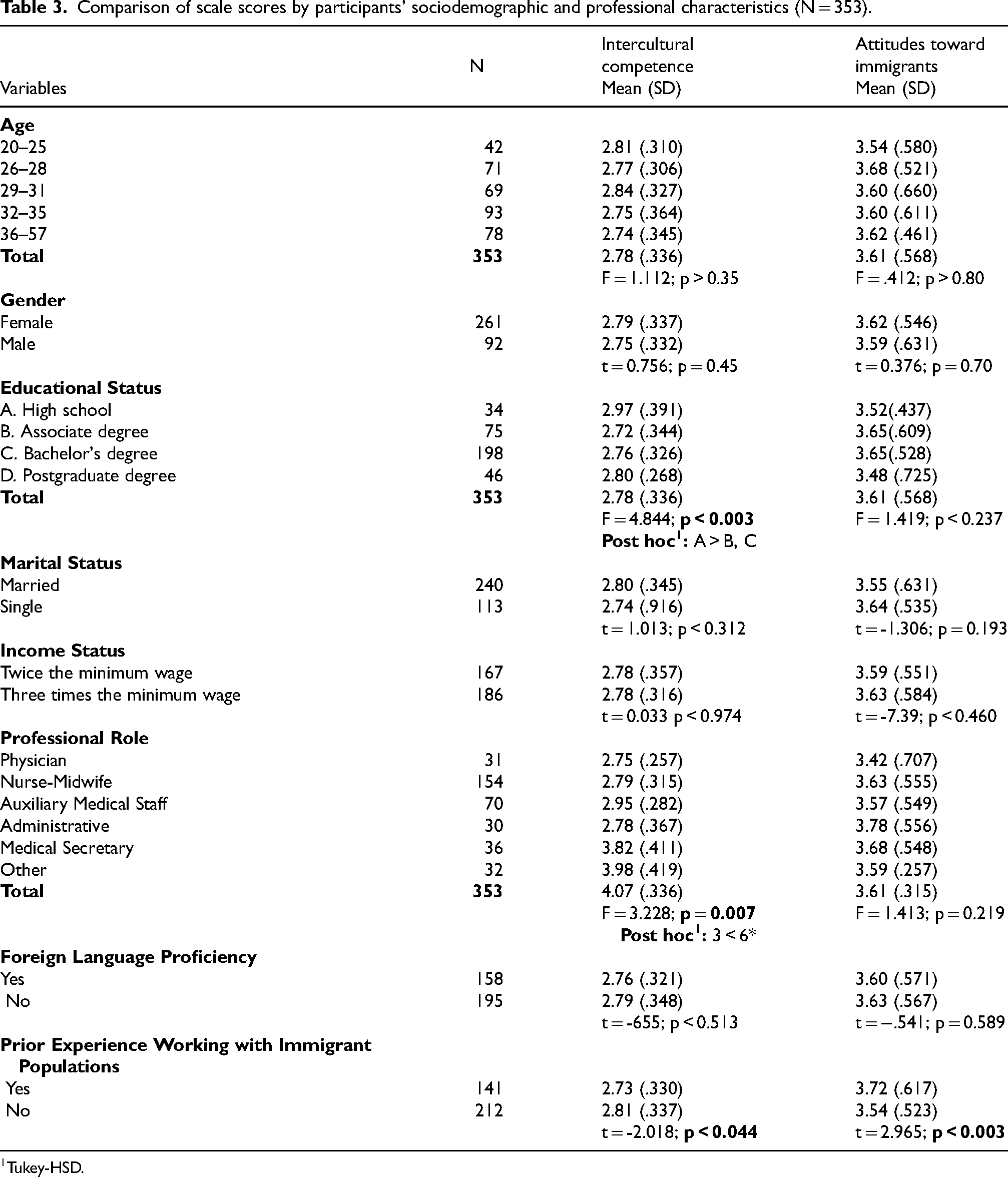
Tukey-HSD.
Correlations between participants’ sociodemographic and professional characteristics, intercultural competence, and attitudes toward immigrants (N = 353).
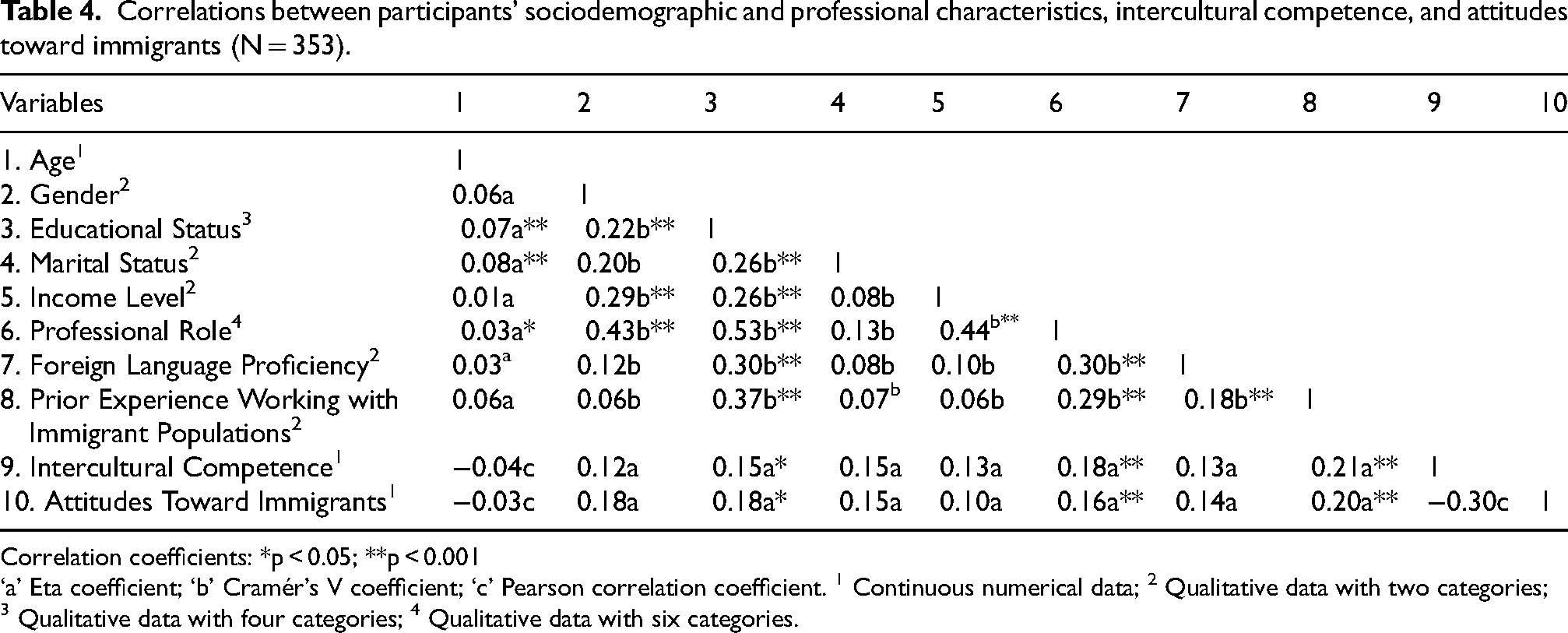
Correlation coefficients: *p < 0.05; **p < 0.001
‘a’ Eta coefficient; ‘b’ Cramér's V coefficient; ‘c’ Pearson correlation coefficient. 1 Continuous numerical data; 2 Qualitative data with two categories; 3 Qualitative data with four categories; 4 Qualitative data with six categories.
A moderate, negative, and statistically significant correlation was found between scores on the Attitudes Toward Immigrants Scale and the Intercultural Competence Instrument (r = –0.30, p < 0.001). A statistically significant but weak positive correlation was observed between attitude scores and both professional role and prior experience working with immigrant populations (p < 0.001). No statistically significant correlations were found between attitudes toward immigrants and age, gender, educational status, marital status, income level, or foreign language proficiency (p > 0.05) (Table 4).
The results of the hierarchical multiple regression analysis, conducted to assess the predictive value of intercultural competence and selected sociodemographic and professional variables on attitudes toward immigrants, are presented in Table 5.
Results of hierarchical multiple linear regression analysis (N:353).
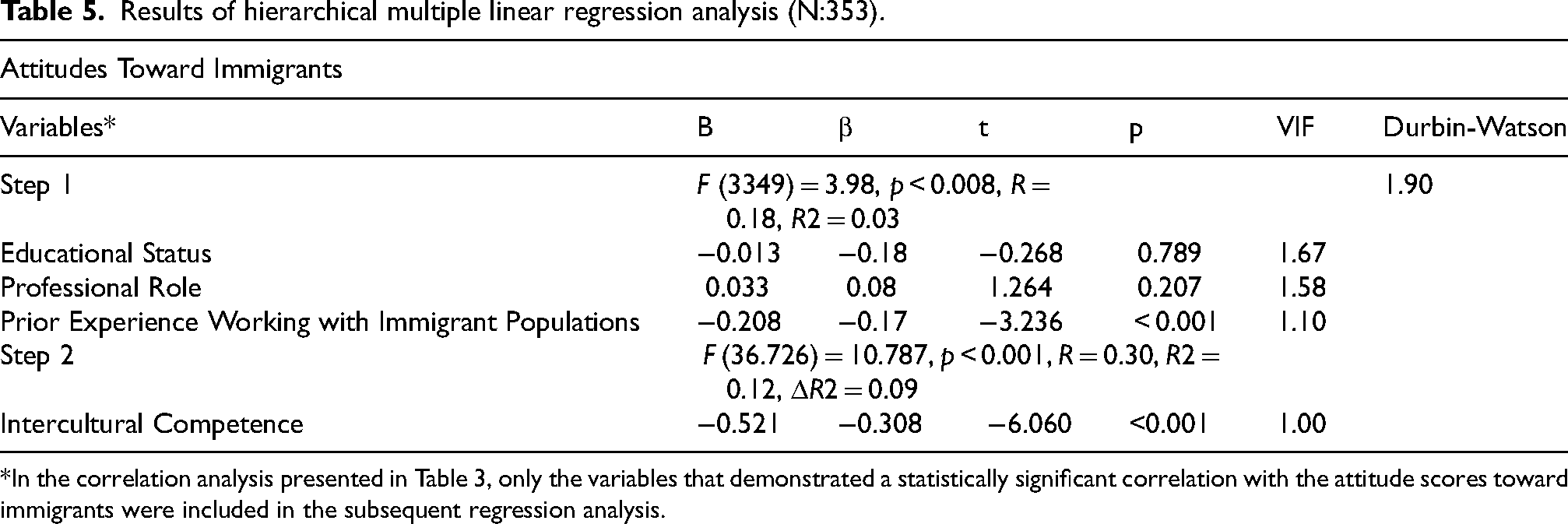
*In the correlation analysis presented in Table 3, only the variables that demonstrated a statistically significant correlation with the attitude scores toward immigrants were included in the subsequent regression analysis.
The Durbin-Watson statistic and Variance Inflation Factor (VIF) values were examined to assess autocorrelation and multicollinearity, respectively. A Durbin-Watson value between 1.5 and 2.5 is considered acceptable, indicating the absence of autocorrelation, while VIF values below 10 suggest no multicollinearity. 26 In this study, the Durbin-Watson value was 1.90, and VIF values ranged from 1.00 to 1.67, indicating that the assumptions of regression analysis were met. In the hierarchical regression analysis, educational status, professional role, and prior experience working with immigrant populations were entered as control variables in Step 1. In Step 2, intercultural competence was added as the primary predictor variable. The analysis demonstrated that intercultural competence was a statistically significant predictor of attitudes toward immigrants (p < 0.001). Furthermore, the inclusion of intercultural competence in the model significantly increased the proportion of explained variance in attitudes toward immigrants. Professional and personal variables accounted for 3% of the variance in attitudes (R2 = 0.03; p < 0.001), while the addition of intercultural competence increased the explained variance to 12% (R2 = 0.12, ΔR2 = 0.09; p < 0.001). Among the control variables, only prior experience working with immigrant populations was identified as a statistically significant predictor of attitudes toward immigrants (p < 0.001). However, educational status and professional role did not have a significant effect (p > 0.05).
Discussion, conclusions and recommendations
In recent years, social, economic, and political developments have led to increased immigration in Türkiye, thereby elevating the relevance of intercultural competence among health professionals. As healthcare systems adapt to serve increasingly diverse populations, the ability to delivery culturally responsive care has become more essential.
This study examined the relationship between health professionals’ intercultural competence and their attitudes toward immigrants. The findings revealed a statistically significant, moderate negative correlation between intercultural competence and attitudes toward immigrants. Specifically, higher levels of intercultural competence were associated with lower levels of negative and obstructive attitudes. These results suggest that enhancing intercultural competence among health professionals may be a key strategy for improving equitable care delivery to immigrant populations. Consistent with previous literature the regression analysis further confirmed intercultural competence as a significant predictor of attitudes toward immigrants. For instance, Çetişli et al. (2016) reported that increased empathy was associated with increased intercultural sensitivity. 27 Similarly, Karakuş et al. (2013) noted that nurses recognized cultural differences as integral to the care process. 28 While Kıvrak et al. (2023) found no direct relationship between intercultural competence and caring attitudes among pediatric nurses they identified various contextual factors influencing both constructs. 29 Zengin et al. (2021) documented challenges in personal care delivery among immigrant patients, emphasizing the need for culturally sensitive approaches. 30 Moreover, Gönderen Çakmak et al. (2020) observed that 70% of nurses did not report any altered emotional response when caring for immigrant patients. 31
Regarding demographic variables, no statistically significant differences were observed in intercultural competence or attitudes toward immigrants based on gender, marital status, income level, foreign language proficiency, or age (p > 0.05). However, significant differences were found in intercultural competence based on educational status, professional role, and prior experience working with immigrant populations (p < 0.05). Similarly, experience working with immigrants was associated with more positive attitudes (p < 0.05). Comparable findings are evident in the literature. Kılıç and Sevinç (2018) reported that female nursing students exhibited higher levels of intercultural sensitivity. 32 Alpern and Davey (2016) highlighted common barriers in immigrant care—language differences, cultural misunderstandings, time constraints, limited region-specific medical information, and challenges in explaining treatment plans. 33 Patel et al. (2021) also identified linguistic and cultural barriers as the primary challenges faced by nurses. 34 In a study by Akkoç and Tok (2017), 24% of health professionals reported providing care to 3–5 refugee and asylum-seeking individuals annually, while 16% to 5–10 individuals, and 17% to more than 10. These professionals frequently encountered challenges related to patient compliance, including issues with documentation, the presence of non-authorized companions, elevated noise levels in care areas, and adherence to institutional rules. 35
To address the increasing cultural diversity in healthcare settings, the following recommendations are proposed: Develop structured training programs to improve the intercultural competence of health professionals. These programs should integrate both theoretical and practical components, emphasizing communication, empathy, cultural humility, and reflective practice. Structured training programs include both theoretical and practical components to enhance the cultural competencies of healthcare professionals. The theoretical component encompasses lectures and seminars on cultural awareness, migrant health, and ethical principles, while the practical component enables participants to develop effective communication and empathy skills with patients from diverse cultural backgrounds through role-playing, simulations, and case studies. Learning outcomes are assessed and reinforced throughout the training process using surveys, tests, and feedback.
Incorporate stress management and resilience-building techniques into professional development activities, helping health professionals navigate the complexities of culturally diverse care environments.
Implement awareness-raising initiatives for immigrant communities to promote mutual understanding and respect for the cultural norms and expectations of the host society.
Support ongoing research into patient-centered outcomes, such as satisfaction with care and health literacy levels among individuals receiving services from migrant health centers.
Study limitations
This study is subject to several contextual and methodological limitations. The findings are limited to the specific time frame during which data were collected, as well as to the geographical and institutional settings in which the research was conducted—namely, two public hospitals in Kocaeli, Türkiye. Health professionals who were on leave or unavailable during the data collection period could not be included in the sample.
Footnotes
Acknowledgments
Not Applicable.
Ethical approval
Ethical approval for the study was obtained from the Ethics Committee of Selçuk University Faculty of Health Sciences (Non-Interventional Clinical Research Approval No. 2024/658). In addition, written permissions were obtained from the Kocaeli Provincial Health Directorate and the administrative bodies of the participating hospitals.
Informed consent
All participants provided written informed consent before joining the study. Participation was voluntary, and participants were informed that they could withdraw from the study at any time.
Authors’ contributions to the article
The authors contributed equally to the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of suppoting data
Research data and analysis results are stored. It can be shared as needed.
Statement of support and acknowledgment
No support was received from any institution or organization in the study.