
Abstract
Background
Breast cancer survivors often face substantial challenges in social reintegration, the process of resuming roles, relationships, and community participation after treatment. However, existing research has largely focused on Western contexts, with limited attention to how cultural factors shape these experiences in non-Western settings, particularly in China.
Objective
To explore breast cancer survivors’ experiences of social reintegration and provide insights for developing culturally sensitive interventions.
Methods
A qualitative study was conducted between June and November 2024. Using purposive sampling, we recruited 16 breast cancer survivors. Data from in-depth, semi-structured interviews were analyzed using Braun and Clarke's reflexive thematic analysis approach.
Results
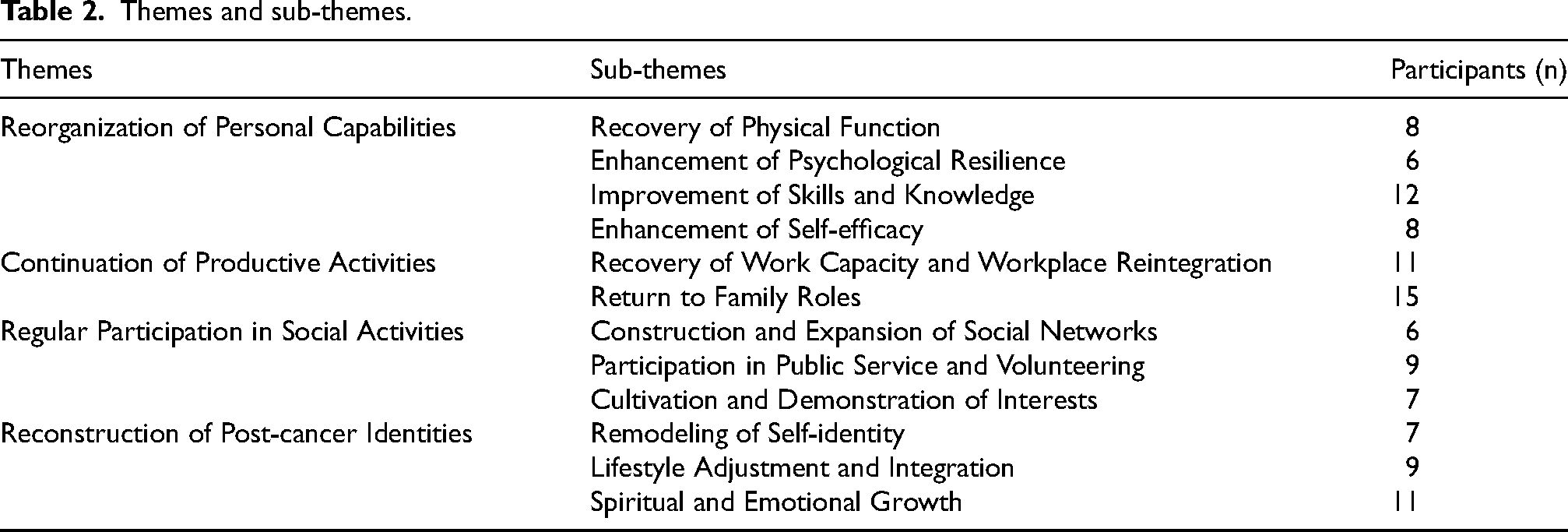
Four major themes were identified: (a) reorganization of personal capabilities, including recovery of physical function, enhancement of psychological resilience, improvement of skills and knowledge, and enhancement of self-efficacy; (b) continuation of productive activities, including recovery of work capacity and workplace reintegration, and return to family roles; (c) regular participation in social activities, including construction and expansion of social networks, participation in public service and volunteering, and cultivation and demonstration of interests; and (d) reconstruction of post-cancer identities, including remodeling of self-identity, lifestyle adjustment and integration, and spiritual and emotional growth.
Conclusions
The findings highlight the need to comprehensively consider survivors’ personal experiences and social support when developing more effective social reintegration intervention programs. Future research should further explore the effectiveness of various intervention strategies to facilitate better integration and adaptation among breast cancer survivors.
Public significance statement
This qualitative study provides an in-depth understanding of how breast cancer survivors experience social reintegration after treatment. By illuminating the key challenges they face and the critical facilitators, including family support, community resources, and healthcare systems, that enable successful return to daily life, the findings underscore the need for a holistic approach to cancer care. The insights gained can inform targeted psychosocial interventions, healthcare policies, and community programs aimed at improving survivors’ long-term quality of life and well-being.
Introduction
Breast cancer is the most common malignancy among women worldwide. According to the International Agency for Research on Cancer (IARC), there were approximately 2.3 million new cases and 666,000 deaths globally in 2022.1,2 Although advances in early detection and treatment have significantly improved survival rates,3–5 breast cancer continues to impose substantial physical and psychological burdens on survivors. 6
During diagnosis and treatment, survivors often experience treatment-related side effects, body image disturbances, and fear of recurrence, leading to psychological distress and social isolation.7–9 After completing active treatment, many survivors face the complex process of social reintegration. This involves reestablishing their roles and identities within family, workplace, and community contexts. This transition is critical to their overall quality of life but is often fraught with challenges. 10
Successful social reintegration has been associated with improved physical health and positive emotional outcomes.11,12 Although these studies provide valuable evidence of the benefits of social integration in general populations, their findings are also relevant to cancer survivors. For these survivors, physical recovery and emotional well-being are critical components of post-treatment adjustment. However, for breast cancer survivors, this process can be complicated by persistent physical limitations, emotional vulnerability, and societal attitudes toward cancer.13,14 Supportive social networks have been shown to facilitate reintegration, 15 yet many survivors report feelings of stigma and isolation that hinder their reconnection with social environments.16–19 This paradox may be explained by the distinction between the quantity and quality of social interactions. While supportive networks provide essential resources, stigmatizing attitudes from others, whether overt or subtle, can undermine survivors’ confidence and willingness to engage socially.
Despite the growing recognition of social reintegration as a key aspect of cancer survivorship, a critical examination of the literature reveals significant gaps that warrant attention. A systematic review of existing research indicates that the majority of studies have been conducted in Western countries, particularly in the United States and Europe, with limited representation from Asian or other non-Western contexts.20,21 These studies have primarily employed quantitative designs, measuring reintegration outcomes through standardized scales that may not capture the culturally specific meanings and experiences of social reintegration. 22 Furthermore, existing qualitative research has largely focused on physical recovery and psychological adjustment, with comparatively less attention to the social and occupational dimensions of reintegration. 23 Notably, no studies to date have systematically examined how Chinese breast cancer survivors navigate this process. This leaves a critical gap in understanding the culturally specific resources, barriers, and coping strategies that influence reintegration in this population.
In China, family dynamics, social expectations, and healthcare systems differ markedly from those in Western countries. Specifically, family dynamics in Chinese culture are characterized by strong intergenerational ties and the principle of filial piety. In this context, family members often assume primary caregiving responsibilities and are deeply involved in medical decision-making. 24 Social expectations emphasize maintaining interpersonal harmony and avoiding “loss of face.” This may lead survivors to conceal their diagnosis or minimize their struggles to avoid becoming a burden on others. 25 Healthcare systems in China are structured differently as well. Patients navigate a tiered hospital system, limited integration of primary care, and doctor-patient communication that tends to be more hierarchical than collaborative. 26 These cultural and structural factors may shape the reintegration experiences of breast cancer survivors in ways that are not captured by research conducted in Western settings. Addressing these gaps is essential for developing culturally sensitive interventions that can effectively support survivors in non-Western settings. As such, the reintegration experiences of breast cancer survivors in China may present unique challenges and coping strategies. Challenges may include managing family expectations while balancing caregiving responsibilities with personal recovery. They also include navigating employer attitudes and concerns about career progression during workplace reintegration, and facing stigma while attempting to rebuild social networks. Coping strategies may involve leveraging family support, engaging with online peer communities such as WeChat groups, and finding meaning through volunteer activities.
While quantitative approaches such as surveys and standardized scales can measure the prevalence and correlates of social reintegration outcomes, they are less suited to capturing the nuanced, context-dependent meanings that survivors attach to their experiences. Qualitative methods are particularly appropriate when the goal is to understand how individuals make sense of complex life events within their specific cultural and social contexts. 27 Given that little is known about how Chinese breast cancer survivors navigate social reintegration, an exploratory qualitative design allows for the emergence of themes and patterns. These may not be anticipated by existing theories or measures developed in Western settings. This approach enables the study to capture the richness and complexity of survivors’ lived experiences, including the culturally specific challenges they face and the resources they draw upon.
This study aims to address these gaps by providing an in-depth, contextually grounded exploration of social reintegration among breast cancer survivors in China. While previous research has documented the challenges of reintegration in Western contexts, limited attention has been paid to how cultural values, social structures, and healthcare systems shape these experiences in non-Western settings. This study illuminates survivors’ lived experiences, including the challenges they encounter, the resources they draw upon, and the strategies they develop. In doing so, it seeks to inform culturally sensitive interventions that support successful reintegration. Specifically, it aims to: (a) identify the challenges survivors encounter within the Chinese sociocultural context; (b) understand the resources and strategies they utilize to reintegrate; and (c) provide evidence-based insights for developing culturally sensitive interventions. The findings are expected to inform healthcare providers, social workers, and policymakers in designing support systems that foster resilience and community connection, while contributing to the global discourse on post-cancer reintegration across diverse cultural settings.
Method
Design
A descriptive qualitative design was employed to explore the lived experiences of social reintegration among breast cancer survivors in China. This design is particularly appropriate when the goal is to provide a comprehensive summary of participants’ experiences in everyday language, staying close to the data without imposing predetermined theoretical frameworks. 28 Given that little is known about how Chinese breast cancer survivors navigate social reintegration, a descriptive qualitative approach allows for the emergence of themes and patterns directly from participants’ accounts, making it well-suited for exploratory research in understudied populations. 29 The study was conducted and reported in accordance with the Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist, a 32-item guideline for ensuring transparent and complete reporting of qualitative studies. 30 Data were analyzed using reflexive thematic analysis as outlined by Braun and Clarke. 31 This approach was selected for several reasons. First, reflexive thematic analysis is particularly well-suited for exploratory research where little is known about the phenomenon of interest. Second, unlike coding reliability approaches that seek to minimize researcher influence, reflexive thematic analysis recognizes the researcher as an active participant in knowledge production, treating subjectivity as a resource rather than a threat to validity. This framework conceptualizes themes as actively generated by the researcher through a process of reflexive engagement with the data, rather than passively “emerging” from the data. It provides a structured yet flexible six-phase approach: (1) familiarization with the data, (2) generating initial codes, (3) generating initial themes, (4) reviewing themes, (5) defining and naming themes, and (6) writing the report. This alignment with the study's aim to understand survivors’ lived experiences from an interpretive perspective made this approach preferable to other qualitative methods such as content analysis or grounded theory. These methods may impose predetermined frameworks or aim for theoretical development beyond the scope of this study.
Participants
Participants were recruited between June and November 2024 using purposive sampling with a maximum variation strategy; however, practical constraints led to a demographically homogeneous sample. Recruitment took place in outpatient clinics across Nantong in Eastern China, including one tertiary hospital and two secondary hospitals.
The inclusion criteria were: (1) aged 18 years or older; (2) confirmed diagnosis of breast cancer and aware of their diagnosis; (3) ability to communicate effectively in Chinese; (4) completion of active hospitalization, with disease under control and in the recovery phase; (5) Reintegration to Normal Living Index (RNLI) score ≥ 60, indicating moderate to high levels of reintegration 32 ; and (6) voluntary agreement to participate. Patients with severe cardiac, cerebral, or renal comorbidities, multiple organ failure, or metastatic disease were excluded to minimize confounding effects of other serious illnesses on the social reintegration process. This ensured that the experiences captured were primarily attributable to breast cancer survivorship rather than coexisting medical conditions.
Interview guide
The semi-structured interview guide was developed through a multi-step process. First, we conducted a review of relevant literature on cancer survivorship and social reintegration to inform the initial draft.33,34 Next, the research team discussed and refined the draft through iterative feedback. We then pilot-tested the guide with two breast cancer survivors to assess the clarity, relevance, and comprehensiveness of the questions. Based on feedback from these pilot interviews, we consulted a panel of experts, including clinical nurses, psychologists, sociologists, and oncologists specializing in breast cancer. The final interview guide was revised to incorporate insights from both the pilot interviews and expert consultations. The core questions included in the interview were as follows: (a) Can you tell me about your cancer experience? (b) What changes have occurred in your life since your illness? (c) Do you feel that you have returned to your normal life now? (d) What efforts have you made to restore your normal life? What obstacles have you encountered? What support have you received? (e) What suggestions would you share with other patients to help them return to their normal life?
Data collection
Eligible participants were invited to take part in face-to-face, semi-structured interviews conducted in Chinese. Interviews were carried out by two graduate nursing students and a psychological counselor, all of whom had received training in qualitative research methods from the research team. The research team included an experienced qualitative researcher and a sociologist specializing in health-related stigma. To protect participant privacy, all information was kept confidential and not shared with medical staff involved in their care.
Prior to each interview, written informed consent was obtained, including permission for audio recording. With participants’ consent, interviews were recorded using a digital audio recorder. The interviews lasted between 20 and 50 min. During the interviews, researchers followed the semi-structured interview guide to explore participants’ experiences, while remaining flexible to pursue emergent topics. Researchers also took field notes, recording key words and nonverbal cues such as facial expressions and body language.
Consistent with Braun and Clarke's reflexive thematic analysis framework, 31 sample size was determined by data saturation rather than a priori statistical considerations. Saturation was assessed through an iterative process: after each interview, the research team met to discuss emerging themes and identify whether new information was being generated. Initial analysis suggested that thematic saturation was reached after 12 interviews, as no new codes or themes emerged from the data. To confirm saturation, we conducted four additional interviews; these confirmed that no new themes were identified, and the final two interviews yielded no novel insights. This sample size (n = 16) is consistent with previous qualitative studies on cancer survivorship, which have reported that data saturation typically occurs within 12–20 interviews. 35 At the end of each interview, participants completed a brief questionnaire to provide demographic information.
Data analysis
Data were analyzed following the reflexive thematic analysis framework described in Section 2.1. 31 To align with this paradigm, we explicitly engaged with our positionalities throughout the analysis process.
Our research team comprised three women, each bringing distinct perspectives. These included an oncology nurse with 10 years of clinical experience in breast cancer care, a sociologist specializing in health-related stigma, and a patient advocate who had completed breast cancer treatment five years prior. The patient advocate's inclusion was deliberate; she contributed insider knowledge of survivorship and a critical perspective on clinical narratives, but also held assumptions about the primacy of peer support that required reflexive scrutiny.
Before analysis, we identified several assumptions that could shape our interpretations. We initially assumed that social reintegration primarily meant returning to pre-diagnosis roles, and that physical appearance changes would be the most significant barrier. Each team member also acknowledged discipline-specific biases. The oncology nurse tended to prioritize clinical recovery, the sociologist focused on structural barriers, and the patient advocate emphasized emotional resilience, sometimes at the expense of acknowledging ongoing physical struggles.
We managed these positionalities through structured reflexive practices. After each analytical session, team members maintained individual reflexive journals, documenting emotional responses, emerging interpretations, and moments of dissonance. For example, the oncology nurse noted her initial impulse to code any mention of symptoms under “clinical concerns,” which she later challenged as potentially reducing participants’ lived experiences to medical categories.
We held regular peer debriefing sessions where we explicitly discussed how our biases were influencing coding. In one instance, during early coding, the team realized we were overlooking peer support groups, a blind spot attributed to the oncology nurse's clinical focus and the sociologist's emphasis on formal institutions. By revisiting transcripts with renewed attention to community-based resources, we were able to fully capture this theme. The patient advocate's perspective was particularly valuable here, as she helped the team interpret subtle references to online support communities that others might have missed. Conversely, we also remained attentive to her inclination to prioritize peer support, ensuring that other facilitators of reintegration, such as family or professional healthcare, were not under-coded.
We also attended to power dynamics by reminding ourselves during analysis that participants’ narratives should not be filtered through clinical or academic lenses. When interpreting potentially sensitive excerpts, we asked: “Would this interpretation resonate with the participant's own understanding?” Member checking further served to balance interpretive authority by returning transcripts and preliminary findings to participants; we invited them to act as co-interpreters of their own experiences, ensuring that our thematic conclusions remained grounded in their lived realities.
The analysis began with data familiarization, during which researchers repeatedly read transcripts while listening to audio recordings to immerse themselves in the data. In the initial coding phase, two researchers (the oncology nurse and the sociologist) independently conducted systematic line-by-line coding of the entire dataset using NVivo 11.0 Software. Each coder generated initial codes by assigning descriptive labels to segments of text that captured meaningful content related to social reintegration. Throughout this process, both researchers maintained individual reflexive journals in which they documented analytical decisions, emerging interpretations, and moments of uncertainty or dissonance. These journals served as a tool for tracking how personal assumptions and disciplinary biases might be shaping coding choices.
In accordance with the reflexive thematic analysis paradigm, we did not calculate inter-rater reliability coefficients such as Cohen's kappa. However, to provide transparency regarding the coding process, we noted that the two coders reached consensus on approximately 85% of the codes through initial discussions. The remaining 15% required further deliberation through the structured process described below. This approach recognizes that coding disagreements are not methodological errors to be eliminated, but rather generative opportunities for deeper engagement with the data. Within this framework, the goal is not to achieve uniform coding through statistical agreement, but to enrich interpretation through dialogue and reflexivity. Therefore, rather than quantifying agreement, we focused on how disagreements were interrogated and resolved. This resolution followed a structured process designed to enhance the richness and trustworthiness of our findings.
Discrepancies in coding were resolved through a structured process. First, the two coders engaged in peer debriefing to discuss divergent interpretations, returning to original transcripts for contextualization. When disagreements persisted, such as whether a statement reflected “acceptance” or “resignation”, the full team convened consensus meetings to collectively examine coded segments and explore alternative interpretations. For conflicts that remained unresolved, we employed member checking, referring relevant transcript excerpts back to participants for clarification.
Following coding, we collaboratively organized refined codes into candidate themes and constructed preliminary thematic maps. These themes were rigorously reviewed against coded extracts and the complete dataset through four iterative team discussions, each lasting approximately two hours. During theme refinement, we paid particular attention to ensuring that themes reflected participants’ lived experiences rather than our preconceptions. For example, an initial theme labeled “Overcoming physical barriers” was refined to “Reconstructing identity beyond physicality” after recognizing that participants’ narratives centered on redefining self-worth independent of physical appearance. This shift was prompted by the patient advocate's observation that clinical language of “overcoming” failed to capture the existential dimensions of their experiences.
The final analysis was synthesized into a coherent narrative, supported by illustrative data extracts. This systematic approach to coding and theme development, paired with ongoing reflexive practice, enhanced the trustworthiness and confirmability of the findings.
Ethical considerations
This study was approved by the Ethics Committee of a tertiary hospital in Nantong, Eastern China (Approval No. 2024041). All procedures adhered to the principles of voluntariness and confidentiality. Participants were informed of their right to withdraw at any time without consequence.
Results
Participants
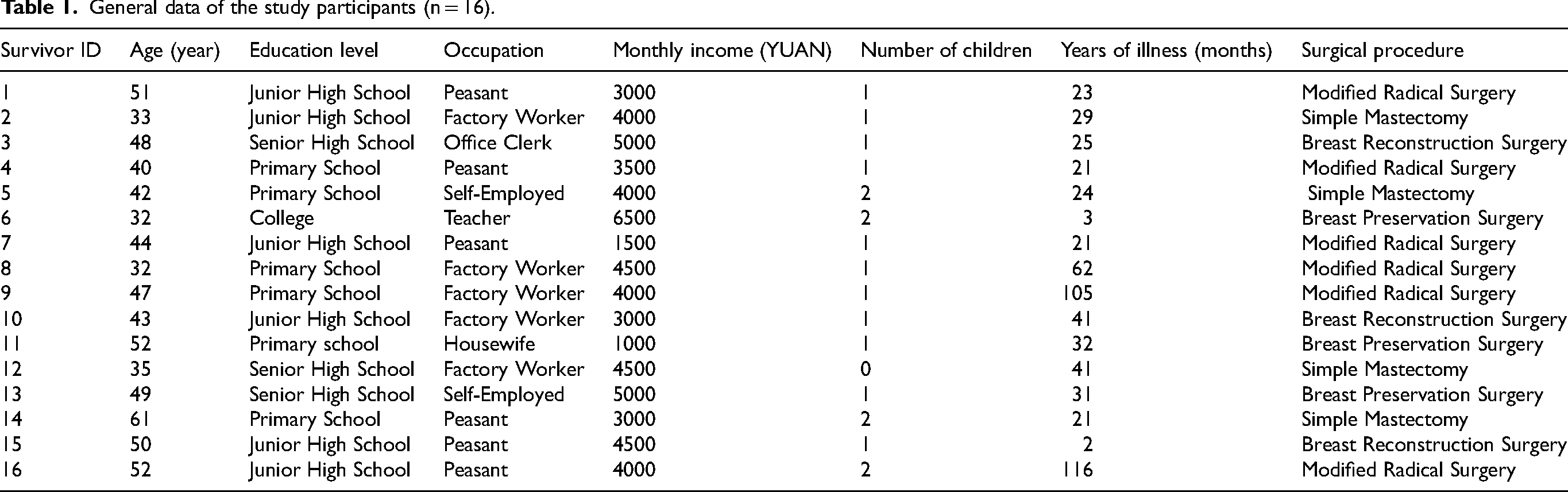
A total of 20 breast cancer survivors were invited to participate. Of these, two declined due to lack of interest and two declined due to privacy concerns, resulting in a final sample of 16 participants (see Table 1). The mean age of participants was 44.4 years (SD = 8.41; range: 32–61 years). The majority were married (n = 14, 87.5%) and had at least one child (n = 15, 93.7%). Interviews lasted an average of 35 min (range: 28–49 min).
General data of the study participants (n = 16).
Thematic analysis
Qualitative analysis identified four major themes that together illuminate the trajectory of social reintegration among breast cancer survivors. These themes capture a sequential yet iterative process: (1) reorganization of personal capabilities, (2) continuation of productive activities, (3) regular participation in social activities, and (4) reconstruction of post-cancer identities. Each theme comprised several sub-themes, which are summarized in Table 2. The number of participants who contributed to each theme is also indicated in the table.
Themes and sub-themes.
Theme 1: Reorganization of personal capabilities
Following cancer treatment, participants described an ongoing process of rebuilding their personal capacities to meet the demands of daily life. This theme captures how survivors actively engaged in restoring their physical health, strengthening their psychological resilience, acquiring new knowledge and skills, and building confidence in their ability to manage future challenges.
Sub-theme 1: Recovery of physical function
Participants described how breast cancer treatments, including surgery, radiotherapy, and chemotherapy, resulted in significant physical impairments such as reduced muscle strength, decreased joint mobility, and diminished cardiorespiratory function. For many survivors (n = 8), recovery of physical function was a foundational step toward social reintegration. They described how physical therapy, rehabilitation programs, and nutritional support facilitated their physical recovery, enabling them to resume daily activities and regain a sense of normalcy. “The chemotherapy is finally over. I feel like I'm much better than before; I can walk longer distances now and do light housework. My spirit has improved significantly too.” (Survivor 16) “I feel like I am gradually recovering, although the process is a little difficult. Now I can do things I used to enjoy, and my mood is much better. “ (Survivor 11)
Sub-theme 2: Enhancement of psychological resilience
Despite the profound distress associated with diagnosis and treatment, several survivors (n = 6) demonstrated remarkable psychological resilience. Their narratives revealed an ability to adapt to adversity, find meaning in their experiences, and develop new coping strategies.
One survivor described how her cancer experience helped her develop a more positive outlook: “I think this experience has made me stronger and taught me to cherish every little moment in my life. Sometimes I feel depressed, but I have learned how to adjust my mindset and look for the positive.” (Survivor 10)
For another survivor, resilience took on additional meaning given the cultural context. For Chinese women, divorce can carry significant social stigma, and survivors may be perceived as lacking family support. Her statement reflects not only personal resilience but also a reclaiming of autonomy: “Although I am divorced, I can now handle this on my own and no longer feel afraid.” (Survivor 13)
Sub-theme 3: Improvement of skills and knowledge
A majority of survivors (n = 12) actively sought out educational opportunities to better understand their condition and manage their health. These included hospital-based education sessions, lectures on disease management, and guidance from healthcare providers. Acquiring knowledge and practical skills empowered survivors to take an active role in their recovery and enhanced their sense of control. “In the ward, doctors and nurses often teach me how to exercise, especially exercises that are particularly helpful for recovery. After these classes, I not only learned how to take care of my own body but also gained a more thorough understanding of my disease.” (Survivor 2) “I’ m from the countryside, and the nurses here are really patient. They explained everything to me very clearly, and now I have a general understanding of this disease.” (Survivor 1)
Sub-theme 4: Enhancement of self-efficacy
Self-efficacy, the confidence in one's ability to execute behaviors necessary for recovery, emerged as a crucial outcome of the reorganization process. For several survivors (n = 8), successful experiences in treatment and daily management reinforced their belief in their capacity to overcome challenges, creating a positive feedback loop that sustained their efforts. “I trust the doctors, and my family has always been by my side. I believe that I can definitely recover from this illness.” (Survivor 7) “After this experience, I will definitely pay more attention to my own health and learn how to better deal with the pressure in my life. This experience has taught me that by facing challenges positively, no matter what difficulties I encounter, I have the ability to overcome them!” (Survivor 9)
Theme 2: Continuation of productive activities
Following treatment, survivors described a gradual process of re-engaging in productive activities that had been disrupted by their illness. This theme captures how survivors resumed both paid employment and unpaid roles, such as family caregiving, as integral components of their social reintegration. The continuation of productive activities not only restored a sense of normalcy and purpose but also reinforced survivors’ identities as capable and contributing members of society.
Sub-theme 1: Recovery of work capacity and workplace reintegration
For many survivors (n = 11), returning to work represented a significant milestone in their recovery journey. Survivors described how physical rehabilitation, including exercise and nutritional support, enabled them to regain the stamina and functional capacity required for employment. Additionally, psychological counseling and peer support groups helped survivors (n = 10) rebuild confidence, develop coping strategies, and approach workplace challenges with a renewed sense of resilience.
Workplace factors played a crucial role in this process. Several survivors (n = 5) cited accommodations like flexible hours, reduced workloads, and supervisor understanding as key facilitators. Attitudes from employers and colleagues could either help or hinder reintegration. While some found support, others faced stigma. Participants also faced occupational barriers, including physical limitations, cognitive challenges, and concerns about career progression. “I’ m a teacher… After chemo, I sometimes forget things mid-sentence. I wonder if it will affect my evaluations.” (Survivor 6) “When I first went back to the factory, the team leader arranged for me to work half-days for the first two weeks.” (Survivor 8) “Most of my colleagues were great, but there was one who kept asking if I was really well enough to be back.” (Survivor 10) “I've been with this company for over a decade. Before I got sick, I was being considered for a promotion. Now, no one mentions it. I don't know if they've forgotten or if they think I'm no longer capable.” (Survivor 13)
Sub-theme 2: Return to family roles
Family roles, the specific responsibilities and positions individuals hold within their family system, were profoundly disrupted by cancer treatment. As survivors’ physical health improved, most (n = 15) gradually resumed their roles in daily family life, including childcare, household management, and participation in family activities. This re-engagement not only contributed to family harmony but also reinforced survivors’ sense of being needed and valued, strengthening emotional bonds with family members.
One survivor described the tension between accepting help and fulfilling her perceived role as a homemaker: “My husband keeps telling me to leave all the household chores to him so that I can rest peacefully. However, I see that he is very busy, and I feel guilty. I still try my best to help him with the housework that I can manage.” (Survivor 3)
In the Chinese cultural context, where women are traditionally expected to manage domestic responsibilities, a husband's willingness to take over household tasks represents significant support. However, the survivor's guilt reflects the internalized pressure to fulfill her expected role, highlighting how cultural expectations can complicate the process of accepting care.
Another survivor highlighted the importance of resuming caregiving responsibilities: “Now I am responsible for supervising the children's homework at home. It's strange, but ever since I started overseeing their studies, I feel like I have become more patient.” (Survivor 10)
Theme 3: Regular participation in social activities
This theme captures how breast cancer survivors actively re-engaged with their social worlds through meaningful interactions and activities. Beyond simply “being social,” participation in social activities represented a deliberate effort to rebuild connections, reclaim a sense of normalcy, and construct a positive post-cancer identity. By engaging with others, whether through support groups, volunteering, or shared interests, survivors not only alleviated feelings of isolation but also reaffirmed their value and place within their communities.
Sub-theme 1: Construction and expansion of social networks
For several survivors (n = 6), connecting with others who shared similar experiences was a vital source of support. Through cancer-specific support groups, often facilitated by online platforms such as WeChat, survivors found spaces where they could openly share their struggles, exchange practical advice, and receive emotional validation. These networks provided a sense of belonging and reduced the loneliness that often accompanied the cancer journey. “We have a WeChat group full of people with this disease. We usually chat casually and cheer each other up. This communication makes me feel less lonely, and sometimes I get useful advice that helps me relax a lot.” (Survivor 15) “I follow a public account about breast cancer that often shares relevant information. From time to time, I click in to check it out, and I can ask any questions I have in the comments section.” (Survivor 5)
Sub-theme 2: Participation in public service and volunteering
A notable group of survivors (n = 9) channeled their experiences into public service and volunteer activities. By helping others, whether through promoting cancer screening, sharing their stories, or supporting fellow patients, these survivors transformed their illness experience into a source of meaning and purpose. This altruistic engagement not only facilitated their own psychological healing but also contributed positively to their communities. “There are two cancer screening activities in our community every year. Now I also help promote them, urging everyone to care more about their own health, take the initiative to get screened, have regular physical examinations, and take preventive measures in advance.” (Survivor 4) “I often share my anti-cancer journey in the anti-cancer WeChat group, chat with other survivors, and encourage each other, hoping they can get through this difficult time.” (Survivor 5)
Sub-theme 3: Cultivation and demonstration of interests
Re-engaging with personal interests and hobbies emerged as another important pathway to social reintegration for several survivors (n = 7). Whether tending to gardens, listening to music, or pursuing other creative outlets, these activities provided survivors with opportunities for self-expression, joy, and connection with others. Cultivating interests was not merely a distraction from illness but a deliberate act of reclaiming life and identity. “Before I got sick, I loved taking care of flowers. Now that I’m slowly recovering, I’ve filled my garden with flowers again and water them every day.” (Survivor 12) “I really loved listening to music when I was undergoing chemotherapy. It helped ease the pain of the treatment.” (Survivor 14)
Taken together, these forms of social participation did more than simply fill time or reduce loneliness. They provided the interpersonal context and relational experiences through which survivors could begin to renegotiate who they had become after cancer. This external re-engagement with the social world thus laid the groundwork for a deeper, internal process of identity transformation.
Theme 4: Reconstruction of post-cancer identities
Building on the social engagements described above, this theme captures the profound internal process through which survivors redefined who they were in the aftermath of cancer. Far from simply “returning to normal,” participants described a fundamental renegotiation of their sense of self, one that involved coming to terms with bodily changes, reorienting their priorities, and discovering new sources of meaning and purpose. This identity reconstruction was not a linear process but an ongoing negotiation between the person they were before cancer, the person they became during treatment, and the person they aspired to be in the future.
Sub-theme 1: Remodeling of self-identity
For many survivors (n = 7), the most intimate and challenging aspect of recovery was learning to live with a changed body and a changed self. Breast cancer treatment, particularly mastectomy, had altered their physical appearance and, with it, their sense of femininity and wholeness. Remodeling self-identity involved a gradual process of accepting these changes, redefining personal worth beyond physical appearance, and integrating the cancer experience into a new, coherent sense of self. “My breasts were removed, and I really struggled to accept that at first. But then, when I thought about it, this is also a new beginning in my life. I slowly accepted the change in my body, which made me feel that it was no big deal.” (Survivor 12) “Now I try to wear loose clothes and a hat when I go out. I feel like a normal person again.” (Survivor 2)
Sub-theme 2: Lifestyle adjustment and integration
Identity reconstruction was not confined to internal psychological processes but was enacted through tangible changes in daily life. For several survivors (n = 9), adopting healthier routines, including dietary changes, regular exercise, and consistent medical follow-up, became a way of embodying their new identity as someone who prioritizes health and well-being. These lifestyle adjustments were often supported by family members, further reinforcing survivors’ sense of being cared for and their commitment to recovery. “My husband now cooks for me every day, making meals with meat, eggs, and vegetables, and he won’t let me eat greasy, high-calorie foods.” (Survivor 1) “This illness made me suddenly realize that my body is my most valuable asset. Now I go to bed by 10 o’clock every night and walk in the neighborhood after dinner. My husband even quit smoking for me.” (Survivor 11)
Sub-theme 3: Spiritual and emotional growth
For the majority of survivors (n = 11), the cancer experience catalyzed profound spiritual and emotional growth. Confronting mortality and enduring significant suffering led survivors to reevaluate their priorities, deepen their appreciation for life, and strengthen their connections with loved ones. This growth was not about finding a silver lining but about fundamentally reorienting one's relationship to self, others, and the world. “Despite this illness, I’ve come to understand how important my family is to me. I’m truly grateful for them being by my side, and I will cheer up and face all of this more positively.” (Survivor 3) “I trust my doctor, and I believe in current medical technology. I know I can get better. Once I’m well, I’m going to keep living my best life!” (Survivor 13)
Discussion
This qualitative study explored the lived experiences of social reintegration among breast cancer survivors in China, revealing four interconnected themes: reorganization of personal capabilities, continuation of productive activities, regular participation in social activities, and reconstruction of post-cancer identities. These findings illuminate the multifaceted nature of post-treatment recovery and have important implications for clinical practice, policy development, and future research.
Consistent with previous research, 36 our findings underscore the crucial role of partner support in facilitating reintegration. Partners contributed across emotional, practical, and social domains.37–39 Importantly, partner support also facilitated identity reconstruction; by accepting and affirming survivors’ changed bodies and selves, partners helped them integrate the cancer experience into a coherent and positive self-concept. 40 Our findings extend this understanding by revealing the mechanisms through which partner support operates in the Chinese cultural context. Participants frequently described their partners’ support as “not needing to ask”, an attunement that reduced the burden of having to articulate needs. This tacit, anticipatory form of support may be particularly valued in cultural contexts where direct expression of needs is less normative. Moreover, for several participants, partner support was intertwined with family-based care, reflecting a collective approach to recovery that extends beyond the dyadic relationship. This highlights that reintegration is not an individual journey but a relational one, embedded within intimate partnerships and broader family systems. Interventions in collectivist cultural contexts should therefore consider the couple and the family as a unit, providing support and resources to partners and family members alongside survivors.
Another distinctive finding was the role of digital platforms in facilitating social connection. Participants who engaged in rehabilitation groups, support groups, and community activities reported feeling “still part of society”, a powerful indicator of successful reintegration. These findings align with a growing body of evidence41–43 demonstrating that collective participation fosters learning, mutual support, and a sense of belonging. Through sharing experiences and coping strategies, survivors gain practical knowledge, validate their own experiences, and find meaning in helping others. Our study adds a novel dimension by highlighting the role of digital platforms, particularly WeChat, in facilitating these collective experiences. In China, where geographic distance and time constraints can limit in-person participation, online support groups provided accessible, continuous, and often anonymous spaces for connection. Participants described these digital communities as “always there”, offering both practical advice and emotional validation outside of scheduled meetings. This finding has important implications for healthcare systems. Integrating digital peer support platforms into standard survivorship care can extend reach to survivors in rural or underserved areas where in-person resources may be limited.
Workplace reintegration emerged as a particularly challenging domain within the theme of continuation of productive activities. Our findings extend the occupational rehabilitation literature by revealing several underappreciated tensions that Chinese breast cancer survivors navigate when returning to work. First, participants described a tension between their motivation to resume professional roles and the reality of cognitive side effects (“chemo brain”), including persistent difficulties with memory, attention, and processing speed. 44 These challenges were particularly distressing for survivors in high-demand occupations, yet remain underrecognized in workplace accommodation policies in China. 45 Second, our data revealed a pervasive tension around career progression. Younger survivors expressed anxiety that their cancer history would permanently derail their career trajectories, describing being overlooked for promotions or steered toward less demanding roles. These experiences reflect what occupational rehabilitation scholars have termed “stalled careers”, where survivors face invisible barriers to advancement that profoundly affect long-term economic security. Third, employer attitudes emerged as a critical factor shaping reintegration outcomes. Participants described a spectrum of responses, from supportive accommodations to subtle discrimination. Notably, several reported “compassionate overprotection”, where managers reduced survivors’ responsibilities with good intentions, inadvertently undermining confidence. This resonates with literature on benevolent ableism. 46 Importantly, successful reintegration was often attributed to specific, negotiated accommodations rather than generalized “protective” reductions in responsibility, suggesting a need for employer training on autonomy-preserving accommodations.
Consistent with prior research,10,13 our findings confirm that disease-related knowledge and self-management skills are foundational to successful social reintegration. However, beyond simply confirming this association, our study reveals how knowledge functions as an empowerment tool in the Chinese context. Participants who engaged in education programs and peer support networks described not only acquiring information but also developing a sense of legitimacy to question healthcare providers and advocate for their own needs. This form of empowerment may be particularly significant in hierarchical medical systems where patient passivity is often expected. This suggests that knowledge-based interventions in China should aim not only to inform but also to cultivate patients’ confidence in actively participating in their own care decisions.
Our findings also highlight the pervasive impact of public stigma on survivors’ reintegration. Participants described experiences of being avoided, questioned, or pitied, consistent with previous studies documenting the psychosocial burden of cancer survivorship.47–49 This cultural nuance suggests that public education campaigns in China should move beyond simply raising awareness to actively challenging stereotypes about cancer survivors’ competence and agency. Such efforts may be particularly important in workplace settings, where misconceptions about survivors’ ability to perform effectively can create subtle but significant barriers to career advancement.
A cross-cultural comparison reveals both commonalities and distinctive features of social reintegration among Chinese breast cancer survivors relative to Western populations. Consistent with studies from the United States and Europe, 37 our participants identified partner support, workplace reintegration, and stigma management as central to their recovery. However, several culturally specific patterns emerged. First, the tacit, anticipatory nature of partner support (“not needing to ask”) contrasts with Western studies that emphasize explicit communication of needs as a marker of healthy dyadic coping. 50 In individualistic Western contexts, partners are encouraged to openly discuss care needs. In China's collectivist culture, attunement and nonverbal understanding are highly valued, potentially reducing the emotional burden of articulating needs during a vulnerable period. Second, the role of digital platforms, particularly WeChat, in facilitating peer support appears more pronounced in China than in Western countries, where in-person support groups remain prevalent. This reflects both the ubiquity of WeChat in daily Chinese life and the geographic and time constraints that make online communities a pragmatic solution. Third, while workplace discrimination against cancer survivors is documented globally, 51 the subtle, overprotective behaviors we observed in Chinese workplaces appear to be particularly salient in Confucian-influenced settings. In such settings, hierarchical relationships and paternalistic care norms can blur the line between support and condescension. These cross-cultural differences suggest that Western interventions cannot be directly imported to China without cultural adaptation. Conversely, our findings on cognitive symptom management and stalled career progression echo Western occupational rehabilitation literature, 52 suggesting these challenges may be universal and amenable to cross-cultural intervention strategies. Future comparative research should directly examine reintegration experiences across multiple cultural contexts using harmonized methods to identify which barriers are context-specific and which are shared globally.
A notable finding was that younger survivors expressed stronger motivation and more active strategies for reintegration, including efforts to manage appearance changes, return to work, and engage proactively with treatment. While this aligns with existing literature53–55 suggesting that developmental context shapes survivorship experiences, our findings extend this understanding by revealing the tensions that younger survivors navigate. For these women, often in critical phases of career building and family formation, the urgency to return to pre-illness roles coexisted with heightened anxieties about fertility, body image, and long-term career trajectories. This duality suggests that age-sensitive interventions should not merely leverage younger survivors’ motivation but also provide targeted support for the specific challenges they face. These include workplace accommodations, fertility preservation counseling, and body image interventions that address the unique pressures of maintaining appearance in youth-oriented social and professional contexts.
Finally, our findings confirm that emotional experiences play a pivotal role in shaping reintegration outcomes. Positive emotions, such as hope, optimism, and gratitude, facilitated engagement with social life, while negative emotions, including anxiety, sadness, and fear, posed significant barriers. While this aligns with prior research,46,56,57 our study reveals the dynamic interplay between emotions and social participation that has been less fully characterized. Participants described how initial anxiety about returning to social situations gradually gave way to confidence through repeated positive experiences, creating a self-reinforcing cycle. Conversely, experiences of stigma or misunderstanding could trigger emotional setbacks that required renewed coping efforts.
This study makes several contributions to the literature on cancer survivorship and occupational rehabilitation. First, it provides one of the first in-depth qualitative accounts of social reintegration among breast cancer survivors in China, addressing a significant gap in non-Western contexts. Second, by employing a reflexive thematic analysis approach, it captures the nuanced, culturally specific meanings that survivors attach to their reintegration experiences. These include the previously underexplored dynamics of workplace reintegration, such as cognitive symptom management, stalled career progression, and the paradoxical effects of compassionate overprotection from employers. Third, the study identifies culturally distinctive mechanisms of support, including the tacit, anticipatory nature of partner support (“not needing to ask”) and the role of digital platforms (WeChat) in facilitating peer connection. These findings have practical implications. First, interventions should consider the family as a unit rather than focusing solely on the individual survivor. Second, healthcare systems should integrate digital peer support platforms into standard survivorship care. Third, workplace-based interventions should include employer training on cancer-related cognitive impairment, the development of flexible and autonomy-preserving return-to-work policies, and the establishment of clear pathways for addressing subtle career stagnation. Fourth, educational efforts should aim to cultivate survivors’ self-advocacy skills alongside disease-related knowledge. Future research should explore the effectiveness of culturally adapted interventions across different regions of China and among diverse survivor populations, with particular attention to testing workplace accommodation models that address both the cognitive and career progression challenges identified in this study.
Strengths and limitations
This study offers an in-depth, contextually grounded exploration of social reintegration among breast cancer survivors in China, using rigorous qualitative methods and adhering to the COREQ checklist.
However, several limitations should be acknowledged. First, the RNLI ≥60 inclusion criterion required participants to have moderate to high reintegration levels at enrollment, systematically excluding survivors with poor reintegration (RNLI < 60). Our findings therefore represent survivors who have achieved at least partial success in resuming social roles, leaving unexamined those who remain persistently isolated, unemployed, or role disrupted. This substantially affects transferability to clinical populations with poor reintegration outcomes, including those with physical debility, mental health comorbidities, inadequate support networks, or structural barriers such as poverty or geographic isolation.
Second, the sample was demographically homogeneous: most participants were married (87.5%), had children (93.7%), and resided in Eastern China. Findings may not transfer to unmarried, divorced, or childless survivors, nor to those from Central/Western China or rural areas, who may face different barriers related to healthcare access, economic resources, and cultural attitudes.
Third, as with all qualitative research, the findings are shaped by participants’ subjective accounts and the researchers’ interpretive lens. This introduces potential for interpretive bias.
Fourth, the cross sectional design captures reintegration at a single time point. The recovery trajectory from treatment to full reintegration is prolonged and nonlinear. Our data miss both the very early phase, marked by acute uncertainty immediately after active treatment, and the late consolidation phase, when reintegration may stabilize or deteriorate years post-treatment. Consequently, we cannot determine whether positive adaptations like identity reconstruction are sustained over time. Moreover, our thematic trajectory suggests a linear progression that cross sectional data cannot validate; we do not know whether survivors follow this sequence, whether phases overlap, or whether some cycle back after setbacks.
Fifth, we recognize the inherent power imbalance between our team (including a nurse and sociologist) and participants, which may have influenced responses. Participants may have provided socially desirable answers or been reluctant to disclose critical views of medical professionals. To mitigate this, we emphasized voluntary participation, assured confidentiality, used open ended questions, and engaged in reflexive practices (Section 2.5). Nevertheless, this power dynamic remains inherent to qualitative research and should be considered when interpreting findings.
Conclusion
This qualitative study provides a comprehensive exploration of social reintegration among breast cancer survivors in China, identifying four core themes: reorganization of personal capabilities, continuation of productive activities, regular participation in social activities, and reconstruction of post-cancer identities. These themes illuminate the multifaceted challenges survivors face and the adaptive strategies they employ, offering a nuanced understanding of the reintegration process.
The findings have important implications for clinical practice, highlighting the need for individualized, age-sensitive, and relationally oriented interventions that address not only physical recovery but also psychological, social, and identity-related dimensions of survivorship. For policymakers, the results underscore the value of public education, peer support infrastructure, and community engagement in creating environments that facilitate reintegration.
Future research should build on these findings by including larger, more diverse samples across multiple institutions and geographic regions. Longitudinal designs are particularly needed to trace the dynamic evolution of reintegration needs and strategies across different phases of recovery, offering deeper insight into long-term adaptation and well-being. 58 Additionally, intervention studies testing the effectiveness of specific support programs, such as peer mentoring, couple-based interventions, or workplace reintegration initiatives, would provide actionable evidence for improving care. By advancing both understanding and practice, we can better support breast cancer survivors in not only surviving but thriving in the years beyond treatment.
Footnotes
Acknowledgements
The authors would like to thank all the participants who generously shared their experiences and time for this study.
Ethical considerations
This study was reviewed and approved by the Medical Ethics Committee of Nantong Tongzhou Hospital of Traditional Chinese Medicine (Approval No. 2024041). All procedures performed were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments.
Consent to participate
Written informed consent was obtained from all individual participants included in the study. Participants were fully informed of the study purpose, procedures, potential risks and benefits, and their right to withdraw at any time without consequences.
CRediT authorship contribution statement
Dandan Gu: Writing – original draft, Validation, Methodology, Investigation, Formal analysis, Data curation. Ming Yu: Writing – original draft, Software, Methodology, Formal analysis. Yangyang Zan, Lili Jiang: Writing – review & editing, Investigation. Yizhou Gu: Investigation, Data curation. Yangyang Cao: Writing – review & editing, Supervision, Project administration, Methodology, Conceptualization.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Nantong Municipal Social and Livelihood Science and Technology Program (Grant No. MSZ2025177) and the Scientific Research Project of Nantong Municipal Health Commission (Grant No. QN2024071).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.