
Abstract
Background
Major public health events have wide-ranging and far-reaching effects, while also causing significant psychological problems for healthcare professionals, particularly those directly involved in patient care.
Objective
The present study aimed to explore the mediating role of mental health and the moderating role of caring for COVID-19 patients in the relationship between hospital violence and self-efficacy expectation among Chinese healthcare professionals.
Methods
This was a cross-sectional study conducted in the early stage of the epidemic. A total of 3006 Chinese healthcare professionals completed the assessment of hospital violence, self-efficacy expectation (SEE), and mental health using a set of instruments, including the visual analog scale (VAS), the Patient Health Questionnaire-9 (PHQ-9), and the Generalized Anxiety Disorder-7 (GAD-7).
Results
The study found that hospital violence experience was significantly correlated with higher depressive symptoms (r = 0.168, p < 0.001), higher anxiety (r = 0.171, p < 0.001), and lower SEE (r = -0.062, p < 0.01). The association between hospital violence and lower self-efficacy expectations was stronger among those who directly provided healthcare services to patients (B = -5.35, p < 0.01) than among those who did not provide direct patient care (B = -2.07, p < 0.05). Depression and anxiety, as mediating variables, accounted for 54.4% and 48.66% of the total effect of the relationship between hospital violence and SEE, respectively.
Conclusions
During major public health events, experiences of workplace violence may reduce the self-efficacy expectations of healthcare professionals, particularly among those who directly provide patient care. Mental health plays a mediating role in this relationship.
Keywords
Background
Self-efficacy expectation (SEE), derived from Bandura's self-efficacy theory, refers to an individual's belief in their capability to perform a specific behavior in a given situation.1,2 The study found that when individuals are exposed to highly threatening environments for a prolonged period, they may experience strong emotional arousal, such as anxiety, which can reduce SEE.3,4 Public health crises, such as the COVID-19 pandemic, represent a typical form of large-scale environmental trauma exposure. Healthcare professionals were exposed to frightening and threatening conditions, including workplace violence, infectious risks, and work overload, which may reduce their confidence in successfully treating patients. On the other hand, the collective determination to fight the pandemic, as well as public dependence on and recognition of medical personnel, may enhance healthcare workers’ sense of personal achievement and help them overcome difficulties, 5 which may increase the SEE of healthcare professionals. Few studies have explored the relationship between environmental factors and SEE. Previous studies have shown that high self-efficacy improves employees’ overall health. 6 An increase in SEE is associated with a reduction in depressive symptoms. 7 Improving SEE can effectively reduce psychological exhaustion among healthcare professionals during public health emergencies and improve work efficiency. Therefore, the relationship between highly threatening environments (such as major public health events, including the COVID-19 pandemic) and SEE among healthcare workers warrants further investigation.
Violence in the workplace, such as hospital violence, has become a global public health problem. Healthcare workers have been reported to be one of the most vulnerable groups to such violence. In the context of China, hospital violence is often closely related to medical disputes or physician-patient conflicts, 8 which significantly reduces their job satisfaction. 9 This may also increase their intention to leave. Recent research has found that the impact of hospital violence has worsened during the COVID-19 pandemic. The physical and emotional burden on healthcare workers is substantial, which further threatens patient care and hospital productivity. 10 There are two types of violence: physical and psychological violence. 11 The frequency of verbal violence is often higher. 12 Besides, the harm caused by direct violence primarily affects those who have experienced it, whereas witnessing violence has a different impact, and their work motivation differs significantly. 13 Regardless of the type of violence experienced, the impact of direct personal experience is greater and warrants further investigation.
Violence against healthcare professionals engaged in patient care not only affects their health but also leads to a decline in self-efficacy expectations. However, there are few related studies on this issue. 14 Previous studies have suggested that workplace violence can lead to job burnout among healthcare workers. 15 A decrease in self-efficacy expectation is one of the characteristics of burnout. 16 Besides, hospital violence can lead to emotional exhaustion, 17 which is an important factor influencing self-efficacy expectation. Thus, hospital violence may be associated with self-efficacy expectations. In addition, numerous studies have shown that hospital violence can affect individual mental health. Violence against healthcare workers is associated with an increased risk of mental health problems, such as depression, anxiety, and suicidal ideation. 18 Compared with healthcare workers who have not experienced hospital violence, those who have experienced hospital violence are more likely to experience anxiety and depression. 19 This may be because workplace violence causes psychological stress, which in turn damages individuals’ mental health. 20 Therefore, we hypothesized that hospital violence may affect self-efficacy expectations by leading to poor mental health (i.e., depression and anxiety).
It is worth noting that this relationship may vary during major public health events. During the COVID-19 pandemic, there were not only healthcare professionals on the front line who directly provided medical treatment to COVID-19 patients in affected areas, but also those who did not come into direct contact with COVID-19 patients and were mainly responsible for epidemic prevention and control in areas with relatively effective epidemic management. As a populous transitional economy with 1.39 billion citizens, China faces the challenge of meeting healthcare demands with limited medical resources. 21 COVID-19 has led to a substantial increase in the number of patients and the rapid consumption of medical resources, which has had an adverse impact on healthcare workers, especially frontline staff. Direct contact with patients is associated with a greater risk of infection. 22 They have faced difficult decisions due to the enormous influx of patients with life-threatening infections and the limitations in available effective medications and lifesaving equipment.23,24 Healthcare professionals involved in the treatment of COVID-19 may experience both short- and long-term psychological consequences associated with this period. 25
This may be due to emotional instability, which may contribute to an increased occurrence of violent incidents during the pandemic. 26 During this special period, those who have experienced or witnessed violence may also witness violence toward their colleagues and even experience varying degrees of hospital violence themselves.27,28 Hospital violence may reduce self-efficacy. 29 The positive effects of the COVID-19 pandemic may weaken this effect. When healthcare workers receive public gratitude and develop a sense of professional mission in combating the pandemic, they may experience corresponding positive emotions, which may help them overcome negative emotions under difficult conditions. 30 Therefore, the COVID-19 pandemic may have both negative and potentially protective effects simultaneously. 31 For front-line healthcare professionals involved in the treatment of COVID-19, the impact of hospital violence on self-efficacy expectations warrants further investigation. Moreover, the mediating role of psychological factors in the relationship between hospital violence and self-efficacy expectation may also differ.
It should be noted that the data used in this study were collected during the early phase of the COVID-19 pandemic and should therefore be interpreted as reflecting a historical baseline rather than being considered outdated. Factors contributing to the high incidence of workplace violence during this period included extended working hours, close contact with patients, and concerns about viral infection. 32 In particular, front-line staff have experienced increased negative emotional distress, accompanied by a significant decline in quality of life. 33 In the context of major public health crises, ensuring a safe working environment for healthcare workers is essential. 34 In addition, higher levels of self-efficacy expectation among healthcare workers are significantly associated with greater well-being. 35 Although there are existing studies that have implemented interventions among healthcare workers involved in the COVID-19 pandemic to reduce the impact of workplace violence and enhance their self-efficacy, evidence on the underlying mechanisms remains limited, 36 It remains unclear whether direct involvement in the care of COVID-19 patients moderates the relationship between workplace violence and self-efficacy. The present cross-sectional data may provide a useful reference for the assessment and intervention of front-line healthcare workers during the pandemic.
Research on the relationship between hospital violence and self-efficacy expectations among healthcare professionals remains limited. Recent evidence synthesized by Eshah et al. highlights that workplace violence against healthcare workers remains a pervasive global problem with serious implications for staff well-being, quality of care, and workforce retention. 37 The purpose of this study was to investigate the psychological effects of hospital violence on self-efficacy expectation (SEE), as well as the moderating effect of caring for COVID-19 patients on the relationship between hospital violence and SEE. Therefore, we hypothesized that: (1) Hospital violence is associated with reduced self-efficacy expectations. Moreover, this association may vary among healthcare workers involved in frontline patient care during the pandemic; and (2) mental health conditions mediate the relationship between hospital violence and SEE.
Methods
Participants and procedure
This cross-sectional data in this study were derived from an online survey conducted between March 27 and April 26, 2020, approximately one month after the pandemic had been brought under control in China. Details of the participant enrollment process have been reported elsewhere. 38 First, an initial group of respondents was selected. After completing the survey, these respondents were encouraged to recruit additional participants who met the study criteria, and subsequent participants were enrolled based on these referrals, forming a snowball sampling process. In total, invitation letters were initially distributed to 19,583 potential participants via the WeChat network. Of these, 4003 individuals agreed to participate. Among them, 28 participants declined after reading the informed consent form, resulting in 3975 completed questionnaires. After data screening, 968 questionnaires were excluded due to missing values, duplicate submissions, or ineligible participants. A total of 3006 valid questionnaires, including 583 nurses and 2423 physicians, were retained for the final analysis. The inclusion criteria were physicians and nurses with at least two years of clinical experience in hospitals in mainland China. The exclusion criteria were as follows: (1) having been absent from clinical practice for six months or longer in the past two years; (2) inability to complete the online questionnaire due to visual or other impairments affecting the use of the internet or mobile devices; and (3) not holding a valid license to practice.
The survey was conducted anonymously. Participants were not permitted to submit the questionnaire multiple times using the same device, and the survey platform was configured to prevent duplicate submissions. Online informed consent was obtained by asking participants to indicate their agreement by selecting one of the following options on the screen: “I agree to participate in the study” or “I do not agree to participate in the survey”. If a participant selected “I do not agree to participate in the survey”, the survey was terminated immediately.
Measures
Sociodemographic characteristics
The sociodemographic questionnaire collected information on age, gender, educational attainment, ethnicity (Han or minority groups), specialty, work setting (general ward, intensive care unit, or emergency department), and years of practice. Participants were also asked whether they were directly involved in the care of patients with COVID-19, and were categorized into two groups accordingly (yes or no).
Self-efficacy expectations
Previous studies have suggested that a visual analog scale (VAS) can serve as a simple and efficient measure of self-efficacy, with acceptable validity. It may also improve participant compliance, particularly when multiple assessments are required. 39 Similarly, VAS has been used to assess self-efficacy expectations. 40 In this study, self-efficacy expectation (SEE) was measured using a VAS ranging from 0 (“not at all”) to 100 (“completely”), based on the following question: “In general, to what extent do you think doctors can solve patients’ health problems?” Lower scores indicate lower levels of self-efficacy expectation.
Hospital violence
In China, the frequency of hospital violence against healthcare professionals was assessed using the Chinese version of the Workplace Violence Scale (WVS), which has demonstrated good reliability and validity. This scale measures experiences of physical, psychological, and verbal violence over the past 12 months. 41 However, to reduce respondent burden and improve participation rates, hospital violence was assessed using a single self-reported dichotomous item adapted from the conceptual framework of the Chinese version of the WVS. Participants were asked: “Have you experienced physical or verbal violence from a patient or their family member (including abuse, physical assault, intimidation, etc.) in the past 12 months?” Response options were “yes” or “no”. Individuals who reported at least one incident of violence were classified as violence-positive.
Mental health conditions
Depressive and anxiety symptoms were assessed using the 9-item Patient Health Questionnaire (PHQ-9) and the 7-item Generalized Anxiety Disorder scale (GAD-7), respectively. 42 Both the PHQ-9 and GAD-7 are scored on a 4-point Likert scale ranging from 0 (“not at all”) to 3 (“nearly every day”). The total PHQ-9 score ranges from 0 to 27, with higher scores indicating more severe depressive symptoms. The total GAD-7 score ranges from 0 to 21, with higher scores indicating more severe anxiety symptoms. In this study, total scores were used to assess levels of depression and anxiety. Cronbach's α coefficients for the present sample were 0.91 for the PHQ-9 and 0.94 for the GAD-7.
Data analysis
All analyses were conducted using SPSS statistical software. Descriptive statistics were used to summarize participants’ sociodemographic characteristics. Pearson correlation analyses were performed to examine the relationships between variables. Several covariates were included in subsequent analyses, including age, profession (nurse or physician), location, educational attainment, and work setting.
Prior to regression analyses, statistical assumptions were assessed. Normality of residuals was evaluated using histograms and Q-Q plots. Homoscedasticity was examined through visual inspection of standardized residual plots. Multicollinearity was assessed using variance inflation factors (VIFs), with all values below the acceptable threshold (VIF<5), indicating no significant multicollinearity. Linear regression analyses were conducted to examine the association between hospital violence and SEE, as well as the moderating role of caring for COVID-19 patients. Mediation analyses were performed using the PROCESS macro developed by Hayes. 43 Model 4 was specified to test the mediating effect, with 5000 bootstrap samples. Bias-corrected 95% confidence intervals were used to estimate the indirect effects, and mediation was considered statistically significant if the confidence interval did not include zero.
Results
Demographic characteristics
As shown in Table 1, 65.1% of the participants were female, 75.4% were married, and 87.7% were of Han ethnicity. Most participants were physicians (80.6%) and held a bachelor's degree (67.5%). The majority worked in general wards (57.5%), followed by outpatient departments (17.5%), intensive care units (3.7%), and other departments (21.4%). More than half of the participants (61.8%) were located in the western region of China. Overall, 64.2% of participants reported experiencing hospital violence, and 79.7% reported witnessing violence toward their colleagues. In addition, 22.2% of the sample were directly involved in the care of COVID-19 patients. Participants who had experienced or witnessed hospital violence reported significantly lower SEE scores. Compared with physicians, nurses reported significantly higher levels of self-efficacy expectation. Healthcare workers with higher educational attainment reported lower self-efficacy expectations.
Comparison of differences in self-efficacy expectation among different groups.
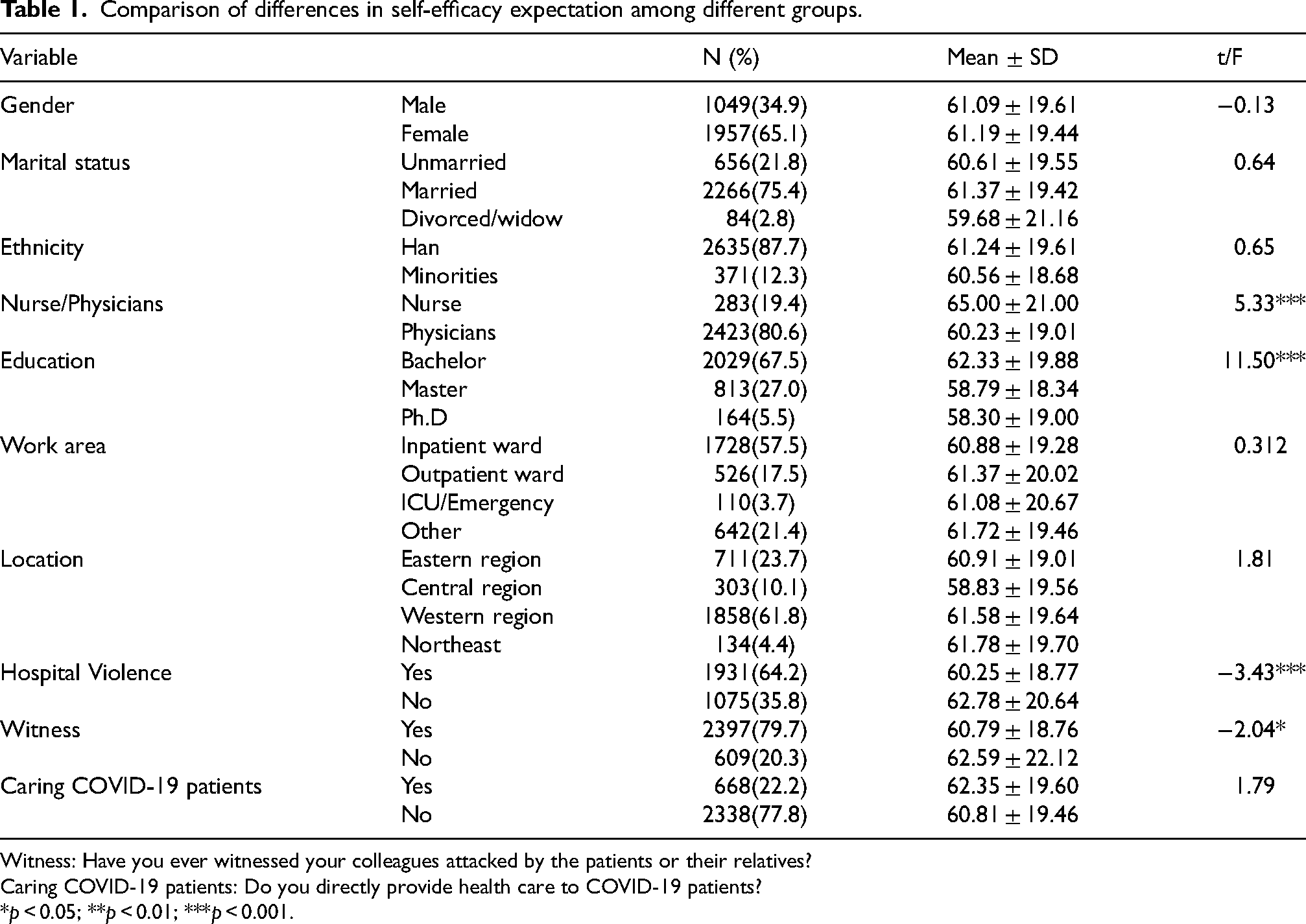
Witness: Have you ever witnessed your colleagues attacked by the patients or their relatives?
Caring COVID-19 patients: Do you directly provide health care to COVID-19 patients?
*p < 0.05; **p < 0.01; ***p < 0.001.
Correlation analysis among variables
The correlation matrix of the main variables is presented in Table 2. The mean SEE score was 61.15 ± 19.5. The mean PHQ-9 score was 10.64 ± 6.03, and the mean GAD-7 score was 8.30 ± 5.31. Hospital violence experience was significantly correlated with higher depressive symptoms (r = 0.168, p < 0.001), higher anxiety levels (r = 0.171, p < 0.001), and lower SEE (r = -0.062, p < 0.01). Depressive symptoms were negatively correlated with SEE (r = -0.193, p < 0.001), whereas involvement in the care of COVID-19 patients was not significantly correlated with SEE during the pandemic. Although several correlations were statistically significant, most effect sizes were small, suggesting modest associations among the study variables.
Correlation matrix among variables.
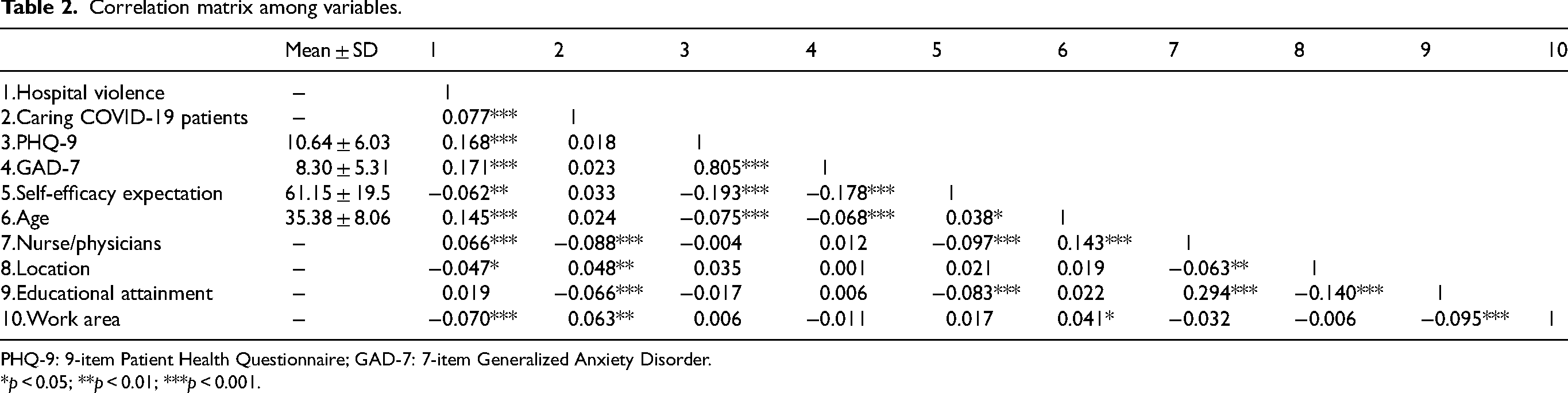
PHQ-9: 9-item Patient Health Questionnaire; GAD-7: 7-item Generalized Anxiety Disorder.
*p < 0.05; **p < 0.01; ***p < 0.001.
Associations between SEE and study variables
As shown in Table 3, the multivariate linear regression model indicated that being a physician (B = -4.10, p < 0.001), having a PhD degree (B = -3.23, p < 0.05), and experiencing hospital violence (B = -2.66, p < 0.001) were associated with lower SEE. Among those directly involved in the care of COVID-19 patients, hospital violence was more strongly associated with SEE (B = -5.35, p < 0.01). In contrast, among those not directly involved in patient care, the association between hospital violence and SEE was weaker (B = -2.07, p < 0.05), suggesting a potential moderating effect of involvement in COVID-19 patient care on this relationship. Therefore, hierarchical linear regression analysis was conducted to further examine this moderating effect. As shown in Supplementary Table S1, a marginally significant moderating effect of participation in the treatment of COVID-19 patients on the relationship between hospital violence and SEE was observed (B = -3.29, p = 0.075).
Multivariate linear regression analysis of predictors of self-efficacy expectation.
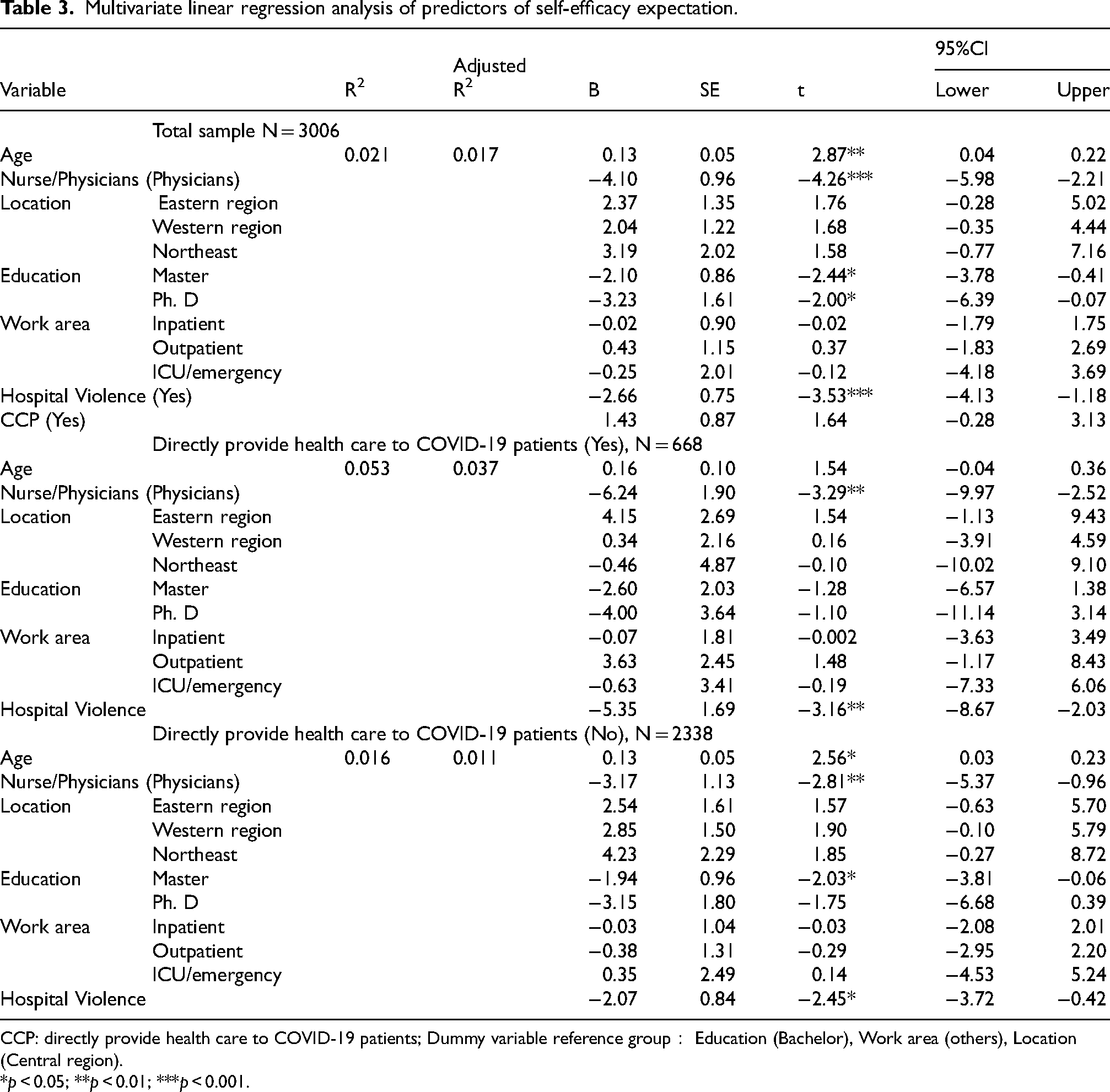
CCP: directly provide health care to COVID-19 patients; Dummy variable reference group: Education (Bachelor), Work area (others), Location (Central region).
*p < 0.05; **p < 0.01; ***p < 0.001.
Mediation effect of mental health conditions on the relationship between hospital violence and SEE
The results of the mediation analyses are presented in Table 4. Depression showed a significant indirect effect on the relationship between hospital violence and SEE (B = -1.42, p < 0.001), while the direct effect was not statistically significant (B = -1.19, p > 0.05). Similarly, anxiety also demonstrated a significant indirect effect (B = -1.27, p < 0.001), whereas the direct effect was not significant (B = -1.34, p > 0.05). Detailed results are presented in Figure 1. The indirect effect through depression accounted for 54.4% (|Indirect effect/total effect|*100%=1.42/2.61*100%) of the total effect of hospital violence on SEE, while the indirect effect through anxiety accounted for 48.66% (|Indirect effect/total effect|*100%=1.27/2.61*100%). Stratified analyses indicated that the mediating effects of depression and anxiety were more pronounced among participants not directly involved in the care of COVID-19 patients than among those who were directly involved (see Supplementary Tables S2 and S3). Specifically, depression accounted for 26.64% (|Indirect effect/total effect|*100%=1.46/5.48*100%) of the total effect among those directly involved in COVID-19 patient care, compared with 69.6% (|Indirect effect/total effect|*100%=1.42/2.04*100%) among those not directly involved. Similarly, anxiety accounted for 32.85% (|Indirect effect/total effect|*100%=1.80/5.48*100%) of the total effect among front-line participants and 55.39% (|Indirect effect/total effect|*100%=1.13/2.04*100%) among non-front-line participants.

Mediating effect of mental health conditions on the relationship between hospital violence and self-efficacy expectation.
Mediating effect of mental health conditions on the relationship between hospital violence and self-efficacy expectation.
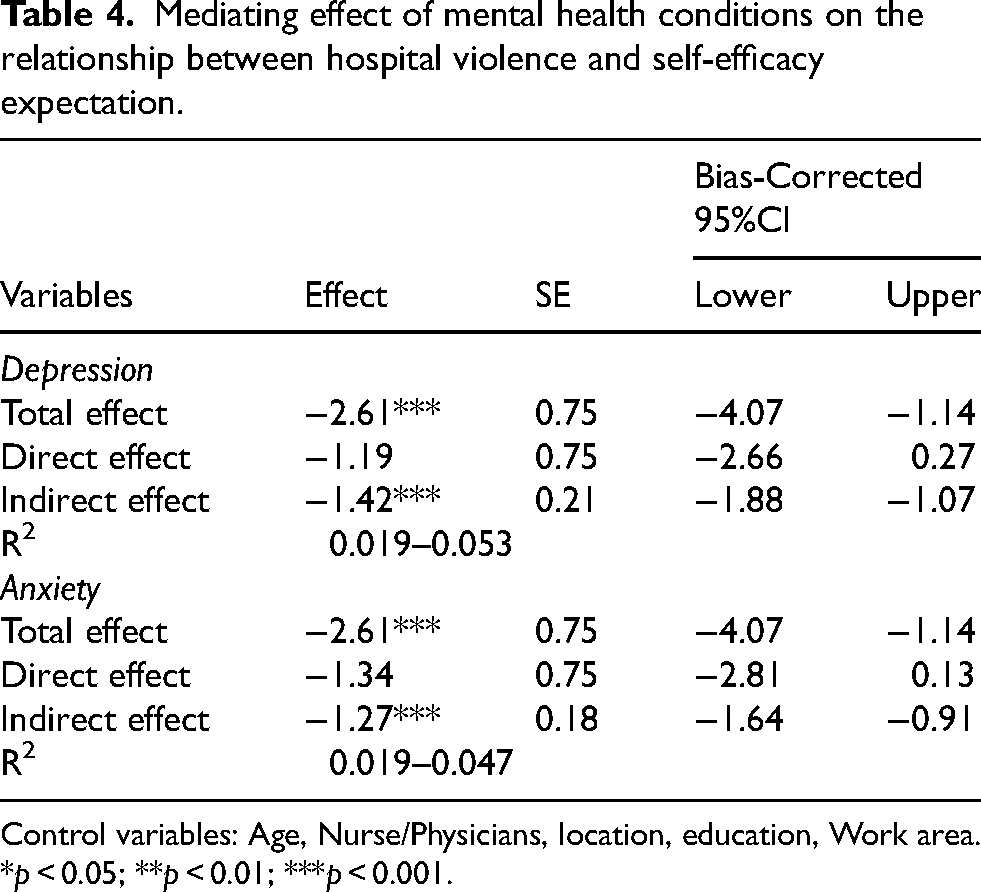
Control variables: Age, Nurse/Physicians, location, education, Work area.
*p < 0.05; **p < 0.01; ***p < 0.001.
Discussion
In recent years, protecting healthcare workers from hospital violence and associated psychological problems has become a global concern. 44 The present study found that both hospital violence and psychological distress were associated with lower self-efficacy expectations. This association remained statistically significant after controlling for demographic variables such as age and occupation in the regression models. These findings are partially consistent with previous research, which reported that hospital violence was associated with general self-efficacy among physicians in China. 13 Regardless of whether healthcare workers were directly involved in the treatment of COVID-19 patients, the association between hospital violence and self-efficacy expectations remained significant. However, this negative association was stronger among frontline healthcare workers, which is consistent with our hypothesis. It is important to note that, in this study, hospital violence refers to personal attacks experienced by healthcare workers, including verbal abuse, physical assault, and intimidation. These experiences may have occurred both before and during the pandemic. Two potential explanations may account for the stronger effect observed among front-line healthcare workers. First, for those who did not experience violence during the pandemic, prior exposure to hospital violence may have contributed to lower SEE. During the early stage of the pandemic, healthcare workers were frequently required to make critical life-and-death decisions under conditions of high uncertainty. This situation was often accompanied by concerns such as rapidly changing infection control procedures and fear of transmitting the virus to family members, 45 which may have reduced their psychological resources and confidence in managing clinical challenges. 46 In this context, prior experiences of hospital violence may further exacerbate the psychological burden among healthcare workers, potentially contributing to lower self-efficacy expectations. This effect may be particularly pronounced among healthcare workers involved in the treatment of COVID-19 patients. Following the outbreak, front-line healthcare workers were more likely to be exposed to hospital violence compared with their non-front-line counterparts. 47 Thus, this relationship may differ among frontline healthcare workers, as their exposure to hospital violence may reflect both pre-pandemic and pandemic-related experiences. In summary, both types of exposure were classified as experiences of hospital violence in this study. To our knowledge, this study is among the first to examine whether involvement in the care of COVID-19 patients moderates the relationship between hospital violence and self-efficacy. It also explores the potential social psychological mechanisms through which hospital violence may contribute to lower self-efficacy in a large sample of Chinese healthcare professionals. Enhancing self-efficacy expectation is an important goal of psychological interventions. 48
Similarly, mental health problems among healthcare workers warrant serious attention. More than two-thirds reported experiencing fear and burnout, while approximately one-third reported symptoms of depression, anxiety, and stress. 49 Depression and anxiety are common mental health problems among healthcare workers during the COVID-19 pandemic. 50 The present study found that both depression and anxiety were associated with hospital violence and SEE. These findings further support the mediation model, indicating that depressive and anxiety symptoms accounted for a substantial proportion of the total effect in the association between hospital violence and SEE. This finding suggests that poor mental health is associated with lower self-efficacy among healthcare professionals, which is consistent with previous evidence reported during the SARS outbreak 51 as well as more recent studies conducted during the COVID-19 pandemic. 52 Experiences of hospital violence may influence self-efficacy expectations through their impact on mental health. Notably, the mediating effect differed depending on whether healthcare workers were involved in the treatment of COVID-19 patients. Among those not directly involved in COVID-19 patient care, depression and anxiety appeared to play a dominant role, indicating a full mediation effect. In contrast, among frontline healthcare workers, mental health problems only partially mediated this relationship, suggesting that additional factors may be involved. Two possible explanations may account for this difference. First, it may be insufficient to focus solely on negative psychological responses arising from experiences of violence, as other emotional processes may also be activated. Second, positive psychological factors during the COVID-19 pandemic may have buffered the adverse effects of negative emotions. Previous studies have shown that healthcare workers may experience positive outcomes during the pandemic, including a renewed sense of purpose, solidarity, and shared mission. 53 These findings warrant further investigation and may provide useful insights for the development of targeted psychological interventions.
The COVID-19 pandemic can be viewed, from a social psychological perspective, as a powerful situational context. 54 The impact of hospital violence on self-efficacy expectations is not a simple “violent incident-decline in ability” process, but rather a psychological transformation embedded within a broader social context. When healthcare workers encounter or witness hospital violence, such experiences may undermine their perceptions of control over the work environment and trigger negative psychological responses, including fear, anxiety, anger, helplessness, and professional insecurity. These reactions may, in turn, diminish their confidence in managing clinical tasks, doctor-patient conflicts, and future risks. In this sense, hospital violence not only conveys the message that the work environment is unsafe, but also reshapes individuals’ perceptions of their own capabilities through emotional responses such as fear, anxiety, helplessness, humiliation, and emotional exhaustion. 55 The Conservation of Resources theory 56 posits that stress arises when individuals’ resources are threatened or depleted, and that sustained resource loss increases the risk of psychological distress and functional impairment. Self-efficacy can be conceptualized as a key personal resource within this framework. Successfully completing challenging tasks represents one of the most important sources of self-efficacy. In conclusion, these findings suggest that mental health services for healthcare professionals should be incorporated into intervention programs aimed at maintaining a resilient healthcare workforce during public health crises. Such interventions may need to be tailored according to whether healthcare workers are directly involved in the care of COVID-19 patients. Furthermore, promoting successful self-regulation strategies may help enhance self-efficacy expectations among healthcare workers.
This study also found that certain sociodemographic variables, including profession and educational attainment, were associated with self-efficacy expectations. Nurses reported higher SEE than physicians, which may be related to differences in job roles, responsibilities, and patient interactions. Interestingly, higher educational attainment was associated with lower SEE in this study. This finding contrasts with previous research suggesting that higher education is generally linked to greater self-efficacy. One possible explanation is that individuals with higher educational levels may have greater professional expectations and awareness of clinical uncertainties, which could lead to lower perceived self-efficacy under high-pressure conditions such as the COVID-19 pandemic. 57 Academic success increases individuals’ self-efficacy beliefs, 58 which may be reflected in higher self-efficacy expectations. However, individuals in clinical training years have been found to report lower self-efficacy than those in preclinical (didactic) years. This suggests a negative association between academic progression and self-efficacy. As exposure to clinical cases increases, self-efficacy may gradually decline. 59 Healthcare workers with higher levels of education may assume greater clinical responsibilities and be exposed to more complex and challenging cases, which may reduce their confidence in their ability to effectively address patients’ health problems. In contrast, no significant differences were observed for certain demographic variables, such as gender and age. However, age showed a significant association with self-efficacy expectations in the multivariate regression analysis, with higher SEE observed among older healthcare workers. Self-efficacy expectations reflect individuals’ beliefs about their capability to perform specific behaviors and achieve desired outcomes. 60 It may be that more highly educated healthcare professionals possess greater knowledge and are more aware of uncertainties in clinical practice.
Recent studies have reported that workplace violence has a stronger impact on self-efficacy among front-line nurses. 36 Factors contributing to hospital violence that are difficult to avoid include patient death, dissatisfaction with treatment outcomes, prolonged treatment duration, and overcrowding. 61 However, timely assessment and mental health interventions for frontline healthcare workers remain relatively limited. 62 The academic value of this study is further underscored when interpreted in the context of major policy and social changes between 2022 and 2026. Following the transition from dynamic zero-COVID measures to a normalized management phase in 2023, China's healthcare system underwent substantial adjustments in service delivery, workforce management, and public health strategies. 63 At the same time, post-pandemic studies suggest that healthcare workers continue to experience substantial psychological burdens, although the nature and intensity of stressors may have evolved. However, there remains limited understanding of the psychological impacts of medical work in the post-pandemic period in mainland China. 64 The present study should be interpreted as a cross-sectional investigation conducted during the early stage of the COVID-19 pandemic, which provides a historical baseline for understanding the relationship between hospital violence and self-efficacy expectations under crisis conditions.
The findings of this study suggest that targeted intervention programs may enhance self-efficacy expectations, which in turn can facilitate individuals’ efforts to achieve desired outcomes. 65 Training is an important strategy for enhancing healthcare workers’ self-efficacy. Its primary aim is to improve their ability to provide patient care. 66 Digital tools can be leveraged to deliver large-scale training efficiently across diverse healthcare populations, thereby enhancing healthcare workers’ confidence in managing patients with COVID-19. 67 The severe conditions of the COVID-19 pandemic may foster a strong sense of meaning among healthcare workers, such as heightened responsibility and professional commitment, which in turn may trigger positive psychological responses. 68 Training that enhances healthcare workers’ capacity to provide patient care may also strengthen their sense of professional pride and meaning derived from successful clinical outcomes. From an organizational perspective, healthcare institutions with clearly defined roles and responsibilities are associated with more effective infection control. This suggests that well-structured organizational systems may be an important condition for enhancing healthcare workers’ self-efficacy. 69 In conclusion, beyond routine measures such as reducing workplace violence and improving mental health, tailored strategies to enhance self-efficacy should be developed according to whether healthcare workers are directly involved in the care of COVID-19 patients. As a baseline investigation conducted during the early stage of the pandemic, this study provides valuable insights for addressing similar challenges in the post-pandemic period and future public health crises.
Limitations
As with many observational studies, several limitations should be considered when interpreting the findings and their generalizability. Firstly, this study employed a snowball sampling method, which has been shown to be effective for studying “hard-to-reach” populations. 70 During the early stage of the pandemic, when direct contact with front-line healthcare workers was not feasible, the use of snowball sampling provided a practical approach to reaching this specific population. However, this method may introduce selection bias and limit the representativeness of the sample. Participants recruited through professional networks may share similar characteristics, such as age and work experience, which could increase sample homogeneity. Although this study controlled for key demographic and occupational variables in the statistical analyses to reduce potential confounding effects, the non-random sampling strategy and relatively low response rate may still limit the generalizability of the findings to the broader population of healthcare professionals. Healthcare professionals who were more technologically engaged or more motivated to participate may have been overrepresented in the sample, which may limit the generalizability of the findings.
Secondly, this study primarily examines the associations among hospital violence, self-efficacy, and related psychological factors. The cross-sectional design prevents making causal inferences. In addition, as all measures were self-reported, response accuracy may be subject to bias. Although validated instruments were used to assess mental health and self-efficacy expectations, the single-item measure of hospital violence may introduce information bias in estimating its prevalence. Furthermore, the assessment of hospital violence relied on retrospective self-report over the past 12 months, which may be subject to recall bias. The use of an online survey may also introduce sampling bias, as participation is influenced by access to and engagement with digital platforms, potentially limiting the representativeness of the sample. Although participants’ residential regions were reported, the geographic distribution of healthcare institutions was not specifically assessed, and thus regional institutional differences could not be fully examined. Finally, this study primarily focused on the impact of hospital violence on healthcare workers’ functioning during public health emergencies. However, differences in the effects of various types of violence (e.g., psychiatric versus general healthcare settings), levels of severity (mild to severe), and timing (pre- versus post-pandemic) were not explored in depth and warrant further investigation in future research.
Conclusion
In this cross-sectional study conducted during the early stage of the COVID-19 pandemic, hospital violence was associated with lower self-efficacy expectations, partly mediated by depressive and anxiety symptoms, with different patterns observed between front-line and non-front-line health professionals. These findings highlight the need to strengthen institutional policies aimed at preventing hospital violence and to integrate mental health support and self-efficacy enhancement into occupational health systems. Greater attention should be given to frontline healthcare workers, particularly during public health crises. Interventions may include targeted training and organizational management strategies to enhance self-efficacy, as well as efforts to leverage positive psychological resources fostered during the pandemic, such as a sense of meaning and professional responsibility.
Supplemental Material
sj-doc-1-wor-10.1177_10519815261460408 - Supplemental material for The relationship between hospital violence and self-efficacy expectation among healthcare professionals during major public health events: The role of mental health and caring patients
Supplemental material, sj-doc-1-wor-10.1177_10519815261460408 for The relationship between hospital violence and self-efficacy expectation among healthcare professionals during major public health events: The role of mental health and caring patients by Lina Ha, Qingning Chang, Zihao Liu and Zhizhong Wang in WORK
Footnotes
Acknowledgements
The authors thank all the participants and researchers who were involved in this study.
Ethical approval
This study was conducted in accordance with the Declaration of Helsinki and received ethical approval from the Ningxia Medical University (approval #2020-112).
Informed consent
Participants were informed that their participation was voluntary and that they could withdraw from the study at any time without explanation.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Science and Technology Support Program of Guizhou province, CMB foundation project, (grant number [2020]4Y171, 16-254).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.