
Abstract
Background
Women living with multiple sclerosis (WwMS) often face significant employment challenges due to the intersection of gender roles, chronic illness, and workplace demands. These challenges can lead to social isolation, economic dependance, and reduced quality of life.
Objective
To explore the employment experiences, needs, and expectations of WwMS, focusing on structural and psychosocial factors influencing job retention.
Methods
A qualitative study using a descriptive phenomenological design was conducted. Semi-structured, in-person interviews were held with 20 WwMS who were actively employed. Data were analysed using Braun and Clarke's six-phase thematic analysis.
Results
Four major themes emerged: (1) Willingness to share the diagnosis, (2) Willingness to work to be involved in life, (3) Social isolation and social support, and (4) Expectations and suggestions from employers. Participants described stigma concerns, emphasized the role of employment in identity and self-worth, and highlighted the importance of both family and workplace support.
Conclusions
Employment is not only a financial necessity but also a psychological and social anchor for WwMS. Inclusive workplace practices, flexible conditions, and greater societal awareness are needed to support sustainable employment.
Keywords
Introduction
Multiple sclerosis (MS) is one of the most common causes of neurological disability during the most productive years of life and is a major contributor to unemployment. Symptoms such as physical disability, fatigue, cognitive dysfunction, and depression are frequently associated with challenges in working life.1,2 The impact of MS on employment significantly affects quality of life, leading to financial difficulties, social withdrawal, and emotional distress.3,4
Maintaining employment has been shown to positively influence health, well-being, and sense of identity in individuals with MS.5,6 However, for women living with MS (WwMS), employment can be even more challenging due to the intersection of gender roles, caregiving responsibilities, and health-related stigma.7,8 Women often face workplace discrimination, limited flexibility and inadequate institutional support, which can lead to early workforce withdrawal or underemployment.9,10
Despite these challenges, WwMS represent a skilled and experienced labor force. The social, psychological, and financial benefits of employment are particularly meaningful for this group. Understanding their lived experiences is therefore essential to identify the specific difficulties they face and the support systems that may enable their continued participation in working life.10,11
This study aimed to provide an in-depth exploration of the employment experiences and workplace perspectives of WwMS. The analysis focused on structural and personal challenges to sustaining employment, with particular attention to workplace conditions, social networks, and family support. Furthermore, the study examined the intersection of gender roles and social stigma, highlighting broader sociocultural dynamics that shape employment trajectories.
To better understand these issues, we drew on Goffman's Stigma Theory, which highlights how individuals with chronic or invisible illnesses may manage their identities in response to perceived social judgments.12,13 For WwMS, decisions about disclosure, workplace expectations and job retention occur within broader societal attitudes toward disability and gender.14,15 By framing the analysis within this conceptual approach, our aim was to interpret the women's experiences not only descriptively but also in relation to the structural and social factors that shape their working lives.
Methods
Research design
This study was designed using a descriptive phenomenological approach, guided by Husserlian principles. While Braun and Clarke's thematic analysis is not part of classical phenomenology, it is increasingly used within descriptive phenomenological research due to its flexibility and systematic structure. In this study, we integrated thematic analysis with a phenomenological stance by operationalizing phenomenological reduction through bracketing and reflexive journaling, which helped the research team set aside preconceptions arising from clinical roles. The thematic analysis steps then enabled the identification of recurring experiential patterns while remaining grounded in participants’ lived experiences, thereby maintaining alignment with Husserlian descriptive phenomenology.16,17
Population and sample characteristics
The population of this study consisted of 20 women diagnosed with MS who were followed up in the Demyelinating Diseases outpatient clinic of a university hospital in Turkey between June 2022 and September 2023. The study included adult WwMS who were 18 years or older, had an EDSS score of 3 or less, had no chronic diseases, and were currently employed. Participants were consecutively selected from WwMS who were followed by the same clinical team at the Demyelinating Diseases Outpatient Clinic and who expressed willingness to participate in the study.
Data saturation was monitored throughout the data collection process. After every three to four interviews, the coding framework was reviewed to assess whether new codes or themes were emerging. Saturation was considered to have been reached when the rate of new codes declined substantially, and no new themes were identified in the last three interviews. Additionally, the two coders agreed that additional interviews were unlikely to generate novel insights. This point was reached by the 18th–20th interviews, at which point thematic repetition became predominant. Accordingly, recruitment concluded at n = 20, consistent with established guidelines for saturation in qualitative research.18,19
Data collection tools
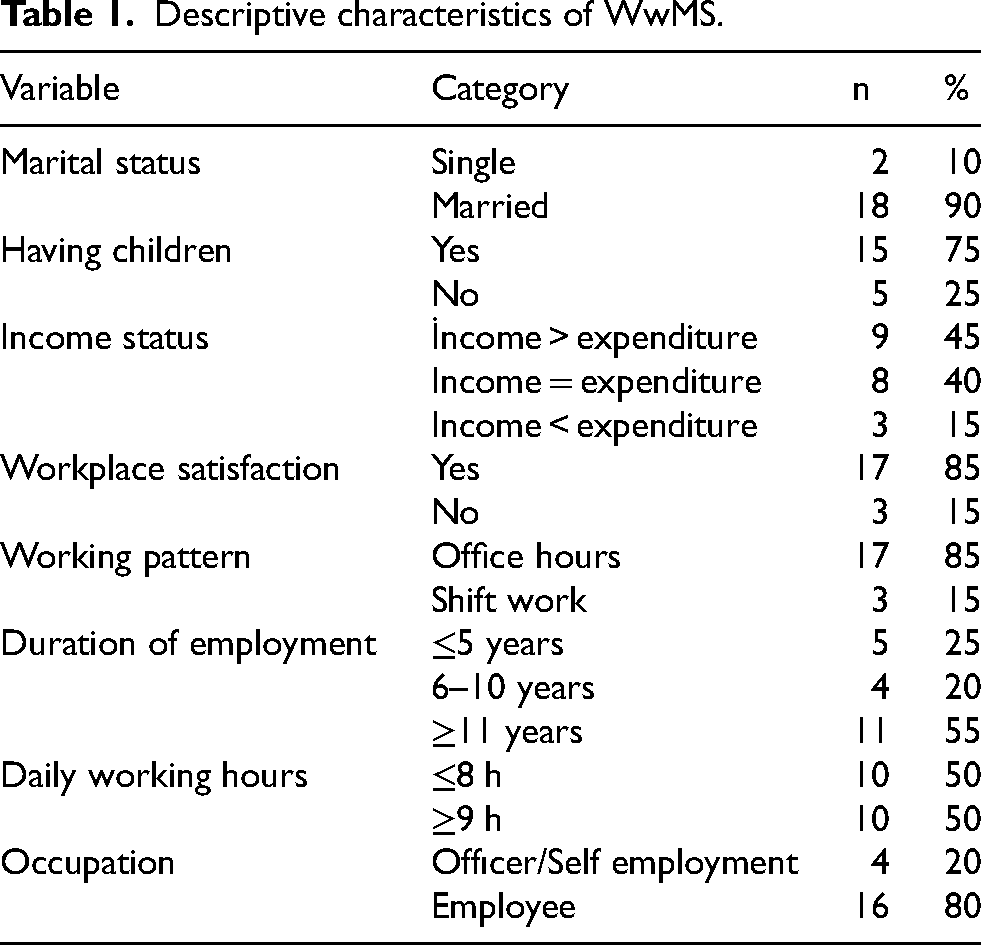
The research data were collected using a socio-demographic form and a semi-structured interview form developed by the researchers based on the relevant literature. The interview form included items assessing participants’ socio-demographic characteristics such as age, occupation, education level, income status, age at diagnosis of MS, working hours, and workplace satisfaction (Table 1). In addition, five open-ended questions were used to explore the participants’ experiences and perspectives regarding their employment (Table 2). To evaluate the comprehensibility of the questions, a pilot study was conducted with two WwMS. Subsequently, the questions were finalized based on feedback from two experts experienced in qualitative research to ensure the content validity of the interview form.
Descriptive characteristics of WwMS.
Open-ended questions and corresponding thematic categories.
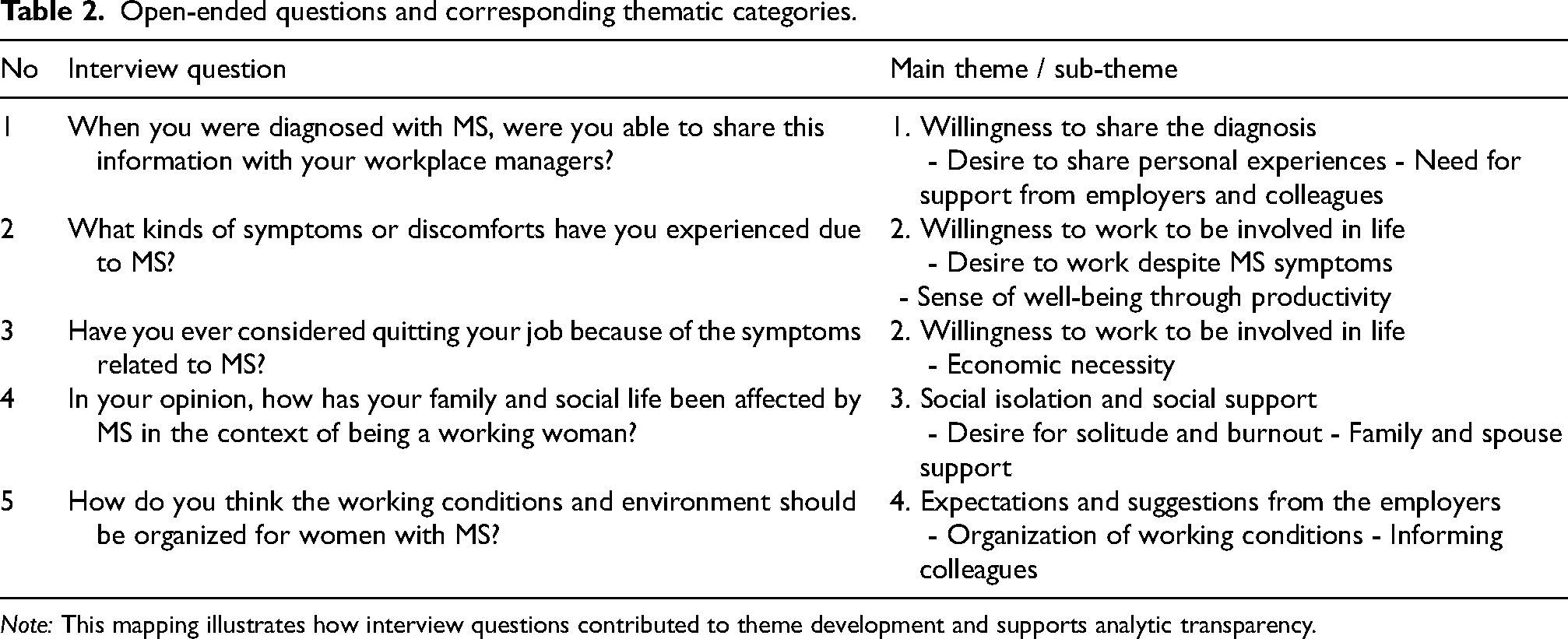
Note: This mapping illustrates how interview questions contributed to theme development and supports analytic transparency.
In this study, in-depth interviews were conducted by two members of the research team to explore the participants’ views on their work life. Before the interview, the participants were informed that the written and audio recording of the interview would depend entirely on the permission of the interviewee and their written consent was obtained. The interviews were conducted in person in the clinic's interview room, which was designed to create a suitable physical environment. The interview with each participant lasted approximately 30–40 min. Immediately after each interview, the notes were reviewed by all five members of the research team, and any missing data were confirmed with the participant.
Data evaluation
Data were analyzed using the six-phase thematic analysis method outlined by Braun and Clarke: (1) familiarization with the data, (2) generating initial codes, (3) searching for themes, (4) reviewing themes, (5) defining and naming themes, and (6) producing the report. During transcription, each participant was assigned a numerical code (e.g., Participant 1, Participant 2) to ensure confidentiality and anonymity. All personally identifiable information was removed from the transcripts. All transcripts were manually coded by two researchers working independently. An initial set of codes was generated after the first few interviews, and the codebook was refined iteratively as additional data were incorporated.
The research team consisted of clinician-researchers with backgrounds in neurology and nursing, and some members had prior clinical relationships with participants. We recognized that these relationships could affect participants’ openness and introduce power asymmetry or socially desirable responses. To minimize these influences, interviewers engaged in systematic reflexive practices, including bracketing exercises, reflexive journaling before and after interviews, and memo-writing to document emerging assumptions. Additionally, an independent researcher reviewed the coding framework and thematic interpretations to reduce potential bias. During the analysis, dual coding and consensus meetings were used to challenge individual interpretations and enhance confirmability. Although formal member-checking was not conducted due to participants’ clinical schedules, reflexive discussions were maintained throughout the analytic process. Participants were reminded of their right to decline or withdraw at any time, and all quotations were anonymized to ensure confidentiality. These combined strategies aimed to strengthen reflexivity and reduce the influence of researcher–participant relationships on the findings.
Data organization and storage were managed using Microsoft Excel. No qualitative analysis software was employed. Formal inter-coder reliability statistics (e.g., Cohen's kappa) were not calculated. Credibility was supported through consensus coding, thick description, and adherence to Lincoln and Guba's trustworthiness criteria (credibility, transferability, dependability, and confirmability). 20
Quotations were selected to demonstrate the range of experiences among participants. Although some individuals provided longer, more detailed narratives and appear more frequently, efforts were made to include diverse voices in each theme. The number of quotations attributed to a given participant does not indicate analytic weighting but rather reflects variation in narrative richness. This approach ensured that the thematic findings were grounded in multiple perspectives across the sample. Quotations are attributed with a unique participant ID and age (e.g., Participant 5, age 38). Other socio-demographic details are reported in aggregate form in Table 1, and were not repeated in the quotations to avoid inconsistencies.
Results
The mean age was 36.7 ± 6.55 years (range: 26–51), mean years of education were 11.1 ± 4.63 (range: 8–16), and the mean age at diagnosis was 29.7 ± 7.86 years (range: 16–50). The average EDSS score was 1.15 ± 0.93 (range: 0–3), and the mean duration since diagnosis was 12.3 ± 7.04 years (range: 1–25). The majority of participants were married (90%) and had children (75%). Nearly half reported income exceeding expenditures. Most participants were satisfied with their workplace and worked standard office hours (85%). Over half had ≥11 years of employment experience, half worked ≤8 h daily, and most were employes (80%). Additional descriptive characteristics are presented in Table 1. The main themes and corresponding sub-themes related to employment experiences are summarized in Table 2.
To enrich the interpretation of the qualitative data, the open-ended interview questions were mapped onto the main and sub-themes that emerged from the thematic analysis. This approach facilitated a clearer understanding of how participants’ narratives aligned with the conceptual framework of the study. Table 2 shows how each question contributed to identifying specific themes, such as willingness to disclose the diagnosis, motivation to remain employed, experiences of social support or isolation, and expectations of employers. This structure not only improved analytic transparency but also enhanced the trustworthiness of the findings.
Most participants felt a strong need to share their diagnosis with supervisors or colleagues. Many hesitated due to fears of job loss, judgment, or lack of understanding. Workplace culture and past experiences strongly shaped disclosure, and lack of institutional protection sometimes led to precarious employment.
Desire to share personal experiences
All participants reported feeling a need to share their diagnosis with supervisors and colleagues. However, many expressed hesitations due to fears stemming from their symptoms, potential job loss, and anticipated negative attitudes. “I own my own business. I share it with my husband and colleagues. The first symptom appeared in my eye. People didn't believe me, so they tied a potato to my eye. Later, I saw a neurologist who diagnosed me. My job involves calculations. After the diagnosis, I feared making mistakes.” (Participant 1, age 41) “I disclosed my diagnosis to my supervisors at work. When I was first diagnosed, I was afraid I would be fired.” (Participant 3, age 30) “I tried not to share my diagnosis because I feared being judged by my colleagues.” (Participant 11, age 36)
Need for support from employers and colleagues
Nearly all participants (n = 18) reported not receiving the expected support after disclosing their diagnosis. One participant noted she had to work without insurance because her employer refused responsibility. Only two participants reported receiving adequate support. “I was afraid they wouldn’t hire me, but I needed to disclose my symptoms. When I did, they said, ‘You can't work here. We can't be responsible for your attacks and fatigue.’ They made me work without insurance.” (Participant 5, age 38) “When I was diagnosed, I was working as a nursery schoolteacher. When I told the headmistress, she said, ‘You can’t take leave; there is no one to replace you.’ I expected support from my colleagues. I received cortisone treatment outside of work hours and went to work afterward.” (Participant 18, age 49) “I’m a teacher. We take turns being on-call supervisors during the day. During the first year after my diagnosis, I had no expectations. Later, I requested to have no duties, and my request was granted. I also requested reduced hours, which was granted. I didn't have any issues with the administration or my colleagues.” (Participant 7, age 32)
Participants continued working despite MS symptoms, driven by identity, purpose, and financial needs. Gendered roles reinforced their commitment. Family, colleague support, and workplace adaptations facilitated employment, while anticipated stigma shaped disclosure decisions and access to accommodations. These findings highlight the interplay of personal, social, and organizational factors in the employment experiences of women with MS.
Desire to work despite MS symptoms
Fatigue was the most frequently reported symptom affecting participants’ working lives. Other symptoms included numbness, weakness, joint pain, dizziness, and balance issues. Participants reported strict adherence to treatment to remain active in life. “After my first and only attack, I lost strength in my feet and had difficulty writing for about nine months. I followed my physician's recommendations, biked, walked regularly, and used coloring techniques to strengthen my grip.” (Participant 9, age 33) “I had leg weakness and temporary blindness, which improved with cortisone. I also experienced double vision that resolved after treatment.” (Participant 18, age 49) “I have fatigue, weakness, muscle cramps, and balance disorders. I work around machines and often lose balance. I seek help from colleagues.” (Participant 20, age 51) “I suffer from attention deficit, fatigue, and joint pain. I can't stand long. My supervisor allows intermittent rest.” (Participant 6, age 38) “The hardest part is arm weakness. I try to avoid using it too much.” (Participant 8, age 32)
Sense of well-being through productivity
Despite experiencing symptoms, participants described working as beneficial to their well-being and a reason to continue. “I made an effort despite dizziness and vision problems. I never considered quitting. Being useful and productive feels good. Work stimulates my brain.” (Participant 18, age 49) “Even though it is tiring, I feel confident knowing I am doing something.” (Participant 16, age 40) “I initially considered quitting due to uncertainty about disease progression. Later, I felt work would prevent me from being stuck in illness-related patterns.” (Participant 11, age 36)
Economic necessity
Most participants (80%) said they had to work to meet essential needs. Married participants emphasized the necessity of contributing financially to their households and supporting their children. “I thought about quitting. I requested changes to my working hours, but nothing changed. My physician is adjusting my shifts. I don't want overtime; I’m too tired. Early retirement would be ideal. I have to work for financial reasons.” (Participant 20, age 51) “Yes, I considered retirement when I had leg weakness. But I’m glad I didn’t quit. I couldn’t have supported my children's needs otherwise.” (Participant 12, age 39) “Although my income is essential for my family, fatigue makes daily work very challenging.” (Participant 4, age 30)
MS symptoms, work, and family duties sometimes led to isolation and burnout. Emotional and practical support from family or colleagues buffered these challenges.
Desire for solitude and burnout
More than half the participants (n = 13) reported occasional desire for solitude and feelings of exhaustion due to symptoms. “Stress and fear managed at work surface unexpectedly at home. I shut down and avoid people.” (Participant 17, age 44) “I get very tired at work and lose motivation for anything else.” (Participant 14, age 30) “Work drains me. I come home exhausted.” (Participant 19, age 32) “After a long day at work, I feel completely drained and just want to be alone for a while.” (Participant 8, age 32)
Family and spousal support
More than half (n = 12) stated that work negatively impacted their family and social life due to fatigue. Those who received support with domestic duties found it easier to cope. “It didn’t affect me much, my mother cares for my child. My husband helped a lot during my leg issues.” (Participant 13, age 39) “I’m extremely tired. My husband drives me home from work. Sometimes, I even forget I’m hungry.” (Participant 20, age 51) “Even my husband doesn’t believe I’m tired. I need his and my family's help with childcare and housework.” (Participant 2, age 41)
Participants expected workplace adaptations such as flexible hours, remote work, manageable workloads, and rest breaks, but these were often unavailable, highlighting the need for employer and coworker MS awareness.
Organization of working conditions
Participants recommended regulating workplace environments (e.g., temperature, workload) to suit individual health needs. Suggestions included flexible hours, no shift work, and reduced weekend obligations. “MS is not well known. Awareness should come first. Reduce working hours and include rest breaks. Avoid weekend work to allow social time.” (Participant 15, age 26) “More remote and flexible working opportunities should be created.” (Participant 1, age 41) “The length of working hours in shift-based employment should be reduced.” (Participant 4, age 30) “Employers should control workplace temperature and assign MS patients to low-stress environments.” (Participant 10, age 33)
Informing colleagues
All participants advocated for MS education among staff to promote understanding and support. “Employees should be informed briefly and simply about the condition.” (Participant 16, age 40) “Colleagues should be informed and encouraged to support us.” (Participant 12, age 39) “It would help if all staff received basic training about MS so they can be more understanding.” (Participant 13, age 39) “If staff knew more about MS, they would understand our challenges better.” (Participant 10, age 33).
Anticipated stigma strongly influenced disclosure decisions across cases. Non-disclosure limited access to workplace accommodations, intensifying fatigue and social isolation. Conversely, support from family and colleagues buffered these burdens and enabled women to maintain their employment. Employer practices, such as flexible hours, adjusted workloads, and environmental adaptations, acted as distal levers that either mitigated or exacerbated these dynamics. Together, these four themes reveal a pathway from stigma and disclosure decisions to support and accommodations that lead to sustained participation in the workforce.
Discussion
This study explored the employment experiences of WwMS using a descriptive phenomenological approach. Our findings revealed four core themes: the challenges and hesitations surrounding diagnosis disclosure, the drive to remain employed despite physical and emotional strain, the interplay between social isolation and support, and concrete expectations from employers. These experiences highlight how gender, chronic illness, and workplace dynamics intersect in shaping employment outcomes for WwMS.
The fear of stigma emerged as a key barrier to disclosure, consistent with Goffman's Stigma Theory. 21 These concerns reflect the anticipated stigma commonly experienced by individuals with chronic, invisible illnesses. Drawing on Goffman's Stigma Theory, participants’ reluctance to disclose illustrates the tension between “passing” as healthy and being authentic in their identity.12,13 This finding aligns with evidence that employes with invisible disabilities often choose non-disclosure as a coping strategy.22,23,24 More recently, Railton et al. reported similar disclosure hesitations among WwMS in the UK, indicating that this remains a cross-cultural challenge across healthcare and workplace systems. 10 These patterns show that concealment is both a personal coping strategy and a reaction to organizational climates lacking adequate protection. Importantly, Stigma Theory functioned in this study as a sensitizing framework rather than a deterministically applied model; we initially identified it as relevant during study design, but its explanatory power became clearer as themes of anticipated stigma and concealment emerged. Our findings therefore extend the theory by illustrating how stigma is reinforced not only through interpersonal interactions but also through structural vulnerabilities, such as lack of formal protections and irregular employment conditions. The findings suggest that fear of discrimination often leads individuals with MS to conceal their condition, even when this compromises their health or well-being. These dynamics highlight the need for proactive employer education and inclusive workplace policies to ensure safe and supported disclosure.
Despite their health challenges, participants demonstrated strong agency in choosing to stay employed. For many, work represented more than financial necessity—it was a source of identity, purpose, and social integration. This aligns with Rumrill et al., who found that employment supports quality of life and self-identity in people with MS. 3 Our results extend this by illustrating how gendered roles intensify the determination to remain employed, even when work exacerbates fatigue or cognitive strain. The resilience observed in our sample echoes Social Role Theory, 25 where societal expectations around caregiving and economic participation intersect to shape women's decisions. In line with Social Role Theory, our findings demonstrate that women internalize not only traditional caregiving expectations but also the responsibility to sustain household income, which amplifies their commitment to remain employed despite health-related barriers. While these theoretical lenses were identified a priori, their relevance was reinforced through the emergent themes, indicating a reciprocal relationship between empirical findings and theoretical interpretation.
The role of support systems was particularly salient. Participants who received emotional or instrumental support from spouses, family members, or colleagues reported better capacity to manage the demands of work. This finding resonates with Román et al., which demonstrated that social support mitigates work-related difficulties and sustains employment among persons with MS. 2 Together, these results reinforce stress-buffering models, highlighting how supportive networks moderate the negative effects of chronic illness on working life. 26 In contrast, women lacking such networks expressed heightened vulnerability to isolation and burnout, further emphasizing the inequities in access to support.
Differences observed by income, education, and occupation echo the findings of Dobson et al., who emphasized the importance of social determinants in shaping MS-related health and employment outcomes. 9 Our results further illustrate how these structural factors intersect with gendered expectations, influencing disclosure decisions and access to accommodations. In this way, socioeconomic position and gender roles jointly shape employment trajectories for WwMS.
Participants clearly and consistently voiced a need for more inclusive work environments. They believed increased awareness would foster empathy, reduce stigma, and improve workplace inclusion. This aligns with disability-inclusive workplace models, which emphasize both structural adjustments and organizational culture change. 27 Participants’ voices underscore that meaningful inclusion requires more than policy—it demands proactive communication, supervisor training, and valuing diverse abilities. Without such changes, even women with mild disability may struggle to maintain employment. Their suggestions, which included flexible scheduling, teleworking, workload adjustments, and disability awareness training, reflected both practical concerns and deeper aspirations for equity. These findings align with international recommendations for reasonable accommodations.27,28 However, our data indicate inconsistent implementation, particularly in the private sector, reflecting the policy–practice gap noted by Vitturi et al.. 15 To enhance the practical relevance of these findings, employer recommendations can be conceptualized at multiple levels. Short-term, feasible adjustments include scheduled rest breaks, temperature regulation, ergonomic modifications, and redistribution of physically demanding tasks. Intermediate strategies involve supervisor training on MS-related symptoms, structured communication protocols for discussing health needs, and routine workplace assessments to identify environmental stressors. Long-term structural changes may include integrating disability inclusion into organizational policies, aligning workplace practices with International Labor Organization (ILO) and Convention on the Rights of Persons with Disabilities (CRPD) standards, and establishing monitoring mechanisms to ensure compliance across sectors.27,28 Evidence from broader chronic illness and disability research supports the relevance of these recommendations. Wong et al. showed that accommodations such as flexible hours, task modification, and ergonomic supports improve both return-to-work outcomes and job retention among people with physical disabilities. 29 Likewise, Varekamp and van Dijk found that employes with chronic diseases benefit from workload adjustments, flexible scheduling, and supportive supervision. 30 These findings indicate that the accommodations identified in our study are consistent with evidence-based strategies that enhance employment sustainability across chronic illness contexts.
One of the key contributions of this study is its emphasis on lived experience and contextualized, gender-sensitive insight. While previous studies have quantified employment rates and general barriers for people with MS,31,32 our findings underscore the nuanced realities of women navigating chronic illness within work cultures often ill-equipped to respond to their needs. Work was not simply a matter of functionality, but an arena where identity, visibility, and value were continuously negotiated. The invisibility of MS symptoms contributes to a culture of silence, where disclosure is simultaneously risky and necessary. This silent tension, characterized by the difficult choice between concealing one's condition for self-protection and disclosing it to gain support, highlights the complex dynamics of self-presentation in chronic illness contexts. 33 Moreover, the emotional labor involved in appearing healthy despite symptoms can intensify psychological strain.
These findings emphasize the need for culturally competent and empathetic organizational environments that acknowledge and address the nuanced realities of living and working with an invisible illness. To improve employment outcomes for WwMS, a systemic shift is required. Legal protections must be supported by proactive organizational practices: education of managers and coworkers, inclusive human resources policies, and accessible workplace designs. Public awareness campaigns and leadership training on disability inclusion can help shift workplace cultures from tolerance to genuine inclusion. Employment must be reframed not merely as a medical feasibility, but as a social right underpinned by dignity, accessibility, and recognition of difference. Our findings reinforce that sustainable employment outcomes depend on both micro-level interactions and macro-level policy commitments, highlighting the need for integrated approaches that bridge theoretical understanding, lived experience, and practical implementation.
This study has several limitations. The sample was geographically restricted and recruited through a physician–patient network, which may have introduced volunteer bias and reduced the diversity of perspectives. In addition, most participants worked regular office hours, with limited representation from shift-based or physically demanding occupations, which constrains the transferability of findings across different work environments. Women with higher disability levels (EDSS > 3) or those who had already left the workforce were excluded, limiting insights into the experiences of individuals with moderate-to-severe disability or employment loss. Although participants’ socio-demographic characteristics such as age, education, income, job satisfaction, and working hours were collected, these variables were not systematically analyzed. Furthermore, as a qualitative study, the findings reflect participants’ subjective experiences rather than objective measures. Future research supported by larger, occupationally diverse samples and complemented by quantitative approaches is needed to more comprehensively evaluate the factors influencing employment among WwMS.
Conclusion
This study shows that employment is not only a financial necessity but also a vital source of identity, resilience, and social participation for WwMS. Our findings show how stigma, gender roles and socioeconomic factors shape disclosure, support and job retention, adding a gender-sensitive perspective. Practically, the results point to clear priorities: flexible scheduling, reasonable workloads, environmental adjustments, and MS-specific awareness training for supervisors and colleagues, supported by stronger policy enforcement against discrimination. Sustainable employment for WwMS requires both individual determination and systemic commitment from employers and policy makers to foster inclusive and equitable workplaces.
Footnotes
Acknowledgements
We would like to thank all participants.
Ethical approval
The study was approved by Tekirdağ Namık Kemal University, Clinical Research Ethics Committee with reference number 2022.70.04.20.
Informed consent
Informed consent was obtained from all participants.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.