
Abstract
Background
The COVID-19 pandemic has affected the physical and mental health of Brazilian workers, especially those who have started working in home offices. Changes in the workplace, increased physical inactivity, and fear of contracting the disease, known as coronaphobia, may be related to increased musculoskeletal pain (MSP).
Objective
To analyze the prevalence of MSP and coronaphobia in home-office workers during the COVID-19 pandemic and to evaluate the relationships between these variables.
Methods
A cross-sectional, observational, and descriptive study with 736 participants was conducted through an online questionnaire. Data on sociodemographic characteristics, working conditions, and pain were collected, along with the evaluation of coronaphobia using the COVID-19 Phobia Scale (C19P-S) and MSP using the Nordic Questionnaire of Osteomuscular Symptoms (NMQ).
Results
Most participants were female (78%), with an average age of 32.8 (SD = 10.7 years). During the pandemic, 71% reported some osteomuscular symptoms, and of these, 64% developed new symptoms of pain during the pandemic, with a higher incidence in the lower back and neck. Participants who began home-office work presented a higher incidence of pain, and among them, 53% reported that their furniture was not suitable for working at home. Most had little fear of COVID-19, but moderate levels of coronaphobia increased the likelihood of MSP (PR = 1.74; 95% CI). Coronaphobia and MSP were significantly associated.
Conclusions
The prevalence of MSP increased after the pandemic, especially among those who worked from home, primarily affecting the lumbar and cervical regions. Coronaphobia was also associated, with a higher probability of pain in individuals with moderate or high fear.
Introduction
The SARS-CoV-2 virus, named COVID-19 by the World Health Organization (WHO), was discovered at the end of December 2019 in Wuhan, China. On March 11, 2020, the WHO declared a pandemic due to the uncontrolled spread of the virus worldwide. 1 Since its discovery, COVID-19 has affected more than 119 million people globally, with over 2 million confirmed deaths, 2 significantly impacting public health and the economies of several countries. In addition to direct health consequences, the pandemic has also triggered various side effects, such as the emergence of new psychological conditions and the worsening of preexisting ones.
Preventive measures such as social isolation, hand and food hygiene, and mask use were necessary to reduce transmission. 3 In Brazil, in March 2020, a quarantine bill was approved, 4 which defined the isolation of healthy individuals and those in the incubation period of the disease, i.e., individuals with symptoms or testing positive for COVID-19. This physical distancing allowed better control and reduced contamination rates. 5 At that time, there was no definitive treatment, and vaccines began to be administered only as a control measure in January 2021.
Home isolation was one of the strategies adopted to control COVID-19 transmission, serving as an effective way to prevent exposure to infection and reduce fatality rates. 6 This strategy, whether voluntary or mandatory, although effective, could also lead to physical inactivity, weight gain, behavioral dependance, and social isolation. 7 Previous studies have indicated that prolonged isolation could be associated with psychological disorders, 7 sleep disturbances, 8 severe phobias,9,10 musculoskeletal conditions and pain, 11 with the latter exacerbated by physical inactivity. 12 Due to the social isolation imposed by the pandemic, many individuals were compelled to work from home and adopt a home-office regimen. 13
Studies on the prevalence of musculoskeletal pain (MSP) during the pandemic remain scarce, particularly among individuals who transitioned to working from home. Similarly, few studies have assessed the phobias acquired during the pandemic, especially coronavirus-related phobia, known as coronaphobia, 10 which is defined as the excessive and irrational fear of contracting COVID-19. This condition has been widely observed in the general population and has led to significant increases in anxiety, stress, and other psychological disorders. 14 Coronaphobia can trigger several physical responses, including increased muscle tension and musculoskeletal pain. 11
The relationship between coronaphobia and MSP can be explained by the impact of chronic stress on the human body. 11 The constant fear of contracting COVID-19 and concerns about its consequences may lead to prolonged muscle tension, which in turn contributes to the development of MSP, particularly in areas such as the neck, shoulders, and back. 13
This situation is particularly relevant for workers who adopted a home-office routine during the pandemic. The sudden shift to remote work, often without adequate preparation of the home environment, resulted in ergonomically inadequate conditions for many workers. Moreover, the combination of emotional stress caused by coronaphobia and the lack of a proper work environment increased the incidence of MSP among this population.15,16
Therefore, the aim of this study is to analyze the prevalence of MSP and coronaphobia in home-office workers during the COVID-19 pandemic and to evaluate the relationship between these variables. Understanding these factors is essential for developing more effective intervention strategies to mitigate these negative effects and promote workers’ health and well-being during public health crises.
Methods
This was a cross-sectional, observational, and descriptive study approved by the Research Ethics Committee of Universidade Paulista/UNIP (Protocol: 46136621.3.0000.5512). The study was based on data collected through an online questionnaire addressing perceived changes in workers’ routines before the pandemic, when they worked in a typical environment, and after isolation, when most transitioned to working from home.
The questionnaire was created using Google Forms and remained open for three months or until a minimum of 700 responses was reached, following the study by Celenay et al. 11 Data collection lasted 3 months and 24 days.
The questionnaire was self-administered, completed by participants without assistance, and disseminated through social media (Facebook® and Instagram®), messaging apps (WhatsApp®), and email.
The sample consisted of individuals who voluntarily completed the questionnaire after agreeing to data collection and providing informed consent (ICF). Responses considered valid were from employed individuals of both sexes, aged 18 years or older. Incomplete or inconsistent questionnaires were excluded.
The variables studied included age, sex, height, weight, marital status, education, occupation/profession, presence of chronic disease or health risk factors, regular physical activity before and during the pandemic, workplace during the pandemic, presence of pain before and during the pandemic, pain location and characteristics, and features related to coronaphobia.
For MSP, the Nordic Musculoskeletal Questionnaire (NMQ) was used, which assesses symptoms in nine body regions: neck, upper back, lower back, shoulders, elbows, wrists/hands, hips/thighs, knees, and ankles/feet. 17 MSP was determined if the participant presented with one or more pain sites, and the last question of the NMQ questionnaire (pain in the last week) was considered to assess pain prevalence.
Coronaphobia was assessed using the COVID-19 Phobia Scale (C19P-S), developed by Arpaci et al. 14 and adapted for Brazil by Faro et al. 18 The scale consists of seven questions rated on a 5-point scale, ranging from “strongly disagree (1)” to “strongly agree (5).” Higher scores indicate greater coronaphobia and fear of the disease. The total score ranges from 7 to 35 points. For analysis, scores were stratified into three categories of approximately 33.3% each: 7–19 points = “low fear,” 20–26 points = “moderate fear,” and ≥27 points = “high fear”. 14
Statistical analysis was performed using R software version 4.0 for Mac iOS. Descriptive statistics were used to calculate means and standard deviations for quantitative variables, and absolute numbers and percentages for categorical variables. The Shapiro-Wilk test was used to assess data normality; since the data did not meet the assumption of normality, group comparisons were performed using Mann‒Whitney tests. Associations between categories and groups were analyzed using Pearson's chi-square test and Fisher's exact test. Prevalence ratios (PRs) with 95% confidence intervals (CIs) were calculated using Poisson regression models with robust variance, assuming an alpha level of 0.05. MSP (from the NMQ) was used as the dependent variable. The independent variables included demographic characteristics (sex and age), obesity, and physical activity. Poisson regression models began with a parsimonious model (dependent variable + one independent variable), followed by an adjusted model including participant characteristics (sex and age). Model fit was evaluated using the Akaike Information Criterion (AIC), while the significance of associated factors (obesity and physical activity) was determined at p < 0.05. To investigate the association between the number of painful body regions and coronophobia levels, a Poisson regression model was performed. To facilitate clinical interpretation, results were expressed as Average Marginal Effects (AME). The AME represents the average absolute change in the number of painful body regions associated with each level of fear, calculated on the response scale. The model fit was assessed using the AIC, and statistical significance was set at.
Results
A total of 1053 individuals responded to the questionnaire. However, 317 respondents were excluded (75 for not meeting the age eligibility criteria and 242 for being unemployed at the time of completion) (Figure 1).
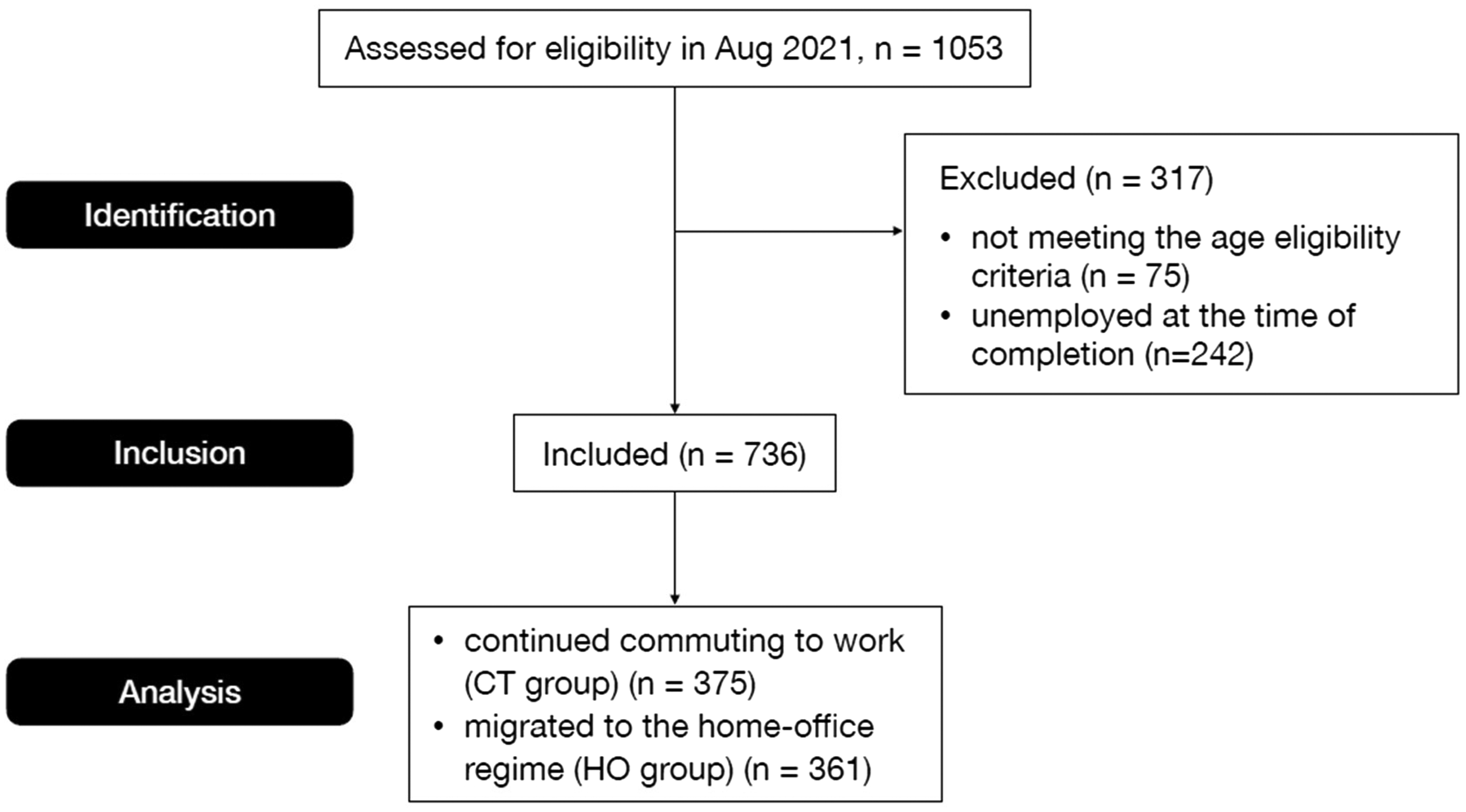
Flow diagram of participant recruitment.
The final sample consisted of 736 participants, the majority of whom were female (78%), with a mean age of 32.8 (SD = 10.7 years). More than half were single (57%) and had completed high school. Table 1 presents the sociodemographic characteristics of the participants according to their workplace during the pandemic.
Sociodemographic characteristics of participants in the CT and HO groups.
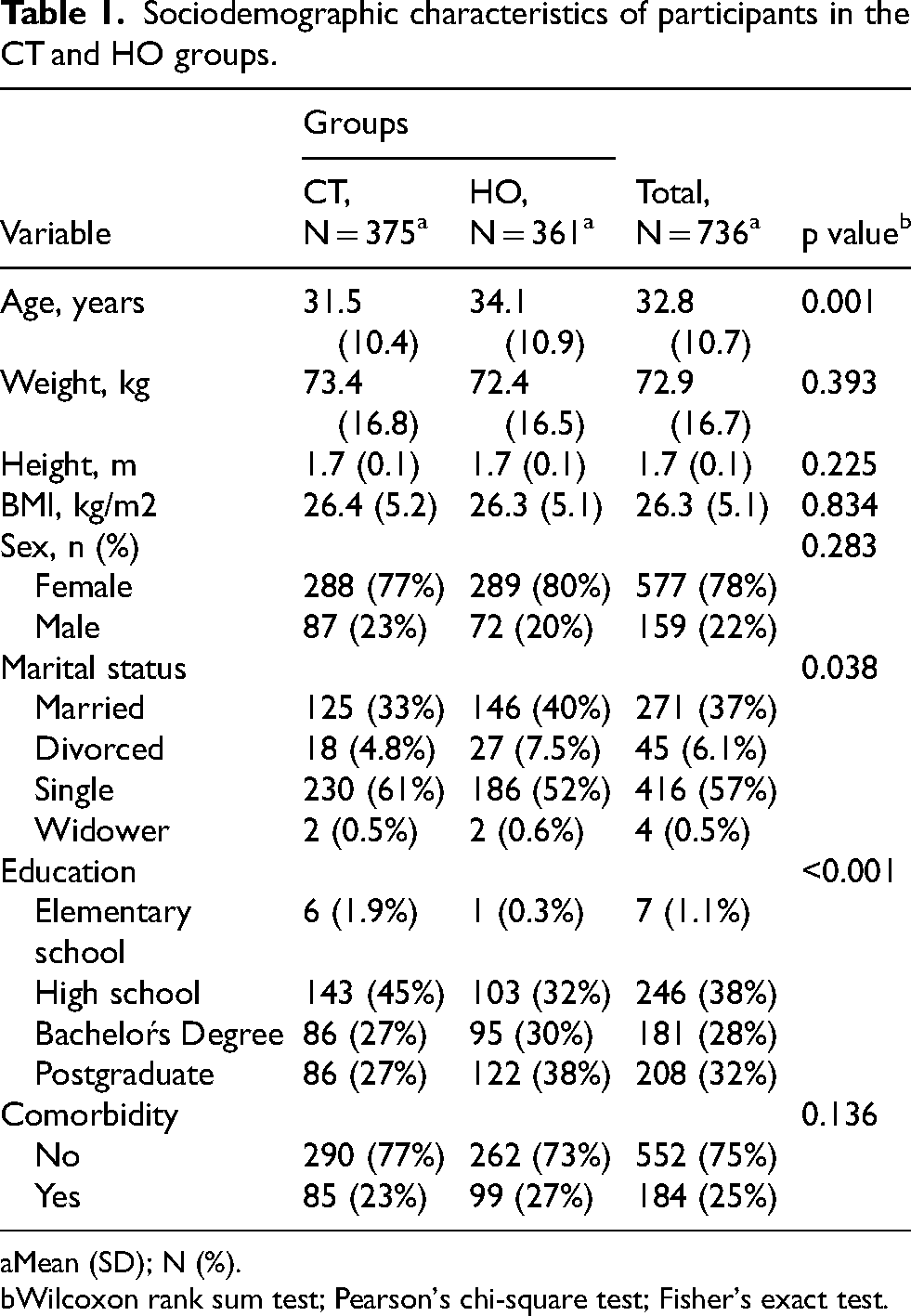
Mean (SD); N (%).
Wilcoxon rank sum test; Pearson's chi-square test; Fisher's exact test.
Overall, participants who transitioned to a home office (HO group) were significantly older (p = 0.001) than those who continued commuting to work (CT group). The groups also differed in marital status (p = 0.038) and educational level (p < 0.001).
During the pandemic, 71% of participants reported musculoskeletal symptoms, and among these, 64% developed new pain conditions during this period. Participants in the HO group showed a higher incidence of pain compared to the CT group (Table 2).
Pain before and during the COVID-19 lockdown in the CT and HO groups.
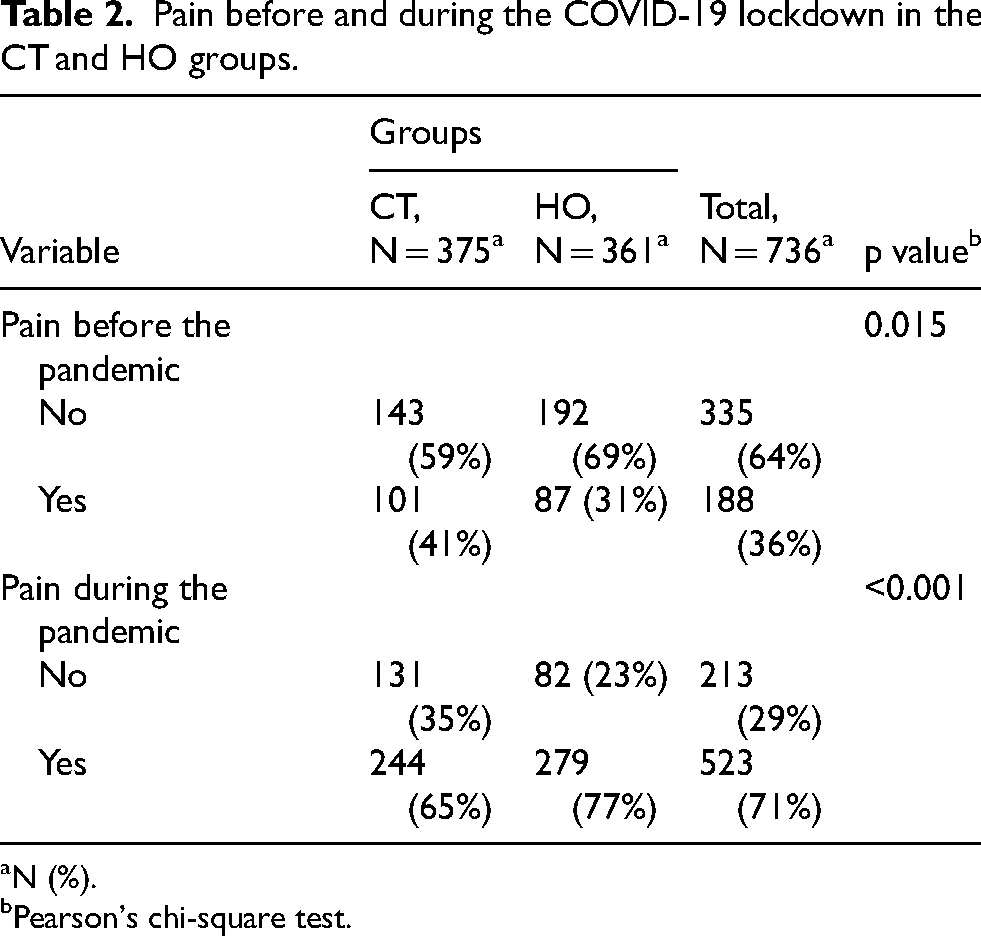
N (%).
Pearson's chi-square test.
The regions most frequently affected during lockdown were the lower back and neck, whereas the least affected region was the elbows (Figure 2). HO participants reported more elbow pain (17.9% vs. 10.7%, p = 0.019) and wrist pain (35.5% vs. 27.0%, p = 0.038) than CT participants. Conversely, compared with HO participants, CT participants reported more ankle pain (26.6% vs. 15.1%, p = 0.001) (Figure 2).
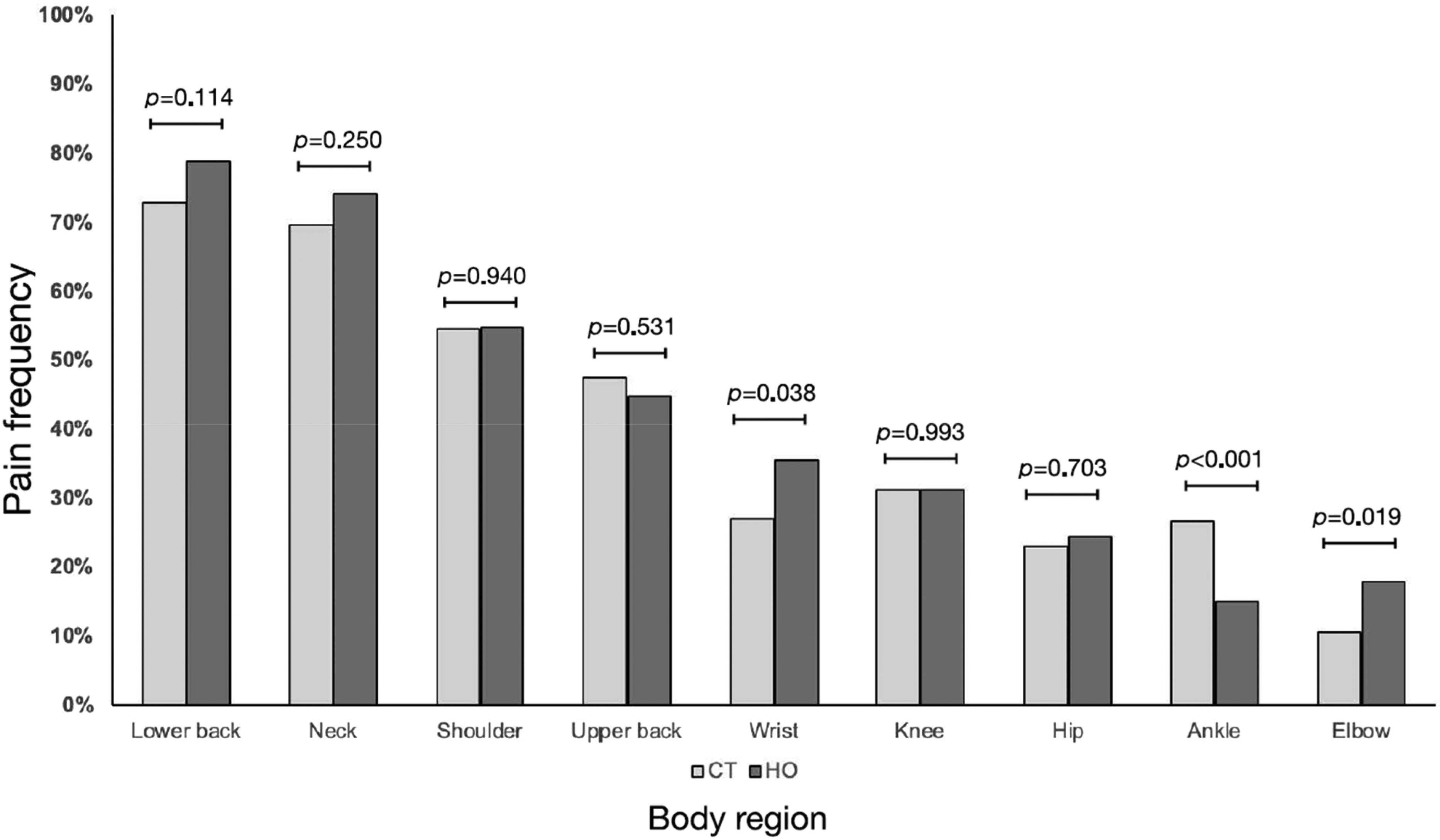
Pain frequency in the CT and HO groups by body region.
Among the 361 HO participants, 53% reported inadequate home furniture for work. However, no statistically significant differences were found in the frequency of pain by body region between those who considered their furniture adequate and those who considered it inadequate (Table 3).
Comparison of MSP location according to perceived furniture suitability (adequate vs. inadequate).
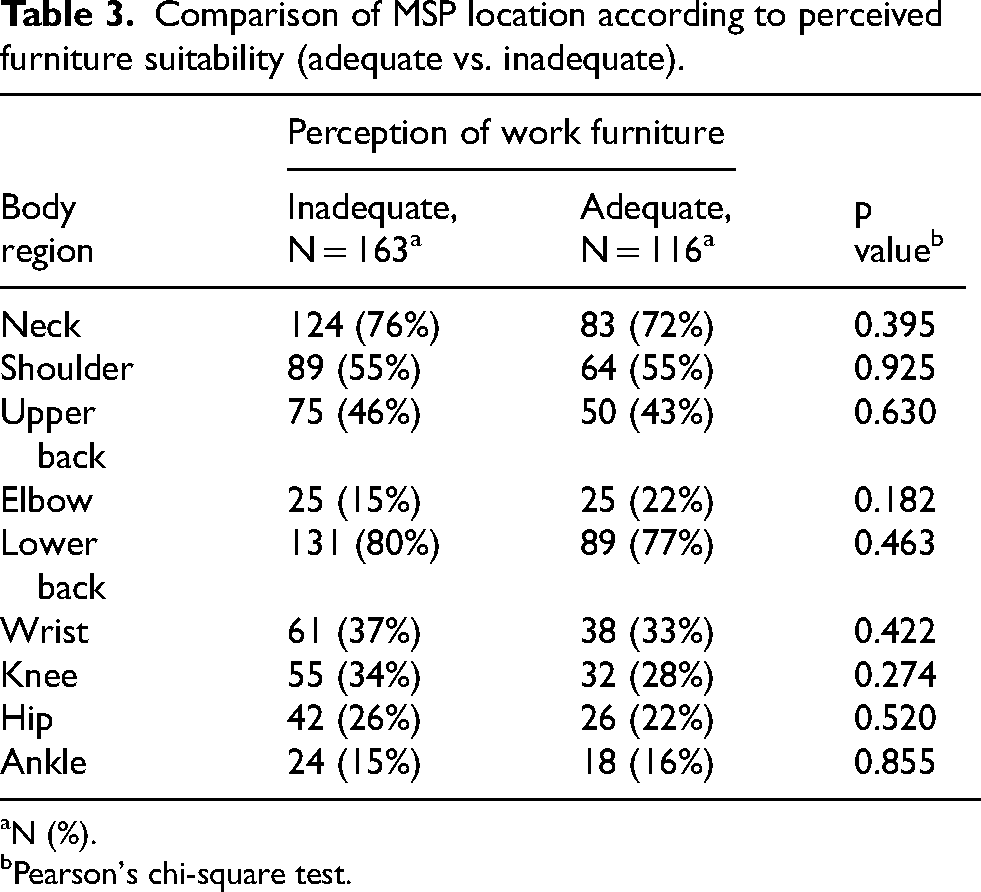
N (%).
Pearson's chi-square test.
Regarding COVID-19 Phobia results, most participants reported “low fear” (64%), followed by “moderate fear” (25%) and “high fear” (11%) (Table 4).
COVID-19 Phobia Scale score vs. pain occurrence during the pandemic.
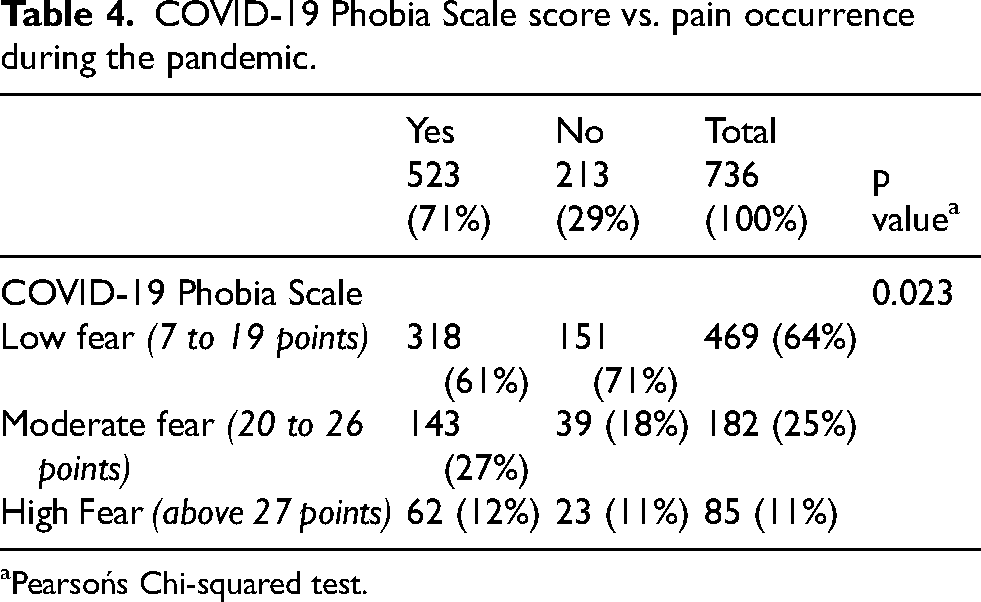
Pearsońs Chi-squared test.
Participants with moderate levels of fear were 74% more likely to experience pain during the pandemic than those with low levels of fear (Table 5).
Association between coronaphobia and MSP during the pandemic.
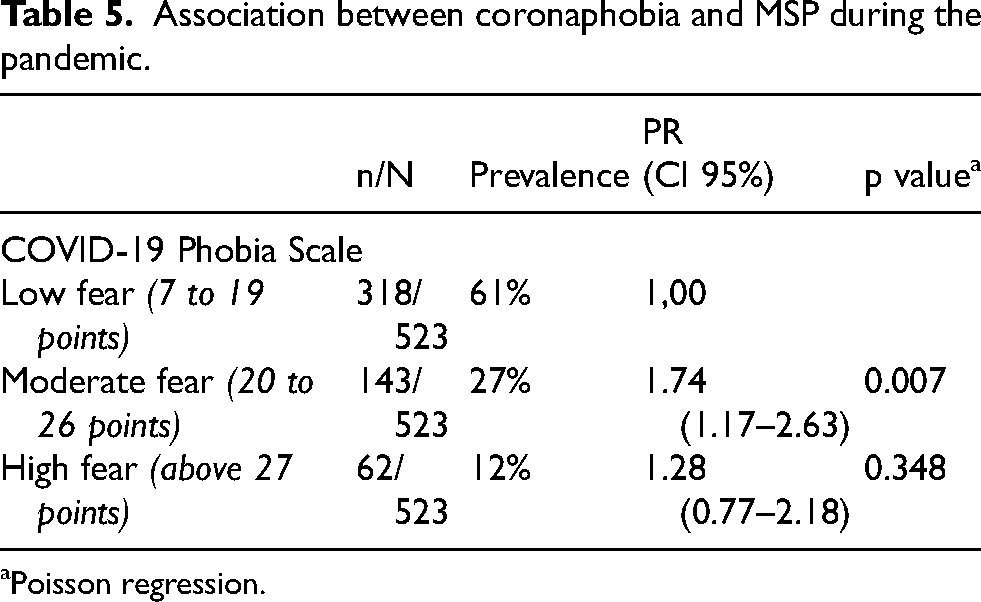
Poisson regression.
The Poisson regression model revealed a significant association between fear levels and the number of body regions with MSP (Table 6). Compared to participants with low levels of fear, those with moderate fear reported, on average, 0.43 additional regions with pain (95% CI: 0.25–0.62). This effect was even more pronounced among participants with high fear levels, who reported an average of 0.74 more painful regions (95% CI: 0.46–1.02) compared to the low-fear group.
Association between coronaphobia levels and number of painful body regions.
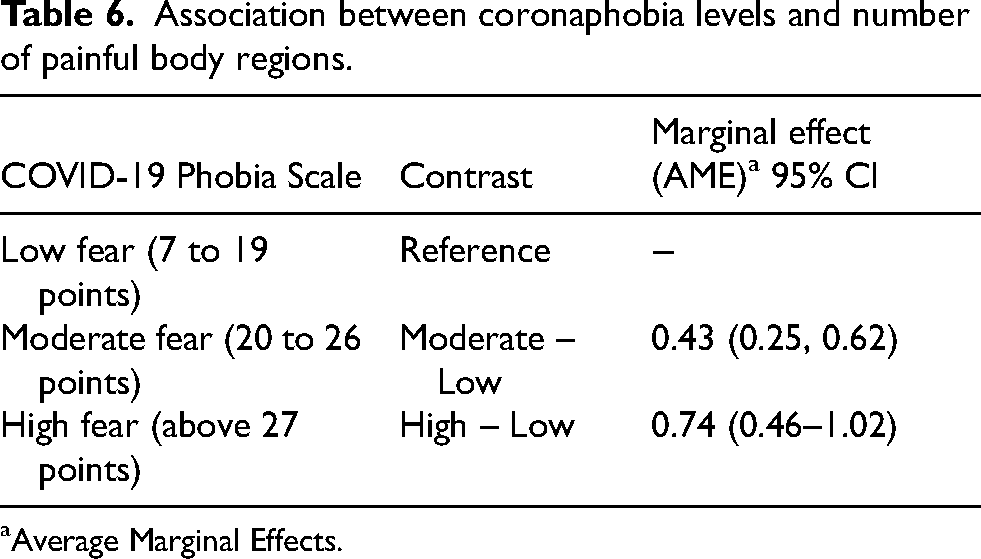
Average Marginal Effects.
Discussion
During the COVID-19 pandemic, several measures, such as social and physical isolation, were implemented to reduce transmission. This strategy, although effective, led to physical inactivity, weight gain, behavioral changes, and musculoskeletal conditions. One of the main drivers of these changes was the compulsory shift to home-office. 13
A study published in 2021 reported an increase in physical health complaints, with approximately 64.8% of respondents reporting that they had developed some health-related issues when they were working from home. 19 Home-office often involves sedentary computer work in nonergonomic environments, which can contribute to health problems, including MSP. 11 Bosma et al. 15 reported that remote workers were at greater risk of developing MSP during the first year of the COVID-19 pandemic.
The present study revealed a high prevalence of MSP and an increase in new pain cases among Brazilian home-office workers during the pandemic, reinforcing previous findings.13,15,16,20 Statistical analyses also revealed significant associations between sociodemographic variables, working conditions, and mental health.
The sample, composed of 736 individuals, predominantly female, with a mean age of 32.8 years, represents a typical profile of young, working-age adults. According to Vargová et al., 21 pandemic-related anxiety manifests differently across age groups and is more reactive and intense among young adults, who often face greater uncertainty regarding financial, academic, and professional futures. The older age of participants in the HO group suggests that this group may have had greater ability or necessity to adapt to remote work, possibly due to professional experience or family responsibilities. Differences in marital status and educational level also suggest that sociodemographic factors influence adaptation to remote work and the potential incidence of MSP.
Regarding MSP, the occurrence of new episodes was significantly associated with the pandemic, increased pain severity compared with the prepandemic period, and working from home. The high prevalence of musculoskeletal symptoms underscores the impact of changes in the work environment on physical health. These findings are consistent with those of Loef et al., 22 who identified sedentary behavior as a mediator between remote work and MSP. Ergonomics and postural habits, therefore, have become key factors in pain development among remote workers, as reported by Celenay et al. 11 The fact that more than half of participants reported inadequate furniture further suggests that domestic environments were not properly prepared for long-term work, contributing to physical discomfort.
The COVID-19 pandemic highlighted inadequate working conditions in many households because ergonomic risk factors are linked to a lack of proper workstations, which is consistent with the findings of Filho and de Lucca. 23 According to these authors, companies that maintain remote work should monitor working conditions and workload to prevent musculoskeletal disorders.
Regarding pain location, the most affected regions were the lumbar and cervical areas, corroborating findings from Argus and Pääsuke 13 and Santos et al. 20 These studies emphasize that sedentary and nonergonomically adapted workers are particularly prone to pain in these areas. Moretti et al. 24 also highlighted the widespread use of inadequate chairs and desks, which contributes to pain, particularly spinal pain. Santos et al. 20 further reported a higher prevalence of cervical MSP among women in telework, possibly due to the dual burden of professional and domestic responsibilities.
Although most participants reported low levels of coronaphobia, the results indicated a greater likelihood of pain with higher fear levels. This suggests a possible relationship between fear intensity and pain experience, reflecting the impact of emotional states on physical health. Celenay et al. 11 reported higher pain and coronaphobia levels among home office workers. Given that the present study's sample was predominantly female, these findings align with those of Peres et al. 25 and Arpaci et al., 14 who reported greater female emotional vulnerability to COVID-19 threats. The significant correlation between fear and worsened MSP also suggests that fear influences not only mental health but also pain perception and processing, as proposed by Ahorsu et al. 26 and confirmed by Yıldırım et al. 27 This may indicate that ongoing stress and inadequate environments act synergistically, amplifying pandemic-related anxiety. Oakman et al. 28 reported that poor workstation quality and high occupational demands were associated with more severe MSP, complementing the present findings.
This study also reinforces the importance of understanding coronaphobia as a multidimensional phenomenon, as highlighted by Vargová et al., 21 who differentiated between health-related and socioeconomic dimensions of pandemic anxiety.
Studies such as Oakman et al. 28 identified distinct MSP trajectories associated with factors such as workplace comfort, autonomy, and job demands. In this study, the association between work modality and MSP was statistically significant and consistent with previous literature. Moreover, Loef et al. 22 reported that sedentary behavior mediated the relationship between remote work and MSP, reinforcing the importance of interventions targeting sedentary behavior in home environments. Physical inactivity and sedentary behavior increased across all Brazilian population groups during the pandemic, 29 suggesting the onset of pain conditions.
From a practical standpoint, the results highlight the need for institutional actions promoting regular physical activity when working from home, ergonomic adjustments to home workstations, and psychological support to reduce anxiety and coronaphobia.
Study limitations include its cross-sectional design, which precludes causal inference, and the use of a convenience sample, which limits generalizability. Future research should explore the mediation between coronaphobia, coping strategies, and MSP in longitudinal models, as well as test interventions aimed at promoting mental and physical health in telework. Another important limitation to mention is the fact that the questionnaire did not collect other occupational variables that may influence MSP, such as work schedule, day or night shift, economic sector involved, position (sitting or standing).
Conclusion
This study revealed that during the COVID-19 pandemic, both physical and emotional health were significantly affected among Brazilian workers, particularly among women and younger individuals.
The prevalence of MSP increased after the onset of the pandemic, especially among individuals working from home, due to the sudden changes in the work environment imposed by lockdown. The most frequently reported pain locations were the lumbar and cervical regions. Coronaphobia was associated with MSP, with individuals reporting moderate or high levels of fear being more likely to experience pain.
The results highlight the importance of an integrated approach that addresses physical, emotional, and environmental factors in promoting the health of teleworkers. The pandemic underscores the urgent need to adapt work environments and provide support from companies or policies to mitigate adverse effects on musculoskeletal health.
Footnotes
Acknowledgements
The authors would like to thank Universidade Paulista (UNIP) and the Graduate Program in Evidence-Based Health at the Federal University of São Paulo (UNIFESP) for its institutional support.
Ethical approval
The study was approved by the Research Ethics Committee of the Universidade Paulista/UNIP (CAAE: 46136621.3.0000.5512).
Consent to participate
All participants consented to participate in the study through a consent form included in the research questionnaire.
Consent for publication
Not applicable.
Author contributions
LAC idealized and designed the study, and wrote the manuscript; JMC and RRM proceeded with data collection; NCJ analyzed the data; VTC and VFMT supervised the study and wrote the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The authors declare that the data are available for consultation through the link: Extract Questionnary.xlsx.