
Abstract
Background
Professional musicians face substantial physical and psychological demands, increasing their vulnerability to musculoskeletal pain and music performance anxiety (MPA). In middle-income settings such as Brazil, additional socio-economic stressors may intensify these occupational health challenges.
Objective
To investigate the association between musculoskeletal pain, MPA, and stress-producing life events (SPLE) among Brazilian orchestral musicians.
Methods
A cross-sectional study was conducted with 273 professional orchestral musicians from Rio de Janeiro, Brazil. Musculoskeletal pain was assessed using the Musculoskeletal Pain Intensity and Interference Questionnaire for Musicians (MPIIQM-Br), MPA using the Kenny Music Performance Anxiety Inventory (K-MPAI), and SPLE through a checklist of stress-producing life events. Descriptive statistics estimated the prevalence of pain and clinically significant MPA (K-MPAI ≥105). Binary logistic regression examined factors associated with pain and clinically significant MPA, while multivariable linear regression analyzed associations between MPA scores and pain intensity and interference.
Results
Musculoskeletal pain was highly prevalent, with 93.4% reporting lifetime pain and 86.8% reporting pain in the previous 12 months. Clinically significant MPA was observed in 60.4% of participants. Higher K-MPAI scores were associated with greater pain intensity and interference. Female musicians reported higher pain levels, and weekly playing hours were positively associated with pain interference. Financial problems and separation/divorce increased the likelihood of clinically significant MPA.
Conclusions
Brazilian orchestral musicians experience a high burden of musculoskeletal pain and MPA. Psychological vulnerability and socio-economic stressors contribute to these conditions, underscoring the need for integrated occupational health strategies addressing both physical and mental health.
Introduction
Achieving excellence in musical performance requires the seamless integration of sensory, cognitive, and emotional abilities, which places considerable physical and psychological demands on musicians that are often comparable to those experienced by elite athletes.1,2 These combined pressures increase vulnerability to occupational health issues, particularly musculoskeletal pain, which is frequently reported by instrumentalists due to repetitive movements, sustained postures, and the psychosocial demands of their work.3–6 From an occupational health perspective, orchestral musicians perform under sustained biomechanical load combined with high-performance expectations, creating a work environment characterized by cumulative physical strain and psychological stress.5,6
Systematic reviews have documented the high global prevalence of musculoskeletal pain among orchestral musicians,7,8 though severity and impact vary across regions. 9 In Brazil, recent studies suggest a lifetime prevalence exceeding 80%.10,11 This figure is especially concerning given the country's large population of professional musicians and the widespread normalization of musculoskeletal pain, often accepted as an unavoidable consequence of artistic commitment and financial necessity.12,13 Despite these consistently high prevalence rates, much of the literature has concentrated on estimating occurrence and anatomical distribution of pain rather than examining how physical symptoms interact with broader psychosocial and occupational determinants.7–13
Importantly, chronic musculoskeletal pain extends beyond a purely physical problem and is closely associated with emotional distress, social withdrawal, and even professional dropout.14,15 While its association with music performance anxiety (MPA) has been increasingly recognized, evidence regarding the direction and nature of this relationship remains inconclusive.14–16 Existing studies have often explored musculoskeletal pain and MPA either independently or through bivariate associations, limiting a comprehensive understanding of how these phenomena coexist within musicians’ professional routines.14–16
MPA itself is a complex phenomenon, influenced by biological predispositions, psychological traits, and situational pressures.17,18 Although occasional anxiety is common among musicians before performances, in its severe form MPA can impair technical execution and overall artistic quality.19,20,21 The literature conceptualizes MPA through multiple lenses, including clinical, psychological, and contextual frameworks that emphasize the role of stress perception, situational factors, and pressure training.18–20 However, fewer investigations have embedded MPA within an integrated occupational framework that simultaneously accounts for physical workload and external stress exposure.
Recent studies have expanded the understanding of MPA and musculoskeletal pain by incorporating broader social and environmental factors.22,23,24 In Brazil, musicians are disproportionately exposed to stress-producing life events (SPLE), including financial hardship, interpersonal conflict, exposure to violence, and forced displacement, factors that may heighten anxiety and erode psychological resilience.23–26 These challenges are intensified by the country's socio-economic landscape, marked by precarious employment, weakened social networks, and increasing urban insecurity. 25 Although SPLE have been associated with mental health outcomes in Brazilian populations,23–26 their concurrent relationship with both musculoskeletal pain and performance anxiety among professional musicians remains insufficiently examined.
Taken together, the current body of literature demonstrates three parallel lines of evidence: (1) high prevalence of musculoskeletal pain among musicians7–12; (2) significant rates of music performance anxiety and its functional consequences17–21; and (3) documented exposure to stress-producing life events in Brazilian contexts.23–26 Nevertheless, these domains have largely progressed independently, with limited research simultaneously integrating physical symptoms, psychological vulnerability, and contextual stressors using multivariable analytical approaches within an occupational health framework.
Accordingly, there is a need for analytical approaches that move beyond isolated prevalence estimates and instead examine how musculoskeletal pain, music performance anxiety, and stress-producing life events interact within professional orchestral environments. Addressing this gap is particularly relevant in middle-income settings such as Brazil, where socio-economic instability may intensify occupational strain and health vulnerability.
Considering these factors, this study addresses a critical gap by examining how musculoskeletal pain, MPA, and SPLE interact among Brazilian orchestral musicians, an underrepresented yet potentially vulnerable occupational group. By integrating physical, psychological, and contextual dimensions within a multivariable analytical framework, this study contributes to occupational health research by clarifying the interrelationships between biomechanical demands, performance-related anxiety, and external stress exposure.
Specifically, the primary aims were to: (1) characterize the prevalence of musculoskeletal pain and MPA among orchestral musicians, and (2) investigate the association between music performance anxiety and musculoskeletal pain outcomes, including pain intensity and pain-related interference. The secondary aim was to explore the influence of stress-producing life events on both musculoskeletal pain and MPA.
Methods
This study adhered to the STROBE (STrengthening the Reporting of OBservational studies in Epidemiology) guidelines to ensure rigorous and transparent reporting of the methods and findings. 27
Study design and setting
This cross-sectional study was conducted from March 2022 to July 2023 across eight cities in the state of Rio de Janeiro, Brazil. The study was approved by the Research Ethics Committee (UNISUAM, ID 1.444.640/CAAE 51947215.6.0000.5235) and conducted in accordance with the Declaration of Helsinki. All participants provided written informed consent, and anonymity was guaranteed. To ensure confidentiality, questionnaires were completed using identification codes rather than names, and any personal identifiers were removed prior to data entry and statistical analysis. The researchers responsible for statistical procedures had access only to anonymized datasets. The first author, alongside another trained interviewer, administered the questionnaires in person.
Participants and sample size
A cluster sampling approach was used for recruitment, with orchestras defined as the primary sampling units (clusters), as musicians are naturally grouped within these institutional ensembles.
In the state of Rio de Janeiro, Brazil, 24 orchestras were identified through a mapping of active ensembles based on publicly available sources, including concert programs, cultural event announcements, institutional websites, and social media platforms used for concert promotion. These orchestras constituted the sampling frame for the study (Figure 1).
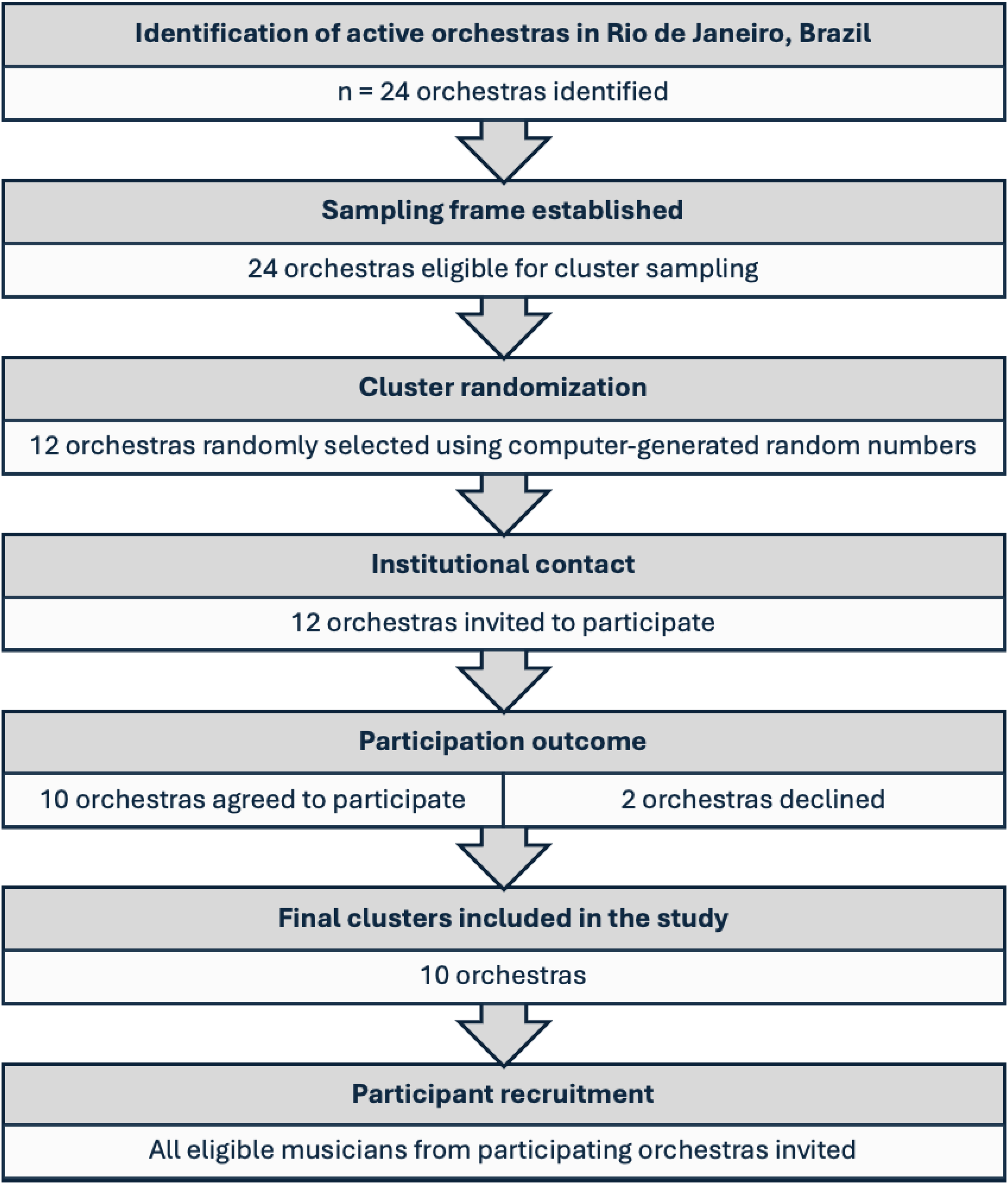
Flow diagram of orchestra identification and cluster sampling.
Each orchestra was assigned a numerical identifier (1–24), and a simple random sampling procedure was performed using a computer-generated random number generator to select 12 orchestras. The selected institutions were contacted and formally invited to participate. Of these, 10 orchestras agreed to participate and were included in the study.
All eligible musicians from the participating orchestras were invited to participate in the survey. To protect institutional and participant confidentiality, the names of the orchestras are not disclosed. Given the relatively small number of orchestras operating in Brazil, identifying the institutions could facilitate deductive disclosure and potentially allow the identification of participating musicians.
Prior to inclusion, all participants completed a brief questionnaire to verify eligibility based on these criteria. Musculoskeletal pain was assessed specifically in the context of musical practice.
An a priori sample size calculation was conducted using G*Power version 3.1. 28 The estimation was based on the primary multivariable analysis planned for the study, using a multiple linear regression model to examine associations between music performance anxiety and musculoskeletal pain outcomes. The following parameters were specified: test family = F tests; statistical test = linear multiple regression (fixed model, R2 deviation from zero); effect size f2 = 0.15, representing a moderate effect size; α error probability = 0.05; statistical power (1 − β) = 0.95; and four predictors (sex, age, weekly playing hours, and music performance anxiety).14–16 Under these assumptions, the minimum required sample size was 129 participants. To account for potential incomplete responses or missing data, an additional margin of approximately 10% was considered, resulting in a target sample of 142 musicians. Ultimately, 273 eligible musicians were included, substantially exceeding the minimum requirement. This larger sample increased the precision of the estimates and provided greater statistical stability for the multivariable regression models conducted in the study.
Although orchestras were used as clusters for recruitment, the unit of analysis in this study was the individual musician. Given the relatively small number of clusters and the study's focus on individual-level associations, all regression analyses were conducted at the participant level.
Materials
The study collected data on musicians’ demographic and professional characteristics, including age, sex, instrument played, work schedule (full-time or part-time), years of experience, and weekly performance hours.
Musculoskeletal pain was assessed using the Musculoskeletal Pain Intensity and Interference Questionnaire for Musicians (MPIIQM). The tool was developed based on the biopsychosocial principles from the World Health Organization's (WHO) International Classification of Functioning, Disability, and Health (ICF). 29 After its adaptation to the Brazilian context, the MPIIQM-Br demonstrated strong psychometric properties, with a Cronbach's α of 0.90 and an intraclass correlation coefficient of 0.84. 30 This 22-item questionnaire collects personal data such as age and sex, and assesses musical practices, the presence and severity of musculoskeletal pain, and its impact on mood, enjoyment of life, and instrumental performance. Each item is scored on a scale from 0 (no pain or difficulty) to 10 (severe pain or inability to perform). 31 Pain intensity and pain interference subscale scores were calculated as the mean of their respective items (range: 0–10), with the intensity subscale including four items (worst, least, average, and current pain) and the interference subscale including five items reflecting psychosocial and performance-related impact. For descriptive purposes, summed scores were also considered, ranging from 0 to 40 for pain intensity and from 0 to 50 for pain interference.
To assess MPA, we used the Kenny Music Performance Anxiety Inventory (K-MPAI). This 40-item inventory is grounded in Barlow's theory of anxiety disorders, which integrates cognitive, behavioral, and physiological dimensions.32,33 It assesses various aspects of anxiety, including negative affect, attentional shifts, and psychological and memory alterations.32–34 The K-MPAI was adapted for the Brazilian context, where it demonstrated high reliability with a Cronbach's α of 0.95. 34
The SPLE inventory was used to assess significant life experiences that may have psychological or physical impacts. It captures events occurring within the past 12 months using closed-ended, dichotomous (yes/no) questions. These events include serious illness, hospitalization, death of a close relative, financial difficulties, forced relocation, separation or divorce, physical aggression, and assault/robbery. 25 The SPLE inventory has been validated in a Brazilian sample, with kappa values ranging from 0.62 to 1.00. 35
Bias control
To minimize potential sources of bias, several procedures were implemented during data collection and data processing. To prevent duplicate participation among musicians performing in more than one orchestra, participants’ full names were temporarily recorded solely for verification purposes. After confirming eligibility and ensuring that each participant was included only once, questionnaires were assigned a numerical identification code, and identifying information was removed prior to data entry.
Questionnaires were reviewed immediately after completion to verify that all items had been answered. When incomplete responses were identified, participants were asked to complete missing items whenever possible. Data were double-checked during entry to minimize transcription errors, and consistency checks were performed before statistical analysis. No missing data were observed for the variables included in the final analyses.
Confidentiality and data protection
To ensure participant confidentiality, all data used for analysis were anonymized and stored using unique numerical identification codes. Any identifying information collected temporarily for eligibility verification and duplicate participation control was stored separately from the analytical dataset and was not accessible during statistical analyses.
Access to the dataset was restricted to the research team, and all files were stored in password-protected systems. Given the relatively small number of musicians within each orchestra, study results are presented only in aggregated form to prevent the potential identification of individual participants.
Statistical methods
Descriptive statistics were used to summarize socio-demographic, occupational, and clinical characteristics of the participants. For normally distributed variables, data are presented as mean ± standard deviation (SD), whereas non-normally distributed variables are presented as median and interquartile range [IQR]. Normality of distributions was assessed using the Shapiro—Wilk test.
Binary logistic regression analyses were performed to examine associations between binary outcomes and potential explanatory variables. These outcomes included the presence of musculoskeletal pain in different time frames (lifetime, previous 12 months, previous four weeks, and previous seven days) and clinically significant music performance anxiety (MPA ≥105). 36 Independent variables included sex and exposure to SPLE, and other demographic characteristics. Results are presented as odds ratios (OR) with 95% confidence intervals (CI).
To examine factors associated with pain severity, multivariable linear regression models were used with continuous outcomes derived from the Musculoskeletal Pain Intensity and Interference Questionnaire for Musicians (MPIIQM). Separate models were constructed for the pain intensity subscale score and the pain interference subscale score. Additional item-level analyses were conducted for specific pain intensity indicators (worst pain, least pain, average pain, and pain at the time of assessment) and pain interference domains. Multicollinearity among predictors was assessed using variance inflation factors (VIF), and no evidence of collinearity was observed.
Based on theoretical relevance and prior literature, the predictors included in the multivariable models were music performance anxiety (K-MPAI total score), sex, age, and total weekly playing hours. These variables were included to control for potential confounding effects. All predictors were entered simultaneously into the models. Results are reported as unstandardized regression coefficients (B) with 95% confidence intervals (CI), indicating the expected change in the pain outcome for each unit increase in the predictor. Assumptions of linear regression were assessed by inspection of residual plots. All analyses were conducted using Jeffreys's Amazing Statistics Program (JASP) software (Version 0.18.3, JASP Team).
Results
Participants
In total, 303 musicians were invited to participate in this study, and 273 accepted, representing a high response rate of 90%. No participants were excluded based on eligibility criteria. The characteristics of participants (Table 1) reveal a balanced sex distribution, with 50.2% male (n = 137) and 49.8% female (n = 136) musicians. The average age was 38.0 years (±6.1), and the majority (85.7%, n = 234) held college degrees. Most participants were string players (77.7%, n = 212), followed by woodwind (13.5%, n = 37), brass (4.8%, n = 13), and percussion players (4.0%, n = 11). In terms of employment, 66.3% (n = 181) worked part-time, while 33.7% (n = 92) were full-time orchestra members. On average, participants had 25.9 years of instrument playing experience (±6.1), with 18.7 years of professional orchestra experience (±5.9). Additionally, they played 20.5 h per week outside the orchestra (±6.7) and 22.2 h in the orchestra (±6.5).
Sociodemographic and professional characteristics of participants (n = 273), n (%) or mean ± sd.
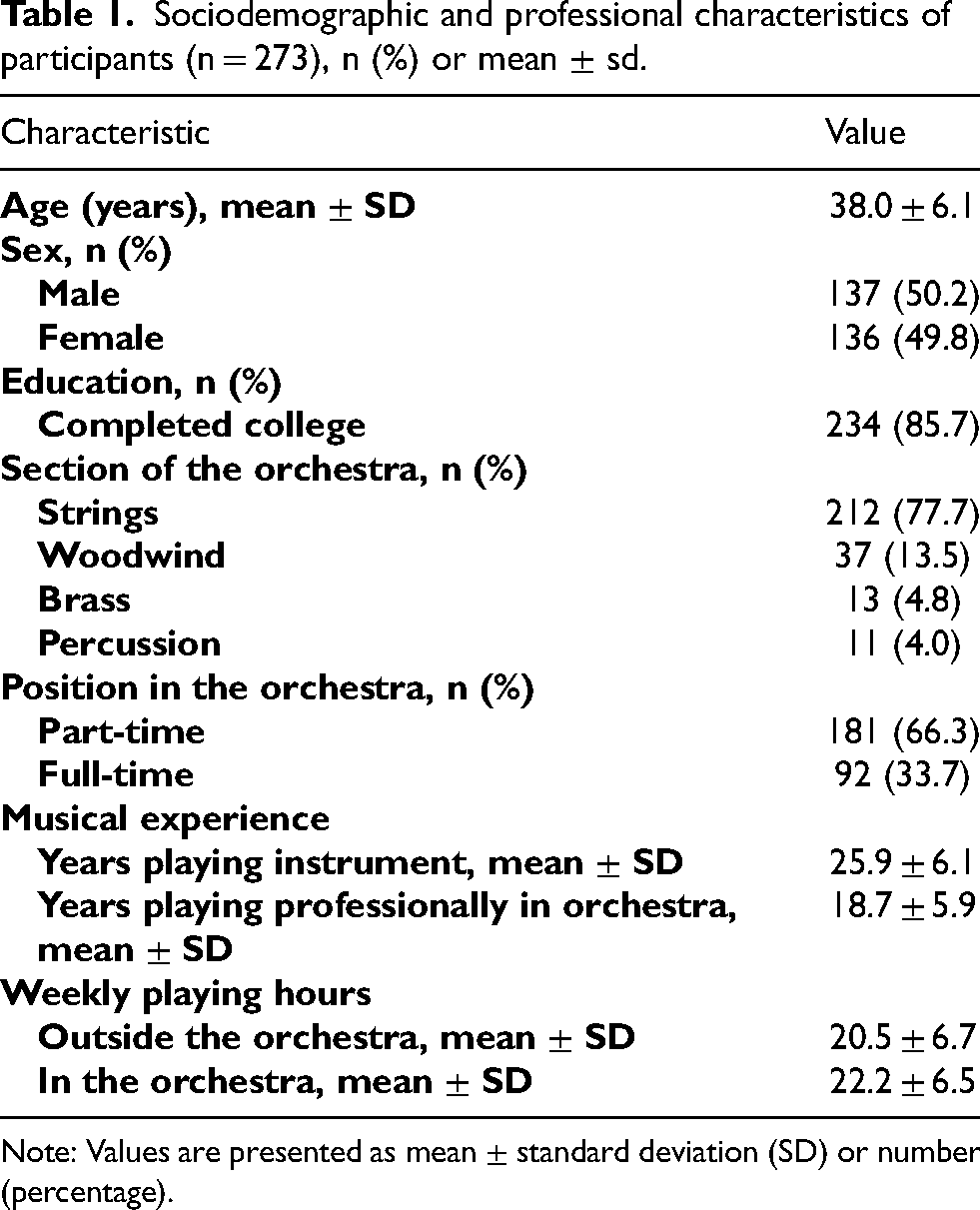
Note: Values are presented as mean ± standard deviation (SD) or number (percentage).
Musculoskeletal pain prevalence
Over the lifetime, 93.4% (n = 255) of participants reported experiencing musculoskeletal pain. In the past 12 months, 86.8% (n = 236) experienced pain, while 75.0% (n = 205) reported pain in the previous month, and 65.9% (n = 180) in the previous week. The prevalence of musculoskeletal pain varied by instrument section, with string and woodwind players reporting the highest rates, exceeding 80%, while brass musicians were the least affected.
The most frequently reported areas of pain in the past month were the left shoulder (38.7%, n = 82), right shoulder (16.9%, n = 36), and lumbar region (16.5%, n = 35) (Table 2).
Prevalence, interference and intensity of musculoskeletal pain among orchestral musicians.
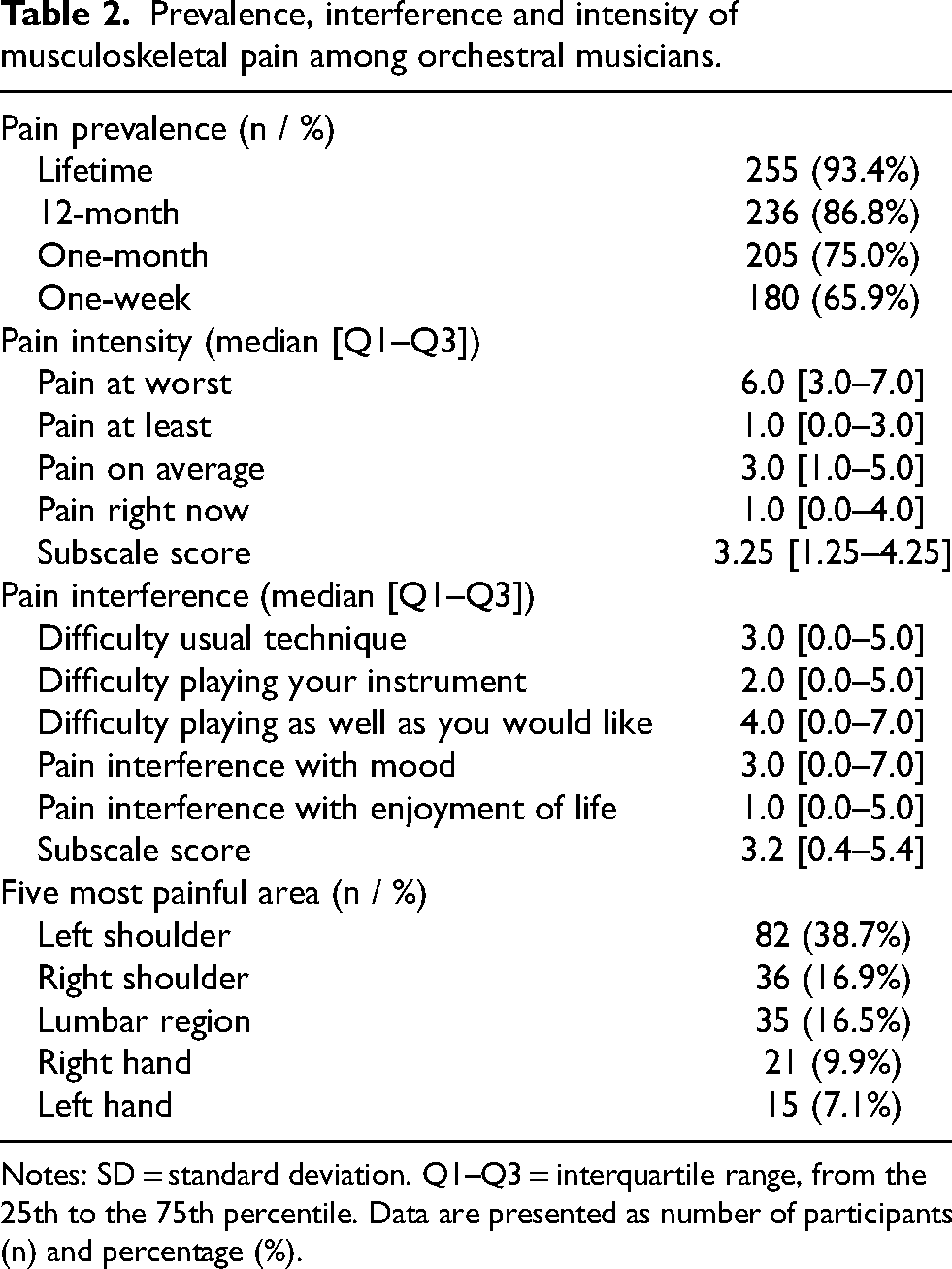
Notes: SD = standard deviation. Q1–Q3 = interquartile range, from the 25th to the 75th percentile. Data are presented as number of participants (n) and percentage (%).
Musculoskeletal pain intensity and interference
When asked about pain intensity in the past week, the median score for worst musculoskeletal pain was 6 [3.0–7.0] on a scale from 0 to 10. The median score for the least musculoskeletal pain experienced was 1 [0.0–3.0], while the average musculoskeletal pain level was 3 [1.0–5.0]. At the time of the survey, participants reported a median pain level of 1 [0.0–4.0].
Pain interference was also assessed in several domains. The median interference with mood was rated at 3 [0.0–7.0], while the impact on enjoyment of life was minimal, with a median score of 1 [0.0–5.0]. Regarding its effect on playing technique, the interference was rated at 3 [0.0–5.0], and musicians rated the interference with their ability to perform as desired at 4 [0.0–7.0] (Table 2).
Music performance anxiety
The average score on the K-MPAI was 115 (± 39.1), with the highest score reaching 214 out of a possible 240. According to Kenny (2015), 36 a score of 105 or higher is considered clinically significant for MPA, and 60.4% (n = 165) of the musicians scored above this threshold. Among the different subcategories of the K-MPAI, the highest mean scores were found in “worry focused on self” (27.0 out of 48), “biological vulnerability” (3.2 out of 6), and “memory” (6.3 out of 12) (Table 3).
Kenny music performance anxiety inventory (K-MPAI) scores, mean ± sd.
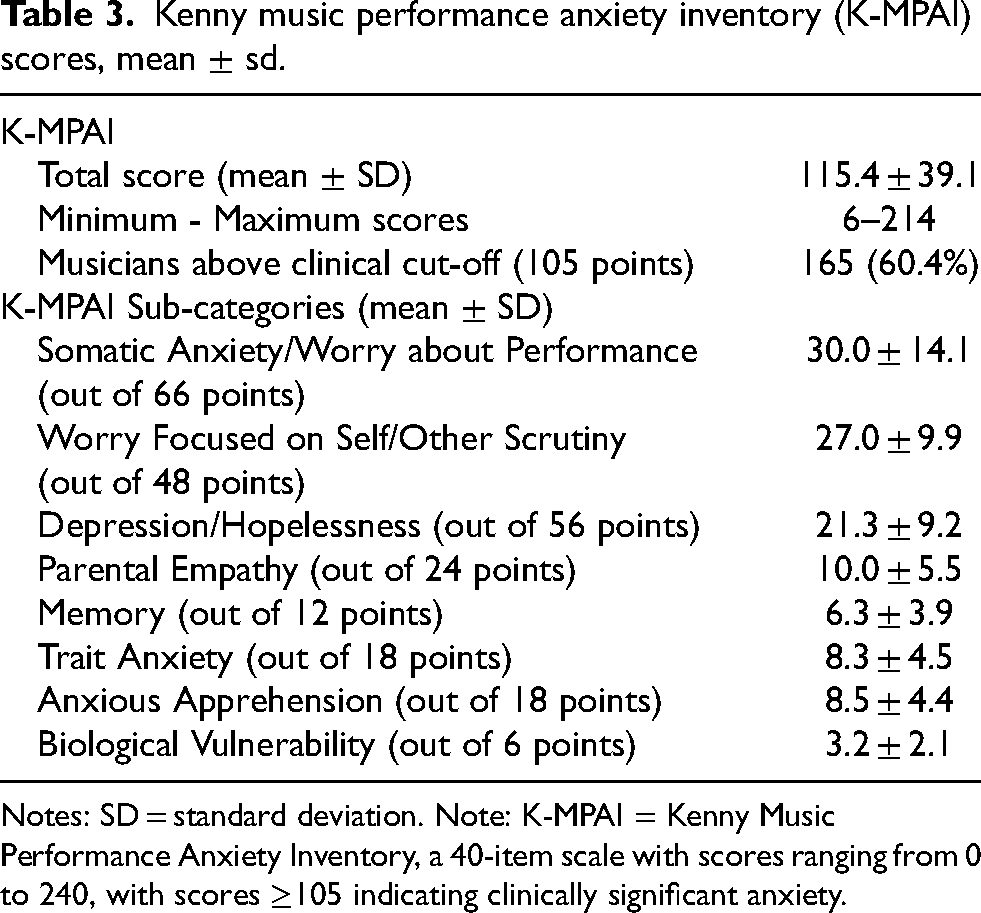
Notes: SD = standard deviation. Note: K-MPAI = Kenny Music Performance Anxiety Inventory, a 40-item scale with scores ranging from 0 to 240, with scores ≥105 indicating clinically significant anxiety.
Stress-Producing life events
The most frequently reported SPLE in the last 12 months included financial problems (59.3%, n = 162), the death of a close relative (32.6%, n = 89), a forced change of residence (26.3%, n = 72), and separation or divorce (24.5%, n = 67) (Table 4).
Stress-producing life events reported in the last 12 months, n (%).
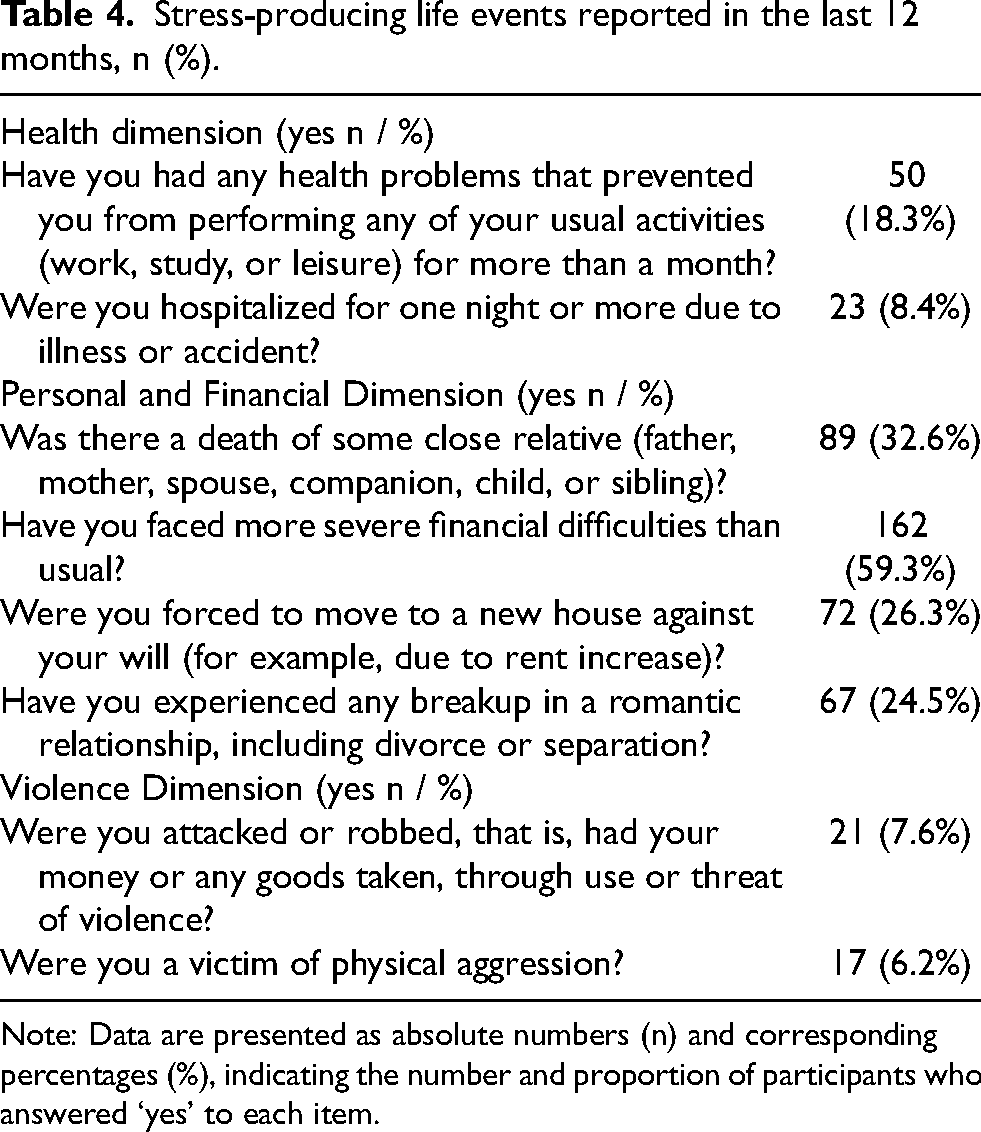
Note: Data are presented as absolute numbers (n) and corresponding percentages (%), indicating the number and proportion of participants who answered ‘yes’ to each item.
Factors associated with music performance anxiety and musculoskeletal pain
Binary logistic regression models were used to examine factors associated with clinically significant music performance anxiety (MPA) and musculoskeletal pain outcomes (Table 5).
Logistic regression analysis of factors associated with music performance anxiety and musculoskeletal pain outcomes (or, 95% ci).
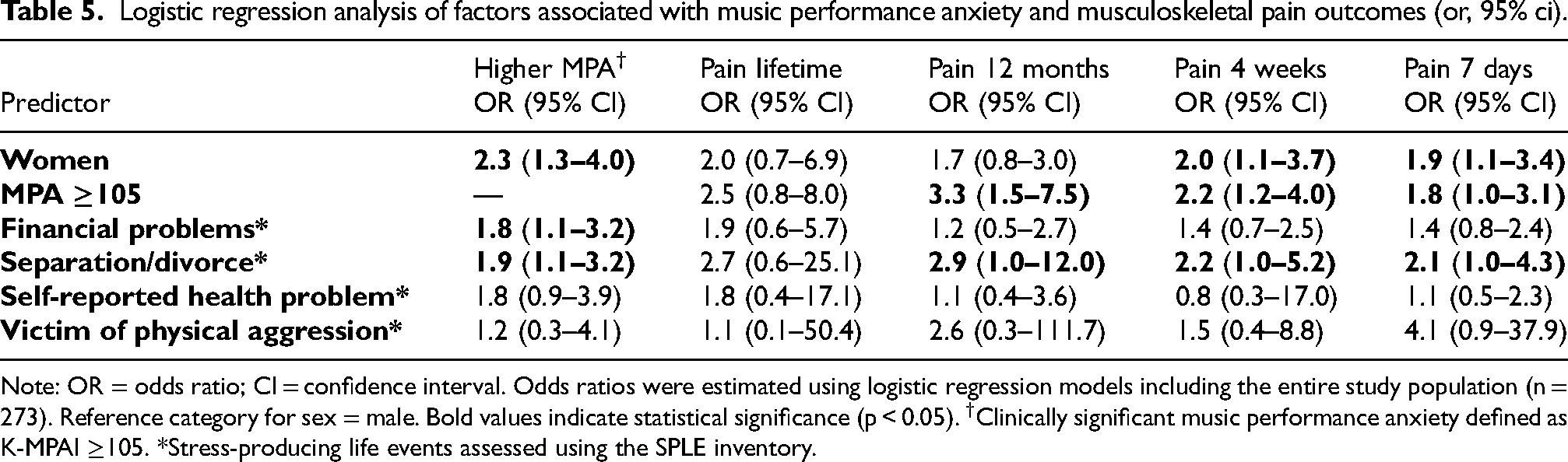
Note: OR = odds ratio; CI = confidence interval. Odds ratios were estimated using logistic regression models including the entire study population (n = 273). Reference category for sex = male. Bold values indicate statistical significance (p < 0.05). †Clinically significant music performance anxiety defined as K-MPAI ≥105. *Stress-producing life events assessed using the SPLE inventory.
Female musicians had significantly higher odds of presenting clinically significant MPA compared with male musicians (OR 2.3, 95% CI 1.3–4.0, p < 0.001). In addition, stress-producing life events were associated with increased odds of MPA. Specifically, financial problems (OR 1.8, 95% CI 1.1–3.2, p < 0.01) and separation or divorce (OR 1.9, 95% CI 1.1–3.2, p < 0.01) were significantly associated with clinically significant MPA.
Clinically significant MPA was also associated with musculoskeletal pain outcomes. Musicians with K-MPAI scores ≥105 had higher odds of reporting musculoskeletal pain in the last 12 months (OR 3.3, 95% CI 1.5–7.5, p = 0.001), the last four weeks (OR 2.2, 95% CI 1.2–4.0, p = 0.004), and the last seven days (OR 1.8, 95% CI 1.0–3.1, p = 0.01).
Stress-producing life events were also independently associated with musculoskeletal pain outcomes. Musicians who experienced financial problems or separation/divorce showed higher odds of reporting pain across several time frames. In particular, separation or divorce was associated with increased odds of pain in the last 12 months (OR 2.9, 95% CI 1.0–12.0, p = 0.04), the last four weeks (OR 2.2, 95% CI 1.0–5.2, p = 0.03), and the last seven days (OR 2.1, 95% CI 1.0–4.3, p = 0.02).
Multivariable associations with pain outcomes
Results from the multivariable linear regression models are presented in Table 6. In the pain intensity domain, higher music performance anxiety scores were significantly associated with greater pain intensity. Each one-point increase in the K-MPAI score was associated with a 0.014-point increase in mean pain intensity (95% CI 0.008–0.020, p < 0.001). Female musicians reported significantly higher pain intensity compared with males, with mean pain intensity nearly one point higher among women (B = -0.919, 95% CI −1.372 to −0.466, p < 0.001). Age and weekly playing hours were not significantly associated with pain intensity outcomes. Item-level analyses showed similar patterns across worst pain, least pain, average pain, and pain at the time of assessment (Table 6).
Multivariable linear regression models examining associations between music performance anxiety and musculoskeletal pain outcomes among orchestral musicians (n = 273).
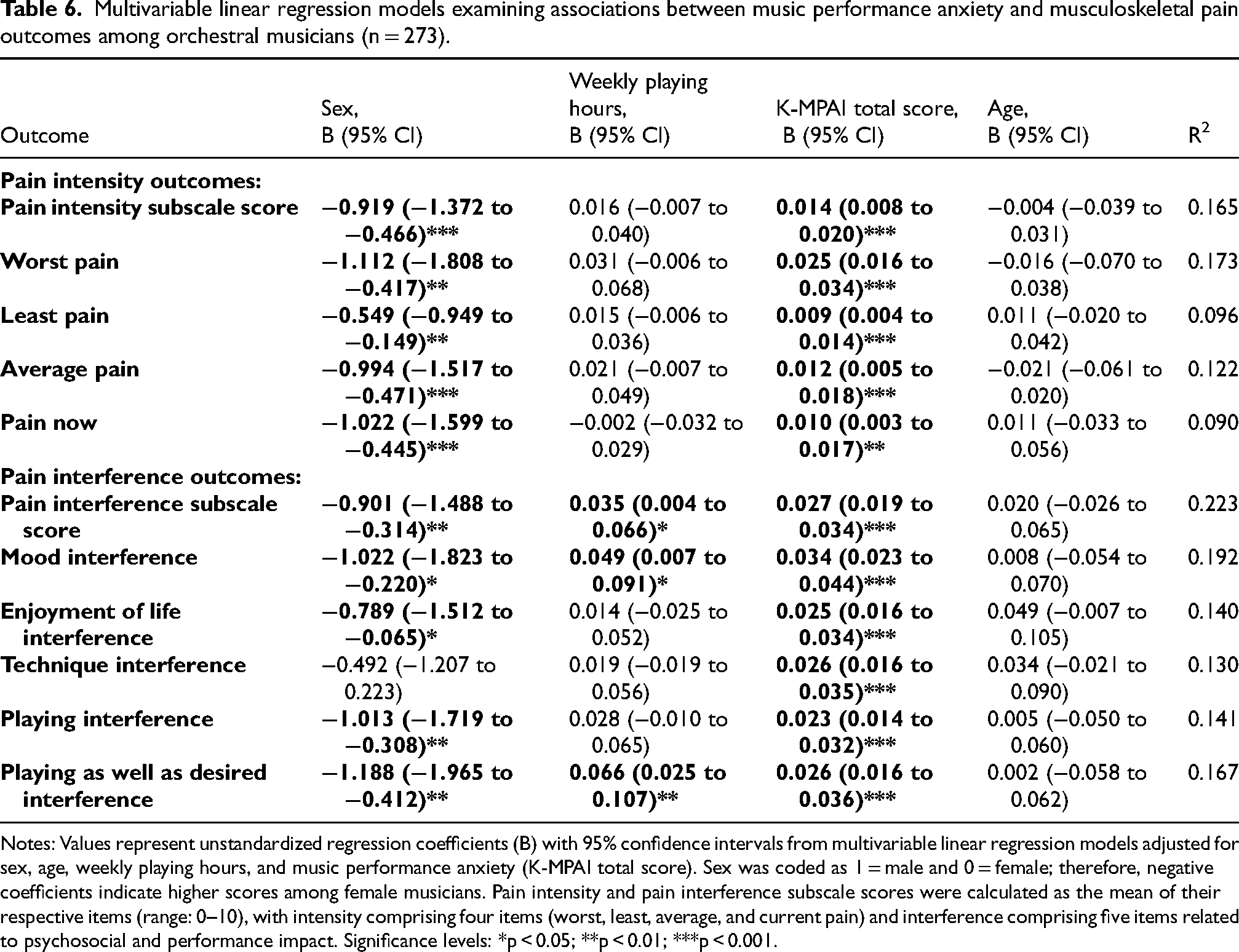
Notes: Values represent unstandardized regression coefficients (B) with 95% confidence intervals from multivariable linear regression models adjusted for sex, age, weekly playing hours, and music performance anxiety (K-MPAI total score). Sex was coded as 1 = male and 0 = female; therefore, negative coefficients indicate higher scores among female musicians. Pain intensity and pain interference subscale scores were calculated as the mean of their respective items (range: 0–10), with intensity comprising four items (worst, least, average, and current pain) and interference comprising five items related to psychosocial and performance impact. Significance levels: *p < 0.05; **p < 0.01; ***p < 0.001.
In the pain interference domain, higher music performance anxiety scores were also significantly associated with greater pain-related interference. Each one-point increase in K-MPAI score was associated with a 0.027-point increase in the pain interference subscale score (95% CI 0.019–0.034, p < 0.001). Female sex was also associated with higher pain interference (B = -0.901, 95% CI −1.488 to −0.314, p = 0.003). Weekly playing hours were positively associated with the interference score (B = 0.035, 95% CI 0.004–0.066, p = 0.027), whereas age was not significantly associated with this outcome.
Similar associations were observed across specific interference domains, including mood, enjoyment of life, and playing-related outcomes (Table 6). In addition to these individual predictors, exposure to stress-producing life events was also examined to explore potential contextual factors associated with music performance anxiety and musculoskeletal pain.
Discussion
This study investigated the relationship between musculoskeletal pain, MPA, and stress-producing life events among professional orchestral musicians in Brazil. Three main findings emerged. First, musculoskeletal pain was highly prevalent across all time frames assessed. Second, a substantial proportion of musicians presented clinically significant MPA. Third, psychological and contextual factors, including MPA and stress-producing life events, were consistently associated with both the occurrence and the functional impact of musculoskeletal pain.
By simultaneously examining musculoskeletal pain, music performance anxiety, and stress-producing life events within a multivariable framework, this study provides new insight into how physical and psychosocial factors interact in orchestral musicians.
Prevalence of musculoskeletal pain in orchestral musicians
In this cross-sectional study of Brazilian orchestral musicians, we observed a very high prevalence of musculoskeletal pain across all assessed time frames. Specifically, 93.4% of participants reported experiencing pain at some point in their lifetime, 86.8% within the previous 12 months, 75.0% within the past month, and 65.9% within the previous week. These results reinforce previous evidence indicating that musculoskeletal pain is one of the most common occupational health problems affecting professional musicians worldwide.7,9,38
The prevalence observed in the present study is slightly higher than that reported in several international investigations. For example, Eliassen et al. (2025) 39 reported an 85% prevalence of musculoskeletal pain among professional orchestral musicians in Norway, with the neck, shoulders, and upper back being the most frequently affected regions. In that study, pain severity was also associated with psychological distress and sleep disturbances, highlighting the importance of considering both physical and psychological factors in musicians’ health. Similarly, Pereira et al. (2025) 40 reported that 88.8% of Brazilian music students experienced musculoskeletal pain during the previous year, particularly in the cervical, thoracic, and lumbar regions, as well as in the right shoulder and hand. These findings are consistent with the present results and reinforce the substantial biomechanical demands imposed by instrumental performance.
The high prevalence observed in our sample may also be partly explained by the characteristics of the participating musicians. Most participants were string players, a group widely recognized as having an elevated risk of musculoskeletal disorders due to prolonged asymmetric postures and repetitive upper limb movements.9,10 Additionally, most musicians in the present sample worked on a part-time basis within orchestras, which may reflect more precarious employment conditions. Such instability can limit access to specialized healthcare, delay treatment seeking, and increase vulnerability to both physical pain and psychological stress.
The broader social and occupational context of Brazil may further contribute to the high burden of musculoskeletal pain observed. A large national survey conducted by Bezerra et al., 41 including more than 60,000 adults, reported that chronic musculoskeletal conditions are highly prevalent in the Brazilian population. Similarly, a systematic review by Aguiar et al. 42 reported chronic pain prevalence estimates ranging from 23.0% to 76.2% across Brazilian studies, with an overall average of 45.3%. These conditions were particularly common among women and were strongly associated with socioeconomic disadvantage and limited access to healthcare services. When combined with the intense physical demands of professional music performance and the scarcity of specialized healthcare for musicians, these structural factors may contribute to the particularly high pain prevalence observed in the present study.
Sex differences in pain outcomes
Sex differences also emerged as an important finding in the present study. Female musicians showed higher odds of reporting musculoskeletal pain in recent time frames and, in the multivariable linear regression models, also demonstrated higher pain intensity and pain interference scores compared with male musicians. These results suggest that female musicians may experience a greater functional impact of musculoskeletal pain within orchestral work environments.
These findings are consistent with previous research on Brazilian violinists, which reported that women were more than four times more likely to develop musculoskeletal disorders than men (OR 4.4, 95% CI [1.9–10.0], p < 0.001).37, 38 According to Kochem et al. (2017), 38 several factors may contribute to this increased vulnerability, including differences in muscle strength, joint mobility, and anatomical structure, which may predispose women to earlier fatigue and greater mechanical overload when performing highly demanding instruments such as the violin.
Beyond physiological differences, broader occupational and social factors may also play a role. In the Brazilian labor context, women often experience greater socioeconomic vulnerability, including lower income, reduced access to healthcare, and disproportionate caregiving responsibilities. 43 These factors may increase cumulative stress exposure and reduce opportunities for recovery from physical strain. Within orchestral environments, where musicians are required to maintain prolonged postures and perform repetitive movements under performance pressure, these overlapping risk factors may contribute to greater musculoskeletal burden among female musicians.
Social stressors and occupational context
In addition to the physical and psychological demands of orchestral performance, our findings suggest that broader social stressors may also contribute to musicians’ health outcomes. Stress-producing life events (SPLE), particularly financial difficulties and relationship-related stressors, were associated with both higher levels of music performance anxiety and increased odds of reporting musculoskeletal pain.
Financial instability may play a particularly important role in this relationship. Many orchestral musicians in Brazil experience irregular employment conditions, limited social protection, and restricted access to specialized healthcare services. These structural constraints may delay treatment for musculoskeletal symptoms, increase psychological stress, and ultimately contribute to the persistence or exacerbation of pain. Previous studies have similarly reported that economic insecurity and job instability are associated with higher levels of performance anxiety among musicians.24,44
The findings of the present study are also consistent with previous research highlighting the potential interaction between psychological stress and musculoskeletal symptoms. Although the cross-sectional design does not allow causal inferences, the results are compatible with a potentially reciprocal relationship between pain and anxiety. Musculoskeletal pain may increase psychological distress and performance concerns, while heightened anxiety may amplify physiological stress responses and increase pain perception during performance situations.15,38,45,46
Relational stressors also appear to play a role in musicians’ well-being. In the present study, separation or divorce was associated with higher odds of both musculoskeletal pain and music performance anxiety. Similar patterns have been reported by Matei and Ginsborg, 47 who observed that relationship difficulties were among the most common reasons music students sought psychological support in a conservatoire setting in the United Kingdom. Emotional stress resulting from interpersonal conflict may intensify psychological vulnerability and increase sensitivity to physical discomfort.
However, it is important to interpret these findings cautiously. The number of participants reporting divorce or physical aggression was relatively small, which limits the precision of these estimates. Future studies with larger samples and longitudinal designs are needed to better understand the potential role of interpersonal stressors in shaping musicians’ physical and psychological health.
Although the study focused on orchestral musicians in Brazil, the findings may be relevant to other professional music environments where high performance demands coexist with limited occupational health support.
Associations with music performance anxiety and pain
The logistic regression analyses provided further insight into the relationships between stress exposure, music performance anxiety, and musculoskeletal pain outcomes. Female musicians had higher odds of presenting clinically significant MPA, and exposure to stress-producing life events, particularly financial problems and separation or divorce, was also associated with increased odds of MPA.
Importantly, clinically significant MPA was associated with higher odds of reporting musculoskeletal pain across multiple time frames. This finding suggests that psychological vulnerability may play a role not only in the perception of pain but also in its occurrence.
These results are consistent with previous studies indicating that psychological stress and anxiety are closely linked to musculoskeletal symptoms in musicians. Kenny and Ackermann (2015) 48 demonstrated that performance-related anxiety is associated with both musculoskeletal pain and depressive symptoms in professional orchestral musicians. Similarly, Baadjou et al. (2016) 15 identified psychosocial factors as important contributors to the development of playing-related musculoskeletal disorders.
Together, these findings suggest that anxiety-related processes, including heightened vigilance and maladaptive stress responses, may increase susceptibility to the occurrence of pain conditions in musicians.24,46
Music performance anxiety and pain severity
The multivariable linear regression models demonstrated that higher levels of music performance anxiety were consistently associated with greater pain intensity and greater pain-related interference, even after adjustment for demographic and occupational factors.
These findings extend the results of the logistic models by demonstrating that MPA is not only associated with the presence of musculoskeletal pain but also with its severity and functional impact. From a physiological perspective, anxiety is associated with increased muscle tension, altered motor control, and heightened autonomic arousal, which may contribute to inefficient movement patterns and increased mechanical strain during instrumental performance. 46
This interpretation is supported by previous literature indicating that psychological stress can amplify pain perception and functional limitation. Baadjou et al. (2016) 15 reported that psychosocial stressors are associated with increased severity of musculoskeletal symptoms in musicians. In addition, Kenny (2023) 46 highlights that MPA involves sustained physiological activation, which may lead to persistent muscle tension and increased biomechanical load during performance. Together, these mechanisms provide a plausible explanation for the observed association between higher anxiety levels and greater pain intensity and interference in the present study.
Biomechanical and physiological mechanisms of pain
In the present study, the most frequently reported pain regions included the left shoulder, right shoulder, lumbar region, and both hands. These areas are biomechanically vulnerable during instrumental performance due to sustained static postures, asymmetric loading, and repetitive upper limb movements required by many orchestral instruments. String players, who represented most of the sample, are particularly exposed to these biomechanical demands because of prolonged shoulder elevation, neck rotation, and fine motor control of the hands and fingers.
However, these anatomical patterns of pain may not be explained solely by biomechanical factors. Music performance anxiety is also known to produce physiological manifestations such as increased muscle tension and autonomic arousal, particularly in the cervical, shoulder, and upper limb musculature. 46 According to Kenny (2023), 46 MPA involves a complex interaction of cognitive, emotional, and physiological responses, which can lead to persistent muscular activation during performance situations.
Previous research has also highlighted the role of psychological stress in both the development and amplification of musculoskeletal pain among musicians. Baadjou et al. (2016) 15 and Kenny & Ackermann (2015) 48 reported that heightened psychological stress can contribute to sustained muscle contraction, reduced motor efficiency, and increased fatigue, potentially increasing the risk of playing-related musculoskeletal disorders. In this context, the pain distribution observed in the present study may reflect the combined effects of biomechanical load and stress-related physiological tension experienced during musical performance.
Strengths
This study presents several strengths that contribute to the understanding of occupational health among orchestral musicians. First, it focuses on professional musicians in Brazil, a population that remains underrepresented in international research on musicians’ health. By examining this context, the study contributes to expanding the geographic and socioeconomic diversity of the literature on performing arts medicine.
Second, the use of validated and culturally adapted instruments, including the MPIIQM-Br and the K-MPAI, strengthens the reliability of the measurements. These tools allowed the assessment of both the physical and psychological dimensions of musicians’ health using instruments with established psychometric properties within the Brazilian context.
Another strength of the study is the analytical approach adopted. By combining logistic regression analyses for pain occurrence with multivariable linear regression models for pain intensity and pain-related interference, the study was able to examine both the presence and the functional impact of musculoskeletal pain. This approach allowed a more nuanced understanding of how music performance anxiety and other factors relate not only to whether pain occurs, but also to the extent to which it interferes with musicians’ daily functioning and performance.
Limitations
Despite its contributions, this study has several limitations that should be considered when interpreting the findings. First, the cross-sectional design does not allow causal relationships to be established between musculoskeletal pain, music performance anxiety, and stress-producing life events. Although the associations observed are consistent with theoretical and empirical models suggesting reciprocal relationships between psychological stress and musculoskeletal symptoms, longitudinal studies are required to clarify the temporal direction of these relationships.
Second, the study relied exclusively on self-reported measures. Although the instruments used are validated and widely employed in research on musicians’ health, self-report data may be subject to recall bias or response bias. Future studies could benefit from incorporating objective assessments, such as clinical musculoskeletal evaluations, biomechanical measurements, or physiological markers of stress.
Another limitation relates to the sampling strategy. Only musicians holding permanent positions in orchestras were included in the study. While this criterion ensured a more homogeneous professional sample, it may limit the generalizability of the findings to freelance or temporary musicians, who may experience different occupational stressors and health risks.
Additionally, the study did not assess other potential psychological comorbidities, such as generalized anxiety or depressive symptoms. These conditions are known to co-occur with both chronic pain and performance anxiety and could contribute to the complex interaction between physical and psychological factors observed in musicians.
Finally, the study did not include qualitative data. Qualitative approaches, such as interviews or focus groups, could provide deeper insight into musicians’ lived experiences, institutional pressures, and cultural expectations within orchestral environments. Integrating qualitative and quantitative methods in future research may therefore offer a more comprehensive understanding of the multidimensional factors influencing musicians’ health.
Conclusion
This study demonstrates a high prevalence of musculoskeletal pain and music performance anxiety among Brazilian orchestral musicians. Higher levels of music performance anxiety were consistently associated with greater pain intensity and pain-related interference, even after adjustment for demographic and occupational factors. Female musicians and greater weekly playing hours were also associated with a greater functional impact of pain.
These findings highlight the importance of adopting an integrated occupational health perspective in orchestral settings, recognizing that musicians’ well-being is influenced by the interaction between physical workload, psychological stress, and socio-economic conditions. Future research should prioritize longitudinal and qualitative approaches to better understand the complex mechanisms underlying musicians’ health and to support the development of contextually relevant interventions in collaboration with musicians themselves.49,50 Ultimately, improving the health and well-being of orchestral musicians is essential not only for individual quality of life, but also for sustaining artistic performance and long-term professional careers within the music profession.
Footnotes
Acknowledgements
The authors would like to thank the artistic directors and the musicians of the participating orchestras for their availability, collaboration, and willingness to take part in this research.
Ethical considerations
The study was approved by the Research Ethics Committee of UNISUAM (ID 1.444.640/CAAE 51947215.6.0000.5235).
Consent to participate
All participants provided written informed consent, and anonymity was guaranteed. The first author, alongside another trained interviewer, administered the questionnaires in person.
Consent for publication
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.