
Abstract
Background
Self-reported musculoskeletal symptoms (SRMSs) are common occupational health problems, particularly among preschool teachers due to physical and psychosocial demands. However, data on their prevalence and associated factors in Turkey are limited to a few studies.
Objective
To investigate the prevalence of SRMSs and associated psychosocial factors among Turkish preschool teachers.
Methods
This cross-sectional study included 304 preschool teachers in Turkey. The Expanded Nordic Musculoskeletal Questionnaire was used to determine the prevalence of SRMSs in the previous 4 weeks (SRMSs-4w) and the previous 12 months (SRMSs-12m). Depression levels were assessed using the Beck Depression Inventory (BDI), quality of life was assessed using the Short Form-36 scale (SF-36), physical activity was assessed using the International Physical Activity Questionnaire-Short Form (IPAQ-SF), and sleep quality was assessed using the Pittsburgh Sleep Quality Index (PSQI).
Results
The prevalence of SRMSs-12m and SRMSs-4w among Turkish preschool teachers was 57.2% and 54.9%, respectively. SRMSs-12m and SRMSs-4w were most commonly reported in the neck (35.5% and 34.9%), lower back (34.9% and 32.2%), shoulders (30.3% and 26.6%), and upper back (25.7% and 20.7%). BDI, SF-36 (energy/fatigue, pain, general health), PSQI, and IPAQ-SF were independently associated with 4-week SRMSs, while BDI, SF-36 (pain, general health), and PSQI were independently associated with 12-month SRMSs (p < 0.05).
Conclusions
The results showed a high prevalence of SRMSs among Turkish preschool teachers. SRMS prevalence was highest in the neck, lower back and shoulder regions. Furthermore, this study demonstrated associations between depression levels, quality of life, sleep quality, physical activity level, and SRMSs in preschool teachers.
Keywords
Introduction
The term ‘musculoskeletal disorders’ (MSDs) is a broad designation covering a range of disorders and functional impairments affecting the musculoskeletal system, which mainly result in daily pain.1,2 MSDs involve injuries to the muscles, cartilages, nerves, tendons, and spinal discs, and common examples of such disorders include strains, back pain, plantar fasciitis, and tarsal tunnel syndrome.1–3 Work-related musculoskeletal disorders (WMSDs) are conditions, and are significantly influenced by environmental factors in terms of their development or exacerbation, and that are triggered by working conditions. 2 MSDs are serious multidimensional occupational complaints that affect working individuals due to various factors, such as sociodemographic and occupational characteristics. 4
The prevalence of MSDs and related symptoms among preschool teachers has been demonstrated to have a significant impact on their professional lives. This phenomenon is believed to be caused by unfavorable working conditions. 4 It has been reported that up to 95% of teachers may be affected by MSDs; this is a primary occupational health hazard leading to absenteeism, early retirement and a decline in quality of life. 5 The prevalence of MSDs in preschool teachers has been documented, with the most common afflictions being neck, shoulder, and lower back pain. 6 The risk factors linked with MSDs in preschool teachers include individual factors, such as chronological age, biomechanical factors (e.g., substantial physical loads, prolonged bending, and lifting positions), genetic factors, behavioral factors, and environmental factors (i.e., organizational work conditions).7–10 In addition to physical workload, psychosocial and organizational factors, including emotional demands, time pressure, job stress, and limited institutional support, have been increasingly recognized as important contributors to musculoskeletal symptoms among teachers.7–10 These factors may interact with physical strain, thereby contributing to the development and persistence of musculoskeletal symptoms in educational settings. Preschool teachers may be particularly vulnerable because of the combined physical and psychosocial demands inherent in their profession.7–10 The prevalence of MSDs among school teachers has been shown to be associated with a number of adverse consequences, including diminished quality of life, frequent absenteeism due to illness, functional impairments, reduced workdays, early retirement, disability, and increased health care expenditures.5–10 These factors can ultimately have a detrimental effect on the education system as a whole.5–10 Despite the high global burden of MSDs, there is a lack of national data on preschool teachers in Turkey. Therefore, this study aimed to determine the prevalence of self-reported musculoskeletal symptoms (SRMSs) among Turkish preschool teachers. Another objective of the study was to reveal the psychosocial factors associated with the prevalence of SRMSs among Turkish preschool teachers.
Materials and methods
Sample size calculation
The minimum sample size was estimated using the Cochrane formula for cross-sectional studies [n = (1.645)2×p × (1−p)/d2)], 11 where n is the minimum required sample size, p is the expected prevalence, and d is the margin of error of the study. A 90% confidence level, 5% margin of error, and expected SRMSs prevalence of 50% were used. 7 Therefore, the minimum sample size was 272 preschool teachers.
Participants
This descriptive cross-sectional study was conducted between October 2023 and November 2024 with 304 female preschool teachers working in public and private preschool institutions in Mersin, Turkey. Participants were recruited using convenience sampling through institutional contacts and voluntary participation. The study sample consisted of teachers who met the inclusion criteria and agreed to participate. The participants were between 20 and 65 years of age and had worked as preschool teachers for at least two years. Individuals with cardiopulmonary, neurological, systemic, or rheumatic diseases were excluded. This study was approved by Toros University Ethics Committee (protocol number 2023/14-09). All participants provided informed consent in the form of oral and written statements. This study was conducted in accordance with the principles of the Declaration of Helsinki.
Assessments
All participants were evaluated by a physiotherapist with a doctorate in orthopedic rehabilitation and 19 years of experience. Detailed information regarding these evaluations is provided below. The selected measurement instruments were chosen based on their widespread use, established validity, and reliability in occupational health research.11–15 These instruments are commonly employed to assess key dimensions relevant to musculoskeletal symptoms, including psychological distress, sleep quality, physical activity, and quality of life. Evaluating these factors together provides a comprehensive framework for understanding the multifactorial nature of musculoskeletal symptoms in preschool teachers.
Demographic data
The initial section of the evaluation form documented the participants’ sex, age, height, weight, marital status, number of children, history of previous surgeries, systemic diseases, physical traumas, and pregnancy status. Furthermore, the following variables were recorded.
the school where the subjects were employed, class age group months (0–36 months, 37–48 months, 49–60 months, 61–72 months) student per class (0–10, 11–20, 21 ≤ number of children) school (governmental, private) institution (divided into independent kindergarten, kindergarten, private nursery and private kindergarten), the duration of experience in the profession, the duration of employment in the current workplace, the number of days and hours of work per week, the school and educational status of the graduates, satisfaction with their job, the duration of standing and sitting-resting times in the institution where they were employed.
Assessment of prevalence of SRMSs
The Expanded Nordic Musculoskeletal Questionnaire is a 27-item instrument designed to assess the presence of SRMSs in the last 4 weeks (SRMSs-4w) and 12 months (SRMSs-12m), encompassing nine distinct anatomical regions. In this form, participants were asked to indicate whether they were experiencing pain, their age when the pain first began, the status of hospitalization and changes in tasks due to pain, and whether they had encountered pain problems in the past week, month, or year. Additionally, they were surveyed whether the pain impacted their home or work life, if they had consulted a doctor or physiotherapist, and whether they had taken reports due to painkiller use. 11
Assessment of the depression levels
The Turkish version of the Beck Depression Inventory (BDI), which has been demonstrated to be valid and reliable, 12 was used to ascertain the depression levels of the study participants. The scale comprises 21 headings, each accompanied by four options. Respondents were instructed to answer based on their personal experience.
Quality of life assessment
The Short Form (SF-36) scale, a tool employed for the assessment of quality of life, comprises 36 items pertaining to the general concept of health and is not disease-specific. The scale encompasses eight subdimensions: general health, function, social function, physical role limitation, mental health, emotional role limitation, body pain, and vitality. Each subdimension ranges from 0 to 100, with higher scores indicating a higher quality of life. Higher scores indicate better quality of life related to general health status, whereas lower scores indicate a worse general health status. 13
Physical activity assessment
In this study, the International Physical Activity Questionnaire-Short Form (IPAQ-SF), which consists of seven items, including activities in the last seven days, was used to assess the level of physical activity of the participants. This scale includes items that assess the frequency and duration of physical activity in three intensity ranges. The questionnaire results in a score in terms of “MET minutes/week” multiplied by minutes, days, and metabolic equivalents (MET). The walking score was calculated by multiplying the walking time in minutes by a constant of 3.3 METs. A value of 4 METs was assigned for moderate activity, whereas 8 METs were designated for vigorous activity. 15
Sleep assessment
The Pittsburgh Sleep Quality Index (PSQI) was used to assess the participants'sleep quality. The PSQI is a 19-item questionnaire that assesses patients’ sleep during the previous month. The PSQI has seven subcomponents: subjective sleep quality, sleep latency, sleep efficiency, sleep duration, sleep disturbance, sleep medication use, and daytime dysfunction. Each component is scored on a 0–3 point scale, and the total score ranges from 0 to 21. Higher scores indicate poor sleep quality. 14
Statistical analysis
We conducted statistical analyses using the Statistical Package for Social Science v21.0 (SPSS Inc., Chicago, IL, USA). We checked the normality of the quantitative data using the Kolmogorov–Smirnov test. Qualitative variables are presented as percentages (%), and numeric parameters are presented as medians and quartile intervals. Logistic regression analyses were conducted to evaluate the association between each independent variable and the presence of SRMSs. The independent variables included sociodemographic characteristics (age, body mass index, and marital status), occupational factors (working hours, professional experience, type of institution, and number of students per class), and psychosocial and health-related variables (BDI, SF-36 subscales, IPAQ-SF, and PSQI scores). Multicollinearity among independent variables was assessed using the variance inflation factor (VIF) obtained from a linear regression model. Variables with high multicollinearity (VIF > 5), particularly those representing similar constructs (e.g., weight, height, and body mass index), were not included in the final model. The body mass index (BMI) was retained because of its clinical relevance. The final model was constructed to ensure the parsimony and stability. The results are presented as adjusted odds ratios (ORs) with 95% confidence intervals (CIs). The level of confidence was set at P < 0.05.
Results
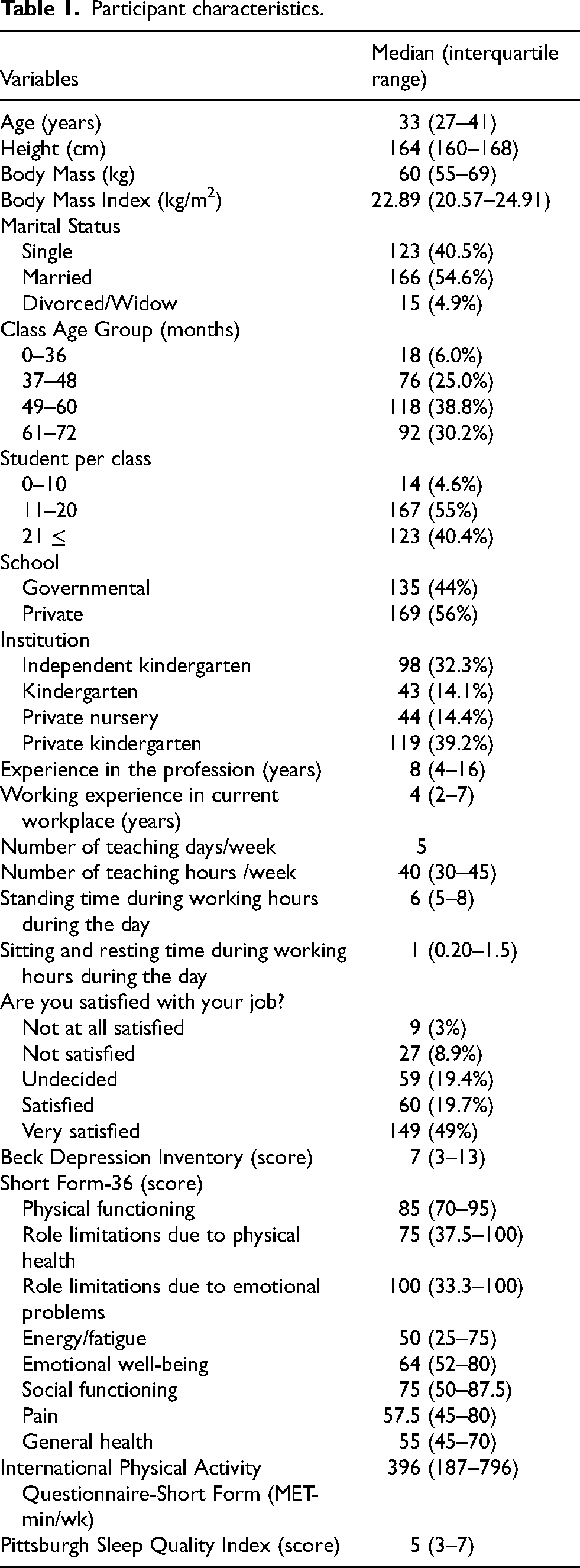
Sociodemographic data are presented in Table 1.
Participant characteristics.
A total of 54.9% of preschool teachers reported the presence of SRMSs in at least one anatomical region within the previous four weeks. Furthermore, 57.2% of preschool teachers reported SRMSs in at least one anatomical region in the last 12 months. SRMSs-4w and SRMSs-12m were most commonly reported in the following anatomical regions: neck (34.9% and 35.5%), lower back (32.2% and 34.9%), shoulders (26.6% and 30.3%), upper back (20.7% and 25.7%), elbows (5.9% and 11.8%), wrists (12.2% and 18.4%), hips/feet (13.5% and 17.1%), knees (19.1% and 22.7%), and ankles/feet (21.1% and 25.7%) (Figure 1).
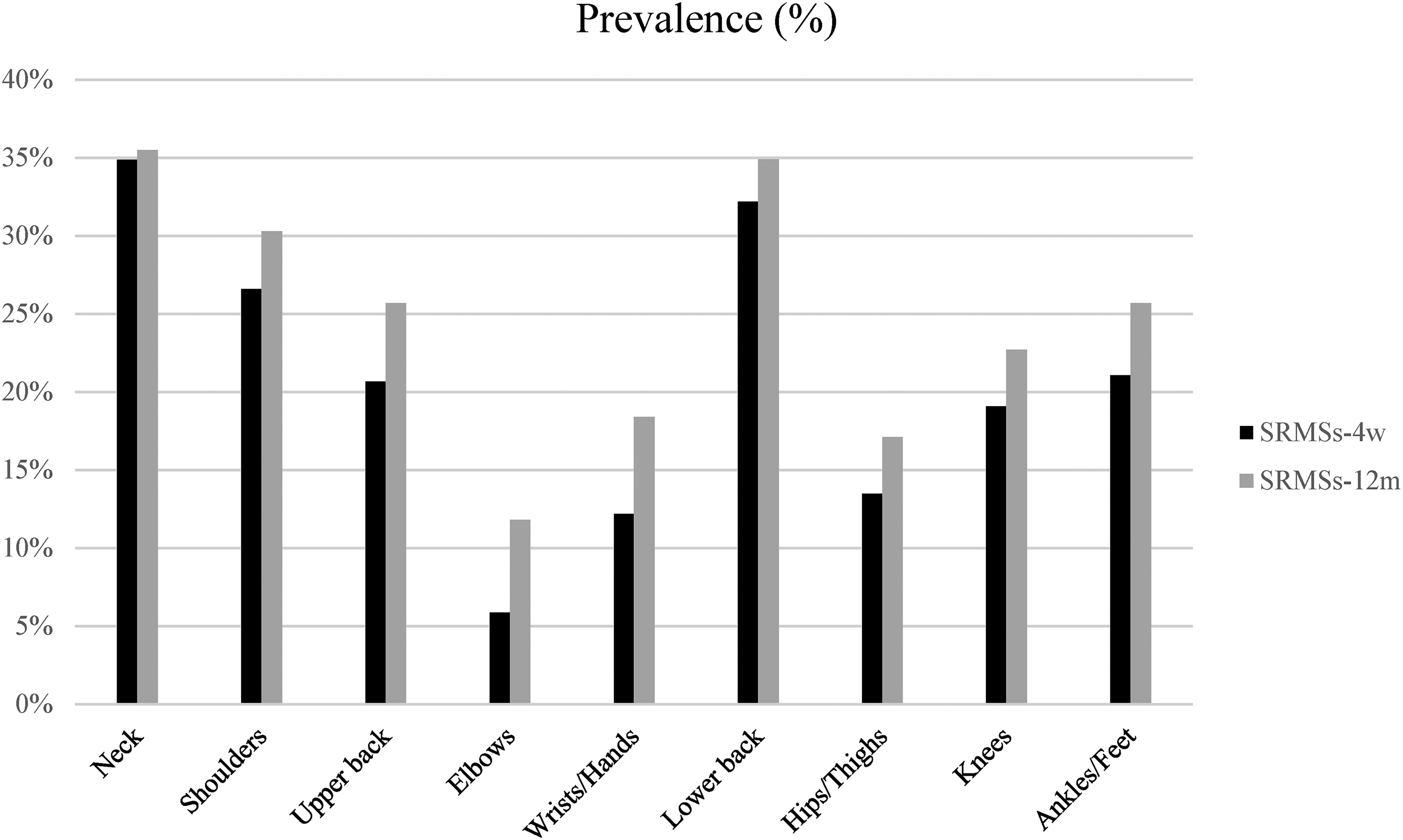
Prevalence of SRMSs in body regions (SRMSs-4w: SRMSs during the last 4 weeks; SRMSs -12m: SRMSs during the last 12 months).
The Hosmer-Lemeshow values obtained for factors associated with SRMSs-4w (p = 0.297) and SRMSs-12m (p = 0.228) as a result of the logistic regression analysis using the parameters evaluated in preschool teachers indicated that the applied model was a good fit. The results of the study demonstrated that scores on the BDI (p = 0.003), SF-36 Energy/Fatigue (p = 0.013), SF-36 Pain (p < 0.001), SF-36 General Health (p = 0.001), PSQI (p = 0.042), and IPAQ-SF (p = 0.013) were independently associated with SRMSs-4w among preschool teachers. BDI (p = 0.001), SF-36 Pain (p = 0.011), SF-36 General Health (p = 0.018) and PSQI (p = 0.040) scores were independently associated with SRMSs-12m among preschool teachers. The investigation further revealed that other evaluated parameters failed to demonstrate statistical significance in predicting SRMSs among this demographic (p > 0.05) (Tables 2 and 3).
Logistic regression analysis of associated factors with SRMSs in the last 4 weeks.
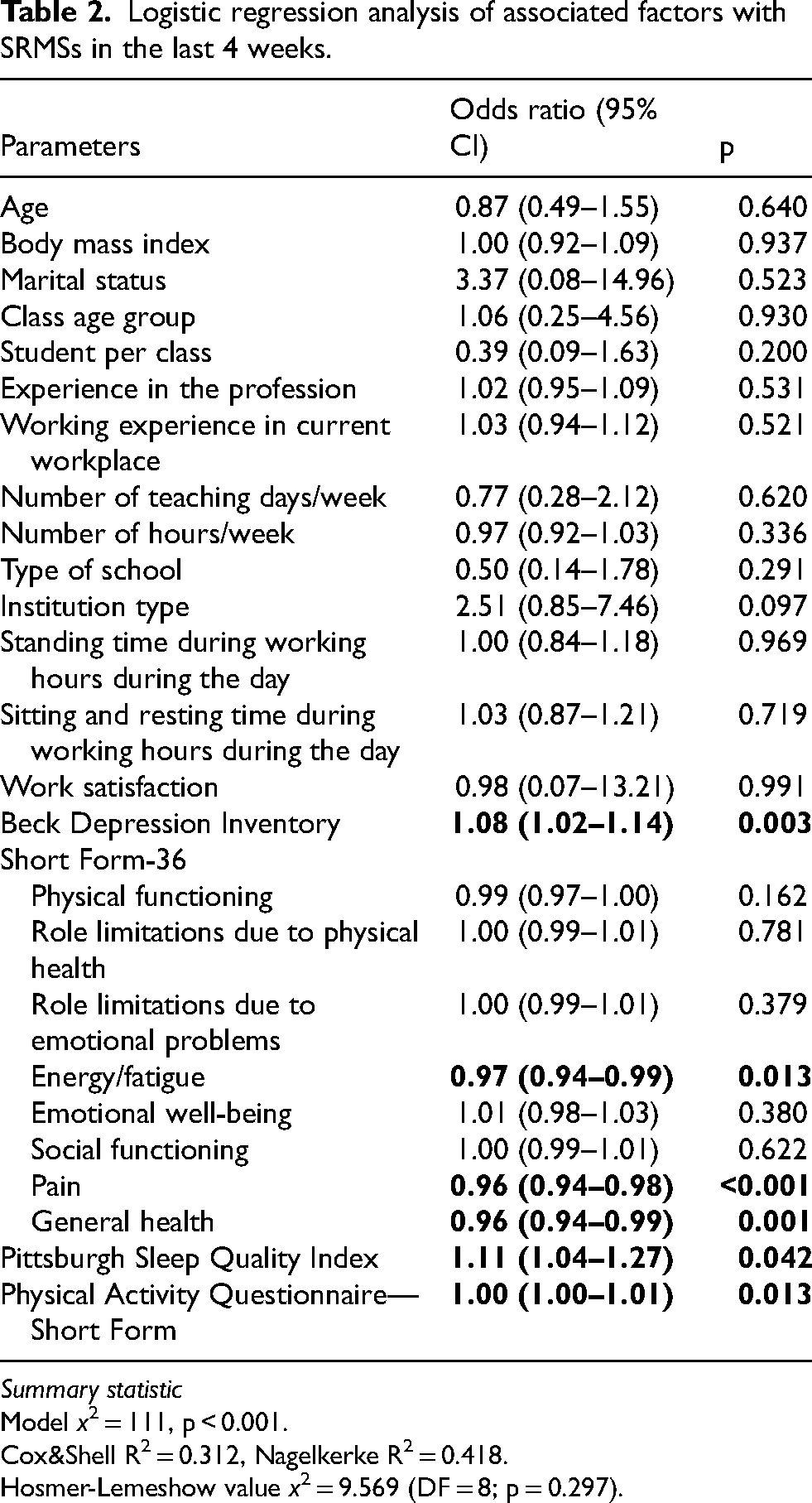
Summary statistic
Model x2 = 111, p < 0.001.
Cox&Shell R2 = 0.312, Nagelkerke R2 = 0.418.
Hosmer-Lemeshow value x2 = 9.569 (DF = 8; p = 0.297).
Logistic regression analysis of associated factors with SRMSs in the last 12 months.
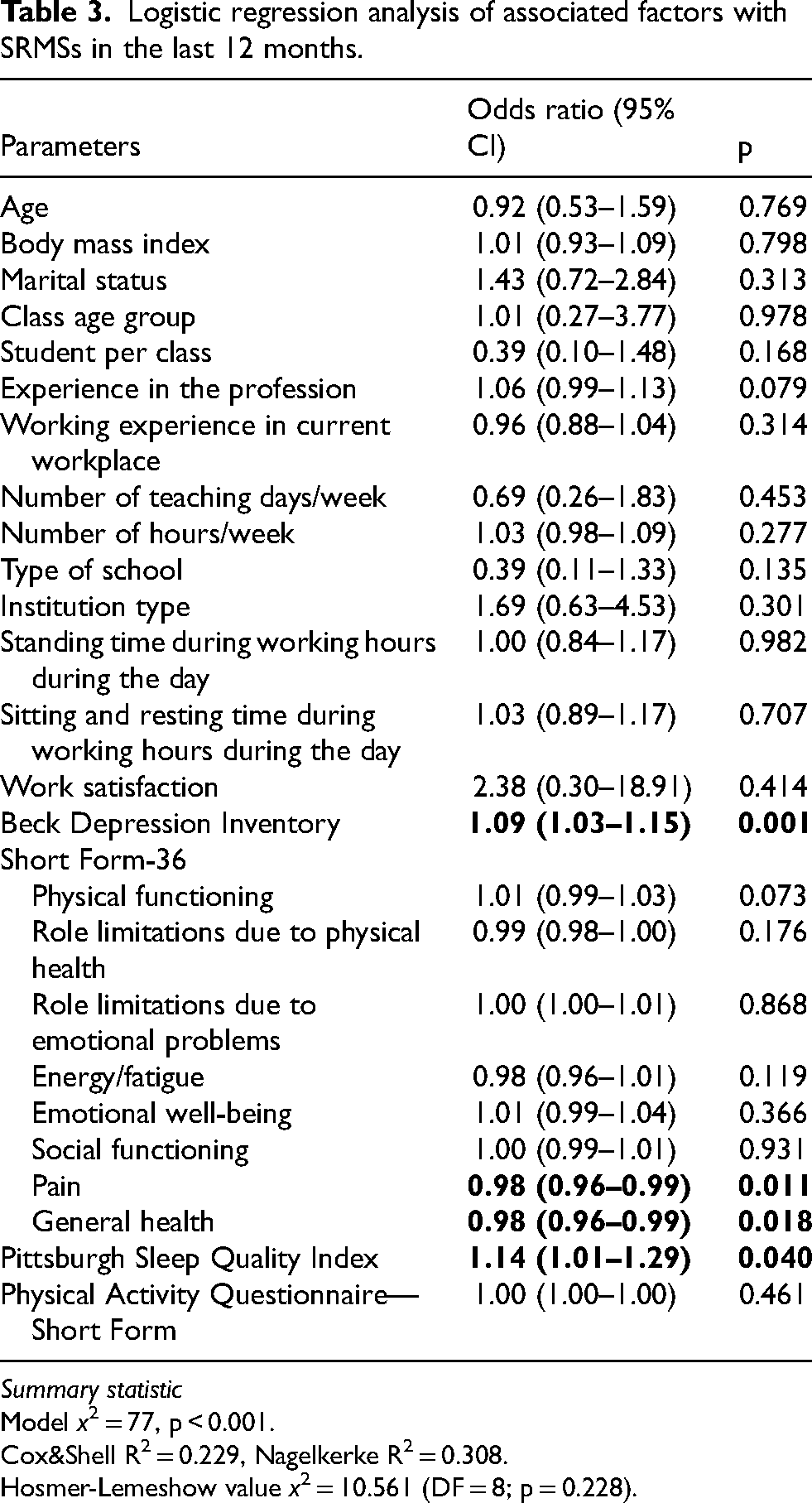
Summary statistic
Model x2 = 77, p < 0.001.
Cox&Shell R2 = 0.229, Nagelkerke R2 = 0.308.
Hosmer-Lemeshow value x2 = 10.561 (DF = 8; p = 0.228).
Discussion
This is the first study to examine SRMSs prevalence-12m and SRMSs-4w in a sample of Turkish preschool teachers. This study examined the prevalence of SRMSs in preschool teachers and the factors contributing to this phenomenon. The distinction between short-term (4-week) and long-term (12-month) musculoskeletal symptom patterns may provide additional insight into the nature of musculoskeletal symptoms among preschool teachers. While short-term symptoms may reflect recent physical strain or temporary workload-related factors, long-term symptoms may indicate persistent or chronic musculoskeletal conditions. Therefore, monitoring both short- and long-term symptom patterns may be important for identifying early risk factors and developing effective preventive strategies in preschool educational settings. The prevalence of SRMSs-12m and SRMSs-4w among Turkish preschool teachers was 57.2% and 54.9%, respectively. As indicated by the SRMSs-12m and SRMSs-4w data, the prevalence of SRMSs was highest in the neck, lower back and shoulder regions. The results of the logistic regression analysis conducted in this study indicate that sleep quality, physical activity, depression, and quality of life levels were independently associated with musculoskeletal symptoms experienced by preschool teachers.
The study found that the prevalence -12m and SRMSs-4w among Turkish preschool teachers was 57.2% and 54.9%, respectively. Furthermore, the highest prevalence of SRMSs among Turkish preschool teachers was in the neck (34.9% in the last 4 weeks and 35.5% in the last 12 months), shoulders (26.6% in the last 4 weeks and 30.3% in the last 12 months), and lower back (32.2% in the last 4 weeks and 34.9% in the last 12 months). The higher prevalence of SRMSs among preschool teachers may be associated with emotional, biomechanical, and environmental risk factors related to their work conditions. The role of a preschool teacher necessitates constant interaction with children who are active (sometimes excessively so), spontaneous, impulsive, and heavy (sometimes to a considerable degree). 16 Moreover, preschool teachers frequently need to bend, lift, or carry children and sit on the floor or small furniture to care for, play with, and encourage interaction with them. All the above-mentioned factors (especially in the load-bearing neck, shoulder, and lumbar regions) can cause increased loads on the musculoskeletal system, which may lead to musculoskeletal disorders over time. Numerous studies have examined the prevalence of SRMSs in preschool teachers; however, the results have varied. This finding is consistent with that of Pirbalouti et al. 7 Among a sample of 105 female preschool teachers in Iran, lower back pain was the most prevalent site of pain, with a prevalence of 30.5%, followed by neck pain (27.6%) and shoulder pain (27.6% for the right side and 25.7% for the left side). Moreover, Vega-Fernandez et al. 17 identified pain sites among 105 female preschool teachers in South America as the lower back (30.5%), neck (27.6%), right shoulder (27.6%), and left shoulder (25.7%). Converso et al. 9 reported that the prevalence of SRMSs was 55.5% in Italian preschool teachers, with upper back pain being the most prevalent site of pain (75.6%), followed by neck pain (70.6%) and lower back pain (56.3%). Randall et al. 10 indicated that the prevalence of SRMSs was 66.6% among preschool teachers. Among them, 55% reported experiencing headaches, while 52.3% reported back pain. This was followed by knee pain (29%), neck pain (28.2%), and shoulder and hand/wrist pain (22.5% each). 10 Different SRMSs prevalence values reported in preschool teachers indicate that cultural and regional differences may also play a role in the development of musculoskeletal disorders.
The results of the logistic regression analysis indicate that depression, selected quality of life domains (energy/fatigue, pain, and general health), sleep quality, and physical activity level were independently associated with SRMSs in the last four weeks. For SRMSs in the last 12 months, only depression, pain, general health domains of quality of life, and sleep quality remained as independent associated factors, whereas physical activity level was not statistically significant. These findings can be attributed to the complex interactions between psychological, behavioral, and physiological mechanisms. For instance, depression and psychological distress may increase muscle tension, alter pain perception, and reduce coping capacity, thereby contributing to the development or persistence of musculoskeletal disorders.3,7,18–20 Poor sleep quality may exacerbate these conditions by impairing physical recovery and increasing fatigue.3,7 Additionally, our results suggest that increased physical activity, specifically related to occupational demands, is associated with a higher prevalence of SRMSs among Turkish preschool teachers. While the general relationship between physical exertion and SRMSs has been documented,3,17–20 the unique working environment of preschool teachers may render physical activity more taxing, leading to cumulative strain on the musculoskeletal system. Given the pivotal role these educators play in early childhood development, mitigating factors that diminish their work efficiency is essential for both individual well-being and societal productivity. These findings align with the broader occupational context in which supportive organizational practices and healthy work environments influence both psychological and physical health outcomes. Psychosocial and organizational factors are crucial in shaping employee well-being.7–10 In line with this, recent research highlights that employee motivation and quality organizational relationships are key determinants of sustainable performance and well-being in demanding work environments, 21 further underscoring the importance of institutional support structures in mitigating musculoskeletal risk among preschool teachers. Recent international studies have similarly highlighted how psychosocial stressors and occupational demands contribute to musculoskeletal symptoms in teaching professions.3,7,18–20 For example, Pirbaloutia et al. 7 found a significant relationship between depression and SRMSs in kindergarten workers, whereas Randall et al. 10 noted that elevated physical job demands and perceived stress were associated with an increased likelihood of SRMSs. Similarly, Yamamoto-Kataoka et al. 20 identified that advanced age, awkward postures, and high psychological job demands were precursors of low back pain in nursery teachers. A multi-faceted approach is required to reduce the prevalence of SRMSs among preschool teachers. Individual-level interventions should focus on improving sleep quality and psychological well-being of the teachers. However, organizational-level strategies are equally critical, including ergonomic improvements (e.g., child-sized furniture adjustments and appropriate workspaces) and structural changes to reduce physical strain, such as increasing recess times or providing assistant teachers in each classroom. Reflective professional development practices may also play a supportive role in addressing occupational health challenges. Collaborative reflection models have been proposed as a means of enhancing professional knowledge-building and role awareness among educators, which may indirectly contribute to healthier work practices and reduced occupational strain. 22 Furthermore, future occupational health strategies should integrate digital and technology-supported tools to monitor workload and enhance ergonomic awareness, provided they are implemented in an ethical, worker-centered manner. Ultimately, fostering institutional support and clarifying role expectations will help reduce psychosocial risks and create a more sustainable work environment for preschool teachers.
Limitations
This study had several limitations. First, it employed a cross-sectional design conducted at a single time point; therefore, causal relationships could not be inferred. In addition, this design limits the ability to determine the temporal sequence between exposure and outcome variables, which may obscure the potential causal pathways. Second, medical confirmation of musculoskeletal disorder diagnoses was not obtained. Most parameters were assessed using self-report measures, which may introduce reporting bias, including recall bias and social desirability bias, potentially affecting the accuracy of the data. Furthermore, reliance on subjective measures may lead to either overestimation or underestimation of symptoms and risk factors. Third, ergonomic evaluations were not performed using objective measurements. The application of objective methods to ergonomic evaluations in the field of education has the potential to enhance the identification of risk factors associated with SRMSs among preschool teachers in the future. Fourth, all participants were female preschool teachers recruited through convenience sampling from a single city (Mersin, Turkey). While this reflects the predominant gender distribution of the preschool teaching workforce in Turkey, it substantially limits the external generalizability of the findings. The results may not be representative of male preschool teachers, teachers from other geographical regions of Turkey, or those working in different cultural or socioeconomic contexts. Future studies employing random sampling strategies across multiple cities and including both genders are warranted to confirm and extend these findings.
Conclusion
This study revealed a high prevalence of SRMSs among Turkish preschool teachers, with 12-month and 4-week prevalence rates of 57.2% and 54.9%, respectively, predominantly affecting the neck, shoulders, and lower back. These findings suggest that depression, sleep quality, and specific quality of life domains represent consistent correlates of SRMSs regardless of the time frame assessed, while physical activity level showed an association limited to the four-week period. To address these challenges, early childhood education systems must transition toward prevention-oriented policies that mandate ergonomic workplace standards, such as providing child-appropriate furniture and optimizing workspace designs, alongside organizational adjustments, such as reducing physical workload through increased recess periods or the assignment of assistant teachers. Furthermore, the study highlights critical implications for training; it is essential for educational institutions to integrate comprehensive programs focusing on ergonomic awareness, stress management, and healthy lifestyle practices into their professional-development curricula. By synthesizing policy-level interventions with structured training and supportive work environments, education systems can effectively mitigate musculoskeletal risks, thereby safeguarding teachers’ well-being and ensuring the long-term quality and sustainability of early childhood education.
Footnotes
Ethical approval
This study was approved by the Ethics Committee of Toros University (Protocol Number: 2023/14-09).
Informed consent
A signed informed consent form was obtained from the participants.
CRediT authorship contributions statement
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.