
Abstract
Background
Surgeons face elevated risks of musculoskeletal disorders due to prolonged operating times, awkward postures, and repetitive tasks, which can impair performance and well-being. Microbreaks have emerged as a potential ergonomic intervention to reduce discomfort and fatigue during surgery.
Objective
The main goal of this study was to investigate and compare the intraoperative usability and effectiveness of two break scheduling strategies using the OR-StretchTM Web-App. Furthermore, surgeons’ feedback on the primary barriers to implementation of the OR-Stretch Web-App was recorded.
Methods
This study used a randomized, within-subjects crossover design. Fourteen surgeons (eight females) performed three surgical procedures with the following microbreak schedules; (1) microbreaks every 30 min with an optional ten-minute snooze (Break-30), (2) microbreaks every 60 min with an optional ten-minute snooze (Break-60), or (3) no microbreaks (Baseline). Outcomes were measured using self-reported subjective surveys (e.g., discomfort, fatigue, workload, and usability).
Results
Surgeons found both Break-30 and Break-60 conditions aided physical performance, mental focus, body pain/discomfort, and level of fatigue (self-reported improvement between 28.6% and 78.6%). No significant differences were observed in surgeons’ subjective evaluations of the Break-30 and Break-60 conditions; however, the data suggest that Break-60 is preferable to the Break-30 condition.
Conclusions
This study provides evidence supporting the OR-Stretch Web-App as a potential surgical ergonomic intervention. However, enhancing the Web-App's user-friendliness and developing strategies to synchronize microbreaks with appropriate times during surgeries, to avoid disrupting the surgical workflow, are critical areas for future studies.
Keywords
Introduction
The high prevalence of musculoskeletal problems has become a widespread health concern in a multitude of industries.1–3 This issue has especially impacted surgeons, with many suffering from work-related musculoskeletal symptoms worldwide4–11 that can be exacerbated as they continue to operate. 12 Long hours in awkward postures, 8 repetitive motions, and high-force exertions increase surgeons’ risk of work-related musculoskeletal disorders (WMSDs), particularly in their back, neck, and shoulder areas.8,9,13 They may include conditions such as degenerative spine disease, thoracic outlet syndrome, tension neck syndrome, tendinitis, and carpal tunnel syndrome.13,14 This can affect not only surgeons’ quality of life but also their ability to perform optimally in the operating room (OR). 15 Increased time away from the OR and economic and societal problems are other consequences of surgeons’ WMSDs.10,15–17
An increasing number of studies are evaluating surgical ergonomics across different surgical modalities, including open,18,19 laparoscopic,20–23 and robotic surgery.24–27 Considering that surgeons play a crucial role in performing medical procedures, improving their working conditions would contribute to improved patient safety and healthcare quality. 8 Although most surgeons experience musculoskeletal problems, fewer than 30% seek medical treatment or intervention for these issues. 9 Various ergonomic interventions such as anti-fatigue mats, body supports, training, and OR setup adjustments (e.g., adjusting monitor heights) have been attempted. However, many of these strategies have not been shown to sufficiently mitigate musculoskeletal symptoms.9,28–31 One promising intervention is intraoperative microbreaks to reduce ergonomic risks.32–35 This intervention originally consisted of short (1.5–2 min) researcher-guided calisthenic exercises performed in the sterile field during appropriate surgical pauses.34–36 These intraoperative microbreaks were then prompted through the use of a web application (OR-Stretch Web-App), which helped reduce physical pain, discomfort, and fatigue, and improve mental focus with minimal disruption. 37
Sarker et al. (2021) showed that alternative break scheduling strategies can have different effects on muscular fatigue and discomfort. Frequent microbreaks (every 10–20 min) prevented neck muscle fatigue and discomfort during static flexion postures, whereas less frequent breaks showed no preventive effect. 38 Despite this physical benefit, more frequent microbreaks may cause distractions and negatively affect the workflow inside the OR. Both usability and acceptability of the OR-Stretch are key factors that should be balanced. Thus, it is necessary to evaluate different break scheduling strategies to find the strategy that will maximize physical improvements and acceptability while minimizing cognitive burdens and usability issues.
The OR-Stretch™ Web-App is a free tool that prompts short (70-s) guided intraoperative stretching microbreaks in the sterile field to help reduce discomfort and fatigue. 36 The aim of this study was to evaluate the usability and effectiveness of two intraoperative microbreak scheduling strategies using the OR-Stretch Web-App and to gather surgeons’ feedback regarding barriers and facilitators to implementation. To the best of our knowledge, OR-Stretch is currently the only application specifically designed to facilitate active intraoperative microbreaks within the sterile field. Its use in this study also enables continuity with prior investigations evaluating the feasibility and ergonomic impact of intraoperative microbreak interventions.
Method
Participants
Attending surgeons from a large quaternary academic hospital system participated in this study. This study was approved by this hospital's institutional review board (IRB). Oral consent was obtained from all participants. The surgeons’ primary specialties included breast and melanoma surgical oncology, colon and rectal surgery, gynecologic surgery, hepatobiliary and pancreas surgery, thoracic surgery, and vascular surgery.
Experimental procedure
Each surgeon met with the research team to become familiar with the experimental procedure and select appropriate surgical procedures for incorporating intraoperative stretching microbreaks. Surgical procedures with expected durations of two hours or longer that had participants performing at least half of the surgical procedure were targeted. The surgeons’ schedules were screened for their chosen surgical procedures throughout the data collection period. Prior to each surgical procedure, the appropriateness of the surgical day was again confirmed with the surgeons.
The OR-Stretch™ Web-App (ORStretch.mayoclinic.org) was used for conducting intraoperative microbreaks in this study. OR-Stretch is a web application designed by the Human Factors Engineering Laboratory at Mayo Clinic (Mayo Clinic, Rochester, Minnesota, USA) to help surgeons and surgical teams conduct intraoperative stretching moves. The OR-Stretch Web-App allows users to schedule microbreak reminders with a frequency ranging from every 30 to 120 min in 15-min increments (e.g., every 45 min or 90 min). When the alarm (harp) sounds, the surgeon and surgical teams are prompted to follow a 70-s video to perform the stretching moves. Participants do not break the sterile field to perform the stretches while either seated or standing. Additionally, a snooze button can delay the microbreak by five minutes, with the option to increase the delay in five-minute intervals, up to a maximum of 40 min. In this study, only the attending surgeon was asked to perform the stretching moves while the rest of the surgical team could choose whether to participate and were not queried. Additionally, to control the impacts of potential confounders in this study, the stretches were always performed while standing, and the snooze was set at 10 min, when used.
Each surgeon performed three cases of their selected surgical procedure including, (1) taking the OR-Stretch breaks every 30 min with an optional 10-min snooze (Break-30), (2) taking the OR-Stretch breaks every 60 min with an optional 10-min snooze (Break-60), or (3) taking no OR-Stretch breaks (Baseline). The order of these three conditions was randomly assigned to surgical procedures for each surgeon. Thus, this study used a randomized, within-subjects crossover design where each surgeon completed three surgical procedures, one under each condition (Baseline, Break-30, Break-60). During trials where OR-Stretch was used (Break-30, and Break-60 conditions), an experimenter was present in the OR to support the usage of OR-Stretch on an OR computer.
Data collection instrumentation
Participants were asked to complete the following surveys:
Demographics: On the first day of data collection, participants completed a single demographic survey including questions about their age, gender, height, weight, primary specialty, and post-residency surgical experience. Intraoperative discomfort and fatigue: Participants were asked to complete a modified NORDIC body part discomfort and overall fatigue survey before and after each surgical procedure.39,40 This survey recorded participants’ levels of discomfort in the neck, shoulders, upper back, lower back, wrists/hands, knees, ankles/feet (from 0 = “no discomfort” to 10 = “significant discomfort”) and overall fatigue (from 0 = “no fatigue” to 10 = “extremely fatigued”). The difference between post-surgical and pre-surgical scores was calculated for each body part and overall fatigue. These differences in the scores were used as intraoperative body part discomfort and overall fatigue scores. Intraoperative workload: A workload survey based on NASA-TLX, SURG-TLX, and a question from Global Operative Assessment of Laparoscopic Skills (GOALS)41–43 was used after each surgical procedure. This survey evaluated workload subscales including mental demands, physical demands, temporal demands, task complexity, situational stress, distractions, effort, frustration, and degree of difficulty (all from 0 = “very low” to 20 = “very high”) and performance (from 0 = “failure” to 20 = “perfect”). OR-Stretch evaluation: On the days with OR-Stretch (Break-30 and Break-60 conditions) participants completed an OR-Stretch evaluation survey. It recorded the distractive effects of the stretching exercises on performing or assisting in the surgical procedure (from 0 = “no impact” to 20 = “extremely distracting”), the negative impact of the stretching exercises on the flow of the surgery (from 0 = “no impact” to 20 = “extreme impact on the flow”), and the intraoperative impacts of OR-Stretch microbreaks on the participants’ physical performance, mental focus, body pain/discomfort, and level of fatigue (5-level scale (“much worse,” “worse,” “no change,” “better,” “much better”). A question also recorded participants’ feedback on their desired frequency of taking breaks for that specific surgical procedure (5-level scale from “many fewer breaks” to “many more breaks”). The final question recorded participants’ feedback regarding the main barrier(s) to using OR-Stretch microbreaks inside their OR.
The experimenter also recorded the frequency and duration of actual breaks and alarm snoozes throughout the surgery. Additionally, the skin-to-skin surgical duration of each procedure was extracted from the electronic health record. The number of OR-Stretch microbreaks performed was divided by the number of all possible OR-Stretch microbreaks during a surgical procedure, then multiplied by 100 to calculate “break compliance percentages” for each surgical procedure. Similarly, the number of times that the OR-Stretch microbreak was snoozed was divided by the number of all possible OR-Stretch microbreaks during a surgical procedure, then multiplied by 100 to calculate “snooze utilization percentages” for each surgical procedure.
Post-study usability and overall feedback survey: At the conclusion of the study, participants were asked to complete a modified Standard Usability Scale (SUS) survey44,45 with the ten questions all on a five-level scale (from “strongly disagree” to “strongly agree”). A few additional questions also recorded participants’ feedback on the implementation of OR-Stretch and future research. Participants were asked to rank and comment on four potential strategies that would improve compliance with OR-Stretch: (1) being able to verbally control OR-Stretch, (2) being able to control OR-Stretch using a touchscreen tablet (covered with a sterilized layer) housed by the operative table, (3) having the circulating nurse be responsible for setting up and controlling OR-Stretch, or (4) using a poster describing the stretching moves and an alarm clock instead of the OR-Stretch Web-App. It should be noted that the participants could choose equal ranks for two or more options. Another question compared setting up a pre-defined alarm (e.g., every 30 or 60 min) with taking OR-Stretch breaks at natural transitions during a surgical procedure. The final questions recorded the participants’ overall feedback on the OR-Stretch Web-App, the stretching exercises, and the main barriers to using OR-Stretch microbreaks inside the OR. Figure 1 illustrates a flow diagram of the study design and data collection procedure for clarity.
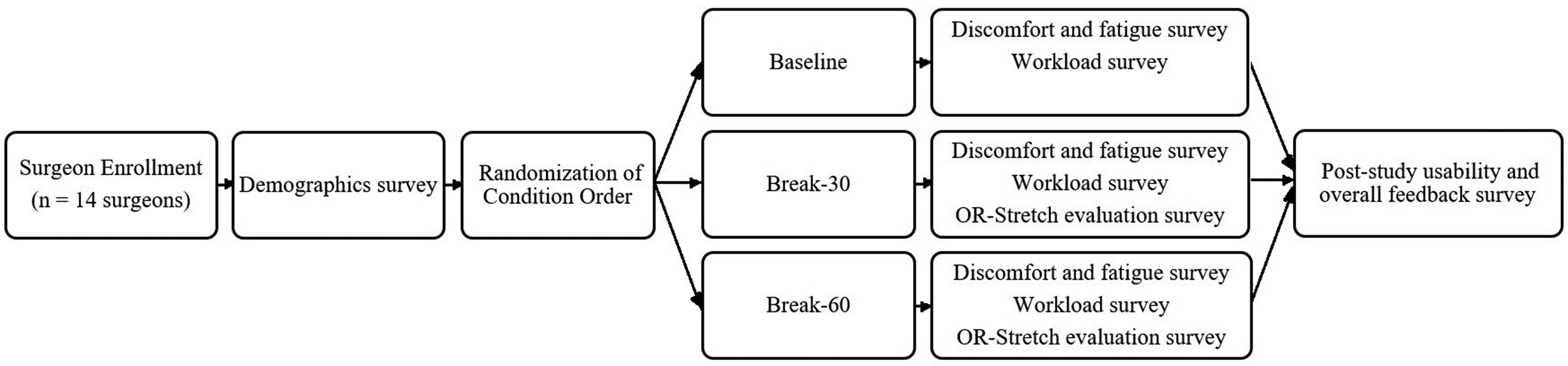
Flow diagram of the study design and data collection procedure.
Statistical analysis
A full factorial model considering OR-Stretch condition (“Break-30,” “Break-60,” and “Baseline”), surgical duration (short and long surgical procedures based on the median duration of all surgical procedures (SHORT and LONG)) and their interaction was performed to evaluate the effects of these factors on surgeons’ body part discomfort, overall fatigue, and workload subscales. If the effect of an OR-Stretch condition on a variable was significant, a post-hoc Tukey test was used for pairwise comparisons among “Break-30,” “Break-60,” and “Baseline”. A similar approach was used to investigate the effects of OR-Stretch condition (“Break-30,” “Break-60”), surgical duration (SHORT and LONG), and their interaction on the results of OR-Stretch evaluation questions and break compliance and snooze utilization. The statistical analyses were conducted using JMP 16.2.0 software package (SAS, Cary, NC). For all the statistical analyses in this study, the significance level of 0.05 was considered.
Results
Demographics
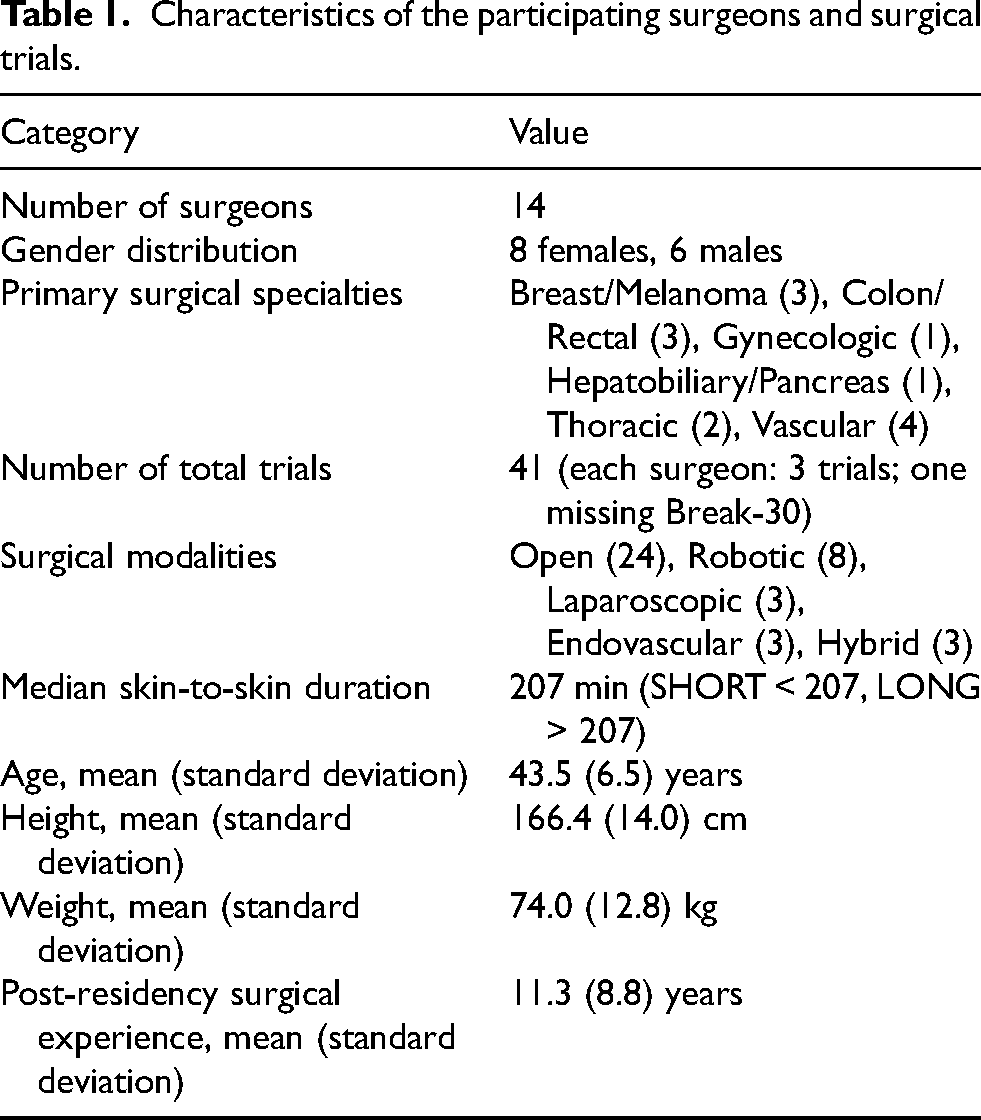
Fourteen surgeons (eight females, six males) participated in this study, performing three trials each for a total of 41 trials. One male surgeon did not complete the “Break-30” condition as the matched surgical procedure with Baseline and Break-60 conditions did not occur during the data collection time limit. The participants’ primary surgical specialties included breast and melanoma surgical oncology (three surgeons), colon and rectal surgery (three surgeons), gynecologic surgery (one surgeon), hepatobiliary and pancreas surgery (one surgeon), thoracic surgery (two surgeons), and vascular surgery (four surgeons). The surgical modalities were 24 open cases, 8 robotic cases, 3 laparoscopic cases, 3 endovascular cases, and 3 hybrid cases. The median duration of all surgical procedures was 207 min; surgical procedures longer than the median (207 min) were categorized as LONG, while shorter cases were categorized as SHORT procedures. The mean (M) and standard deviation (SD) of the participants’ anthropometrics were age 43.5 (6.5) years, height 166.4 (14.0) cm, weight 74.0 (12.8) kg, and post-residency surgical experience 11.3 (8.8) years. Table 1 summarizes the characteristics of the participating surgeons and surgical trials.
Characteristics of the participating surgeons and surgical trials.
Intraoperative body part discomfort and fatigue
The full factorial analysis showed that the OR-Stretch condition and the interaction between the OR-Stretch condition and surgical duration had no significant effects on surgeons’ body part discomfort and overall fatigue (all p > 0.05). Surgical duration had a significant effect on intraoperative discomfort in the neck (p = 0.0146), shoulders (p = 0.0049), upper back (p = 0.0088), lower back (p = 0.0068), and overall fatigue (p < 0.0001) (Table 2).
The impacts of surgical duration on the intraoperative body part discomfort and overall fatigue (from 0 = “no discomfort”/ “no fatigue” to 10 = “significant discomfort”/ “extremely fatigued”).

*Mean (standard deviation) of the body part discomfort and overall fatigue.
Intraoperative workload
The OR-Stretch condition did not have a significant effect on any of the workload subscales. The interaction between the OR-Stretch condition and surgical duration had a significant impact only on the degree of difficulty (p = 0.0195) (Figure 2). The post-hoc Tukey test revealed that the degree of difficulty for the Baseline*SHORT and Break-30*SHORT were both smaller than Break-30*LONG (Figure 2). The surgical duration had a significant impact on mental demand (p < 0.0001), physical demand (p < 0.0001), temporal demand (p = 0.0008), task complexity (p = 0.0004), situational stress (p = 0.0011), effort (p = 0.0006), frustration (p = 0.0001), and degree of difficulty (p = 0.0003) (Figure 3).
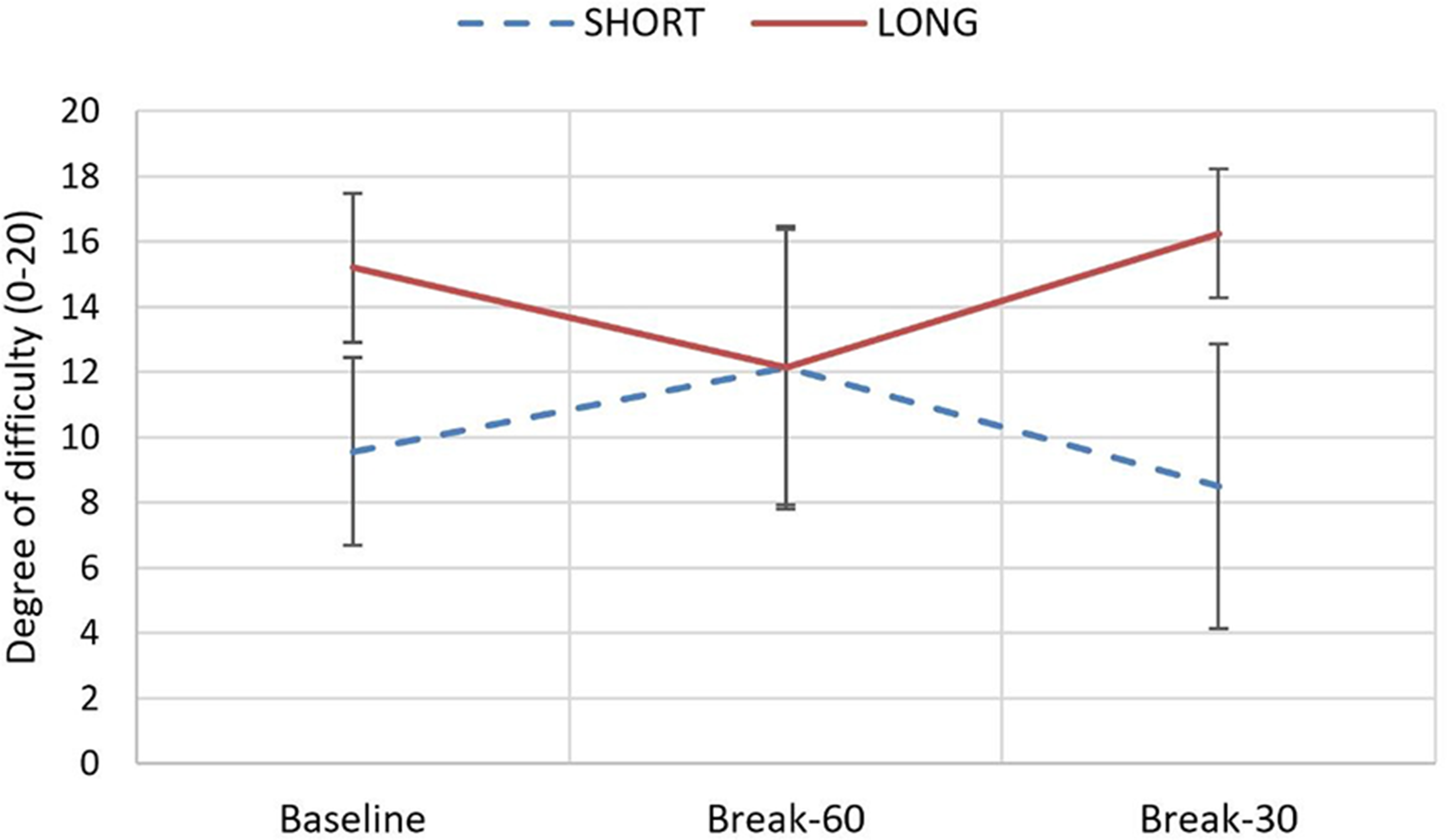
The interaction between OR-StretchTM condition and surgical duration on degree of difficulty of surgical procedures (based on mean and standard deviation) (p = 0.0195).
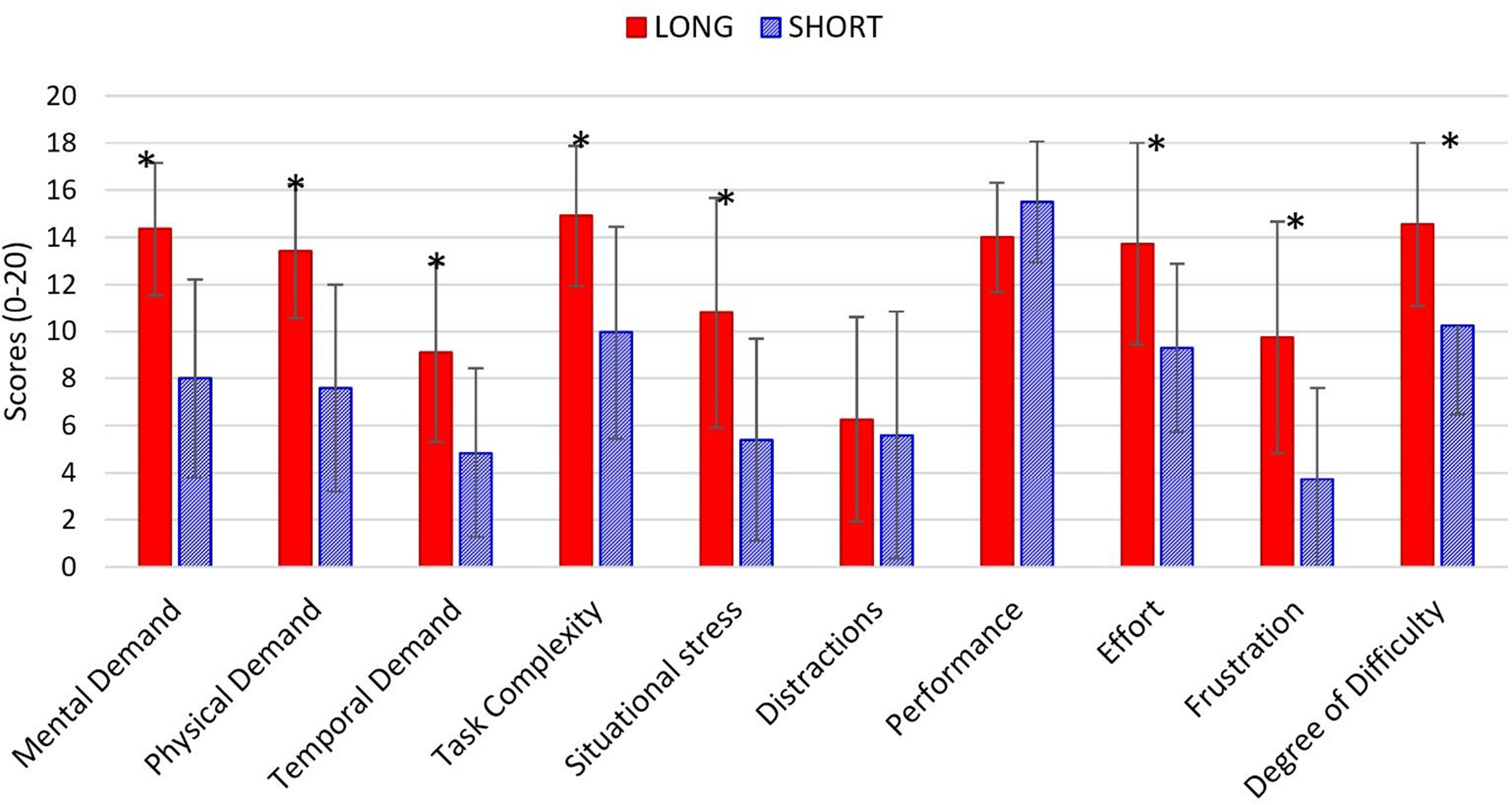
Mean and standard deviation of workload subscales by surgical duration (LONG and SHORT). * means that LONG and SHORT conditions were statistically different (significance level of 0.05).
OR-Stretch evaluation
The participants’ responses to questions asking about the intraoperative impact of OR-Stretch microbreaks on their physical performance, mental focus, body pain/discomfort, and level of fatigue (5-level scale (“much worse,” “worse,” “no change,” “better,” “much better”) showed that both Break-30 and Break-60 conditions helped surgeons with these factors with a response rate of improvement (better or much better) between 28.6% and 78.6% (Figure 4). None of the surgeons reported that the incorporation of the OR-Stretch breaks during the surgical procedure had a negative impact (worse or much worse) on their physical performance, body pain/discomfort, or level of fatigue. There was only one surgical procedure for the Break-30 condition where the surgeon reported that the incorporation of the OR-Stretch breaks worsened their mental focus (Figure 4(b)). Furthermore, the full factorial model did not find any significant effect of OR-Stretch condition, surgical duration, or their interaction on these variables.
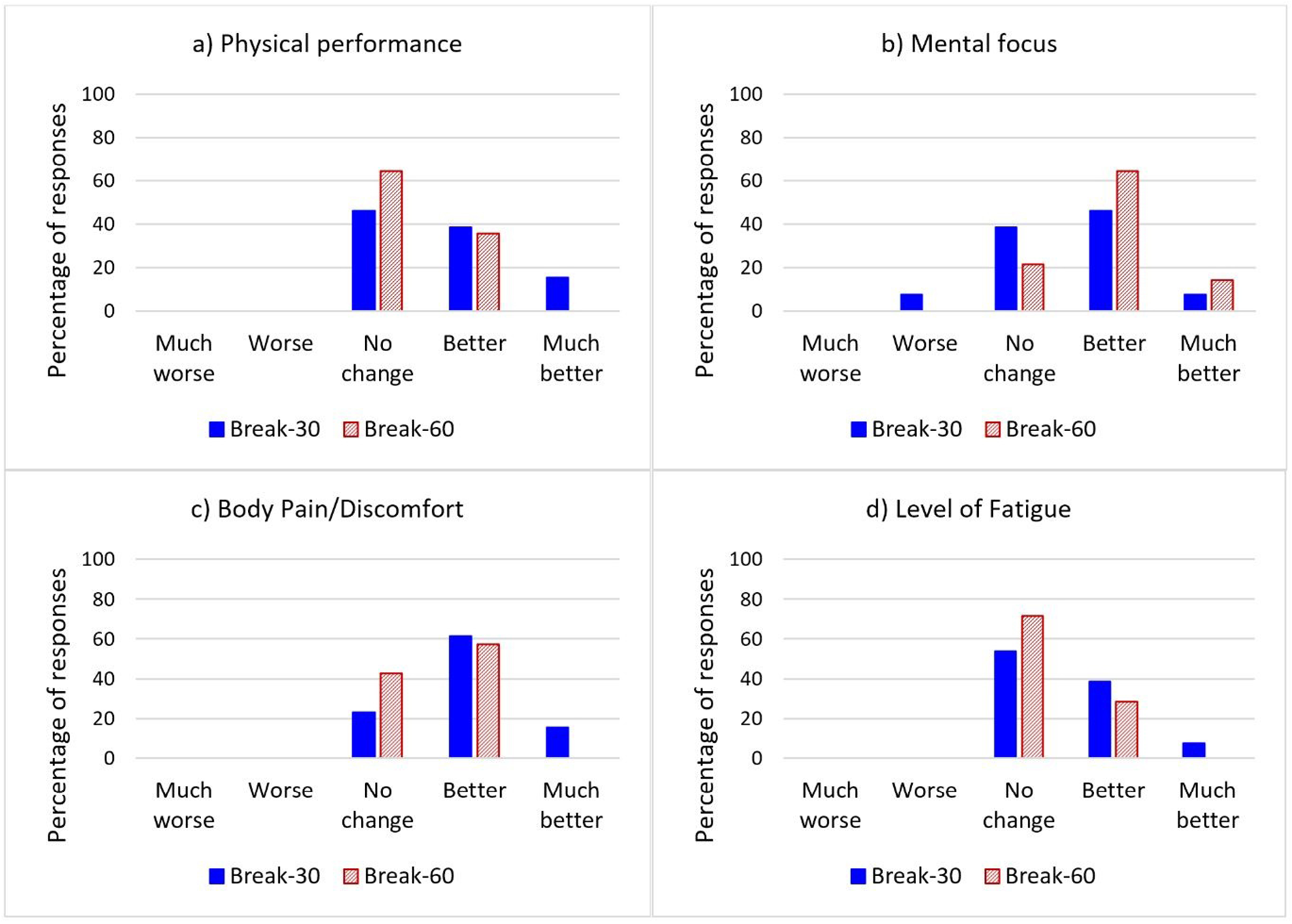
Percentage of participants’ responses to questions asking the intraoperative impact of OR-StretchTM microbreaks on their physical performance, mental focus, body pain/discomfort, and level of fatigue for break-30 condition (13 surgical procedures) and Break-60 condition (14 surgical procedures).
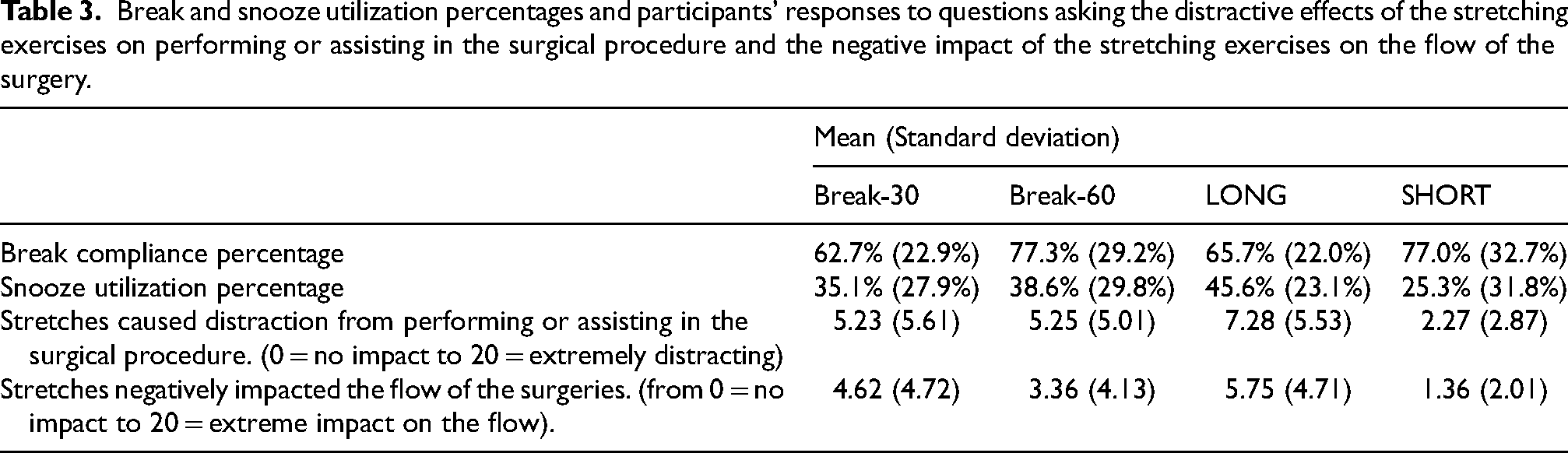
Table 3 presents the percentages of break and snooze utilization for Break-30 and Break-60 conditions. OR-Stretch condition, surgical duration, or their interaction did not have a significant effect on these variables. Additionally, Table 3 summarizes participants’ responses to two questions that recorded the distractive effects of the stretching exercises on performing/assisting in the surgical procedure and the negative impact of the stretching exercises on the flow of the surgery. The scores for both questions were higher for LONG surgical procedures (p = 0.0128 and p = 0.0119, respectively) relative to SHORT procedures. OR-Stretch condition and its interaction with surgical duration did not have a significant effect on the responses to these two questions.
Break and snooze utilization percentages and participants’ responses to questions asking the distractive effects of the stretching exercises on performing or assisting in the surgical procedure and the negative impact of the stretching exercises on the flow of the surgery.
The participants’ feedback on their desired frequency of taking breaks for the studied surgical procedures showed that during the Break-30 condition, they preferred fewer breaks (“less” or “much less”) during 61.5% of the surgical procedures. Alternatively, fewer breaks were preferred in only 28.6% of the surgical procedures for the Break-60 condition, and for this condition in 21.4% of the surgical procedures more breaks were preferred (Figure 5). Despite these meaningful trends in the data, the statistical analysis did not reveal any significant effect of the OR-Stretch condition, surgical duration, or their interaction on this variable. It is important to note that during a vascular surgical procedure and a thoracic surgical procedure, which both were Break-30 condition, the surgeon/circulating nurse asked to terminate the study. The break and snooze utilization percentages were calculated based on data up to the point the studies were terminated. Terminations were both due to complex surgeries and additional complexities that occurred during the surgical procedures.
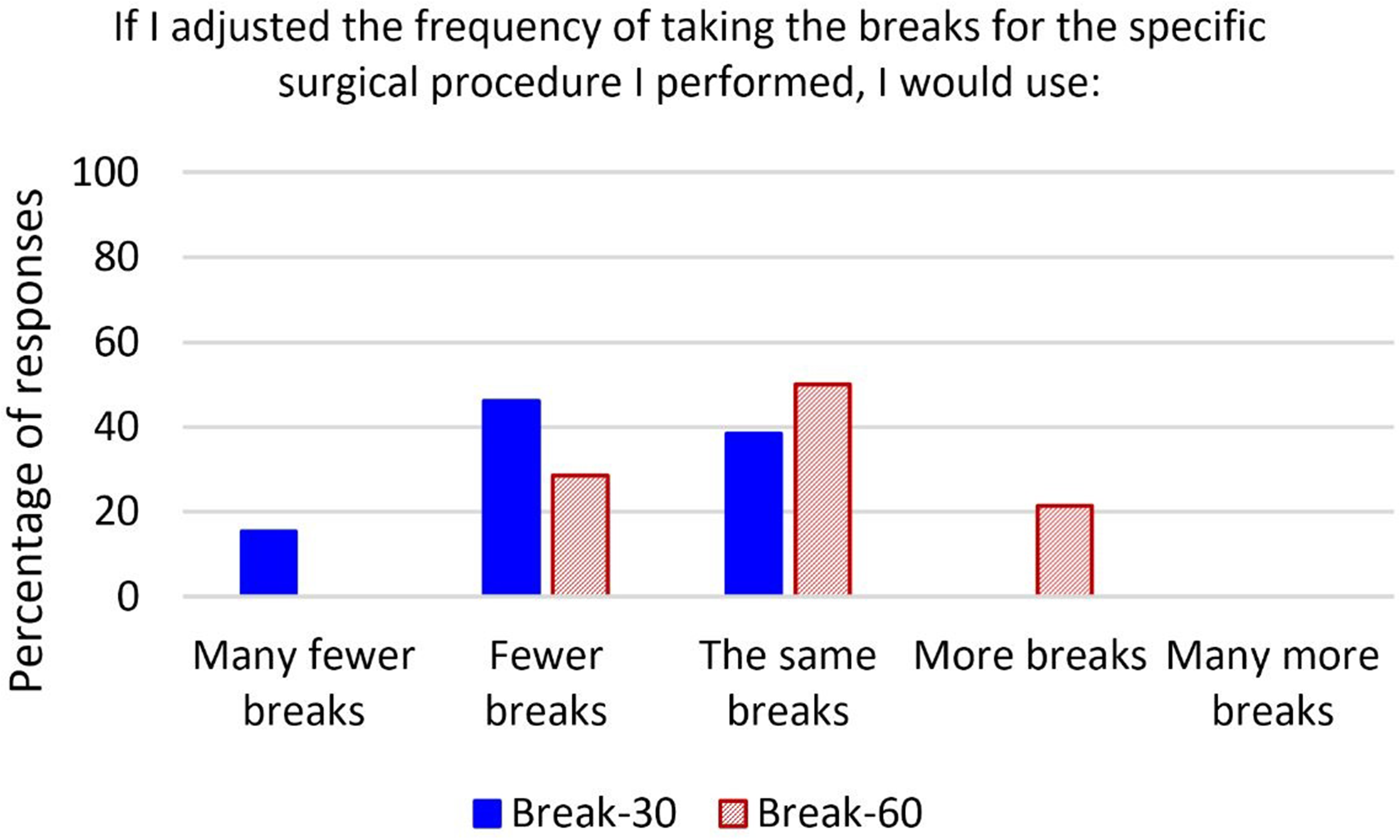
Percentage of participants’ feedback on their desired frequency of taking breaks for the studied surgical procedures.
Post-study usability and overall feedback survey
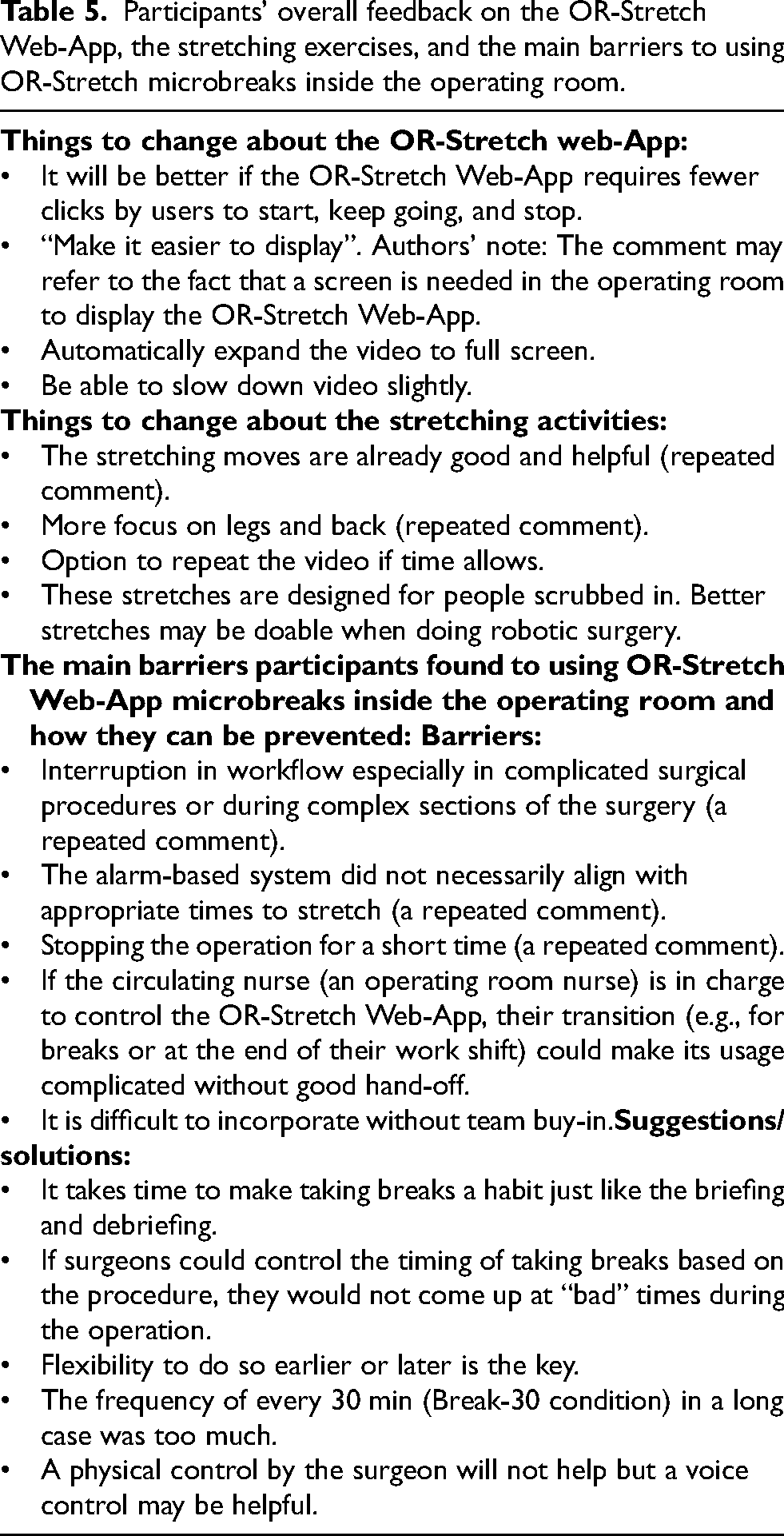
Participants’ responses to the modified SUS survey have been presented in Figure 6. While Figure 6 illustrates their evaluation of the application of the OR-Stretch Web-App microbreaks in this study, they also shared their opinion on four potential strategies that may help with using OR-Stretch in the future (Table 4). When the participants were asked to compare using a regularly scheduled alarm (e.g., every 30 or 60 min) versus taking OR-Stretch breaks at natural transitions during a surgical procedure, seven participants (50.0%) chose a pre-defined alarm (e.g., every 30 or 60 min), five participants (35.8%) chose to take OR-Stretch breaks at natural transitions during a surgical procedure, one participant (7.1%) did not specify either strategy to be better but stated their viewpoints, and one participant (7.1%) did not answer to this question. Participants’ comments supporting the pre-defined alarm repeatedly highlighted the importance of a reminder and the fact that without it, the surgeons may lose track of time when performing surgery and forget to take a break. Comments in favor of taking breaks at natural transitions focused on the fact that the surgeon would know optimal times for taking breaks, thus improving workflow, and would be more likely to be incorporated into practice. Surgeons that preferred natural transitions were asked about the best way to remind the surgeon to take a break at these intervals; they recommended discussing breaks pre-operation during their briefing, having the scrub technician or circulating nurse remind the surgeon at appropriate times, or using signage in the OR. One participant recommended a silent system that notifies the OR team to consider a stretch in a 30- to 90-min window, with an alarm only at the 90-min mark. Finally, Table 5 summarizes participants’ overall feedback on the OR-Stretch Web-App, the stretching exercises, and the main barriers to using OR-Stretch microbreaks inside the OR.
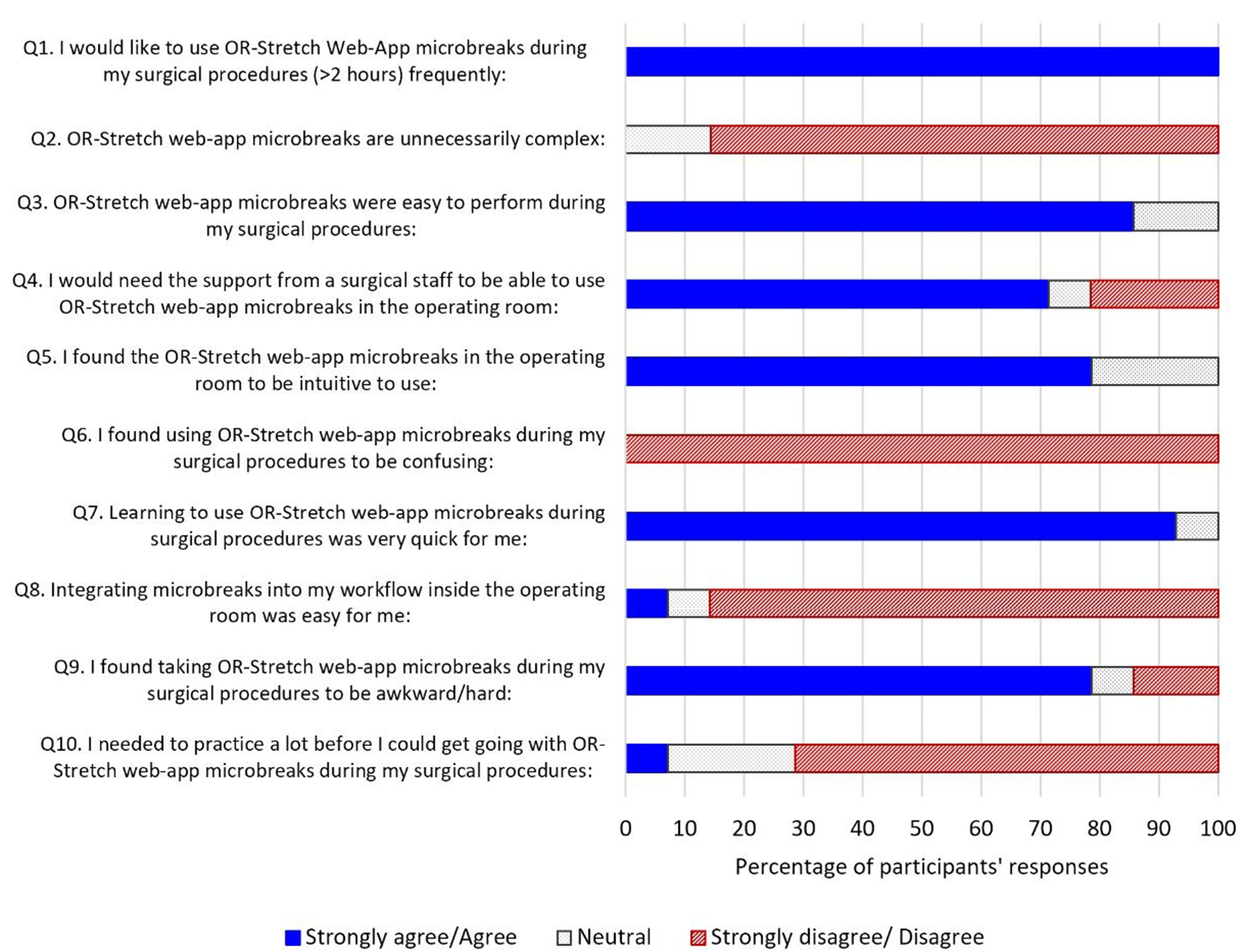
Participants’ responses to the modified standard usability scale (SUS) survey. Note that to simplify the graph the Strongly agree and Agree responses were combined. The Strongly disagree and Disagree responses were combined.
Participants’ responses to a question that asked them to rank and comment on four potential strategies that may help with using OR-Stretch in the future. It should be noted that the participants could choose equal ranks for two or more options.

* One participant did not rank this option and was treated as a missed data point for this option.
** Two participants did not rank this option and were treated as missed data points for this option.
Participants’ overall feedback on the OR-Stretch Web-App, the stretching exercises, and the main barriers to using OR-Stretch microbreaks inside the operating room.
Discussion
This study evaluated the usability and effectiveness of two intraoperative microbreak schedules (Break-30 and Break-60) using the OR-Stretch Web-App, compared with no microbreaks (Baseline). Procedures covered multiple specialties and surgical modalities. Subjective surveys were used to assess the microbreaks’ effects on surgeons’ physical workload and to identify barriers and facilitators to long-term implementation.
Intraoperative body part discomfort and fatigue
Surgical duration was the primary factor influencing intraoperative discomfort in the neck, shoulders, upper back, lower back, and overall fatigue (all p < 0.05). In contrast, neither OR-Stretch use nor its interaction with surgical duration significantly affected discomfort or fatigue (all p > 0.05). These results indicate that OR-Stretch microbreaks during a single surgical procedure (median duration = 207 min) were not sufficient to produce measurable reductions in discomfort or fatigue. This is partially consistent with previous literature; Bonsch et al. (2024) found no significant difference in surgeons’ ratings of perceived musculoskeletal discomfort between taking no microbreaks and taking 2.5-min passive and active microbreaks every 30 min during 90-min laparoscopic simulations. 46 Similarly, Hallbeck et al., (2017) found that the usage of 1.5–2-min guided microbreak exercises every 20–40 min decreased body part discomfort significantly in the shoulders (p < 0.05) but not in the neck, back, hands, knees, and feet. 35 In contrast, Dorion and Darveau (2013) found that 20-s microbreaks every 20 min significantly reduced discomfort across multiple body regions. 33 This inconsistency may be explained by the shorter, more frequent work/break intervals, 33 though such schedules may not be feasible in real surgical workflows.
Intraoperative workload
Similar to discomfort and fatigue, OR-Stretch conditions had no significant effect on any workload subscales, whereas surgical duration significantly influenced mental and physical demands, temporal demand, task complexity, situational stress, effort, frustration, and degree of difficulty (all p < 0.01) (Figure 3). These findings indicate that OR-Stretch did not reduce workload but also did not worsen other aspects such as distractions, performance, or perceived difficulty. The subjective surveys used in this study may not have been sensitive enough to detect microbreak effects (either positive or negative) during a single procedure, which may differ for a full day of procedures. It also highlights the importance of surgeons’ general evaluations and post-study feedback to understand broader usability and potential impact.
The interaction between OR-Stretch conditions and surgical duration had a significant impact on the surgeons’ reported degree of difficulty of the surgical procedures (p = 0.0195). The results of the post-hoc Tukey test in conjunction with Figure 2 explain how the effects of the surgical duration (SHORT vs. LONG) on the degree of difficulty are also associated with the OR-Stretch condition (Baseline vs. Break-30 vs. Break-60). The combination of LONG procedures with Break-30 condition, which is the most frequent microbreak strategy, led to the highest score of degree of difficulty (mean = 16.25 out of 20); significantly larger than the degree of difficulty for SHORT surgical procedures combined with Baseline (mean = 9.56 out of 20) or Break-30 conditions (mean = 8.50 out of 20). Additionally, Figure 2 indicates the complex interactive effects of surgical duration and OR-Stretch condition on the degree of difficulty of the surgical procedures. While more research is essential to clarify this relationship, it could be speculated that based on the degree of difficulty, which is not the only factor that should be considered in the OR-Stretch implementation, Break-60 is a better fit for LONG surgical procedures and Break-30 works better for SHORT surgical procedures.
OR-Stretch evaluation
The body part discomfort, fatigue, and workload subscale questions may be too granular to capture the impact of OR-Stretch during a single surgical procedure; however, the more general yes or no evaluation questions of the survey helped clarify the effectiveness and usability of OR-Stretch microbreaks. The incorporation of the OR-Stretch microbreaks during the surgical procedure (either Break-30 or Break-60 conditions) improved surgeons’ physical performance and mental focus while it decreased their body pain/discomfort and level of fatigue (from 28.6% up to 78.6%; Figure 4). These findings are consistent with previous literature that found similar positive impacts of taking microbreaks during surgical procedures.35,37,46 In a single surgical procedure (7.7%, Break-30 condition), the surgeon reported that the incorporation of the OR-Stretch microbreaks worsened their mental focus (Figure 4). The more frequent Break-30 showed trends of being better for surgeons’ physical performance, body pain/discomfort, and fatigue, but that came with more interruptions which non-significantly degraded the mental focus compared to the less frequent Break-60 (Figure 4).
Surgeons’ responses to questions regarding the distractive effects of the stretching exercises on performing/assisting in the surgical procedure and the negative impact of the stretching exercises on the flow of the surgery (mean = 3.4–5.3 out of 20) were higher than previous literature,35,37 and were both higher for LONG surgical procedures relative to SHORT procedures (Table 3). There was no statistically significant difference in the evaluated factors between Break-30 and Break-60 conditions. However, the findings provide some evidence that Break-60 condition is preferred over Break-30 condition, especially during longer and more complicated surgical procedures. These findings are (1) The participants’ feedback on their desired frequency of taking microbreaks showed that surgeons preferred fewer breaks in 61.5% of the procedures for the Break-30 condition compared to 28.6% of the procedures for the Break-60 condition, (2) The incorporation of OR-Stretch microbreaks was terminated during two surgical procedures for the Break-30 condition (due to complex surgeries and additional complexities that occurred during the surgical procedures) and worsened mental focus during one LONG surgical procedure for the Break-30 condition, and (3) One surgeon mentioned that taking microbreaks every 30 min (Break-30 condition) in a long case was too frequent (Table 5).
Clinically, these patterns suggest that Break-60 may be more suitable compared to Break-30 condition especially during longer or more complex procedures. In contrast, Break-30 may be more challenging to implement due to more frequent workflow disruptions.
Post-study usability and overall feedback survey
Participants’ evaluations of the application of the OR-Stretch Web-App microbreaks from the modified SUS survey showed that all participants showed interest in continuing to use OR-Stretch microbreaks, similar to a previous study that reported 87% percent of their participants wanted to continue using microbreaks with exercises in the OR. 35 Surgeons overall found OR-Stretch microbreaks easy and intuitive to use in the OR. However, surgeons were primarily concerned about (1) Integrating the microbreaks into the workflow in the OR, (2) Finding OR-Stretch microbreaks during surgical procedures to be awkward/difficult, and (3) The need for support from a surgical staff to be able to use OR-Stretch microbreaks in the OR.
Surgeons’ feedback on OR-Stretch highlighted key facilitators and barriers. They found the microbreaks easy and intuitive to use but recommended several improvements to enhance user-friendliness, such as reducing the number of clicks, enabling video speed control, and adding an auto-full-screen option which we will be incorporating into subsequent iterations. They also emphasized the need for more specialized stretching videos tailored to specific surgical modalities (e.g., robotic surgeons are not confined to the sterile field) or body regions. The primary barrier to implementation was workflow interruption, particularly when alarms occurred during complicated surgical procedures or complex phases of surgery. This issue is exacerbated when the alarm-based system signals a time for stretching that is not appropriate or convenient. However, it should be noted that the reminder itself was viewed as important for preventing loss of time awareness.
Potential directions for future research include aligning microbreak timing with natural workflow transitions, improving user-friendliness through simplified or hands-free app control (e.g., verbal commands), and assigning an OR staff member (e.g., circulating nurse) to manage the app. These recommendations are consistent with findings by Anderson et al. (2024), who compared scheduled microbreaks (every 45 min) with self-determined intervals (30–60 min). Although the self-determined approach did not show clear performance advantages, it was viewed as a potentially more favorable implementation strategy. 47
Limitations
The main limitation of this study is the small sample size. While we attempted to cover a range of surgical durations from several surgical subspecialties and surgical modalities, the small sample size limited the inclusion of all these factors in the analyses. Future studies should target larger sample sizes and evaluate potential solutions to address some of the concerns regarding the implementation of OR-Stretch in the OR. Additionally, our evaluations were limited to single surgical procedures per data collection and three data collections per surgeon. In the future, the effectiveness of OR-Stretch in reducing body part discomfort and fatigue over a full surgical day should be studied in more comprehensive and longitudinal studies. It should also be noted that this study relied on subjective measures (e.g., discomfort, fatigue, workload surveys) but did not include objective ergonomic assessments such as posture or muscle activity measures. The study's subjective evaluation methods and modest sample size limit generalizability. Although validated instruments were used, larger studies incorporating objective biomechanical measures are recommended to confirm these findings.
Another limitation is that some trials were terminated due to intraoperative complexities. Such events are common in surgical practice and reflect the dynamic and unpredictable nature of the operating room. These findings highlight a key implementation challenge for intraoperative microbreak interventions, as their feasibility may be reduced during complex or rapidly evolving surgical situations. These findings suggest that implementation of intraoperative microbreak interventions may benefit from a gradual integration into surgical practice, particularly by first applying them in less complex procedures before broader adoption into more complex cases. Finally, participation was voluntary, which may have introduced selection bias, as surgeons with greater interest in ergonomics or microbreak interventions may have been more likely to enroll. This may limit the generalizability of the findings to the broader surgical population.
Conclusion
This study provides further evidence supporting the OR-Stretch Web-App as a potential ergonomic intervention in the OR. Overall, OR-Stretch™ positively influenced surgeons’ physical performance, mental focus, body pain/discomfort, and level of fatigue. However, enhancing the Web-App's user-friendliness and developing strategies to synchronize microbreaks with appropriate times during surgeries, to avoid disrupting the surgical workflow, are critical areas requiring attention. Additionally, no significant differences were observed in surgeons’ subjective evaluations of the Break-30 and Break-60 scheduling strategies. Nonetheless, the subjective data and surgeons’ feedback suggest that Break-60 is preferable to Break-30 condition as taking microbreaks every 30 min (Break-30 condition) may be too frequent, particularly during long or complex surgical procedures.
Footnotes
Acknowledgements
The authors would like to acknowledge the support and participation of the surgeons involved in this study. We would also like to thank the Robert D. and Patricia E. Kern Center for the Science of Health Care Delivery for their support.
Ethical approval and informed consent statements
This study was approved by the Institutional Review Board of the Mayo Clinic (protocol 22-001114), as communicated on March 1, 2022, and was classified as minimal risk.
Consent to participate
This study was approved by Mayo Clinic's institutional review board (IRB). Oral consent was gained from all participants. Mayo IRB 22-001114. Project Full Title: Evaluating the Effects of Active Microbreaks Using OR-Stretch Web-app on Surgeons’ Intraoperative Workload and Body Part Discomfort.
Informed consent
Participants provided oral informed consent to voluntarily participate in the study's research protocol.
Author contributions
Hamid Norasi: Conceptualization, Data curation, Methodology, Project administration, Visualization, Writing – original draft.
Joseph Y Kim: Conceptualization, Data curation, Methodology, Project administration, Visualization, Writing – review and editing.
Mojgan Zoaktafi: Data curation, Methodology, Project administration, Visualization, Writing – review and editing.
Susan Hallbeck: Conceptualization, Methodology, Resources, Supervision, Writing – review and editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.