
Abstract
Background
Despite demonstrated physical and psychological benefits of employment after spinal cord injury (SCI), there are many barriers that must be navigated to promote job acquisition, retention, and advancement.
Objective
Our purpose was to identify the underlying dimensions of perceived barriers and facilitators to employment so that they may be measured and used in vocational practice to improve employment outcomes.
Method
2830 adults with traumatic SCI completed a 32-item measure of barriers to employment, developed based on previous research.
Results
Using principal axis factor analysis with varimax rotation, four factors emerged: (1) health considerations, encompassing pain, fatigue, stress, and SCI-related care needs; (2) poor job fit, reflecting perceptions of limited, inaccessible, or low-paying job opportunities; (3) low motivation/confidence, indicating low desire or self-efficacy for work; and (4) limited resources, representing insufficient education, training, transportation, and related supports.
Conclusion
These factors offer a parsimonious framework for vocational counseling, which will allow vocational counselors to examine sets of barriers and facilitators simultaneously, rather than just individually. Future research is needed on the relationship of these themes to employment outcomes, including job stability and quality, as well as for developing targeted interventions to improve employment outcomes.
Introduction
Employment is an integral component of adult life, and, for individuals living with spinal cord injury (SCI), being employed is related to enhanced psychological (Meade et al., 2015) and physical health, including life expectancy (Krause et al., 2012). Despite this knowledge, employment rates among people with SCI remain significantly lower than those in the general population (Chen et al., 2022; NSCISC, 2025), and vocational rehabilitation efforts are focused more on job attainment rather than quality employment outcomes. Understanding the factors which contribute to obtaining, maintaining and advancing employment after SCI is essential for informing policy and practice to improve employment rates and outcomes.
Research is abundant on the demographic and injury characteristics associated with employment after SCI; yet few studies have explicitly focused on barriers and facilitators. The limited research has identified a wide array of both barriers, such as physical limitations, inaccessible workplaces, and employer discrimination, and facilitators, including educational attainment, job accommodations, and social support, as influential to employment after SCI (Karcz et al., 2022; Krause et al., 2021; Krause & Reed, 2011; Sturm et al., 2020). For example, Karcz et al. (2022) specified personal and environmental factors as key facilitators to sustainable employment after SCI. When participants perceived work as beneficial, maintained a positive attitude, and were able to practice self-acceptance and self-advocacy, they were more likely to persist in the workplace. Similarly, aspects of the work environment, whether social, physical, or policy-oriented, were viewed as facilitators when they were supportive and accommodating. Krause et al. (2021) identified the diagnostic-specific barriers related to employment status for individuals with SCI or multiple sclerosis, finding inaccessibility and lack of training and support to be the predominant barriers for those with SCI. Another cross-disability study (Dinelli et al., 2024) explored the relationship between multiple personal, health status-related, and work-related characteristics, as well as several external factors, with the likelihood of working after disability and likelihood of keeping the longest held job. Older age, financial strain, and the need for assistive devices were linked to decreased likelihood of employment after disability, while identifying as a non-Black minority, experiencing fatigue, and maintaining higher levels of physical function were associated with greater likelihood of employment. Participants were more likely to maintain their longest held position if the disability was acquired in the workplace, they received accommodations, they valued opportunities for advancement and health benefits, and they were in in a supportive living situation. However, dissatisfaction with the job and negative supervisor attitudes emerged as key barriers to maintaining employment.
Even fewer studies have analyzed the latent constructs organizing these barriers and facilitators into meaningful categories. One study (Karcz et al., 2022) used focus groups to explore how individuals in two condition groups, SCI and traumatic brain injury, perceived these influences and found perceived facilitators and barriers across three themes of personal, environmental, and impairment-related factors. While personal factors were perceived as facilitators and impairment-related factors were noted as barriers, environmental factors, depending on their nature, were perceived as either a facilitator or barrier. Krause and Pickelsimer (2008) found a health-related factor to be the most prominent barrier when exploring future employment status in a sample of 343 unemployed individuals with SCI, even more so than lack of resources or potential loss of disability benefits. In a study of 781 participants with SCI, factor analysis of 30 items on barriers and facilitators identified six dimensions (Krause & Reed, 2011). These included: resources, health status, disability considerations, lack of importance, disincentives, and motivation. Although identifying the six dimensions has been valuable, preferably, there would be a smaller number of themes to optimize counseling. Furthermore, these dimensions included a scale with less than three items which limits the validity of measurement. Identifying a smaller set of themes provides counselors a better framework from which to discuss barriers and facilitators, when compared with long lists of individual barriers.
Our purpose was to expand upon previous research by applying factor analysis to 32 items on barriers and facilitators to employment after SCI to identify the underlying dimensions. This establishes the foundation for better understanding for focusing on a new set of barriers and facilitators by identifying common themes that may ultimately be used in vocational practice and future research linking barriers and facilitators to important employment outcomes. It also lays the foundation for the development of conceptual schemes to help us better organize and understand barriers and facilitators to employment after SCI and other disabling conditions.
Method
Participants
Institutional Review Board approval was obtained prior to contacting participants. Potential participants were identified from participation rosters of two longitudinal studies, including the 45-year SCI Longitudinal Aging Study (Krause et al., 2015, 2017) and the 15-year SCI Health and Longevity Study (Krause & Saunders, 2010). Participants in the SCI Longitudinal Aging Study were enrolled from universities and specialty hospitals in the Midwestern United States in 1973, 1984, and 1993, and from a specialty hospital in the Southeastern United States in 1993 and 2002. The SCI Health and Longevity Study participants were enrolled from three sources including the same specialty hospital in the Southeastern United States (1997, 2007, and 2011) and two population-based surveillance systems (one from the Midwest and one from the Southeast). Participants met the following inclusion criteria at the time of enrollment in each longitudinal study: 1) traumatic SCI with non-complete recovery, 2) at least 18 years of age, and 3) a minimum of one year since SCI onset. There was no initial restriction on age at injury onset. There were 2830 respondents from an initial pool of 4,248.
Data Collection Procedures
All data were collected by self-report. Potential participants were mailed a recruitment letter to describe the study and alert them that materials would be forthcoming. Assessment packages were mailed to participants 4–6 weeks later. Participants were given the option of completing the measure online. There were two follow-up mailings and a follow-up phone call. Participants received $50 in remuneration. Data were collected between December 2015 and October 2017.
Measures
Participants completed a self-report assessment regarding their employment history, as well as their demographics and disability characteristics. There were 32 items related to barriers and facilitators of employment, with five response options ranging from strongly disagree to strongly agree. The items were mixed in terms of direction, with some items stated in the direction of facilitators and the other items as barriers, to maximize the validity and avoid response bias. For instance, the first question is stated as a facilitator, “I have the proper education and/or training to work,” and the final question is framed as a barrier, “Memory problems or confusion make working difficult.”
The items set was developed based on previous research. The forerunner to the current item set was originally developed for an earlier study of SCI where similar questions were asked solely of participants who were unemployed at the time of the study (Krause & Pickelsimer, 2008). The list was expanded and reassessed to be used with both employed and unemployed participants in a subsequent study (Krause & Reed, 2011) by changing the wording of some items. Additional items were added over time as new content areas were identified and developed through general focus groups with stakeholders with lived experience with SCI and through discussion and input of the research team. The measure may best be considered a working set of items that may be better defined over time through research with additions to refine underdeveloped constructs.
Analyses
Data analyses were conducted using SPSS v25a and R version 4.4.2. Basic descriptive statistics were used to identify the participants’ characteristics. Principal axis factor analysis was used to identify all factors with eigenvalues greater than 1.0, followed by a varimax rotation to clarify the nature of factors. Additionally, in the “psych” package in R, a parallel analysis scree plot was constructed using 10,000 resampled analyses (Figure 1). This was done to provide additional information to guide the selection of the number of factors. Items with factor loadings of ±0.4 were retained with the factor. Only factors with three or more items loaded with the factor were retained in the final model. Factor based scales were created by reversing the scoring of some items so that all were consistent with higher scores indicating greater barriers, as this provides clarity for interpretation for vocational counseling. Scales were generated by summing the questions loading with each factor. Alpha coefficients were generated for each of the resulting scales to determine the internal consistency.

Parallel analysis scree plot for the EFA.
Results
The initial factor analytic solution indicated seven factors with eigenvalues greater than 1.0. The eigenvalues of the EFA (Table 1) demonstrate that approximately one-third of the variance in the individual barriers and facilitators is explained by factor 1. Factors 2–7 by contrast explain much less variance in the set of questions, with a high of 6.21% and a low of 3.16%. However, all seven factors explain more variance than a single item would on average. The parallel analysis scree plot suggested five factors and indicated factors 6 and 7 may not be stable. Additionally, their eigenvalues are particularly close to the threshold of 1. The final three factors did not have loadings from the minimum of three items and therefore were eliminated (Table 2). The model root mean square error of approximation (RMSEA) was 0.046 (90% CI = 0.044, 0.048), which indicates a good model fit using the standard threshold of 0.05 or less. The four factors that were retained had alpha coefficients that ranged from 0.73 and 0.89.
Eigen Values for the Seven Selected Factors, Including Variance Explained, and Number of Items Loaded to Each Factor.

Rotated Factor Matrix of Spinal Cord Injury Employment Barriers and facilitators.
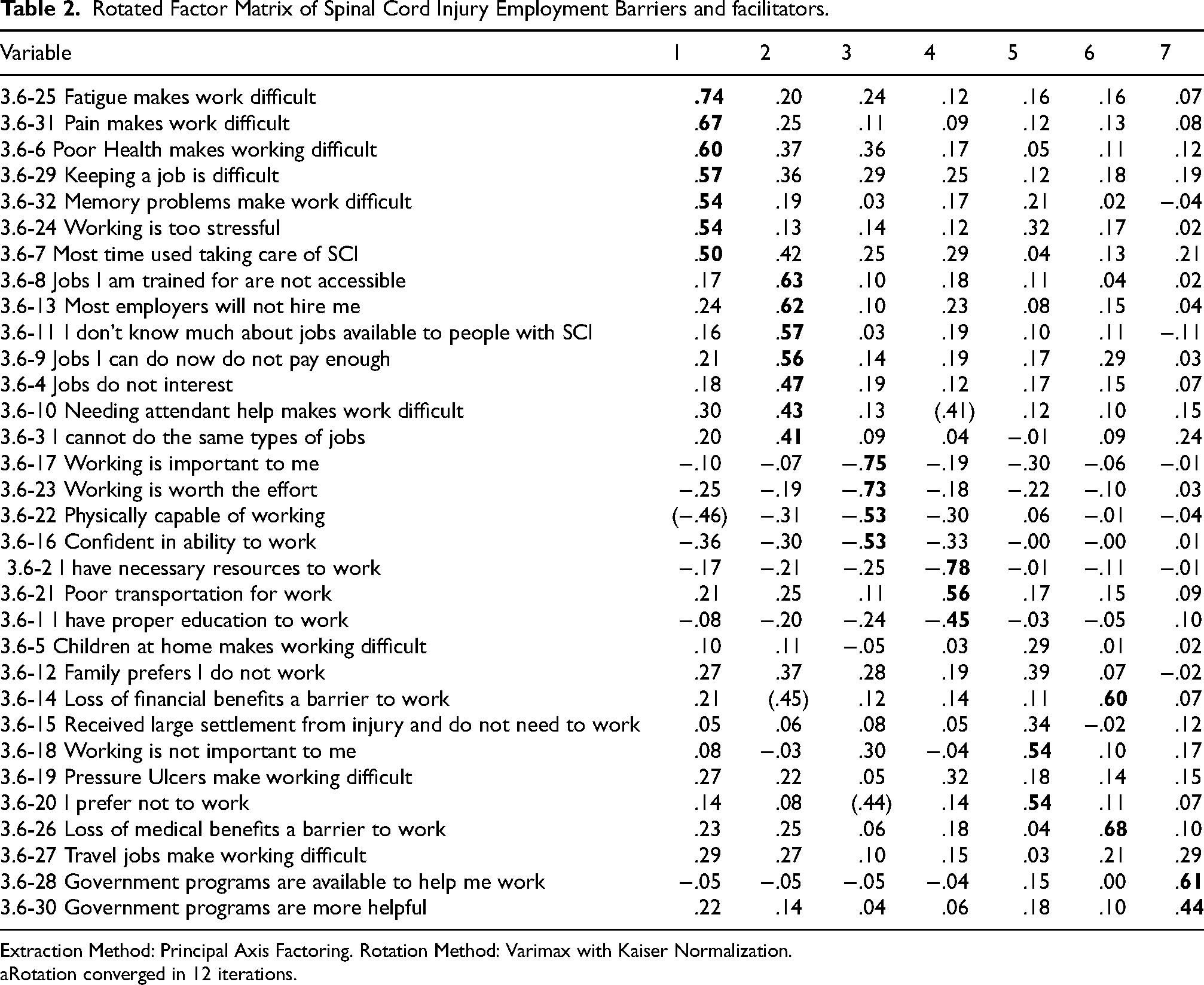
Extraction Method: Principal Axis Factoring. Rotation Method: Varimax with Kaiser Normalization.
Rotation converged in 12 iterations.
Factor 1, entitled health considerations, had seven items load with it ranging in magnitude from 0.5 (time taken up by SCI related needs) to 0.74 (fatigue makes working difficult). The items clearly reflected health and that SCI is a barrier to employment, with other items including: working is too stressful (0.54), memory problems make work difficult (0.54), keeping a job is difficult (0.57), poor health makes working difficult (0.6), and pain makes work difficult (0.67). The alpha coefficient was 0.89.
Factor 2 (poor job fit) also had seven loadings ranging from 0.41 (cannot do the same types of jobs) to 0.63 (appropriate jobs are not accessible). The items included: needing attendant help makes working difficult (0.43), jobs do not interest me (0.47), jobs I can do now do not pay enough (0.56), I don’t know much about jobs available to people with SCI (0.57), most employers will not hire me (0.62). The item on attendant care had very high loadings on the fourth factor (−.43). The alpha coefficient was 0.82.
Factor 3 (lack of motivation and confidence) had four loadings ranging from 0.53 (which was tied between “confident in ability to work” and “physically capable of working”) and 0.75 (working is important to me). The remaining item was: working is worth the effort (0.73). The alpha coefficient was 0.85.
Factor 4 (insufficient resources) had three loadings ranging from 0.45 (having the necessary education to work) and 0.78 (having the necessary resources to work). The third item loaded with this factor was, poor transportation for work (0.56). The alpha coefficient was 0.73.
Discussion
The primary contribution of this study was the identification of the underlying dimensions of barriers and facilitators to employment after SCI. This is important because it reduces the amount of information to underlying themes which will allow vocational counselors to look at and discuss the four themes, rather than individual barriers and facilitators one at a time. For instance, they may discuss issues related to health, rather than needing to focus on each individual aspect of health. Alternatively, they could begin with a general theme and then move to particular barriers within the vocational counseling process. Evaluating the scores across themes will give a general sense of individual readiness for employment. The development of the items and factor analysis also establishes the foundation for identifying the relationships of the theme as related with important employment outcomes, such as transition to employment, job stability, job quality, earnings, and work life expectancy.
The health considerations factor measures many of the fundamental physiologic complications that may accompany SCI, including pain and fatigue, as well as the need for taking care of SCI needs. It also reflected perceptions of stress, and they simply did not appear to feel capable of working. This is important because it would suggest that, for some people, work may not be a current consideration or may be too overwhelming to consider, at least at a particular point in time. In short, the individual simply may not see herself/himself ready to take a step toward employment. Some physical complications may be direct targets for therapy, such as controlling pain, and this would require an interdisciplinary approach where the vocational counselor would work with other professionals that would more directly address the physiologic and secondary complications, while the vocational counselor worked to promote employment as health improved.
The second factor (poor job fit) represents perceptions that jobs available after SCI simply are not attractive (low pay), are not accessible either physically or because of employer attitudes, there are expenses that preclude working (attendant care) or that they simply do not know enough about them. In some ways, this factor is straightforward for the vocational counselor in that perceptions may be challenged by education, as the counselor may help the individual learn about jobs, consider training that might improve the wages, and by introducing the individual to concrete opportunities. By considering the factor as a whole, the vocational counselor may be able to challenge those aspects of the individuals’ perceptions that are easiest to change with education, then hopefully other aspects of the theme may either change naturally or be less difficult to change. Certainly, addressing this as a theme would be easier than addressing each individual barrier. Previous research has indicated that vocational interests remain mostly stable after SCI (Rohe & Krause, 1998), particularly long-standing SCI. It therefore underscores the importance of working in areas of interest to the individual. For instance, even though someone who is interested in high motor skill occupations, such as auto mechanic, may not be able to do the same work after SCI, it may be possible with additional training and counseling to help them find an alternative occupation in the same general area of expertise (e.g., auto parts sales).
The third factor reflected low motivation and confidence for work, ultimately that it just was not worth the effort. Unlike the previous factor that reflected more specific issues with job fit, accessibility, and pay, this factor simply appears to reflect a lack of desire for employment. Individuals high on this factor may be particularly resistant to even the idea of vocational counseling, since they do not reflect an interest in employment. Vocational counseling in these instances would need to address the basic desire to work at a fundamental level and no doubt would be an uphill struggle. Individuals with this profile may be particularly unlikely to initiate or even be receptive to engage in vocational counseling.
The final factor (limited resources) represents the one where there are the clearest targets for intervention, as it is the factor that may most directly be addressed with resources that relate to favorable funding policy and a focus on working with individuals with severe physical disabilities such as SCI. Whereas health considerations and poor fit between abilities after SCI and available jobs present more substantial barriers, allocation of resources has historically been part of the vocational rehabilitation process. Individuals who lack resources as an underlying reason for employment are by definition good candidates for employment, all things being equal, so long as those resources could be provided. Lack of education is a fundamental shortcoming, as education has been widely known to improve employment opportunity and is associated with higher quality employment, including earnings and benefits (Krause et al., 2023; Krause & Reed, 2009). Clearly, multiple efforts are needed to improve overall employment outcomes among those with SCI. Inadequate transportation is also another fundamental barrier to employment that needs to be and can be addressed with additional resources.
The four-factor model is a more condensed and efficient version of that obtained with six factors in previous research (Krause & Reed, 2011). It has fewer dimensions which are more parsimonious, each dimension is a minimum of three items, and the research is based on a substantially larger cohort (2830 versus 781). The four factors identified overlap with the six factors found previously with the same instrument (Krause & Reed, 2011). From the earlier study, health status aligns with Factor 1 on health in the current study, as both included items on pain, fatigue, stress, and SCI needs. The second factor (poor job fit) intersects with the earlier factor on disability considerations, reflecting concerns about knowledge of work opportunities appropriate after SCI, inaccessibility, and insufficient pay. The third factor (lack of motivation and confidence) encompasses two factors from earlier research focused on lack of importance and motivation with items on interest in working, having financial freedom from other sources, value placed on working, and confidence in ability. Factor 4 (insufficient resources) aligns with the factor on availability of resources from previous research, with items on education, training, transportation, and additional resources. The consolidation of the six factors into four more stable factors, with more items per factor, may lead to more efficient information for vocational counselors. It will simplify discussions with clients who are exploring their barriers to employment.
One caveat that deserves consideration when using the items is that disincentives are widely viewed as an important barrier to employment. We measured both financial and medical disincentives which were correlated but did not have other items that loaded with them sufficiently to form an individual factor. Any discussion of employment options with someone who has SCI should include identification of fundamental financial and health disincentives (i.e., what the individual may lose if they become employed). Therefore, we recommend using these two items individually in addition to the four factors.
Methodologic Considerations
There are several methodologic considerations, both favorable and unfavorable, that should be considered when interpreting the results. First, all data were self-report. This is necessary to identify perceived barriers and facilitators, but they would not necessarily measure actual barriers, only those through the lens of the individual. Second, factor analysis is a way of identifying underlying dimensions that are useful frames of reference for a given purpose, particularly as used in the current study where we are identifying common themes that may serve as the basis for vocational counseling and future research. This does not mean that the observed themes are the only way that the individual barriers and facilitators could be classified, nor does it mean that the factors reflect true underlying dimensions. Rather, it simply represents a frame of reference that may be useful clinically and in research. Alternative methods of factor analysis may produce somewhat different results, although they will all be based on the same underlying pattern of correlations. We ran alternative models using different types of correlation coefficients and the observed pattern seemed to be the most interpretable and beneficial, based on producing four stable factors, each with no less than three items per factor. Third, not all items loaded with one of the four main factors and three factors were represented by less than three items. This suggests there are potentially more domains that may be tapped with additional items, as well as that some of these items perhaps have limited meaning. This is something that needs to be addressed with additional research. Fourth, we used a combination of state surveillance population-based cohorts and clinical cohorts as research participants. Population-based cohorts are the gold standard for research as they include all cases within a select geographic region, even those who may otherwise fall through the cracks of the traditional healthcare system. These cohorts have rarely been included in SCI research. Using participants from clinical settings, while not as strong as population-based cohorts, is far superior to use of general advertisements where there is no independent confirmation of diagnosis and unknown selection bias. Fifth, the data are cross-sectional. This is not particularly a problem for the current study, given the purpose of identifying underlying dimensions, but would be a limitation in terms of identifying relationships with outcomes. Additionally, this study focused solely on people with SCI. Therefore, we do not know the generalizability of the findings to other diagnoses. Lastly, even though the scales that were developed are framed as barriers (i.e., negative direction), it was necessary to have them in a single direction for analysis. In reality, the items can be used as is with a combination of items that are stated all favorably and unfavorably, and they could be scored in a positive direction (facilitators) by reversing the scoring on the negative items instead of those stated positive.
Conclusion
Future Research
First, whereas the current research identifies underlying themes for barriers and facilitators, this is only the first step in their utilization. Additional research is needed to identify how the underlying themes relate to future employment outcomes, including job retention and work life expectancy, as well as serve as the basis of further studies of barriers and facilitators upon conceptual schemes and/or utilize factor analytic studies as the basis for developing new conceptual schemes. Secondly, research should further explore the nature of the underlying themes and look for additional barriers and facilitators that were not sufficiently covered within the current assessment, such as additional incentives. This is particularly true for factors with insufficient numbers of items loading with that factor, particularly disincentives. Further definition of these factors with additional items would better define each content area and provide additional benefit for vocational rehabilitation counseling. Further, modified assessments may identify new additional themes that would be useful for vocational counseling. Lastly, there is always a need for focused intervention research which is the goal of improving employment outcomes for people with SCI and other disabling conditions. Interventions are not only needed for the initial transition to post SCI work, but additional transitions that relate to the stability and quality of employment over time.
Footnotes
Acknowledgment
n/a
Ethics Statement
We certify that all applicable institutional and governmental regulations concerning the ethical use of human volunteers were followed during the course of this research. This study was approved by the Institutional Review Board (IRB) of the Medical University of South Carolina (Pro00114871).
Informed Consent
In accordance with the IRB approval, completion and return of the self-report assessment indicated implied consent under a waiver of written consent.
Funding
The contents of this publication were developed under grants from the National Institute on Disability, Independent Living, and Rehabilitation Research (NIDILRR grant numbers 90DP0050 and 90DPEM0006). NIDILRR is a Center within the Administration for Community Living (ACL), Department of Health and Human Services (HHS). The contents of this publication do not necessarily represent the policy of NIDILRR, ACL, HHS, and you should not assume endorsement by the Federal Government.
National Institute on Disability, Independent Living, and Rehabilitation Research, (grant number 90DP0050, 90DPEM0006).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.