
Abstract
Students with autism and developmental disabilities, including autism, have the right to access the age-appropriate sex education being provided to their peers, but may be unable to do so without adaptations and modifications. Psychologists, counselors, therapists, special educators, and social workers who work with those with autism and developmental disabilities are often called on to supplement sex education, but do not always have the background in both specialized instruction and sex education. This article provides examples of sex education using high-leverage practices for students with disabilities in both clinical and school-based settings. Resources are also provided for teaching sex education, and examples are offered of how sex education can be included in individualized education plans (IEPs).
Keywords
Despite calls for inclusive sex education for students with disabilities (Sexuality Information and Education Council of the United States [SIECUS], 2021), students with autism and developmental disabilities report lower rates of access to sex education than peers with other disability diagnoses, as well as peers without disabilities (Barnard-Brak et al., 2014; Holmes et al., 2022). When school-based sex education is available for those with autism and developmental disabilities, the content is less likely to be comprehensive, leading to reduced knowledge about sex and sexuality (Strnadová et al., 2022). Yet, people with autism and developmental disabilities report similar levels of interest and desire to engage in sexual relationships as those without disabilities (Medina-Rico et al., 2018).
There are a multitude of reasons as to why students with autism and developmental disabilities are less likely to gain access to sex education. United States federal laws do not mandate sex education, leaving sex education school programming decisions up to individual states—few of which require accessible sex education and may therefore not meet the needs of students with disabilities (Schmidt et al., 2021). In addition, parent and educator beliefs that students with certain disabilities will not benefit from sex education programming can serve as a barrier to access (Holmes et al., 2022; Strnadová et al., 2022).
Another barrier to access is educator self-efficacy. Educators who feel proficient at teaching sex education may not have the training to meet the educational needs of students with autism and developmental disabilities. For example, Hole and colleagues (2022) interviewed 19 individuals with intellectual disability about their sex education experiences, finding that many participants reported a lack of accessibility in instruction, largely due to teaching strategies designed for neurotypical audiences that were not supportive in building understanding for neurodiverse audiences. Similarly, educators who are highly skilled in educating students with autism and developmental disabilities may feel uncomfortable addressing sex education topics. Special educators, for example, report low levels of efficacy in teaching sex education topics (Curtiss & Stoffers, 2024; Howard-Barr et al., 2005).
Thus, when sex education is available to individuals with autism and developmental disabilities, it may come from educators who serve in a variety of roles, including teachers, therapists, board-certified behavior analysts (BCBAs), or within community-based agencies (Curtiss & Stoffers, 2024); however, many of these professionals report limited training and education regarding how to teach sex education to those with disabilities (Michielsen & Brockschmidt, 2021). With such an array of potential sex educators and a general lack of self-efficacy, it is unclear who is responsible for providing sex education. Potential educators often suggest that individuals in other professions, such as clinicians, therapists, and social workers, are better equipped to teach sex education to individuals with autism and developmental disabilities (Michielsen & Brockschmidt, 2021).
There are multiple sources to get additional training on teaching sex education. Each year, the Center for Sex Education (CSE; https://www.sexedcenter.org) hosts an annual conference that supports how to teach sex education. The American Association of Sexuality Educators, Counselors, and Therapists (AASECT; https://www.aasect.org) provides a certification process. Unfortunately, the resources do not explicitly provide support at the intersection of sex education and special education. Given these challenges related to access, appropriate instruction, and teacher efficacy, this paper seeks to provide actionable recommendations for those teaching sex education to students with autism and developmental disabilities, utilizing high-leverage teaching practices in both clinical and school-based settings.
High-Leverage Instructional Practices When Teaching Sex Education
High-leverage practices for students with autism and developmental disabilities have consistently been found to be effective at improving student outcomes and have been agreed upon by the Council for Exceptional Children (Aceves & Kennedy, 2024). High-leverage practices are organized into four domains: collaboration, data-driven planning, instruction in behavior and academics, and intensifying and intervening as needed. In the area of instruction in behavior and academics, four of the nine embedded practices in this domain are (a) using strategies to promote active student engagement, (b) providing scaffolded supports, (c) using assisted and instructional technologies, and (d) teaching students to maintain and generalize new learning across time and settings. Outlining these high-leverage practices with specific content areas will illustrate, broadly, how the practices can be applied to sex education topics. In addition, Figures 1 to 4 illuminate the stories of sex educators from school-based and clinical settings. The stories are depicted from authentic situations documented by the authors, with only name changes to provide anonymity. Note that in these examples, there are some content areas (e.g., masturbation) that may only be appropriate to teach in a clinical setting.
Educator Story of Using Role-Playing to Promote Active Student Engagement.
Educator Story of Providing Scaffolding Supports.
Educator Story of Using Assistive and Instructional Technologies.
Educator Stories of Maintaining and Generalizing Learning Across Time and Settings.
Use Strategies to Promote Active Student Engagement: Consent
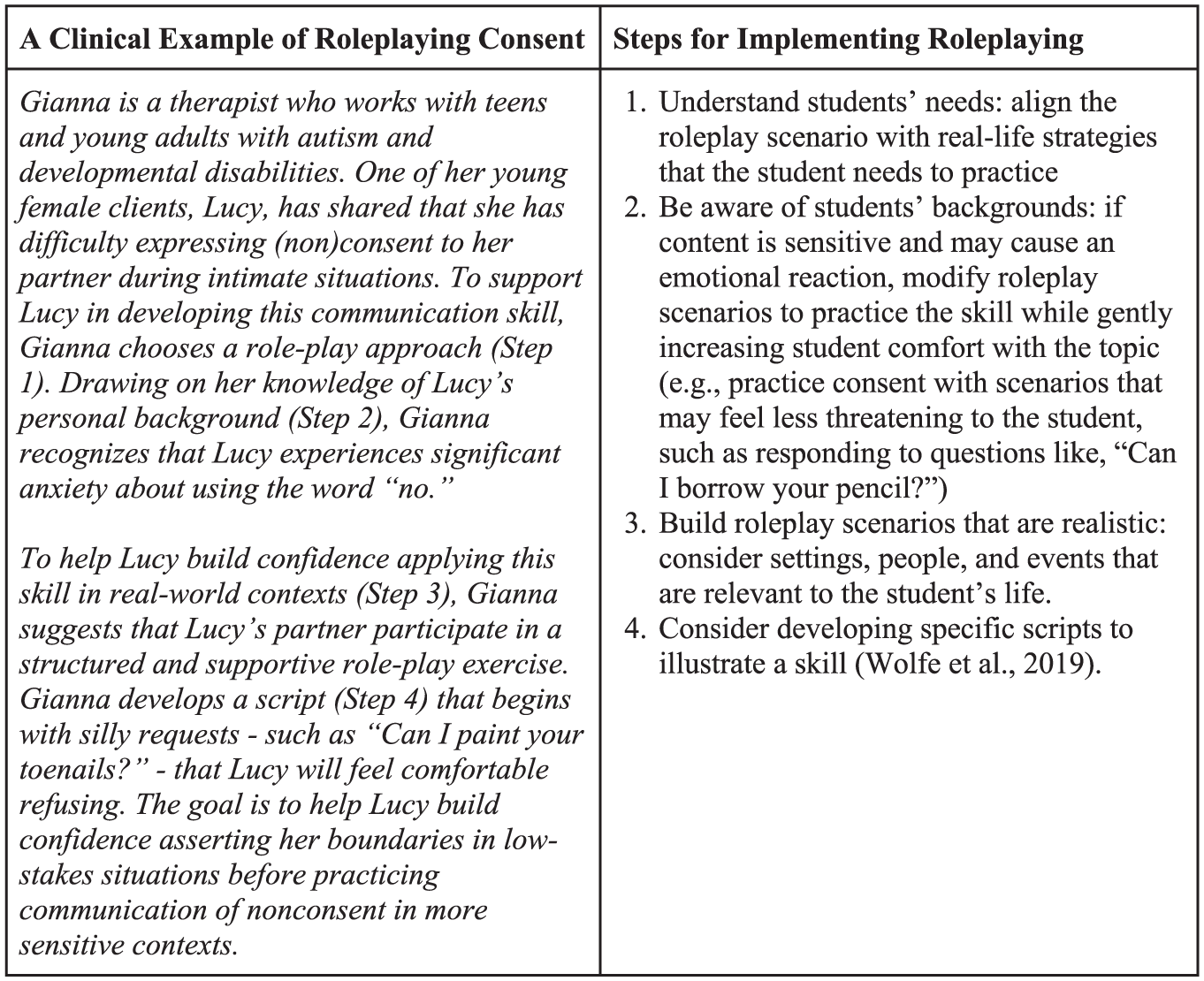
Active engagement is an approach to teaching in which students are given opportunities to interact with one another during learning tasks that expand, apply, or integrate concepts and think about what they are doing (Bonwell & Eison, 1991). One strategy for active engagement is role-playing. Role-playing is based on target content knowledge, provides opportunities to showcase multiple perspectives, involves complex and meaningful situations, and supports students in understanding the meaning behind the activities (McDaniel, 2000). Role-playing is one strategy educators can incorporate when teaching about sexual consent. In Figure 1, the story describes how a therapeutic educator implements role-playing in their instruction to support a student who needed to build confidence to explicitly communicate boundaries. To successfully implement roleplaying, the educator had to consider the sensitive nature of the content and how the student would respond. Having an understanding of the student’s history allowed the educator to plan roleplay scenarios that would address the student’s need, which in this case was to clearly communicate nonconsent by saying, “No,” while also starting with topics that felt non-threatening to the student (e.g., painting toenails). In addition, in this scenario, the educator was able to use a romantic peer to help implement the roleplay, which helped the student consider how these lessons could be naturally applied within her daily life.
Consent is a complex skill that requires communication, decision-making, and self-regulation skills. Ten states mandate that the importance of consent be taught in schools and 27 require the instruction of self-control and decision-making (Guttmacher, 2023). Students with autism and developmental disabilities are at increased risk for sexual abuse and thus explicit instruction on consent is critical (Curtiss & Kammes, 2020). Although consent is highlighted as an example of active engagement in this section, active engagement is a high-leverage practice appropriate across all sex education content areas. The National Sex Education Standards, which can be found at https://siecus.org/wp-content/uploads/2023/12/NSES-2020-web-updated-1-1.pdf, provide grade-based guidelines for appropriate sex education topics such as consent and healthy relationships, sexual health, and interpersonal violence (Future of Sex Education Initiative, 2020).
Use Scaffolding: Masturbation
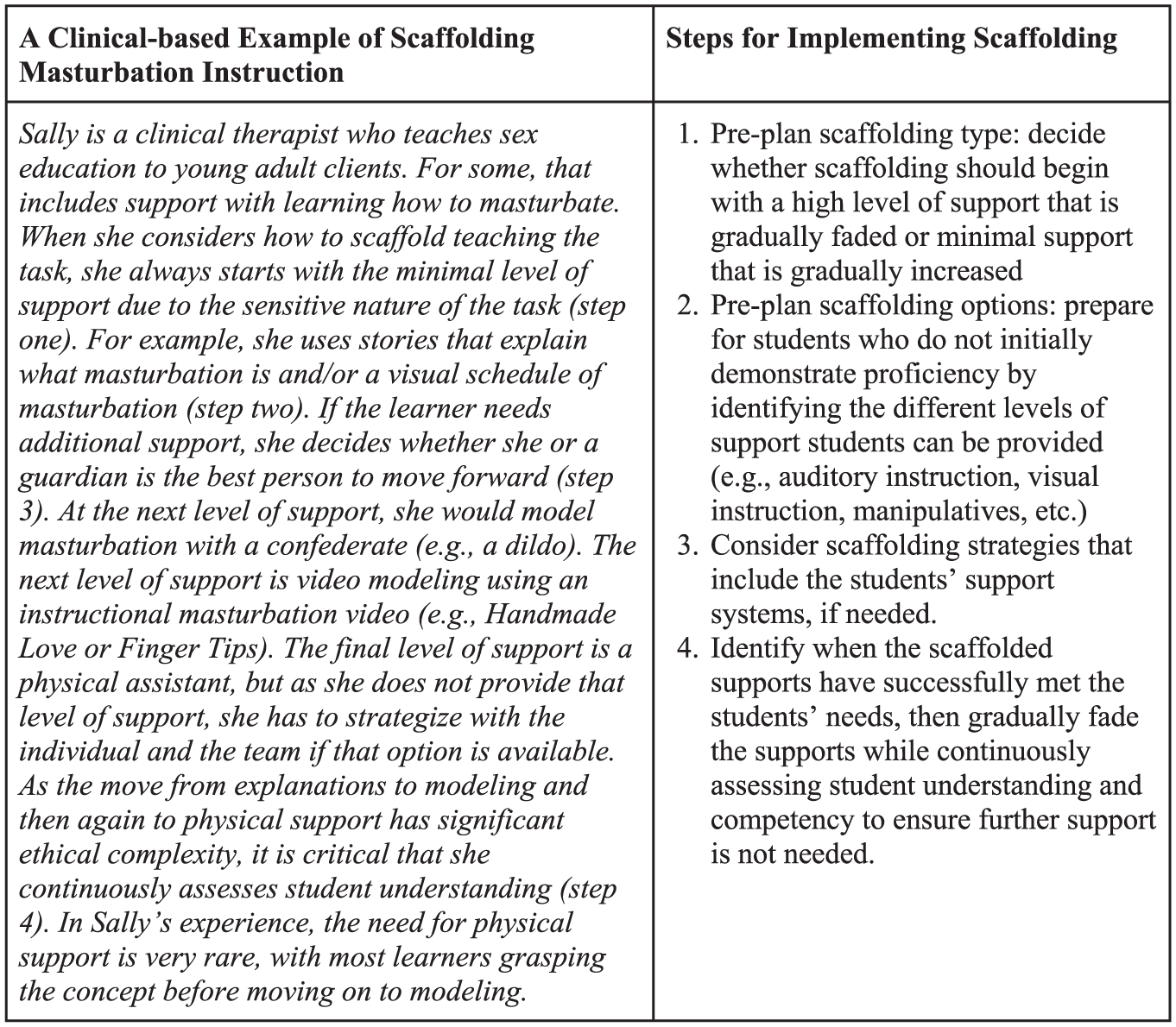
Scaffolding is a responsive form of instructor-initiated support in which the amount and type of support are finely tailored to the learner’s individual needs and progress. Scaffolding is an intensive form of instruction in which the goal is to gradually and intentionally transfer responsibility from the instructor to the learner (van de Pol et al., 2010). As such, the specific types of support provided and the pathway to transferring responsibility are highly individualistic. This type of strategy is typically used when providing one-on-one instruction. In the example provided in Figure 2, a story from a clinical sex educator illustrates how they scaffold the instruction of masturbation from providing the least to the most intensive amount of support. In this example, the educator first provides limited, non-invasive support by offering a simple explanation of masturbation through a story format, but gradually increases the intensity of support if needed. This gradual increase of support includes offering visual cues to support the individual in understanding the steps of masturbation, the demonstration of masturbation using a confederate (e.g., model genitalia), or reviewing a video demonstration. Note that some approaches to scaffolding would start with the maximal amount of support and then fade support as the learner gains mastery, but this path is not ideal in the specific context of masturbation due to the highly sensitive nature of the maximal level of support.
Although it is rare to provide instruction on the mechanics of masturbation, this is an important area of need for many individuals with autism and developmental disabilities. For example, in focus groups with young adults with intellectual disabilities, many reported that they primarily learned about masturbation from pornography (Frawley & Wilson, 2016). The reliance on pornography for sex education is not limited to people with intellectual disability. As individuals age and become more interested in the mechanics of sexual behavior (i.e., 18- to 24-year-olds), a nationally representative sample suggests pornography becomes the most commonly endorsed source (Rothman et al., 2021). Notably, in this study, younger adolescents (14- to 17-year-olds) more often sought out parents and friends for information about sexuality. These findings suggest that early adolescence may be a critical time to provide instruction on masturbation. In addition, knowledge of masturbation is part of the National Sex Education Standards (Future of Sex Education Initiative, 2020). Beyond the topic of masturbation, scaffolding is a critical high-leverage practice for teaching sex education.
Use Assistive and Instructional Technologies: Communicating About Sex Education Topics
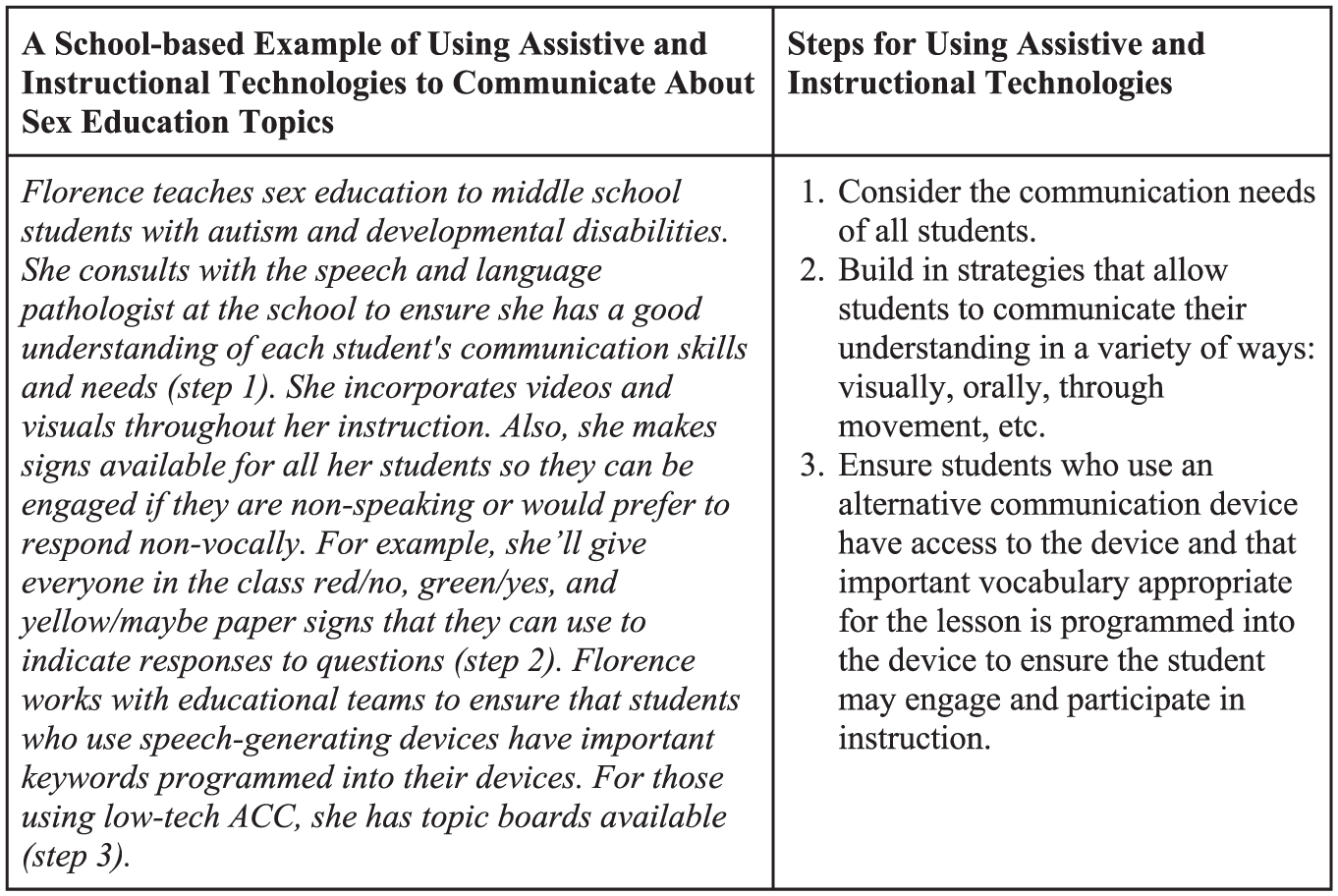
Assistive technologies help students perform tasks, and instructional technologies help students learn; in either case, they can be high-tech or low-tech. An important area of assistive technology is communication—often called alternative and augmentative communication (AAC). Students with autism and developmental disabilities often use AAC to more clearly and fully express their thoughts and ideas. Low-tech examples include using pictures, and high-tech examples include iPads with communication software. Visuals and videos can be useful instructional technologies for sex educators, helping the teacher more fully communicate content and facilitate deeper engagement. In Figure 3, the educator story illustrates how she uses both assistive and instructional technology to support communication and learning. To support students, this educator explains that communication can be supported through low-tech options, such as offering paper in different colors to provide clear responses, as well as high-tech options, like programming appropriate keywords for the topic area on an augmentative and alternative communication device.
Assistive and instructional technologies are another high-leverage practice critical to sex education across topics. When choosing the topics for sex education for students with autism and developmental disabilities, at a minimum, they should be provided with the same content as their same-age non-disabled peers. Some of the most critical topics are consent and healthy relationships, anatomy and physiology, puberty and adolescent sexual development, gender identity and expression, sexual orientation and identity, and interpersonal violence (Future of Sex Education Initiative, 2020). One topic that seems particularly salient to students with autism and is rarely touched upon in sex education is the sensory features of intimacy (Gray et al., 2021).
Maintain and Generalize New Learning Across Time and Settings: Dating and Unwanted Touch
Generalization of learning occurs when a skill is retained across environments, which includes setting, time, and people, beyond where the learning initially took place (Sears & Cornelius, 2023). When a skill is taught, it cannot be assumed that it will generalize to other environments; instead, there must be support put into place to allow students to use learned skills in various settings (Lancaster et al., 2024). As knowledge and skills in sex education often require retention and use in private settings outside of the classroom, such as the use of contraceptives, strategies to support generalization are especially important. Generalization can be encouraged through learning across multiple classroom settings and teachers, as well as through learning experiences that occur within the student’s natural setting (Sears & Cornelius, 2023). Educators can use anecdotal evidence to help evaluate student learning and whether generalization has occurred.
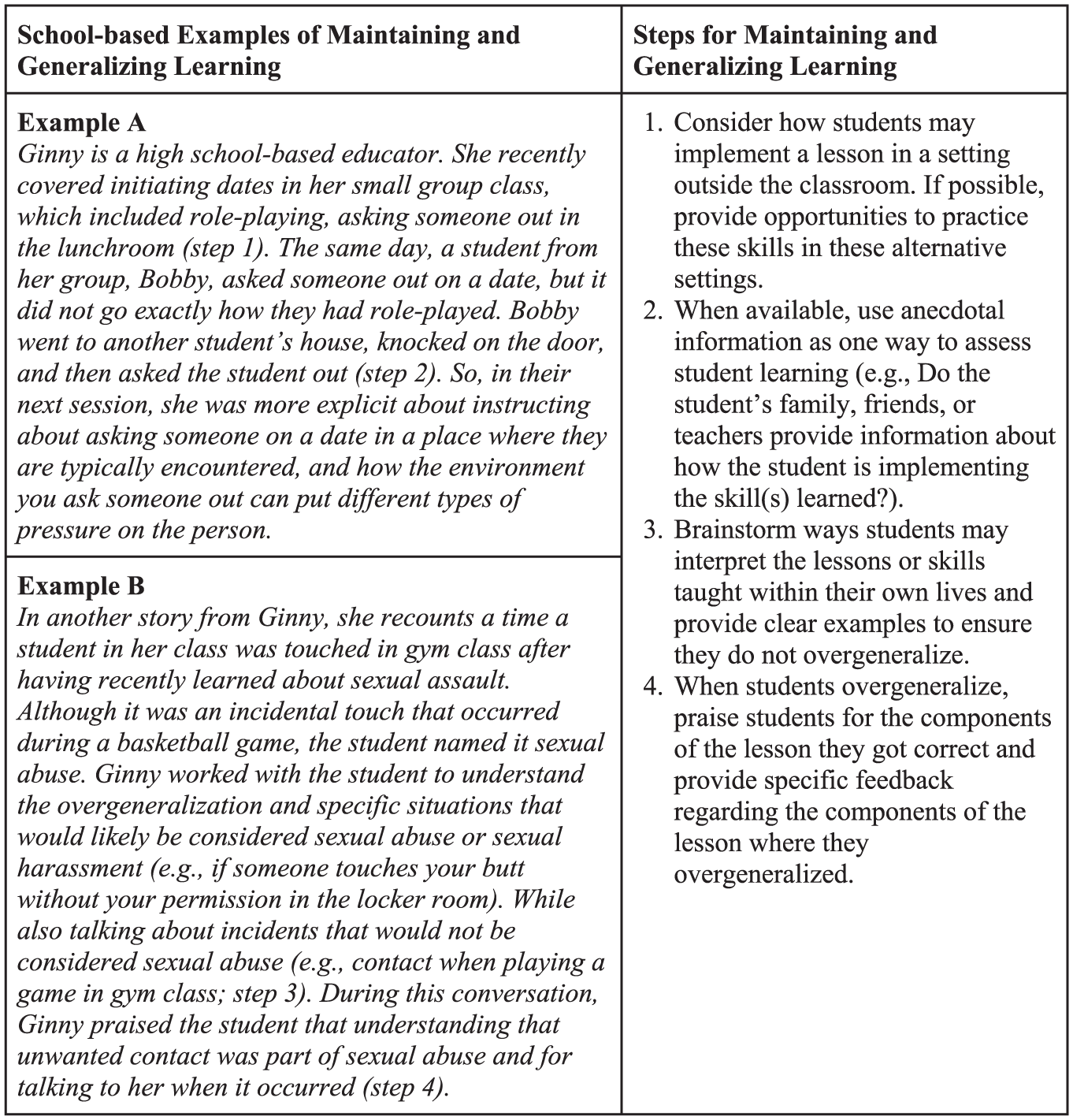
In Figure 4, an educator discusses two instances of students who took the content learned in the classroom and generalized it into their personal lives. In both instances, the students’ actions and behaviors based on their understanding of the content helped the educator find ways to better support these students in comprehending the material. In Example A, the educator was able to hear, anecdotally, how the student applied the classroom lesson about dating within their personal life. Understanding the way in which this student (mis)generalized the instruction helped the educator to modify instruction to support students in understanding important boundaries and norms when pursuing a potential relationship. In Example B, the educator discussed the challenge of overgeneralization, in which a student applied their understanding of sexual assault to an innocuous event that happened in gym class. Through this event, the educator determined that the student was able to generalize skills discussed in class, such as identifying a safe adult to speak to when an event of sexual assault occurs; however, the educator also determined that the student had overgeneralized their understanding of sexual assault to include any unwanted touching, even when accidental.
When teaching sex education concepts, educators should think about the contexts in which students may authentically apply their learning. When possible and appropriate, providing students with the opportunity to implement these skills in various settings, such as across classroom environments or through role-play in community settings, will help students to maintain and generalize their learning. Educators should consider possible misunderstandings that may arise from instruction, such as those described by the educator above, and try to address these possible confusions during the lesson. When available, anecdotal evidence can be a powerful assessment of generalization and provide important feedback about student understanding and potential necessary teaching modifications.
Culturally Inclusive Pedagogies and Practices in Teaching Sex Education
Culturally inclusive pedagogies and practices (CIPPs) are embedded throughout the entirety of the high-leverage practice guidance (Taylor & Harkins Monaco, 2024). Ensuring that students with autism and developmental disabilities receive sex education is inherently a component of CIPP because of the historic exclusion of people with autism and developmental disabilities from domains of sexual life. Having said that, those with autism and developmental disabilities hold intersectional identities that are critical to consider when planning sex education. Particularly salient are sexual identity, gender identity, and ethnicity. The guidance in high-leverage practices for students with autism and developmental disabilities provides important considerations for CIPP that can be applied when teaching sex education: presume competence, engage in professional reflection, prioritize lived experiences, consider language, analyze through an intersectional lens, and connect with disabled communities. Educators are often encouraged to remove their own values from instruction—but there is no clear path toward doing that in the domain of sex education. When sex education is based on the idea that gender is equal, that is a value. Specific values get codified into laws, like abstinence-only or abstinence-first sex education (Kaley, 2020). Basic steps, like representation in instructional materials, are an important step, but CIPP goes beyond representation to consider how sex education can cause harm (Curtiss & Stoffers, 2025). Thus, a learner-centered approach and educator reflexivity are critical for CIPP sex education.
Additional Resources
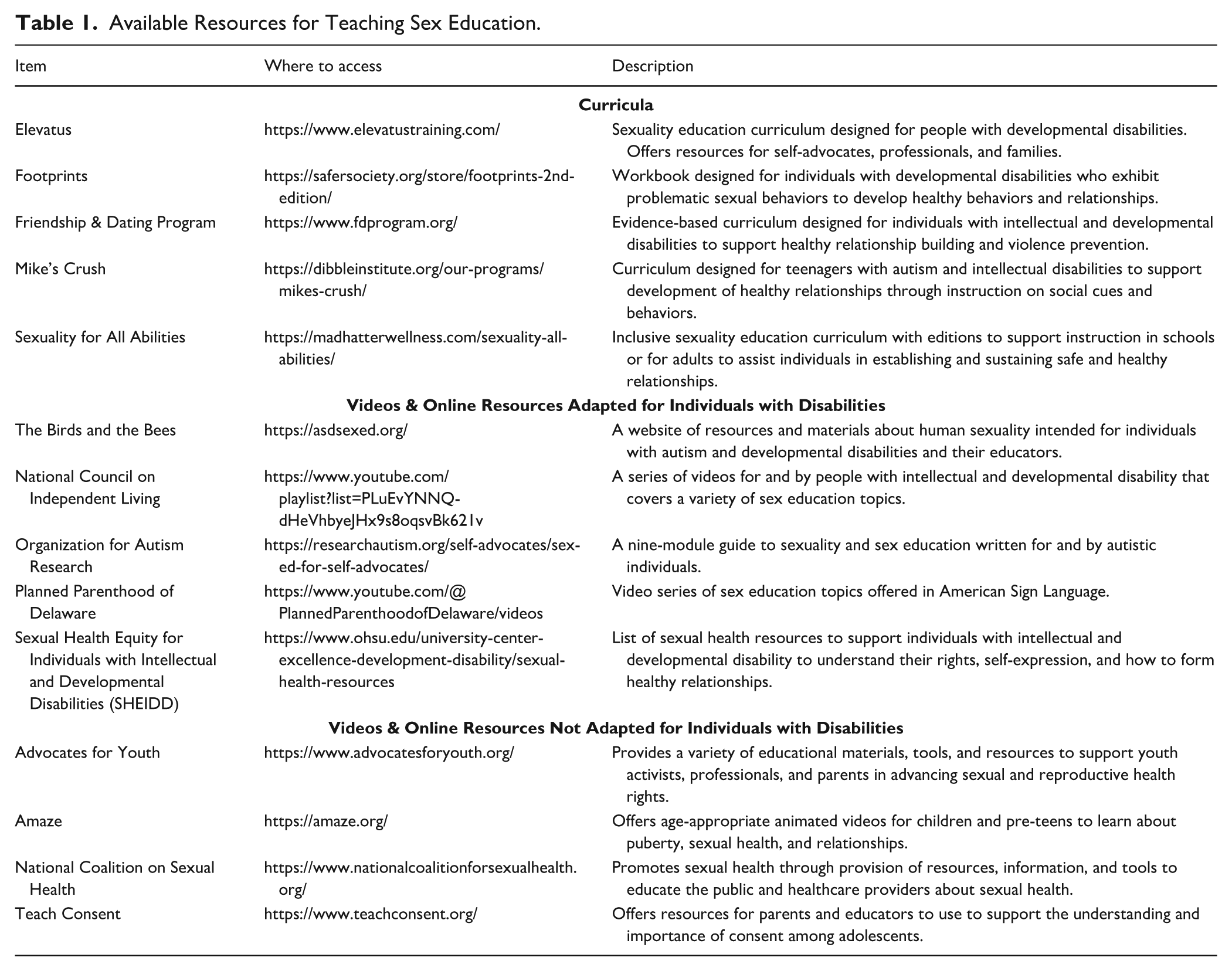
There are a variety of resources for teaching sex education, some of which are disability-specific and others that are not, but many educators and clinicians use them to support their instruction. In terms of adapted resources, Elevatus and Sexuality for All Abilities both have developed comprehensive sex education curricula that are available for purchase (and provide training for educators). The Friendship and Dating Program and Mike’s Crush are two curricula available for purchase that are specifically about dating and relationships. The Organization for Autism Research has free self-paced online modules on a variety of sex education topics. Asdsexed.org has a variety of free resources and lesson plans. The National Council on Independent Living has a series of YouTube videos featuring adults with intellectual disability, and Planned Parenthood of Delaware has YouTube videos in American Sign Language. In addition, there are a variety of free online resources that are not adapted that educators and clinicians who work with students with autism and developmental disabilities find helpful such as Amaze.org, Teach Consent.org, Advocates for Youth, and the National Coalition on Sexual Health. Finally, there is a curriculum for adolescents with disabilities who have sexual behavior problems called Footprints. Table 1 summarizes these resources and how they can be accessed.
Available Resources for Teaching Sex Education.
Sex Education and IEP Goals
One way to ensure students with autism and developmental disabilities are provided with accessible sex education is to write goals in the Individualized Education Program (IEP) that address sex education. Although it is not a common practice, components of sex education can be written into IEPs to ensure students have access to sex education that meets their needs and is being provided to other students at their grade levels. Although IEPs are not used in clinical settings, the goals provide examples of how therapeutic goals in sex education could be written.
There are several entry points for sex education to become part of an IEP, such as (a) when sex education is part of the general education curriculum but may need to be adapted, (b) as part of a behavior intervention plan (BIP), and (c) through related services. In the absence of sex education being written into IEPs, it is common for students with disabilities not to receive any sex education or receive sex education that has not been adapted to meet their learning needs (Holmes, 2021; Holmes et al., 2022). Furthermore, in the absence of appropriate sex education, some people experience sexually inappropriate behavior (Curtiss & Kammes, 2020). To illustrate how sex education can be incorporated into IEPs, three examples (corresponding to the entry points above) have been provided.
In the first example (see Figure 5), sex education is provided in the domain of social skills and is focused on vocabulary related to puberty. In this example, sex education is part of the general education curriculum, but the student data suggests the need for a modified curriculum. Note that this approach aligns with the high-leverage practice domain of data-driven planning, which involves creating action plans in response to student data and analysis (Cornelius et al., 2024). A specialized curriculum may use simplified language to describe biological terms and processes, have more lessons with lesson content covered in each lesson, provide more opportunities to review previously learned content, and use multimodal instructional materials. This goal is ideally introduced proactively; for example, a team member may say at the IEP meeting, “Next year, puberty education is part of the curriculum; let’s discuss what support the student needs to ensure their success with this topic.” Although the goal can also be introduced reactively, I’m concerned because this student only seems to know one change associated with puberty after we covered this material in class. I think this student may benefit from additional instruction in this area that has been modified to make it more accessible.
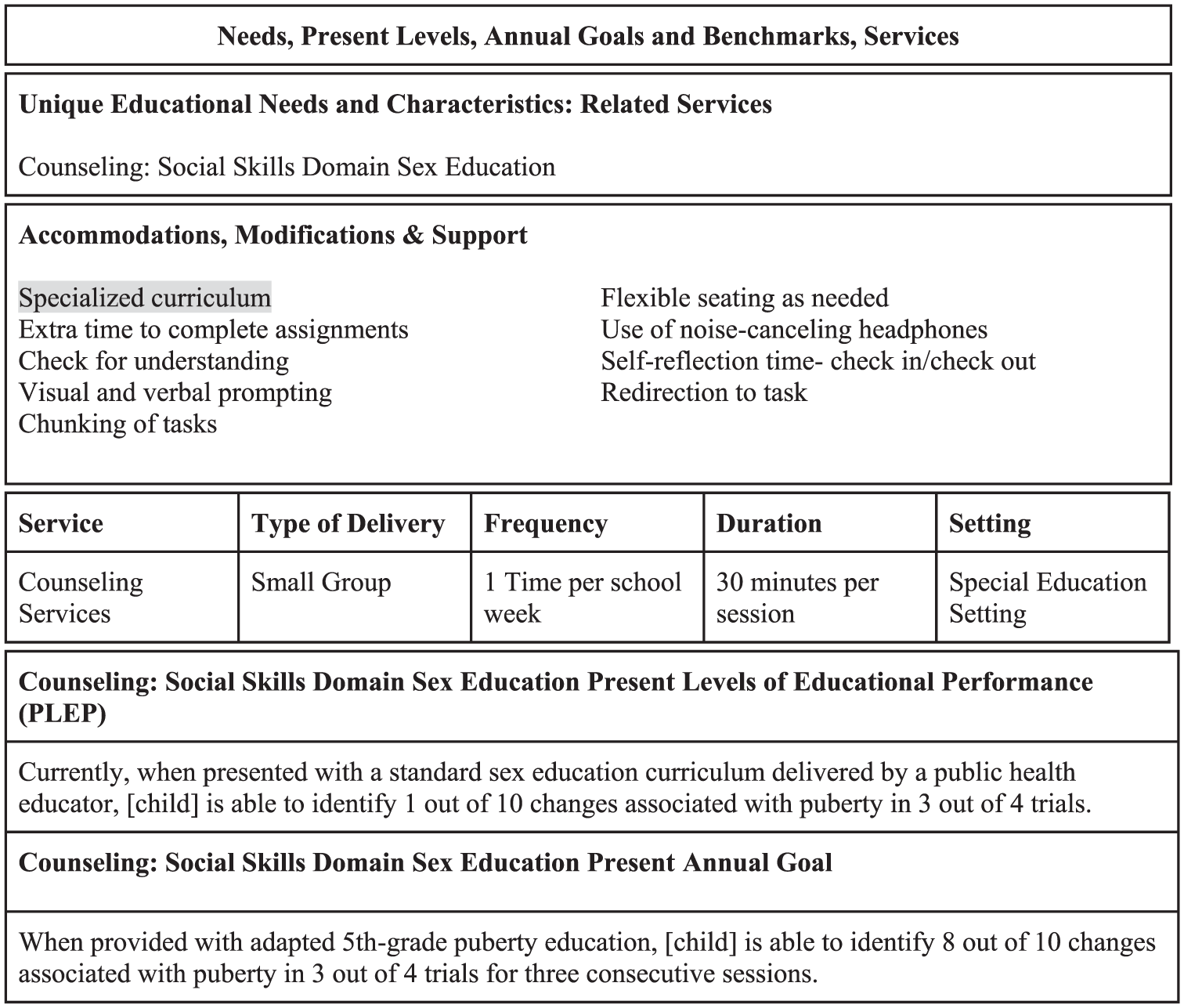
Individualized Education Program (IEP) Example 1: Sex Education Instruction as a Domain of Social Skills (Sex Ed Specific Supports Highlighted in Gray).
Variations on these scripts can help start the conversation about sex education at IEP meetings.
In the second example (see Figure 6), sex education is in the domain of bodily autonomy and is embedded within a BIP. BIPs are developed for students who have problematic classroom behavior that is a manifestation of their disability. Although problematic sexual behavior is unlikely to specifically be a manifestation of a disability, it may be a piece of the function of a behavior that is a manifestation. In our example, the behavior itself is not sexual in nature at all—using physical initiation, which is often inappropriate to the classroom context. But potentially contributing to the function of the behavior may be a lack of understanding of bodily autonomy, norms around respecting bodily autonomy, and understanding of private, public, and semi-public spaces, body parts, and activities. These all fall under the domain of sex education. A student may never receive explicit instruction in these areas without it being written into the IEP. In our example, explicit instruction provides the student with a deeper understanding of why physical touch is perceived as inappropriate and motivates the use of pro-social communication strategies. Note this approach is aligned with the high-leverage practice domain of intensifying and intervening as needed, as it reinforces the importance of a full continuum of instructional supports (Hayes et al., 2024).
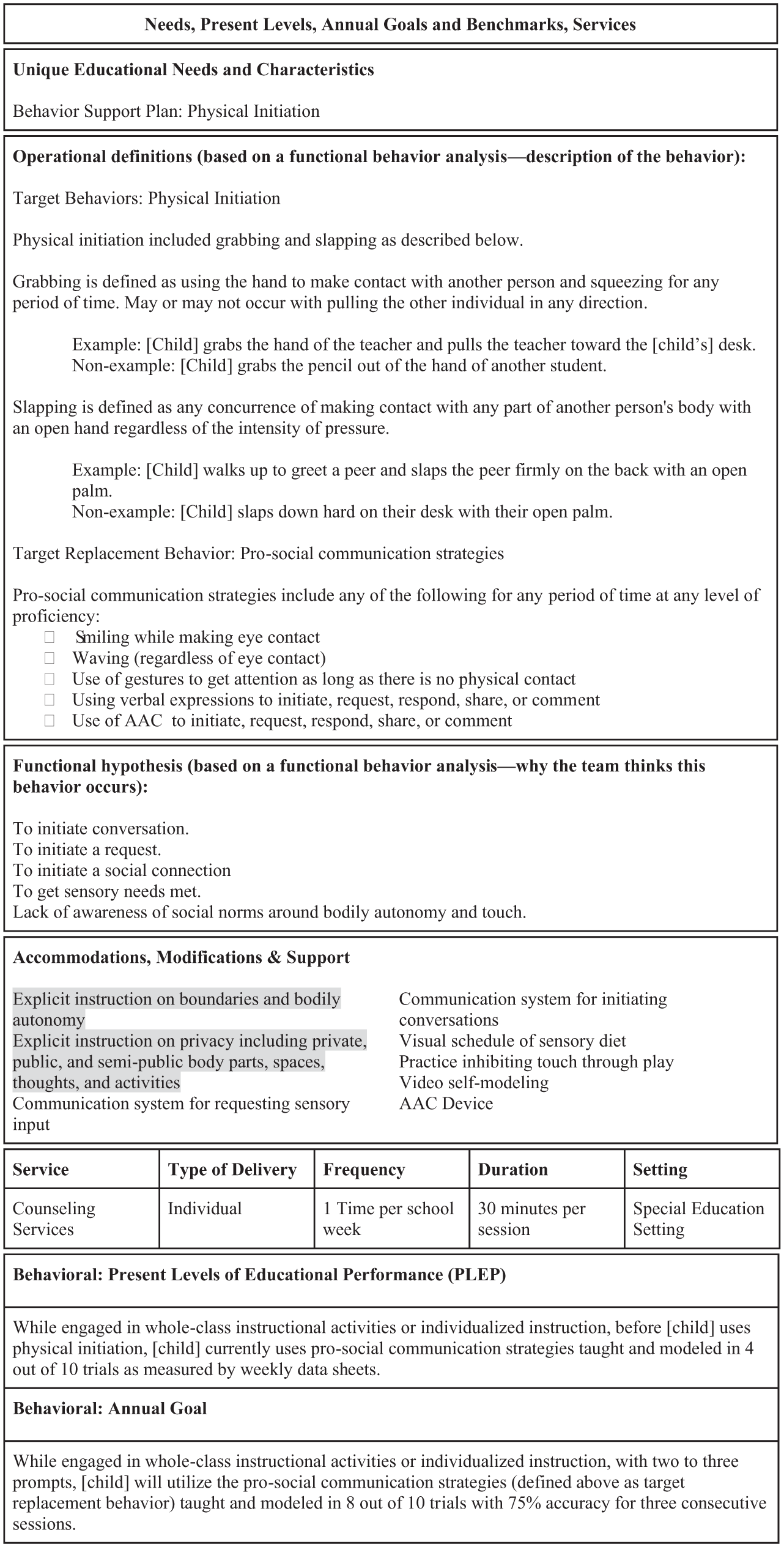
Individualized Education Program (IEP) Example 2: Sex Education Instruction as Part of a Behavior Intervention Plan (Sex Ed Specific Supports Highlighted in Gray).
The third example (see Figure 7) is in the domain of consent, and the goal is focused on communication. This example highlights the role of related services in providing sex education and is aligned with the high-leverage practice domain of collaboration, as it highlights the need to understand a student’s holistic instructional needs and plan for joint progress monitoring and instruction (Billingsley et al., 2024). It may be that a sex education topic, like consent, is covered in the general education curriculum, but not to the extent that an individual student needs. Related services time can provide additional instruction and may be better equipped to support with the socioemotional challenges the topic might raise. In addition, there may be content areas that are particularly important for a specific student, but outside the sex education that is typically provided. This is another case when related services, such as counseling, can help ensure students get the information and skills they need. Notably, in our example, although we included instructions to generalize concepts of refusal to sexualized encounters, the actual measurement of the skill of refusal was for non-sexualized naturalistic opportunities that would exist in the classroom.
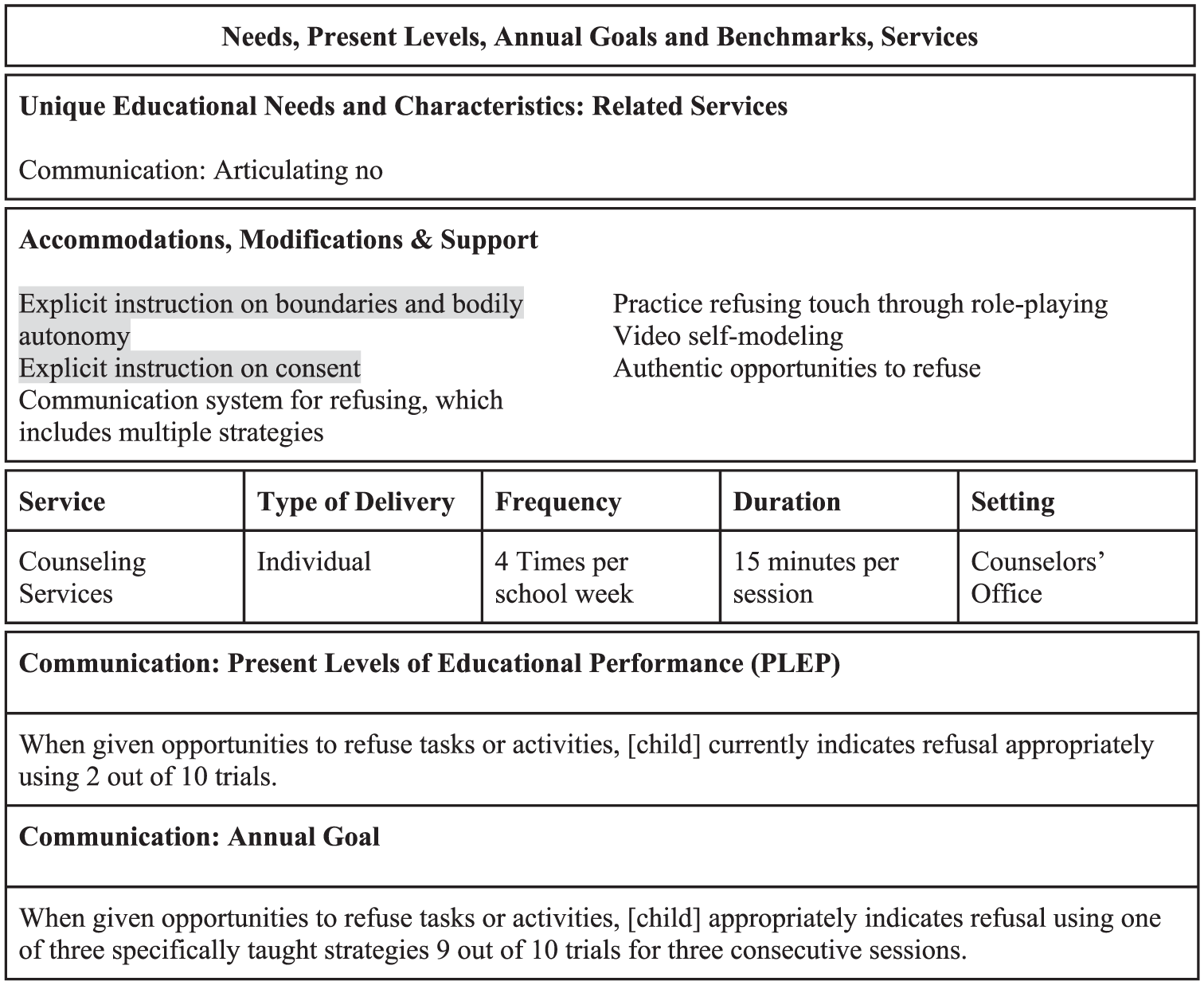
Individualized Education Program (IEP) Example 3: Sex Education Instruction as Part of a Related Services Goal (Sex Ed Specific Supports Highlighted in Gray).
Conclusion
Using examples from practicing sex educators, this paper illustrates how a variety of sex education topics can be taught using four high-leverage practices: active student engagement, scaffolded supports, assisted and instructional technologies, and generalization. Through these examples, resources are provided for instruction in different areas. Finally, included examples offer suggestions for how to incorporate sex education into IEPs.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.