
Abstract
Background
Chronic low back pain (cLBP) is a global health complaint. Acupuncture is an effective therapy for cLBP; however, evidence for an optimal acupuncture practice scheme is limited.
Objective
This study aimed to determine the feasibility of conducting a randomized controlled trial (RCT) to assess the effectiveness of two acupuncture regimes (sensitized-points acupuncture and routine integrative acupuncture package) for cLBP.
Methods
This was a two-arm, assessor-blind, randomized-controlled feasibility study. Thirty adult participants with cLBP were randomly assigned into two groups. Each group received 8 sessions of either sensitized-points acupuncture or routine integrative acupuncture package, respectively. Treatments were conducted twice per week. Outcomes were assessed at baseline (week 0), on a weekly basis for four weeks (week 1, 2, 3, 4), and follow-up (week 12). Student's t-tests, Mann-Whitney U tests, Fisher's exact tests, descriptive analyses, and power analyses were used for statistics.
Results
Participants were recruited over 10 weeks with a recruitment rate of 12 participants per month. The treatment plan in both groups was well accepted and tolerated. Besides, the study was characterized by low adverse event rates (8.0% in Group A, 11.7% in Group B), high completion of the outcome measures (97.8% in Group A, 94.3% in Group B), and high participant retention rate (100% in Group A, 93.8% in Group B). Furthermore, preliminary analyses showed that both regimes of acupuncture were potentially efficacious and safe.
Conclusions
Conducting a fully powered RCT to evaluate efficacy and safety of two acupuncture regimes in the management of cLBP is feasible.
Introduction
Chronic low back pain (cLBP) is a worldwide health complaint, which is defined as back pain that lasts for more than three months. 1 Low back pain (LBP) is a recurrent condition, according to a systematic review of prospective cohort studies, 65% of patients with LBP still report pain 1 year after the onset. 2 In New Zealand, an epidemiological study including approximately 300,000 participants suggests that the prevalence of cLBP among adults is 9.1%, with nearly one-third of these individuals reporting social deprivation. 3 It's reported that low back pain is the dominant cause of years lived with disability globally, with the figure substantially increasing from 1990 to 2017. 4 An epidemiological survey highlighted that the disability, unemployment, depression, and sleep disorders associated with cLBP, result in a significant burden on both individuals and society at large. 5
There are a variety of treatments utilized for cLBP; generally, these are classified as either non-pharmacological, pharmacological, or invasive. 1 Among them, acupuncture treatment is strongly recommended by American College of Physicians as a first-line, non-pharmacologic intervention for cLBP. 1 Nonetheless, there is little consensus on the most effective and optimal form of acupuncture for cLBP; hence a wide variety of diverse regimes of acupuncture are utilized by different practitioners. A review indicates that distinct acupuncture protocols yield varying therapeutic outcomes. 6 Various factors contribute to the diversity of acupuncture techniques, including the selection of acupoints, duration of needle retention, needle gauge, etc. 6 To maximize the effectiveness of acupuncture, it's important to understand the role that each factor plays in the treatment. Among these factors, choosing the most suitable acupoints for stimulation is an essential part of successful treatment: it not only includes the optimal prescription of points, but also accuracy in locating points. 7 The foundational Chinese medicine classic The Inner Canon of yellow emperor instructs practitioners to palpate acupoints to find the most sensitive site before inserting needles. Due to the overwhelming demands on acupuncturists, palpation is neglected as part of routine clinical practice. Alternatively, a simplified practice regime, targeted at sensitized acupoints, might offer potential benefits over the conventional approach. 8 However there has been limited direct ‘head to head’ comparisons of these approaches, and it requires a randomized controlled trial (RCT) to provide robust evidence. Before conducting such a full-scale trial, a feasibility study is needed in advance. We hypothesized that the proposed study design and methodologies are practical, and that the interventions can be feasibly and effectively implemented in patients with cLBP.
The primary objective of the study was to investigate the feasibility of conducting a full-scale study comparing the effectiveness of sensitized-points acupuncture and a routine integrative acupuncture package (routine acupuncture plus dry cupping). Additionally, the study aimed to assess the effectiveness of sensitized-points acupuncture compared with routine integrative acupuncture in reducing pain severity, improving physical function and quality of life in patients with cLBP.
This study is reported under the guidance of the CONSORT statement extension recommendations to randomized pilot and feasibility trials 9 (Appendix A). The protocol of this study is available online. 10
Methods
Study design
This was a two-arm, assessor-blind randomized controlled feasibility study to investigate the feasibility of an RCT of sensitized-points acupuncture and routine integrative acupuncture package (routine acupuncture plus cupping) for cLBP. 30 participants were randomly assigned in a 1:1 ratio into two groups. 10 Each group received eight sessions of either sensitized-points acupuncture (Group A) or routine integrative acupuncture (Group B) over four weeks. Outcomes were assessed at baseline, during treatment (after completion of the 2nd, 4th, and 6th treatment session), post-treatment (after completion of the 8th treatment session), and follow-up (week 12). The schedule of the program was displayed in Appendix B.
The study was registered at Australian New Zealand Clinical Trials Registry (ANZCTR, Ref no.: ACTRN12621001426875). Ethical approval was granted by Health and Disability Ethics Committees (HDEC, reference no. 2022 FULL 11076).
Participants
Participants were recruited in the local community via study flyers and online advertisements. Eligible patients were adults (aged ⩾ 18 years old); met the diagnostic criteria of cLBP (ICD 11, MG30.02) according to NICE clinical guideline (NG 59) 11 ; had pain for more than 3 months; with an average score of Numeric Pain Rating Scale (NPRS) ⩾3; and provided informed consent. Participants were excluded if they reported serious spinal disorders (such as malignancy, vertebral fracture, spinal infection, inflammatory spondylitis, cauda equine compression) or comorbidities (such as serious internal disorders in respiratory, circulatory, endocrine, urinary, digestive, neurological system), clotting disorders, scheduled surgery, current or scheduled pregnancy, post-partum lactation period; received acupuncture in the last 4 weeks; had a restricted ability to make independent decisions about their participation; or were unable to communicate in English or Chinese.
Randomization and allocation concealment
Eligible participants were randomly assigned to one of the two groups by a clinical research administrator (D.J.). The randomization sequence was generated using a computer program to ensure randomness. To maintain allocation concealment, each random number was placed in a sequentially numbered, opaque, sealed envelope.
Blinding
Given the nature of the interventions, patients and practitioners were not blinded to the treatment assignments. Data collection was carried out by an independent research assistant (G.H.) who was blinded to the randomization.
Intervention
The primary intervention group received only acupuncture at sensitized-points, while the routine care group received routine integrative acupuncture package that conventional acupuncture was applied at designated routine acupoints, and dry cupping was performed after removing needles. The details of the clinical setting and interventions have been described in the protocol. 10 Generally, both acupuncture and cupping have fewer severe side effects compared to pharmacological treatments and surgery. The most common adverse event of acupuncture is bleeding or pain at the penetration site, which occurs in 1.14 per 1000 patients. 12 However, both acupuncture and cupping require multiple sessions, which can be relatively time-consuming. Additionally, treatment outcomes are closely associated with the skills and experience of the practitioners. Thus, it's crucial to find a licensed acupuncturist.
Routine integrative acupuncture group
The treatment followed the theory of traditional Chinese medicine that patients were treated individually, in line with syndrome differentiation. Bilateral BL 23, BL 25, BL 40 were chosen as main acupoints. 13 Up to two adjunct acupoints were chosen according to syndrome differentiation, as recommended by clinical guideline and experienced acupuncturists (Appendix C). Treatment was performed by a formally trained acupuncturist, with at least 5 years of clinical experience. Patients were asked to maintain a prone position for treatment. Selected points were inserted and stimulated by sterile, single-use filiform acupuncture needles (Hwato needle, Suzhou, China; 25–40 mm in length; 0.25 mm in diameter) until achieving Deqi sensation. 14 Needles were retained for 30 min, during which manual stimulation (lifting-thrusting, and twirling method) was used every 10 min to maintain the sensation of Deqi.
After removing needles, dry cupping was performed as an adjunct method to routine acupuncture. Four round-shaped vacuum suction cups with an internal diameter of 57 mm (GuoYiYan vacuum cups, Beijing, China) were placed bilaterally in the lumbar region from L1 To L5 vertebrae, with cups 3 cm apart. 15 The cups were sucked three times by a pump to produce medium suction force, 16 and were retained for ten minutes.
Sensitized-points acupuncture group
Pain-sensitized points around bilateral BL 23, BL 25, BL 40 were chosen as the main acupoints. 7 In addition, up to two adjunct acupoints were chosen from pain-sensitized sites around bilateral Jiaji Points along L1-L5 vertebrae. 13 To identify pain-sensitized points, detection started at the documented acupoint location, using the tip of the right thumb to apply pressure, then moving the thumb spirally around the point within a circular area of 2 cm diameter. Even downward force was applied gradually on each point. The most painful point around each routine acupoint was identified by patients and marked with a washable pen. 7 Detection of sensitized points was performed prior to each treatment session, given the potential for changes as treatment progresses. Acupuncture needles were manipulated as described above for the routine acupuncture group by the acupuncturist.
Acupuncture in both groups was administered for eight sessions, twice weekly, over four consecutive weeks.17–19 Cupping in the control group was performed once per week as it took time to resolve the bruising produced by the cups. 20
Outcome measures
Recruitment rate
Treatment compliance
Adverse event rate
Completion of the outcome measures
Participant retention rate
This referred to the average number of participants being recruited per month. The recruitment period was expected to be five months.
21
Thus, completion of enrolment and randomization of 6 participants per month was regarded as a success for the recruitment strategies.
Participants’ compliance to treatment was observed by reviewing participants’ attendance record. In this study, a 75% compliance rate was considered acceptable.
22
This referred to the percentage of participants who reported adverse events; less adverse events indicated safer application. An adverse event rate of less than 20% was regarded as acceptable.12,23
This referred to the amount of missing data in questionnaires. At least 75% completeness of data was regarded as acceptable.
24
This was calculated as the percentage of randomized participants who completed follow-up assessment. 80% retention to final follow-up of those randomized was regarded as acceptable in this study.25,26
1. Numeric Pain Rating Scale (NPRS) 2. Roland-Morris Disability Questionnaire (RMDQ) 3. The short-form version of the Depression Anxiety Stress Scales (DASS-21) 4. 12-Item Short-Form Health Survey (SF-12)
NPRS is one of the most frequently used instruments in assessment of pain severity. It's an 11-point numeric scale scoring from 0 to 10 points. “0” represents “no pain”, and “10” represents “the worst pain imaginable”. NPRS has been shown to have high reliability and validity in subjective chronic pain detection.
28
Participants were asked to rate their current pain intensity, the worst pain intensity in the last 24 h, and the least pain intensity in the last 24 h. The final score is calculated as the average of three independent ratings. A higher score indicates worse pain intensity.
RMDQ is a sensitive, reliable and valid self-administered questionnaire that evaluates impairments of physical function from low back pain.
29
This scale contains 24 items, each item scores 1 point if in line with the description. The higher score represents more severe disability.
DASS-21 is a valid and reliable tool to assess three subdomains: depression, anxiety and stress.
30
Each subscale contains seven items. A higher score indicates worse emotional condition.
SF-12 health survey is a reliable and valid instrument to assess quality of life in patients living with chronic diseases, which comprises physical component summary (PCS) and mental component summary (MCS). 31 Higher score represents better health, and vice versa.
5. Acupuncture Expectation Scale
The Acupuncture Expectation Scale was used at the outset of the trial to rate participants’ expectation related to acupuncture effect on cLBP. The score is positively proportionate to positive expectancy towards acupuncture. This scale has demonstrated satisfactory internal consistency and construct validity.
32
6. Utility of Combined Treatments 7. Client Satisfaction Questionnaire (CSQ-8)
The number of participants who received supplementary treatments during the 4-week episode of treatment in each group was analyzed.
This was a brief but valid and reliable scale to retrospectively estimate participants’ attitude and acceptability toward the treatment they received. Overall score ranges from 8 to 32, with higher score representing higher satisfaction.
33
Data analysis
Mean (Standard deviation, SD) or Median (Interquartile range, IQR) were used to describe continuous variables according to the normality of the distribution, and frequency was used to describe categorical variables.
In the baseline analysis, student's t-tests, Mann-Whitney U tests, and Fisher's exact tests were applied to detect the comparability of the two groups.
Primary analysis was the feasibility assessment by calculating the percentages of treatment compliance, adverse events rate, completion of questionnaires, participants’ retention rate; as well as average number of participants recruited per month.
As a feasibility study, descriptive analysis was applied to clinical data, rather than hypothesis testing. 34 Changes in effectiveness outcomes before, during, and after treatment were described.
In addition, power analyses were carried out using effect sizes calculated on the average NPRS score and RMDQ scale at discharge in two groups to achieve a two-sided significance level of 0.05 and power of 80%. The drop-out rate was 10%.
Feasibility analyses and effectiveness analyses were performed with R (Version 4.2.2, R Development Core Team, New Zealand). Power analyses were conducted by G*Power (Version 3.1.9.6, Erdfelder, Faul, & Buchner, Germany). 35
Results
From 9 May 2022 to 12 July 2022, 73 participants contacted the research group to show their interest in participation. 40 participants were eligible after screening, and 30 of these consented to the study. The participants were randomly assigned to the experimental group (Group A, n = 14) or the control group (Group B, n = 16). The flow diagram of participants in each stage of the study is presented in Figure 1.
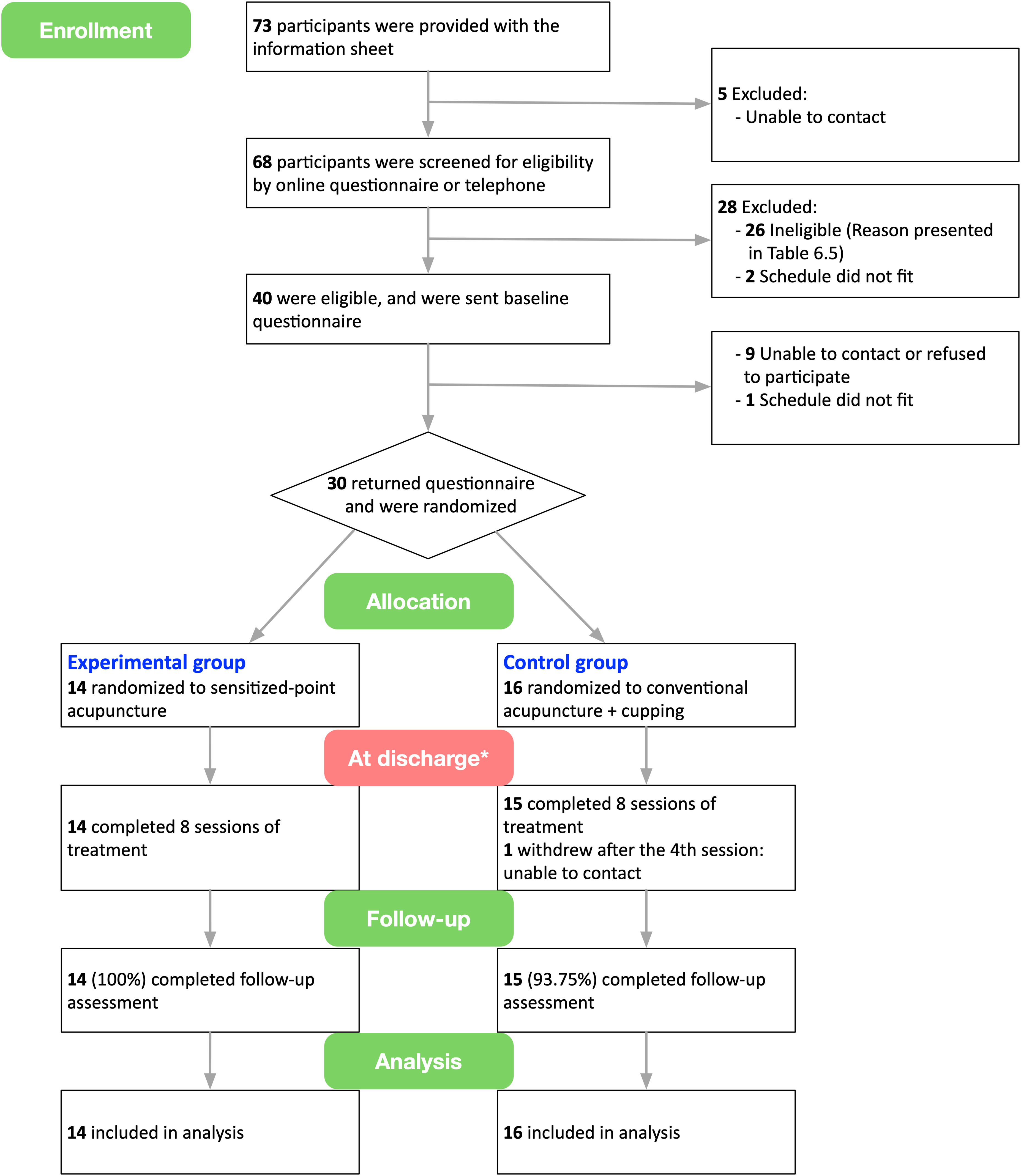
Flowchart of participants throughout the study. *The primary outcome point.
Demographical characteristics
The majority of participants were middle-aged females with diverse ethnicity. The average BMI in the two groups was higher than standard reference value, which suggested that participants in both groups were generally over-weight; this was in accordance with the generally described epidemiological features of cLBP. 36 Participants had different educational levels ranging from less than high school to doctorate. The majority of participants didn’t smoke but most drank alcohol occasionally. These features suggested that the enrolled participants represented the general population, rather than only targeting a particular group. Statistical analysis showed no statistically significant differences between groups in these parameters (P > 0.05), indicating that the randomization was successful (Appendix D).
Health characteristics and expectation towards acupuncture
The back pain in both groups was considered as moderate severity with an average NPRS score of 4.95 ± 1.15 in Group A, and 5.29 ± 1.38 in Group B. The median score of RMDQ was 7.00 ± 5.75 in Group A, and 7.00 ± 3.25 in Group B, indicating there was slight physical function impairment due to back pain in participants in both groups. As participants in Group B received conventional acupuncture, the diagnosis of syndrome differentiation was performed. The patterns of syndrome differentiation presented cold dampness (6, 37.5%), kidney deficiency (5, 31.3%), and blood stasis (5, 31.3%).
The scores of DASS-21 and SF-12 suggested that there was physical health impairment, but no clinical level of mental illness observed in patients of both groups. Student's t-tests and Mann-Whitney U tests suggested that there was no statistically significant difference in pain intensity, physical function, emotional status, or quality of life between the two groups (P > 0.05). The average score of expectation towards acupuncture treatment was 12.64/20 in Group A, compared with 11.69/20 in Group B, without a statistically significant difference between groups (P > 0.05). The statistics of the health characteristics of the population in the two groups are displayed in Appendix E and F.
Primary outcomes: Feasibility analysis
Recruitment rate
Seventy-three participants showed interest in the study, and sixty-eight (93.2%) of them were screened for eligibility. Among which, twenty-eight participants were excluded (Figure 1). The main reasons for exclusion included low pain level with NPRS < 3, serious systematic disorders, the use of acupuncture in the previous 4 weeks, and the use of anticoagulant agents. Forty participants met the inclusion/exclusion criteria, thirty of whom completed the baseline assessment and signed the consent form. There was an average of 3 participants enrolled each week over 10 weeks.
Treatment compliance
Participants were required to receive treatment twice per week. Nevertheless, as the treatment was conducted under the COVID-19 restrictions, the treatment compliance was impacted to some extent. There were 21 (70.0%) participants with 100% compliance with the treatment plan, whereas the treatment schedule of the other 9 participants was disturbed by various factors, including COVID-related issues, business, accidents. Among them, 8 participants returned to the regular treatment once they were recovered or back from the trip. Only 1 participant dropped out following an accident and was unable to be contacted. Despite the pandemic, the treatment compliance was considered satisfactory.
Adverse events
The most common adverse event during the study was slight bleeding at the point of needling. Beyond this, other adverse events included slight bruising and pain around the area of needling, mild dizziness and nausea. All the events were transient and minor. The treatments delivered in both groups were considered safe with an acceptable adverse event rate of 8.0% in Group A, and 11.7% in Group B.
Completion of the outcome measures
The completion rate of questionnaires was 97.8% in Group A and 94.3% in Group B, which exceeded the pre-defined threshold of 75% (Appendix G).
Participant retention rate
One participant dropped out after the fourth acupuncture treatment, and all remaining participants completed the follow-up assessment. The retention rate was 100% in Group A, and 93.8% in Group B, which met the priori criteria of 80%.
Secondary outcomes
The mean differences and 95% confidence intervals (CIs) of clinical outcomes from baseline to each assessment time point were presented in Table 1 and Appendix H.
Mean differences and 95% confidence intervals (CIs) of effectiveness outcomes in two groupsa over 12 weeks.
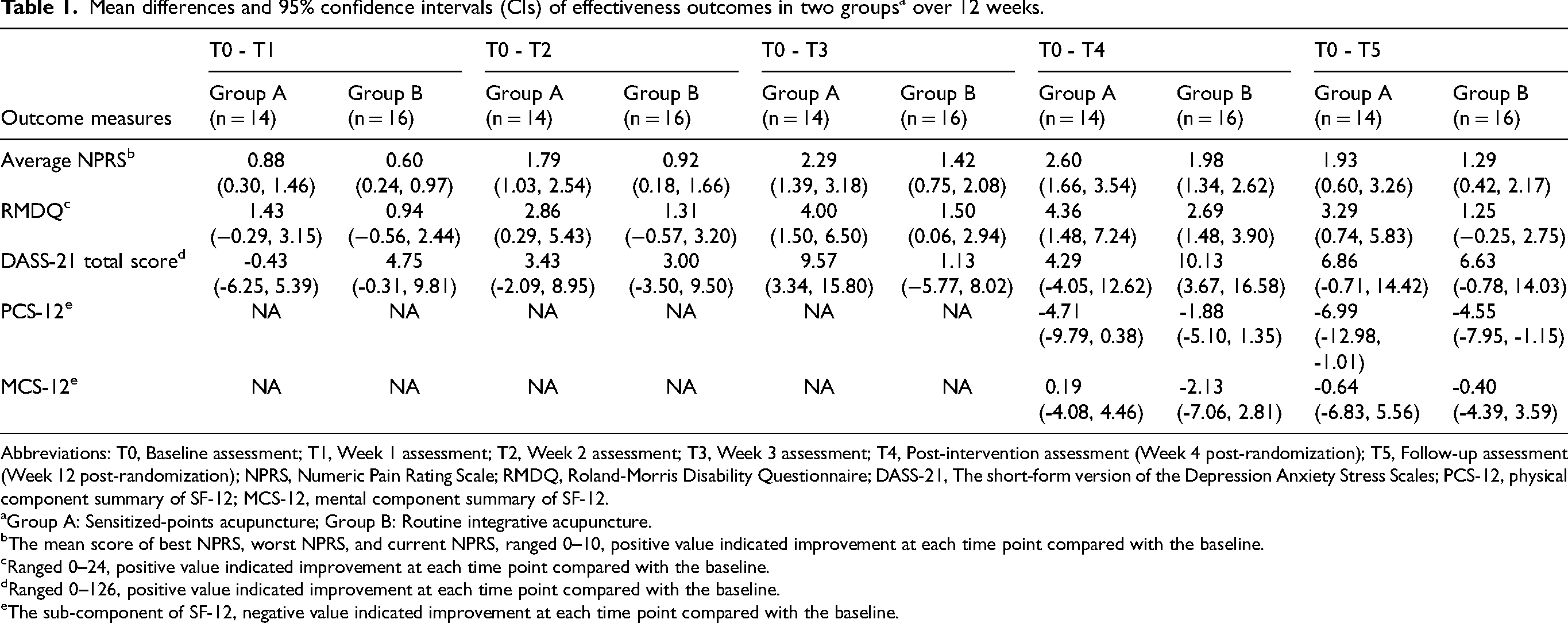
Abbreviations: T0, Baseline assessment; T1, Week 1 assessment; T2, Week 2 assessment; T3, Week 3 assessment; T4, Post-intervention assessment (Week 4 post-randomization); T5, Follow-up assessment (Week 12 post-randomization); NPRS, Numeric Pain Rating Scale; RMDQ, Roland-Morris Disability Questionnaire; DASS-21, The short-form version of the Depression Anxiety Stress Scales; PCS-12, physical component summary of SF-12; MCS-12, mental component summary of SF-12.
Group A: Sensitized-points acupuncture; Group B: Routine integrative acupuncture.
The mean score of best NPRS, worst NPRS, and current NPRS, ranged 0–10, positive value indicated improvement at each time point compared with the baseline.
Ranged 0–24, positive value indicated improvement at each time point compared with the baseline.
Ranged 0–126, positive value indicated improvement at each time point compared with the baseline.
The sub-component of SF-12, negative value indicated improvement at each time point compared with the baseline.
The clinical outcomes of the interventions
Pain intensity
Table 1, Figure 2, and Appendix H demonstrated the average NPRS score of the participants in both acupuncture treatment groups consistently declined as the number of acupuncture sessions increased. Both practice protocols of acupuncture exhibited a positive effect on cLBP. At discharge (T4), the mean average NPRS score was reduced by 2.60 points (95% CI [1.66, 3.54]) compared with the baseline level (T0) in Group A, while the reduction of the mean average NPRS score in Group B was slightly lower than the experimental group, with a figure of 1.98 points (95% CI [1.34, 2.62]); The between-group difference of average NPRS score was 0.96 points at discharge. The average pain intensity in both groups gradually increased in the eight weeks after the completion of treatment (T5). However, it was still lower than the baseline level.
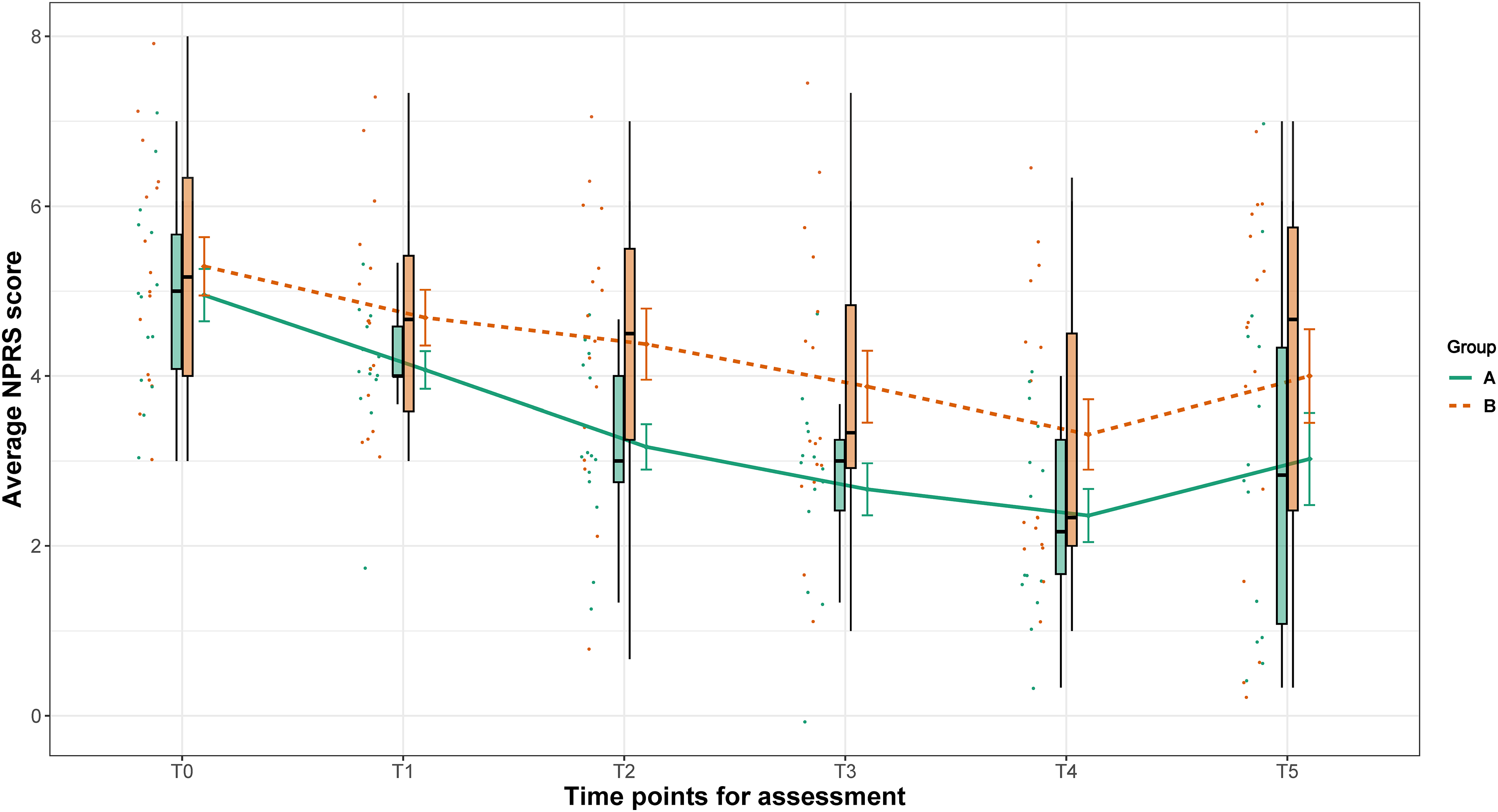
Average pain intensity of participants in two groups at six time points*. *T0, Baseline assessment; T1, Week 1 assessment; T2, Week 2 assessment; T3, Week 3 assessment; T4, Post-intervention assessment (Week 4 post-randomization); T5, Follow-up assessment (Week 12 post-randomization). Raincloud plots indicated the distribution of raw data; Dash lines indicated the changes of means with error bars indicating standard errors.
Physical function
Continuous reduction in the RMDQ scale was seen in both treatment groups as the number of treatment sessions increased. At discharge from treatment (4 weeks), participants reported the lowest level of functional impairment throughout the trial. In Group A, a mean decrease of 4.36 points (95% CI [1.48, 7.24]) was seen in RMDQ scores between baseline and post-treatment; Meanwhile, the mean decrease was 2.69 points (95% CI ([1.48, 3.90]) in Group B before and after treatment. At follow-up, the scores in both groups were slightly elevated but still lower than the baseline level with mean differences of 3.29 points (CI 95% [0.74, 5.83]) in Group A, and 1.25 points (95% CI [-0.25, 2.75]) in Group B (Table 1, Figure 3, Appendix H).
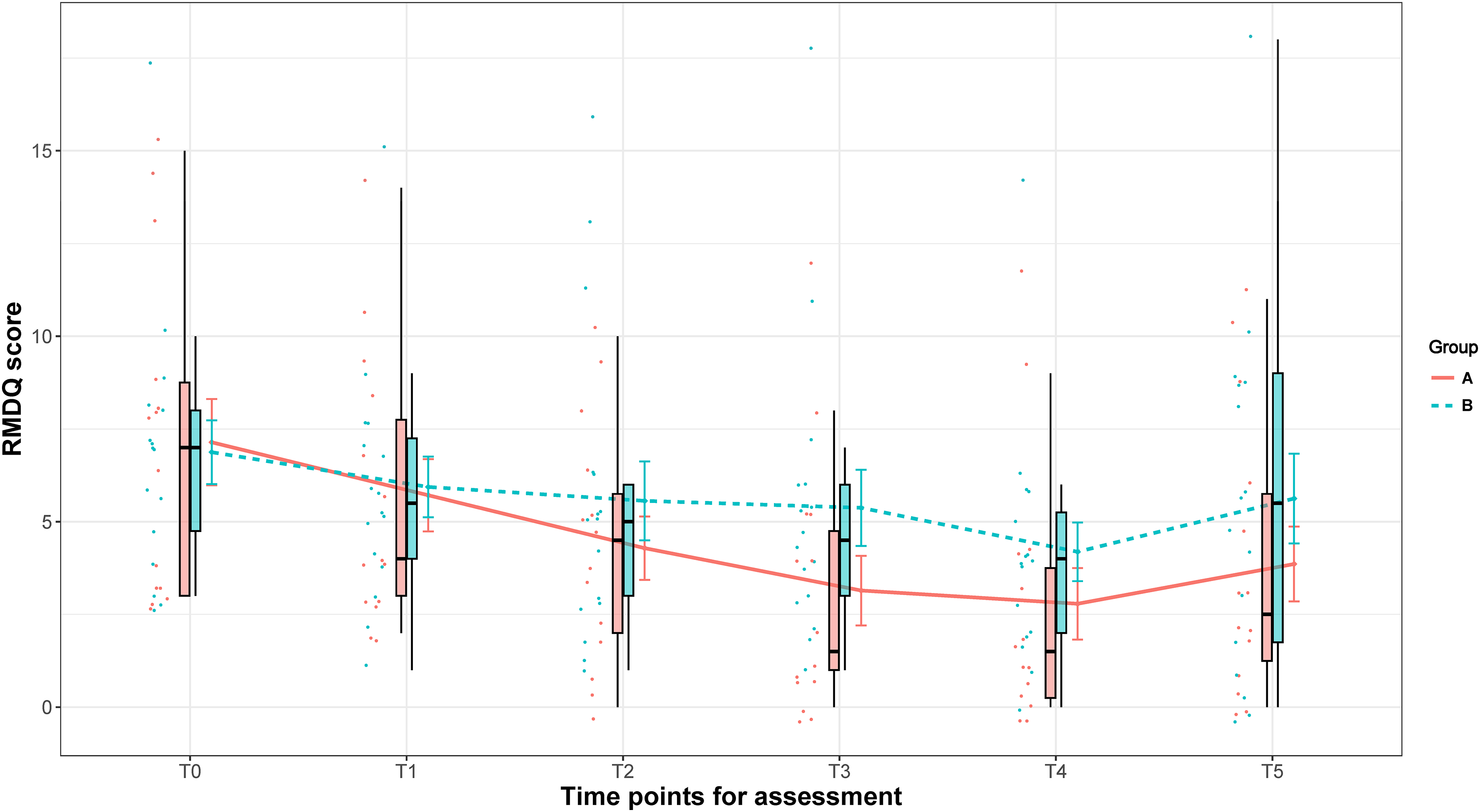
The physical function of participants in two groups at six time points*. *T0, Baseline assessment; T1, Week 1 assessment; T2, Week 2 assessment; T3, Week 3 assessment; T4, Post-intervention assessment (Week 4 post-randomization); T5, Follow-up assessment (Week 12 post-randomization). Raincloud plots indicated the distribution of raw data; Dash lines indicated the changes of means with error bars indicating standard errors.
Emotional status
The changes in the general psychological health of participants in the two groups were displayed in Table 1, Appendix H and Appendix I. There was a decreasing trend in the total score of DASS-21 throughout the study with oscillations in both groups. However, at most time points, the 95% CI of the mean differences included the null value, which suggested that the differences may not be statistically significant.
Quality of life
PCS-12 score increased gradually over 12 weeks. In Group A, there was an increase of 4.71 points (95% CI [-9.79, 0.38]) between the pre- and post-intervention measurements; A growth of 6.99 points (95% CI [-12.98, −1.01]) was seen between baseline and follow-up assessments. In Group B, the score increased by 1.88 points (95% CI [(−5.10, 1.35]) after completing treatment, and by 4.55 points (95% CI [(−7.95, −1.15]) at follow-up compared to baseline. The long-term effect size of PCS-12 seemed to be larger than the short-term in both groups (Table 1, Appendix H, Appendix J).
The average score of MCS-12 in both groups was greater than the reference score of 42 points, which suggested there was no obvious mental health problem observed in participants of this study. In addition, there was no noticeable difference in MSC-12 between baseline and either post-intervention or follow-up in the two groups, with 95% CIs containing the null value (Table 1, Appendix H, Appendix K).
The use of medication during acupuncture treatment
There were ten participants (four in Group A, and six in Group B) who took medications during the study period for a variety of health conditions. Among them, two participants (one for each group) took paracetamol for low back pain; the rest reported the use of paracetamol, NSAIDs, tramadol, or pregabalin for other health problems, such as headache, neck pain, neuropathic pain, et al. Appendix L. displays the frequency, timing, and dosage of taking the medications. Fisher's exact test suggested that there was no statistically significant difference in the use of painkillers between groups (P = 0.71).
Patient's satisfaction with the treatment
The median score of patients’ satisfaction with acupuncture treatment was 31/32 points in both groups, indicating at discharge, participants held a positive attitude towards acupuncture regardless of which manipulation scheme they received. Mann-Whitney U test illustrated that there was no between-group statistically significant difference in the satisfaction score (P = 0.70).
Discussion
In general, conducting a fully powered RCT to compare the effectiveness of sensitized-point acupuncture and routine integrative acupuncture package appears feasible. The methodology is acceptable and practical, with some suggestions proposed to finalize the study protocol for the full-scale study. However, despite the study being well-designed and rigorously conducted, there are acknowledged limitations.
The feasibility of the study
The recruitment rate, adverse event rate, completion of the outcome measures, and participant retention rate met the priori criteria for feasibility success, while the treatment compliance was slightly lower than the predefined threshold. As the treatment was delivered under the influence of COVID-19, the treatment compliance rate of 70% was considered acceptable. With the pandemic subsiding, its negative impact on clinic visits should be decreased in future studies. In general, conducting the fully powered RCT is feasible.
The potential effect of the two acupuncture manipulations for cLBP
The effectiveness of sensitized-acupoints needling for cLBP will be evaluated in a fully-powered RCT. Beforehand, some preliminary trends in clinical outcomes were seen in this feasibility study.
Acupuncture, no matter which practice protocol was delivered, presented a favorable effect in relieving pain and improving physical functions for patients with cLBP. As the number of acupuncture sessions grew, the average NPRS score in both acupuncture groups decreased steadily, which suggested the effect of acupuncture was cumulative. When compared to the baseline, the mean average NPRS score in Group A was decreased by 2.60 points at discharge, which exceeded the recommended minimal clinically important differences (MCID) of NPRS of 2 points in the assessment for LBP 37 ; In addition, the 95% confidence interval of mean difference between baseline and post-intervention was ranged 1.66 to 3.54 points, which indicated that participants had lower pain intensity on average post treatment, and the practice protocol of acupuncture in Group A was related to a clinically meaningful pain reduction. This finding was consistent with the previous clinical studies, which illustrated the favorable post-intervention effectiveness of acupuncture in intreating cLBP. 38
The mechanisms of the analgesic effect of acupuncture are found to be part of a multidimensional modulation process that is dominantly mediated by the neuroendocrine system, accompanied by regulation from numerous transmitters, mediators, and networks.39–41
Implication for future trials
The short-term analgesic effect of acupuncture for cLBP was acknowledged by several systematic reviews.38,42,43 In contrast, the long-term effect was inconclusive. As cLBP is a long-lasting health problem with a high recurrence probability, investigating the long-term effect should be more clinically meaningful. According to the results in this feasibility study, the largest effect size was achieved at discharge as a consequence of the accumulation from the previous treatments. At the week 12 follow-up, even though the improvement of pain intensity and physical function had somewhat deminished, it was still favorable compared to baseline. Therefore, week 12 post randomization can be considered as the primary time point for the fully-powered RCT.
Pain intensity is the most commonly used outcome in the assessment of chronic pain, and is recommended as the core outcome by experts group.44,45 In the results of this study, pain intensity was the most sensitive and straightforward outcome measure to evaluate the effect of acupuncture in the management of cLBP, as the mean differences in both groups were noticeable right after the first week of treatment; While the improvement in physical function was detected after two weeks of treatment. In spite of this, improving physical functioning is also an important treatment goal in the management of chronic pain. A systematic review suggested that long-term improvement of physical function in patients with chronic musculoskeletal pain was related to psychological factors, rather than the reduction in pain intensity and chronicity. 46 Similar results were obtained in other pooled analyses on the efficacy of first-line treatments for neuropathic pain, which demonstrated that the correlation between the changes in pain intensity and physical functioning was weak. 47 As there was no evidence to show the superiority of one outcome over another, both the pain intensity and physical functioning score at 12-week follow-up should be considered as the primary outcomes for a future fully-powered RCT.
In addition, quality of life and emotional functioning will be included in the secondary outcome measures, together with the dosage and frequency of painkillers taken by participants to better establish the effectiveness of acupuncture for cLBP.
According to recommendations from the Cochrane Back and Neck Group, a dropout rate of no more than 20% should be considered appropriate for clinical studies.
48
The drop-out rate in this feasibility study was 3.3%, which was much lower than the threshold, and might result in the underestimated sample size and the increased likelihood of a type II error. Therefore, in sample size calculation, we adopted a more prudent dropout rate of 10%.
As discussed above, the NPRS score and RMDQ score at the 12-week follow-up were selected as the primary outcome for the fully powered RCT. Given the effect sizes in the two groups generated in this feasibility study and the dropout rate, a minimum sample size of 84 participants would be needed in each group to detect a change of 0.98 points in the average NPRS score in a fully powered study, assuming a power of 80% and a significance level of 5%. In addition, according to the improvement of physical functioning, 107 participants per arm would be required for a fully powered RCT to achieve 80% power to detect the between-group difference of 1.77 points of RMDQ score with a two-sided significance of 95%. Taking all into consideration, a total of 214 patients will be needed in a powered study to detect the difference of NPRS score and RMDQ score between two groups.
Several participants reported the use of medications, which might have some impact on the evaluation of acupuncture's effect. Thus, in future data analyses, this information should be included as covariates to mitigate the interference with results, and adjust statistical analysis appropriately.
Limitations of the study
As acknowledged in the previous section, this study aimed to inform the feasibility and methodology of a full-scale RCT. Thus, the findings did not have statistical power to address the explicit effectiveness of the treatments delivered in the study, but they can show some potential trends based on limited evidence.
Beyond this, the assessment of clinical outcomes during follow-up might be influenced by potential confounding factors, including medications, physical therapy, or other interventions received during this time. These potential confounding variables need to be recorded properly in the full-scale study and adjusted using appropriate statistical techniques, such as Analysis of Covariance (ANCOVA) or Multiple Regression Analysis.
In addition, this study was carried out in a single center, and included a local population which might not be representative of the wider population of patients with cLBP, so the external validity of the study should be treated with caution. 49
Conclusion
The findings of the study suggested that it's feasible to conduct a fully powered RCT to evaluate the effectiveness and safety of sensitized-point acupuncture and routine integrative acupuncture package in the management of cLBP. Sensitized-point acupuncture presented a potentially positive effect in improving pain intensity and physical function of patients with cLBP.
Supplemental Material
sj-docx-1-bmr-10.1177_10538127241289343 - Supplemental material for Sensitized-points acupuncture versus routine integrative acupuncture for chronic low back pain: A randomized-controlled feasibility study
Supplemental material, sj-docx-1-bmr-10.1177_10538127241289343 for Sensitized-points acupuncture versus routine integrative acupuncture for chronic low back pain: A randomized-controlled feasibility study by Huijuan Tan, Steve Tumilty, Cathy Chapple, Guangyi Huang and G David Baxter in Journal of Back and Musculoskeletal Rehabilitation
Footnotes
Acknowledgements
We sincerely thank Mr David Jackson for his help with randomization, and all the participants for their contribution to the study.
Ethical approval
Ethical approval was granted by Health and Disability Ethics Committees (HDEC, reference no. 2022 FULL 11076).
Informed consent
All enrolled patients gave their written informed consent.
Author contributions
HT is involved in conceptualization, methodology, investigation, project administration, and writing original draft. ST, CC, GDB are involved in conceptualization, supervision, review and editing draft. GH is involved in data collection, review and editing draft. All authors have read and approved the final manuscript to be submitted.
Funding
This study was supported by PhD budget from School of Physiotherapy, and H.T. was supported by PhD scholarship. The funding was used for facilities in data collection.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data and materials used to support the findings of this study are available from the corresponding author upon request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.