
Abstract
Background
In recent years, the femoral neck system (FNS) has become increasingly widely used for Pauwels type III femoral neck fractures.
Objective
We performed a meta-analysis to investigate the safety and efficacy of FNS and the mainstream internal fixation method, cannulated screw (CS), in the treatment of Pauwels type III femoral neck fractures.
Methods
We systematically searched all research studies from PubMed, Embase, Web of Science, Cochrane, WANFANG, and the Chinese Academic Journal Full-Text Database (CNKI) from 2018 to July 2024 and conducted data extraction. The study was conducted on July 26, 2024. We used the PRISMA guidelines to assess the quality of the results of all included studies. In addition, we searched for references to relevant articles. After completing the literature search, we performed a manual literature screening to obtain studies that met the inclusion criteria. The outcomes were Harris Hip Score, operation duration, intraoperative blood loss, hospital stay, healing time, and postoperative complications.
Results
This meta-analysis ultimately included nine studies (n = 524) and conducted quality evaluations. All nine articles were retrospective cohort studies. The study exhibited statistically significant variations between the FNS and CS groups in relation to total complications (95% confidence interval (CI)= [0.11, 0.40], odds ratio (OR) = 0.21, P < 0.001), Harris Hip Score (95%CI = [2.14, 3.65], mean difference (MD) = 2.89, P < 0.001), Femoral head necrosis (95%CI = [0.17, 0.86], OR = 0.38, P = 0.02), Internal fixation failure (95%CI = [0.06, 0.50], OR = 0.17, P = 0.001), Medium femoral neck shortening (95%CI = [0.17, 0.53], OR = 0.30, P < 0.001), intraoperative blood loss (95%CI = [11.57, 26.80], MD = 19.19, P < 0.001), Operation duration (95%CI = [−15.20, −2.17], MD = −8.69, P = 0.009), and healing time (95%CI = [−1.30, −0.32], MD = −0.81, P = 0.001).
Conclusion
This meta-analysis showed that in Pauwels type III femoral neck fractures, the femoral neck system has a shorter operative time, a lower rate of postoperative complications, a shorter healing time, less shortening of the femoral neck, and a higher Harris Hip Score compared with cannulated screws, but increases intraoperative blood loss. However, more clinical studies are needed to confirm our conclusions due to our small sample size and lack of randomized controlled trials.
Introduction
Hip fractures, as serious disabling fractures, cause approximately 4.5 million disabilities worldwide each year and are expected to increase to 21 million in the next 40 years. 1 Femoral neck fractures account for 3.58% of total body fractures and are common in hip fractures. 2 The Pauwels classification method is usually applicable to adult patients and is a commonly used classification method for femoral neck fractures. This classification system is based on different fracture angles of the fracture line: Pauwels type I fracture angle is less than 30 °, Pauwels type II fracture angle is between 30 ° and 50 °, and Pauwels type III fracture angle is more than 50 °. Adult Pauwels type III femoral neck fractures are often caused by high-energy trauma and have received much attention in recent years.3–5 In younger patients, internal fixation preserves their natural joint structure and avoids unnecessary joint replacement. Therefore, despite the fact that internal fixation may lead to serious complications such as avascular necrosis of the femoral neck, bone nonunion, and internal fixation failure (cutting out/screw loosening/screw penetration of the femoral head), it is currently the mainstay of treatment for Pauwels type III fractures of the femoral neck. 6
At present, the most traditional and widely used fixation method is cannulated screw (CS) internal fixation, which has the advantages of minimal damage to surrounding soft tissues, protection of femoral head blood supply, anti-rotation effect, low surgical difficulty, and short operation duration.7–9 In 2018, a new minimally invasive femoral neck implant system (FNS) was introduced. FNS is fixed to the femoral shaft through a minor incision surgery to reduce the footprint of the prosthesis. This method of fixation also highlights the compressive healing of the fracture ends. 10 Recently, Teng et al. found FNS internal fixation to provide better biomechanical stability than CS internal fixation in the treatment of Pauwels type III femoral neck fracture, with dual effects of sliding compression and angular stabilization. 11 Similar biomechanical studies on the two fixation methods of FNS and CS provided a clinical research basis.
In recent years, many studies have compared the clinical efficacy of CS and FNS in treating Pauwels type III femoral neck fractures. Still, the results of different studies are inconsistent.10,12–19 In Chung et al.'s subgroup analysis of Pauwels type III femoral neck fractures, there was no significant difference between the FNS and CS groups in terms of operative time. 17 Whereas in the study by Huang et al., the FNS group had significantly lower operative time than the CS group. 12 Therefore, in order to help researchers and doctors obtain a more reliable evidence base, assist doctors in selecting the best fixation method in clinical decision-making, and provide patients with a clearer understanding of the expected effects and potential risks of these two fixation methods, we conducted this meta-analysis to integrate existing clinical data on the occurrence of clinical and long-term outcomes such as intraoperative blood loss, operation time, fracture healing time, length of hospital stays, femoral neck shortening, Harris Hip Score, postoperative complications (including bone nonunion, internal fixation failure, and femoral head necrosis). We compared the efficacy and safety of CS and FNS in treating Pauwels type III femoral neck fracture.
Materials and methods
Search strategy
We systematically searched all research studies from PubMed, Embase, Web of Science, Cochrane, WANFANG, and the Chinese Academic Journal Full-Text Database (CNKI) from 2018 to July 2024. We used the following keywords for our search: “vertical,” “Pauwels,” “femoral neck fracture,” “femoral neck system,” “FNS,” and “screws.” The Mesh keywords used for the search were “screw” and “femoral neck fracture.” The study was conducted on July 26, 2024. There were no restrictions on the retrieval language of literature, and to ensure the results of our meta-analysis were verifiable and convincing, we applied the PRISMA guidelines to evaluate the quality of findings reported in all the studies included. In addition, we also searched for references to relevant articles. After completing the literature search, manual literature screening was conducted to obtain studies that met the inclusion criteria. Our systematic review follows the preferred reporting items in the PRISMA guidelines and was registered in PROSPERO under registration number CRD42023456980.
Inclusion and exclusion criteria
When the study we included met the following PICOS criteria, it was considered eligible for inclusion: 20
(1) Population: Patients were adults and with femoral neck fractures of Pauwels type III; (2) Intervention: FNS, or FNS combines other treatments; (3) Comparison: CS [inverted triangle cannulated screws, cannulated compression screw, triple screw]; (4) Outcomes: The final included studies had at least one of the following surgical or follow-up outcomes, including postoperative complications (femoral head necrosis, nonunion, implant failure), operation duration (minutes), intraoperative blood loss (ml), Harris Hip Score, hospital stay (days), and mean healing time (months), where the Harris Hip Score was the primary outcome variable; (5) Study design: The type of study needs to be a randomized controlled clinical trial, prospective cohort study or retrospective cohort study.
Our study requires a follow-up period of no less than six months and a follow-up rate of at least 90%.
Exclusion criteria
(1) Studies not published in English or Chinese; (2) Non-Pauwels type III femoral neck fractures; (3) No relevant data or data cannot be extracted; (4) Repeated literature, biomechanics research, letters, review articles, case report, and unpublished randomized controlled clinical trials.
Data extraction
Our literature screening was conducted by two independent researchers using the same inclusion criteria and exclusion criteria. At each stage of the literature search, Kappa values were calculated to determine the degree of consistency among reviewers in research selection. The consistency among reviewers is a priori correlated kappa value: κ = 1 indicates “complete” consistency; 1.0> κ ≥ 0.8 indicates “almost complete” consistency; 0.8> κ ≥ 0.6 indicates “basic” consistency; 0.6> κ ≥ 0.4 indicates “moderate” consistency; 0.4> κ ≥ 0.2 indicates “generally” consistent; κ<0.2 indicates’ slight ‘consistency. We will discuss the parts with objections with senior authors. Firstly, we imported the collected literature into Endnote's literature management system. Second, duplicates were excluded through Endnote's “Find Duplicates” function and manual screening. Third, titles and abstracts were read and screened according to the inclusion and exclusion criteria. After the initial screening, we read the full text of potential articles and included those that met the criteria. Researchers used standardized data extraction tables to extract relevant data from the final included articles. The extracted data included study design, publishing date, mean operating time, age, authors, duration of follow-up, gender, healing time, sample size, degree of femoral neck shortening, hospital stay, intraoperative blood loss, Harris Hip Scores at final follow-up and postoperative complications (femoral head necrosis, nonunion, implant failure).
Quality evaluation
We conducted a bias risk assessment based on the Cochrane Bias Risk Assessment Manual and used the 9-point Newcastle Ottawa Scale to evaluate the quality of the cohort study. Studies with scores greater than six are considered to be of high quality. Conduct bias risk assessment through eight projects: representativeness of exposure groups; representativeness of non-exposure groups; no outcome indicators to be observed at the beginning of the study; determination of exposure factors; Integrity of follow-up between the exposed and non-exposed groups; evaluation of outcome indicators; adequate follow-up time; consider comparability between exposed and non-exposed groups in the design and statistical analysis.
Statistical analysis and investigation of heterogeneity
We used mean difference (MD) for continuous outcomes (such as mean operative time) with 95% confidence intervals (CI). Mantel-Haenszel odds ratio with a 95% CI was used to evaluate dichotomous results such as complications (implant failure, nonunion, femoral head necrosis). Used the I²-test measuring heterogeneity between studies. When I²>50% indicated significant heterogeneity, we used a random effects model to assess the results. Identify and analyze sources of heterogeneity in literature with significant heterogeneity. When I²≤50%, heterogeneity may not be significant, and we use a fixed-effects model to evaluate the results. The results were statistically significant when the
Results
Study characteristics and search results
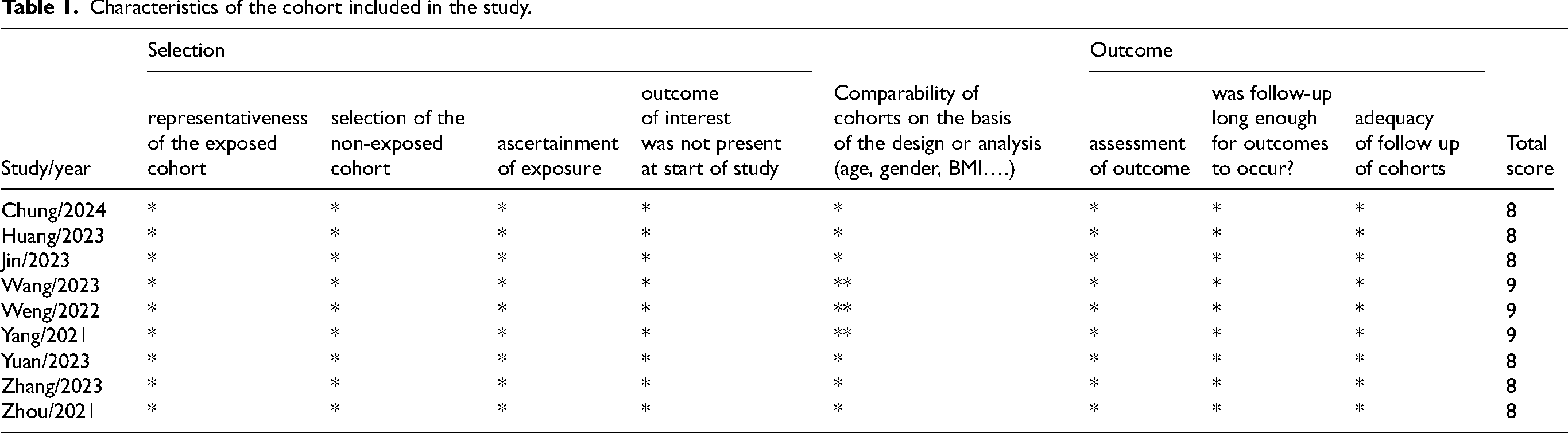
A total of 301 articles that may meet the requirements were retrieved, including PubMed (n = 50), Embase (n = 85), Web of Science (n = 108), Cochrane (n = 5), Chinese Academic Journal Ful Text Database (n = 41), and WANFANG (n = 12). 137 duplicate documents were screened and excluded, and 149 records were excluded through a detailed reading of the title and abstract. Most reasons for exclusion were: unrelated articles (n = 83), biomechanical research (n = 46), and the experimental screw does not meet the requirements (n = 20). After reviewing the complete text of the remaining 15 articles in detail, we ultimately incorporated nine articles into our meta-analysis and evaluated their quality. The nine studies were published between 2021 and 2024, all from Asia, including one from South Korea and eight from China. All nine articles were retrospective cohort studies, and all relevant data from these nine articles were entered into STATA and RevMan by two independent researchers with consistent results. During the title review, abstract review, full-text review stages, and data extraction, the consensus of reviewers on research selection reaches perfection(κ = 1). A total of 524 patients with Pauwels type III fracture of the femoral neck were included; 242 patients were included in the FNS group and 282 in the CS group. The flowchart of the included studies is presented in Figure 1. The experimental group was defined as FNS and the control group as CS. Table 1 summarizes the cohort characteristics of these nine studies. The score for each study is 8 or 9 points, indicating that they are all high-quality articles. In each study, there were no apparent differences in Pauwel's angle, gender, age, BMI, and injury side. The average follow-up time for all studies exceeded six months. Table 2 lists the basic characteristics of the included studies.
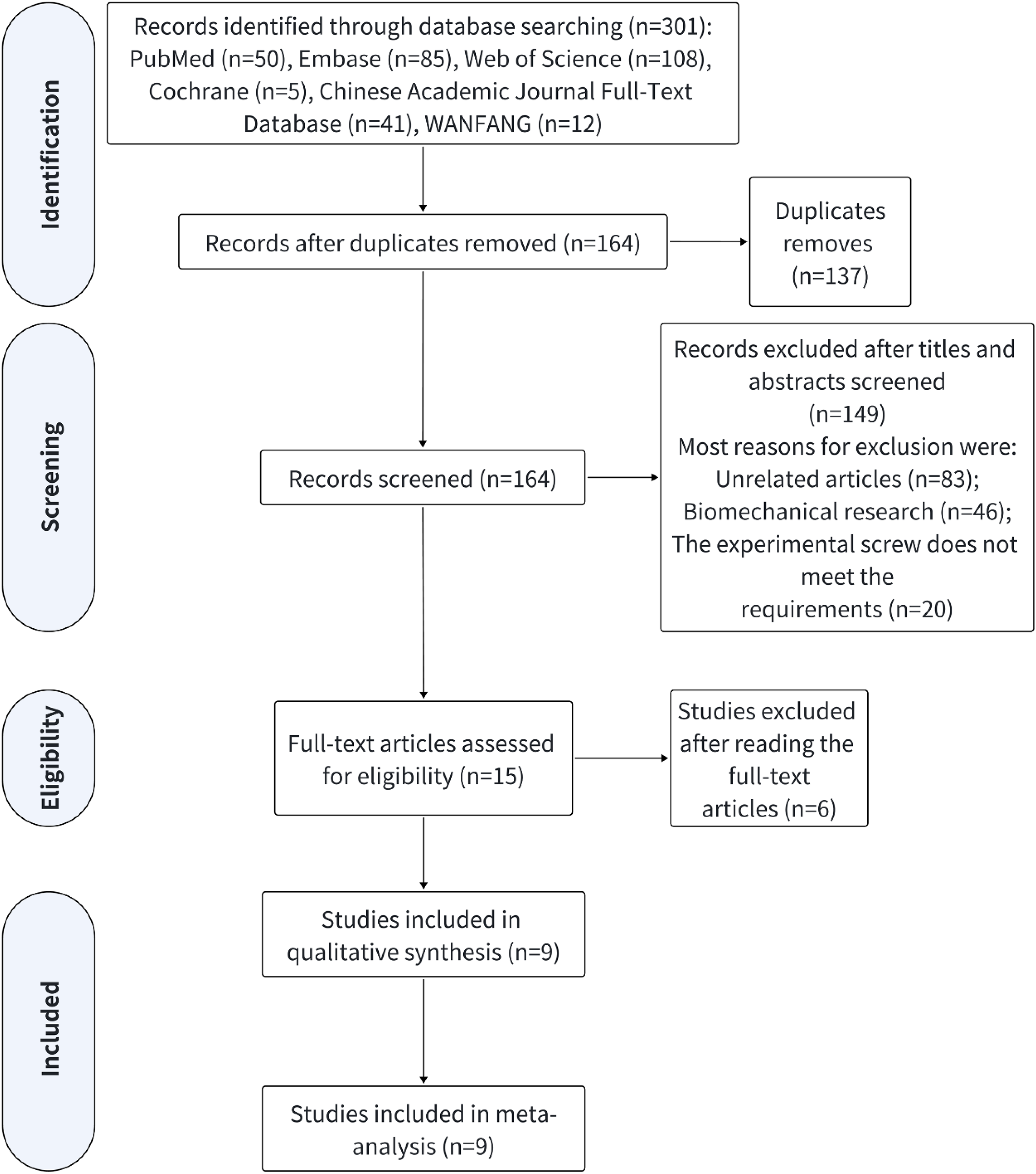
The search process for research and the process of excluding irrelevant articles.
Characteristics of the cohort included in the study.
Essential features of the six articles included.
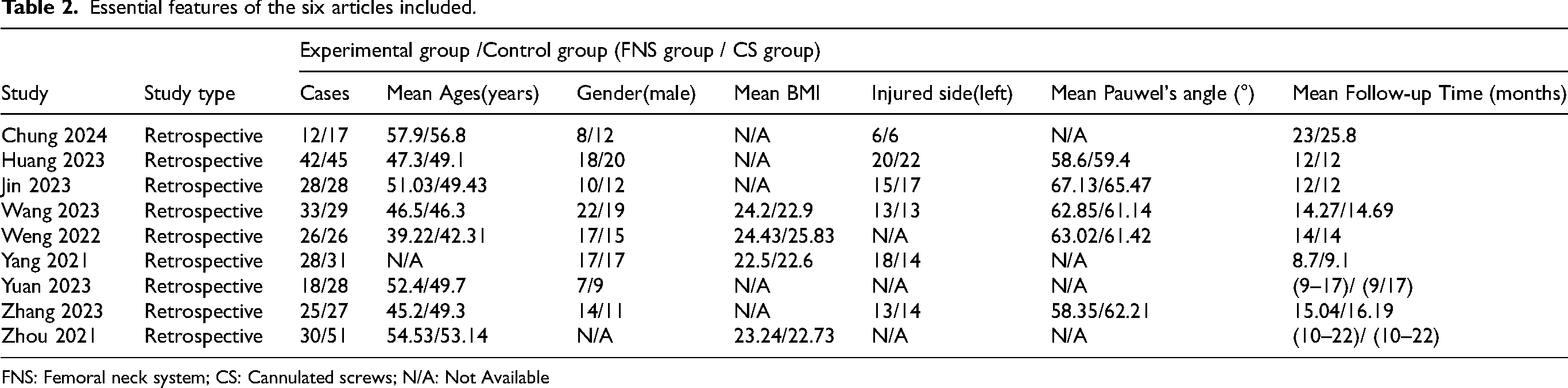
FNS: Femoral neck system; CS: Cannulated screws; N/A: Not Available
Results of meta-analysis
Harris hip score
Seven of the nine included articles compared the Harris Hip Score between the two fixation modalities. Pooled data shows statistically significant differences between the FNS and CS groups. Harris Hip Scores were significantly higher in the FNS group than in the CS group (95%CI = [2.14, 3.65], MD = 2.89,
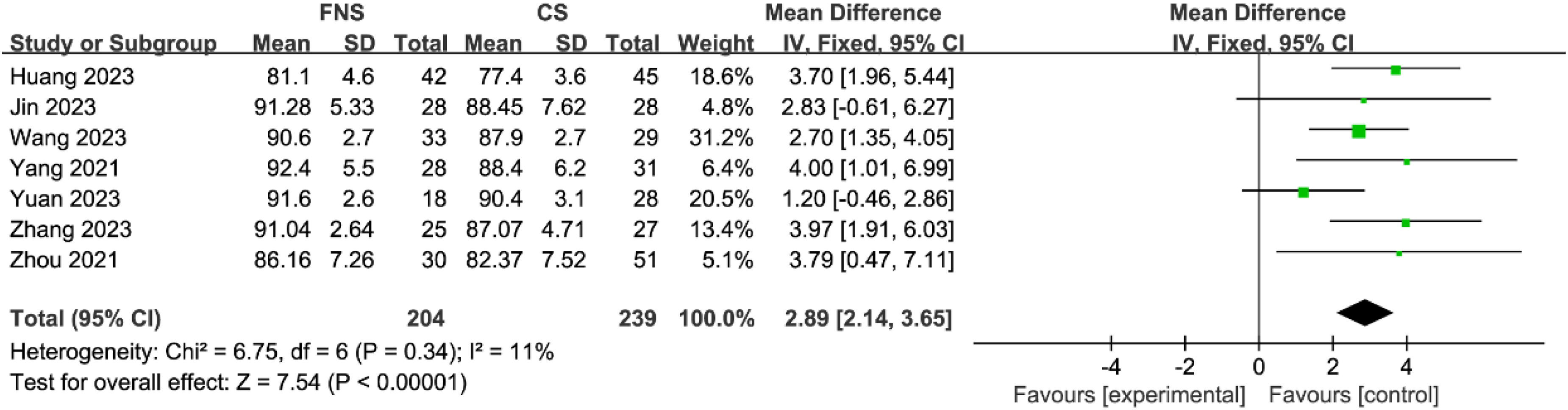
Forest plot of Harris hip scores in experimental and control groups.
Operation duration
Eight articles compared the operation duration of FNS and CS in treating Pauwels type III fractures of the femoral neck. One article was excluded because it used the median to record operation duration.
13
The remaining seven articles were analyzed after summarizing the data. Due to the significant heterogeneity between the research results (I² = 94%), we analyzed them using a random-effects model. It was found that the operation duration in the FNS group was significantly shorter than in the CS group (95%CI = [−15.20, −2.17], MD = −8.69,
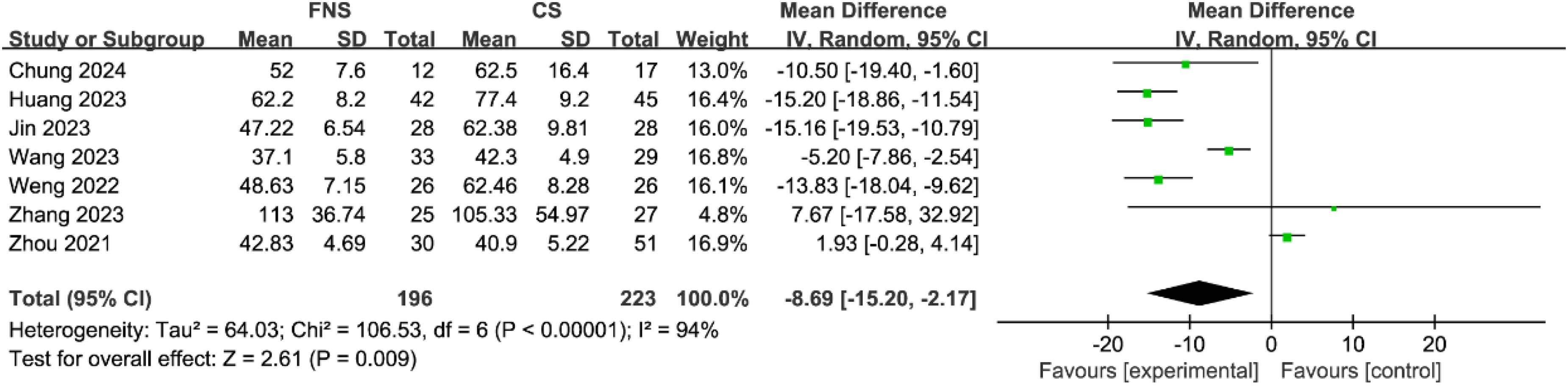
Forest plot of operation duration for experimental and control groups.
Intraoperative blood loss
Seven articles compared intraoperative blood loss between the two fixation modalities of treatment. We analyzed them using a random-effects model (I² = 92%). The study revealed that the amount of blood lost during operations was significantly lower in the CS group than in the FNS group (95%CI = [11.57, 26.80], MD = 19.19,
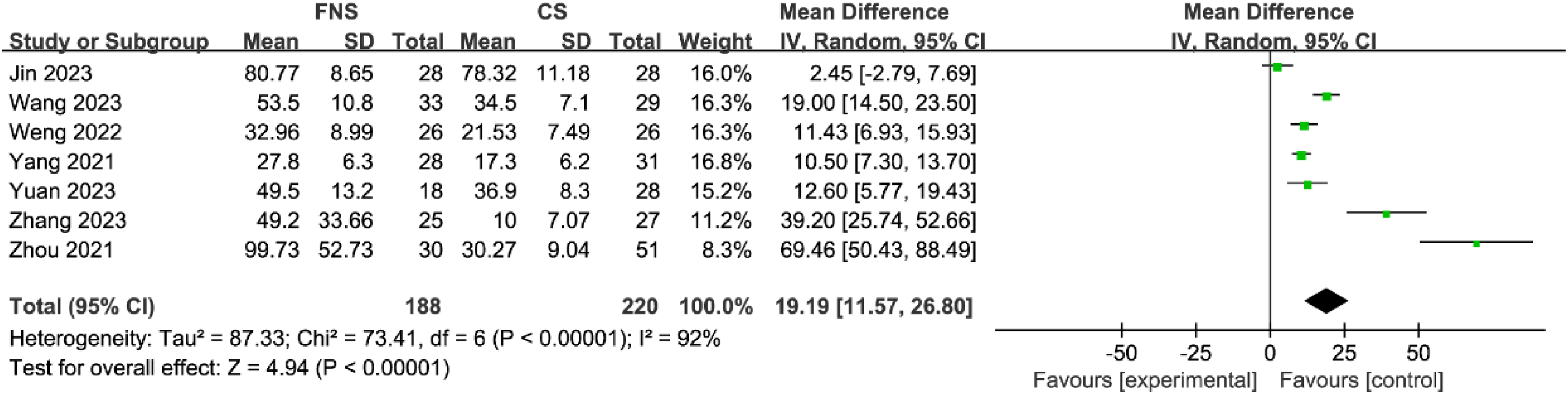
Forest plot of intraoperative blood loss for experimental and control groups.
Hospital stay
Six articles compared the hospital stay of FNS and CS in the treatment of Pauwels type III femoral neck fractures. Due to significant heterogeneity, we found that Huang et al.'s study may be the source of heterogeneity by deleting and reanalyzing the data.
12
After excluding this study, heterogeneity significantly decreased (I² = 0%). The remaining five articles found no statistically significant difference in hospital stay between the FNS group and the CS group (95%CI = [−0.21, 0.27], MD = 0.03,
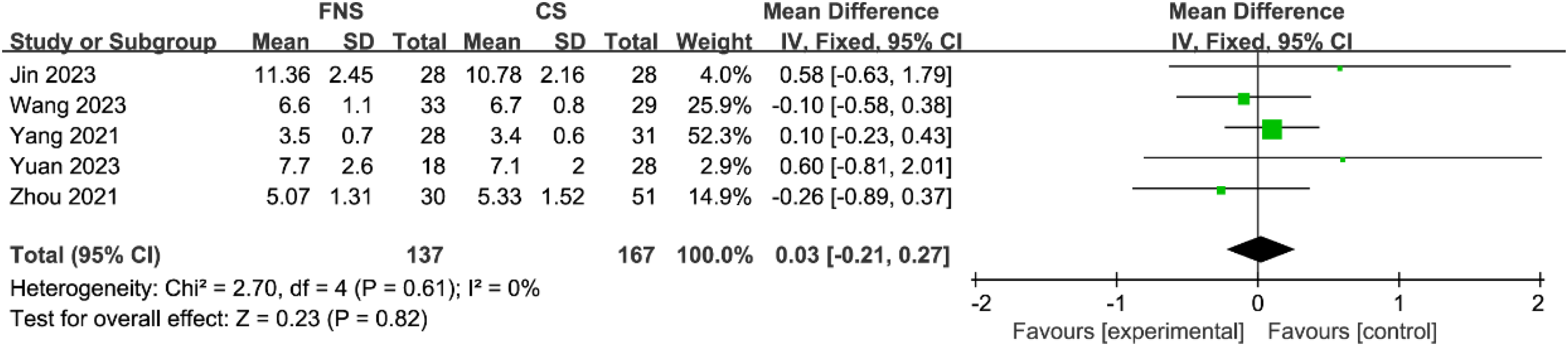
Forest plot of hospital stay for experimental and control groups.
Healing time
There are eight articles comparing the healing times of the two fixation treatments. Two articles were excluded due to the use of “weeks” as a unit to record the healing time of patients’ fractures.12,18 The remaining six articles were analyzed after summarizing the data, and we analyzed them using a random-effects model (I² = 80%). The FNS group had statistically significantly reduced healing time compared to the CS group (95%CI = [−1.30, −0.32], MD = −0.81,
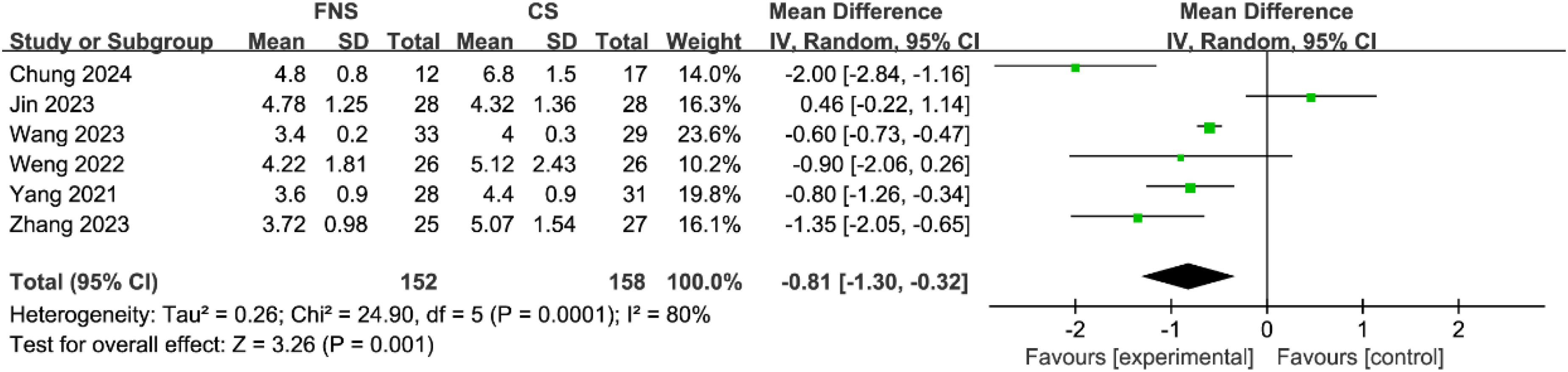
Forest plot of healing time for experimental and control groups.
Postoperative complications (femoral head necrosis/nonunion/fixing failure)
Eight articles compared the rates of postoperative complications (primarily femoral head necrosis, nonunion, and failure of fixation) between FNS and CS for the treatment of Pauwels type III fractures of the neck of the femur. The comparison revealed that the rate of femoral head necrosis in the FNS group was significantly lower than that in the CS group (95%CI = [0.17, 0.86], OR = 0.38,
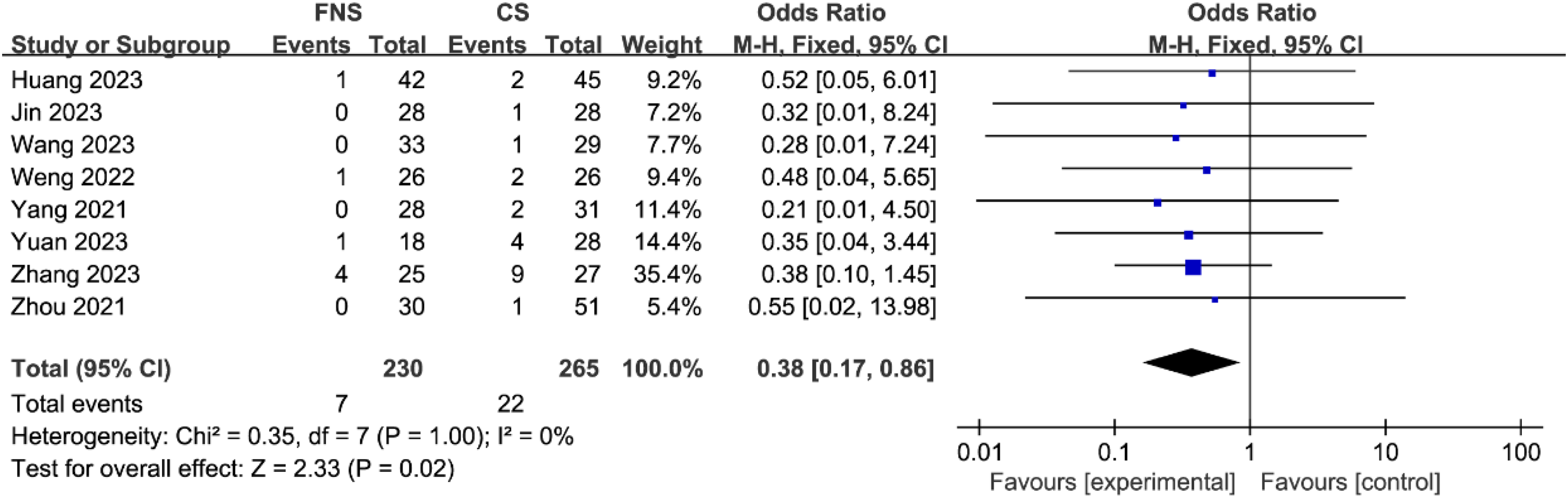
Forest plot comparing femoral head necrosis in the experimental and control groups.
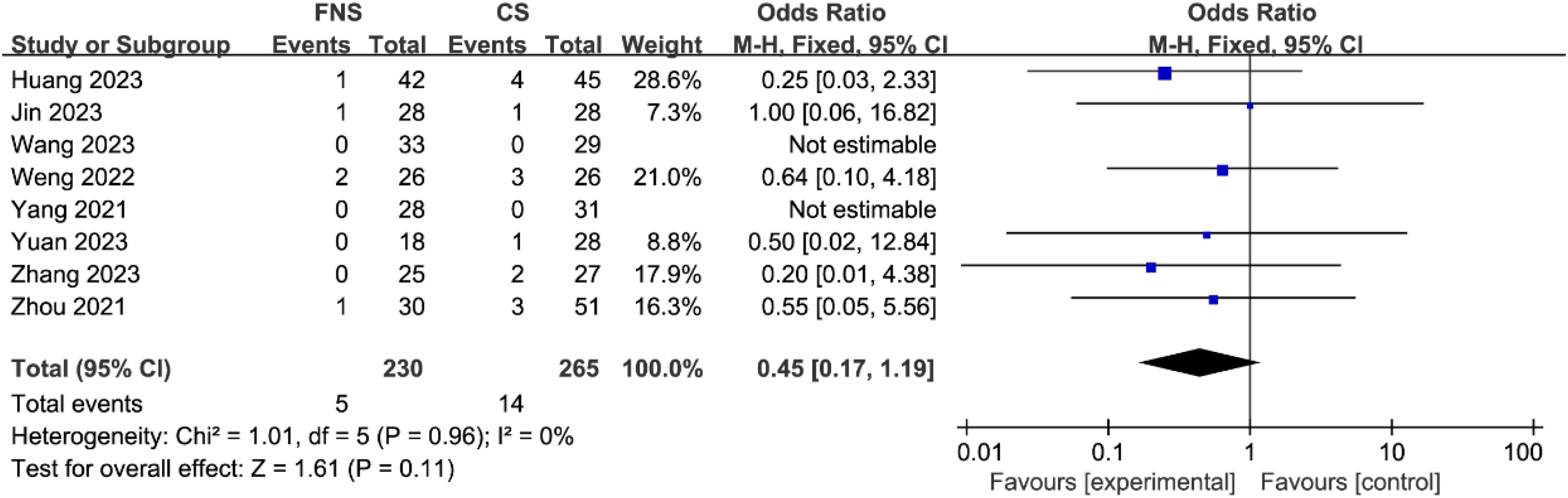
Forest plot comparing nonunion in the experimental and control groups.
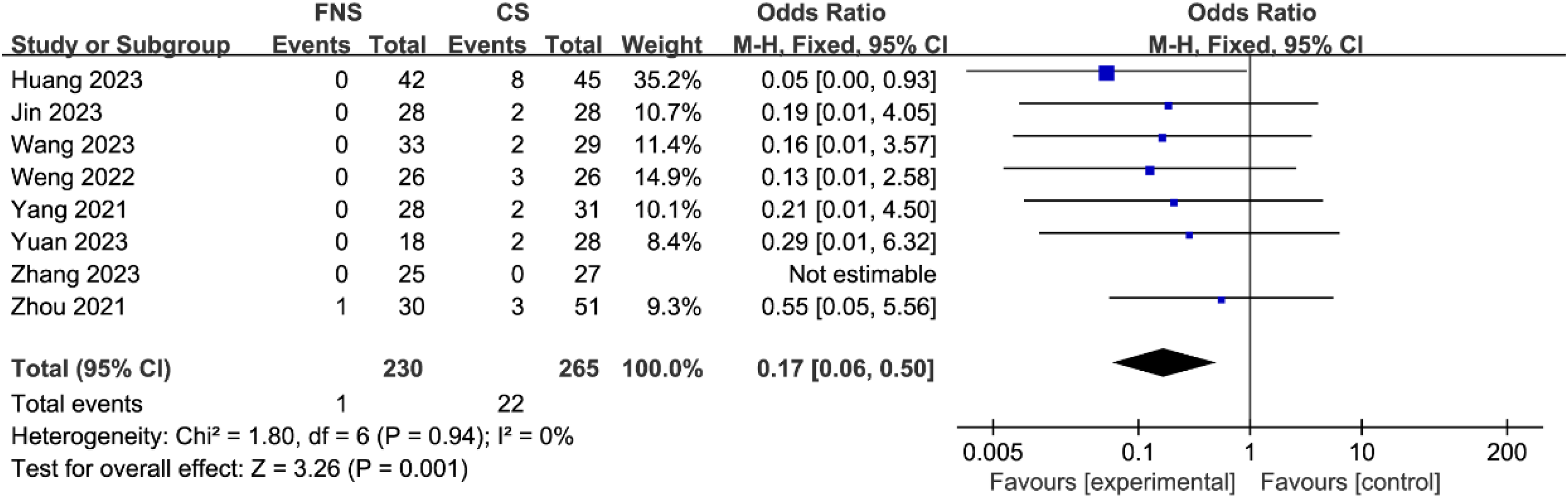
Forest plot comparing fixing failure in the experimental and control groups.
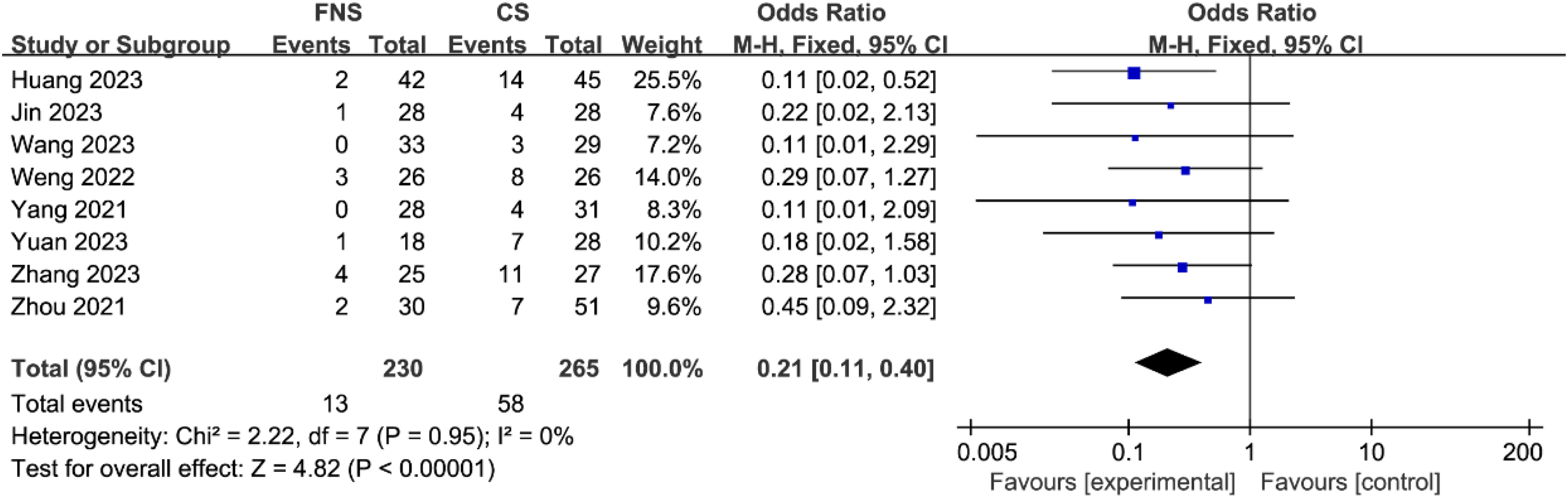
Forest plot comparing total complications in the experimental and control groups.
Femoral neck shortening
Four articles compared the Femoral neck shortening between the two treatment methods. The incidence of medium shortening of the femoral neck was statistically significantly lower in the FNS group than in the CS group (95%CI = [0.17, 0.53], OR = 0.30,
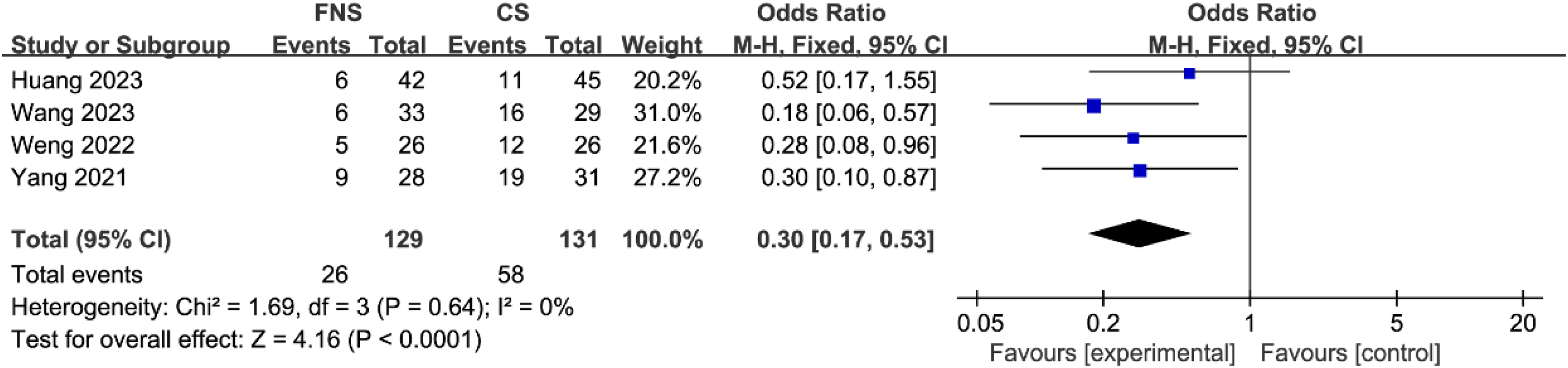
Forest plot comparing medium femoral neck shortening in the experimental and control groups.
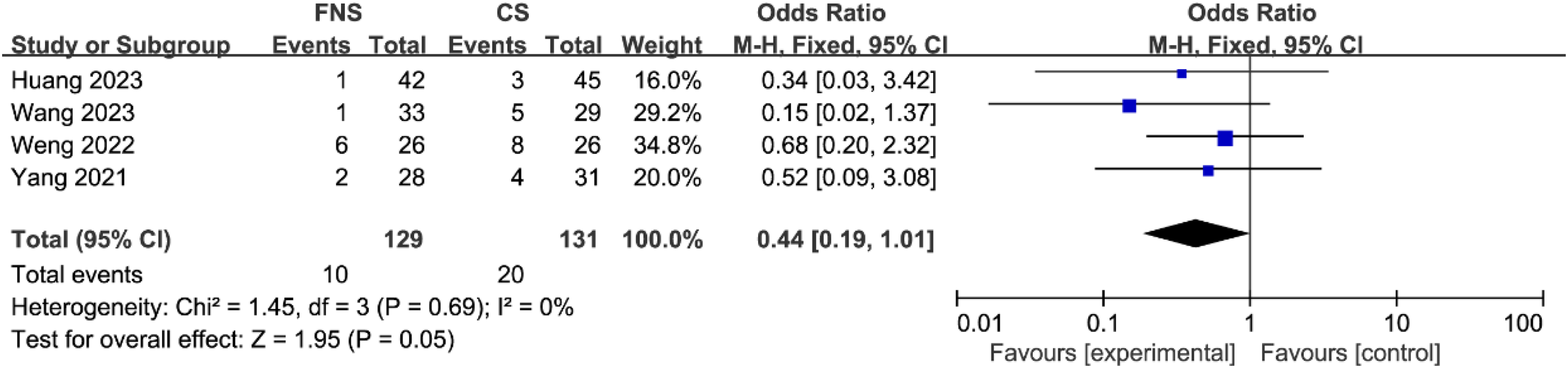
Forest plot comparing heavy femoral neck shortening in the experimental and control groups.
Risk of bias and sensitivity analysis
We performed Egger's test to assess bias, and the results showed no significant bias for each outcome, as shown in Table 3. We used RevMan (Version 5.4) to exclude each study and STATA (Version 11.0) to create metainf plots for sensitivity analysis. Comparing the metainf plots of each result, it was found that all results were stable. Two independent researchers validated the obtained outcome variables separately in RevMan and STATA, and confirmed the accuracy of the data through literature review, with completely consistent results. This indicates that our outcome variables have good reliability and validity.
Weighted mean differences (or odds ratio) in outcomes and Egger's test p-value.
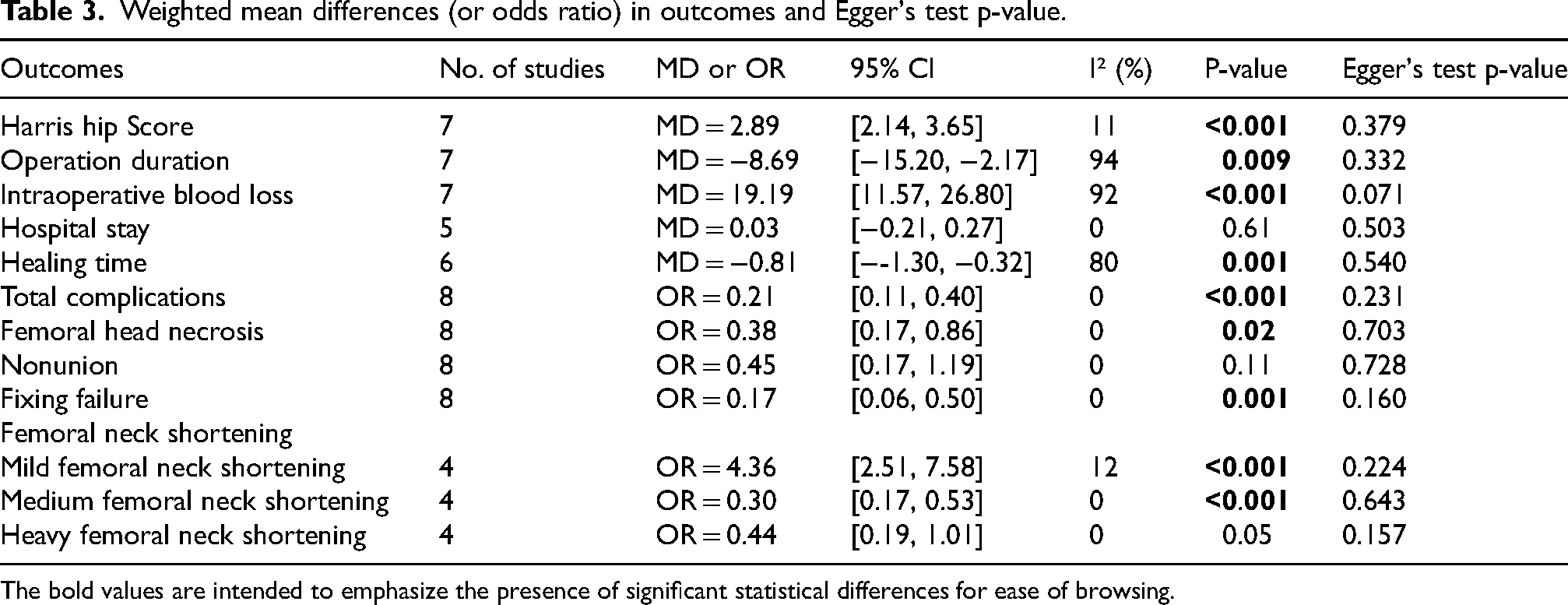
The bold values are intended to emphasize the presence of significant statistical differences for ease of browsing.
Discussion
Femoral neck fracture, known as the “last fracture in life” due to its high disability and mortality rates, is a common and severe type of fracture in the clinic.21,22 The cause of femoral neck fractures in adults with larger Pauwels’ angles is usually high-energy trauma. Such fractures require stronger bone healing structures and more stable fixation to cope with high shear forces.23,24 Anatomical reduction and rigid internal fixation represent the preferred treatment options for adult patients who have suffered from femoral neck fractures of Pauwels type III. Therefore, choosing an excellent internal fixture is extremely important. 25 The choice of internal fixation for femoral neck fractures of Pauwels type III is a contentious issue because of the high incidence of femoral neck shortening, fracture nonunion, and femoral head necrosis, regardless of the type of fixation used. 8 CS is widely used in China for all types of femoral neck fractures. 26 However, since CS cannot suppress vertical shear displacement, the complication rate tends to be high when used to treat Pauwels type III femoral neck fractures. The FNS implant, a new minimally invasive device, has shown initial promise in treating Pauwels type III femoral neck fractures in clinical settings. The FNS design combines the advantages of fixed angle stability of the Sliding hip screw (SHS) with the minimal intrusion of the CS. 27 A finite element analysis by Xia et al. found that FNS has weaker structural stability than CS. 23 Wang et al. performed a biomechanical comparison of the effectiveness of FNS, IT nail, and CS in treating Pauwels type III femoral neck fractures. The results showed that the anteroposterior (AP) bending stiffness and axial stiffness of FNS are higher than CS. 28 Due to the increasing clinical application of FNS in Pauwels III femoral neck fractures in recent years,17–19 it is necessary to integrate existing data through meta-analysis to study the safety and effectiveness of FNS and CS treatment for Pauwels III femoral neck fractures. This helps surgeons make clinical decisions, and patients can also understand the expected effects and risks of different fixation methods based on the analysis results, thereby participating in treatment decisions. Researchers can also use the results of this study to provide direction for future research. At the same time, this can also promote the development and validation of new internal fixation devices.
Our meta-analysis compared the femoral neck system (FNS) with traditional cannulated screws (CS) and analyzed their clinical results in the treatment of Pauwels type III femoral neck fracture. The Harris Hip Score consists of two main components, the pain score and the function score, totaling 100 points, with higher scores indicating better hip function. This scoring system is widely used in clinical practice to help doctors and patients understand the effectiveness of treatment and functional improvement. Analysis of the pooled data showed that the FNS was superior to the CS with respect to the Harris Hip Score. This result is consistent with the studies we included, so FNS may have an advantage in long-term efficacy. Regarding postoperative complications, we focused on exploring three types: femoral head necrosis, nonunion, and internal fixing failure. After comparing and analyzing the data, we found that FNS had a slight advantage over CS in reducing postoperative nonunion. However, the statistical difference in this small advantage was not significant. Compared with the CS group, the probability of femoral head necrosis and internal fixing failure in the FNS group is significantly lower. We think that the angular stability structure and a small side plate of FNS can reduce the implant's footprint while also fixing the femoral head by locking the screws onto the bolts. This characteristic enables FNS to resist the inversion stress of the Pauwels type III femoral neck fracture, effectively reducing the incidence of fixing failure (cut out/Loose screws/Screw penetrates the femoral head).29,30
After pooling the incidence of three types of complications, the rate of postoperative complications was found to be lower and statistically significantly different in the FNS group than in the CS group. Femoral neck shortening is a severe complication affecting the life of patients with high Pauwels angle femoral neck fractures. No matter which fixation method is used for treatment, the incidence of femoral neck shortening is high. 31 The degree of femoral neck shortening is usually measured as a categorical variable and categorized into one of the following groups: mild shortening (<5 mm), medium shortening (6–10 mm), or heavy shortening (>10 mm). 32 The angular stability of FNS gives it a huge theoretical advantage in reducing femoral neck shortening. Our study compared the differences between these two fixation methods in medium and heavy shortening of the femoral neck, and the results showed that for medium femoral neck shortening, the incidence was significantly lower in the FNS group compared to the CS group. Although the incidence of heavy femoral neck shortening was slightly higher in the CS group than in the FNS group, the difference was insignificant. FNS can provide additional intraoperative compression at the fracture site, which is beneficial for reducing femoral neck shortening. 33 The effective prevention of femoral neck shortening by FNS is also the reason why it can achieve a higher Harris Hip Score.
We attempted to address the heterogeneity by excluding studies, but heterogeneity in the included studies was unavoidable because of the different surgeons who performed the procedures and because there were differences in gender, ethnicity, age, length of follow-up, and surgical methods. Due to the significant heterogeneity in research results on operation duration, intraoperative blood loss, and fracture healing time (I²> 50%), we analyzed them using a random-effects model. This is because the use of fixed-effects models in situations of high heterogeneity can lead to biased results, as the model assumes that the studies share a common true effect. Random effects models reduce this risk of bias by recognizing the variability of true effects. Cannulated screw internal fixation is generally a closed reduction internal fixation, so simple cannulated screws often have advantages in operation duration and intraoperative blood loss.
34
Zhou et al.'s study found that the surgical duration of the FNS group was slightly longer than that of the CS group, but the difference was not statistically significant (
Our meta-analysis inevitably has some flaws and limitations. (1) Due to limited clinical research on Pauwels type III femoral neck fractures, our study only included nine articles, including 524 patients. (2) The articles we have entered are all retrospective cohort studies. Due to the lack of randomized controlled trials, our research evidence level is not high. (3) The included articles have heterogeneity, which has a certain impact on some research outcomes. (4) Our meta-analyses are based on existing research data and, therefore, may not reflect the latest research findings or advances in clinical practice promptly. Larger samples, as well as high-quality, multicenter randomized controlled clinical trials, are needed in the future, and further comparisons of the femoral neck system with other commonly used treatments are needed to ensure the broad applicability of the results.
Conclusion
This meta-analysis shows that in Pauwels type III femoral neck fractures, compared to cannulated screw, the femoral neck system has less operation duration, lower incidence of postoperative complications, shorter healing time, less femoral neck shortening, and higher Harris Hip Score but increases intraoperative blood loss. The femoral neck system has significant advantages in treating Pauwels type III femoral neck fractures. However, due to our small sample size and lack of randomized controlled trials, we will need larger samples and high-quality multicenter randomized controlled clinical trials in the future to validate our conclusions.
Supplemental Material
sj-doc-1-bmr-10.1177_10538127241296340 - Supplemental material for Comparison of clinical efficacy between femoral neck system and cannulated screw in Pauwels type III femoral neck fracture: A meta-analysis
Supplemental material, sj-doc-1-bmr-10.1177_10538127241296340 for Comparison of clinical efficacy between femoral neck system and cannulated screw in Pauwels type III femoral neck fracture: A meta-analysis by Kailun Zhuang, Jingyi Wu, Yusen Yang, Tianmo Bai and Baofeng Li in Journal of Back and Musculoskeletal Rehabilitation
Footnotes
Author contributions
All authors contributed to this paper. KZ and JW contributed equally to the meta-analysis. BL, KZ and JW designed the study and performed the literature search, data extraction and analysis. KZ drafted the manuscript. BL, JW, YY, and TB revised the manuscript for grammatical and formatting issues, and critically reviewed the experimental procedures. BL provided funding for this study. BL, JW, and KZ completed revisions of the manuscript. All authors read the final manuscript in detail and agreed to its publication.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (No. 81972895) and General Hospital of Southern Theater Command of PLA Fund project (No. 2022NZA002).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All relevant data is included in the article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.